
Abstract
Background
The US Veterans Health Administration (VA) is transforming its healthcare system to create a Whole Health System (WHS) of care. Akin to such reorganization efforts as creating patient-centered medical homes and primary care behavioral health integration, the WHS goes beyond by transforming the entire system to one that takes a proactive approach to support patient and employee health and wellness. The SARS-CoV-2 pandemic disrupted the VA’s healthcare system and added stress for staff and patients, creating an exogenous shock for this transformation towards a WHS.
Objective
We examined the relationship between VA’s WHS transformation and the pandemic to understand if transformation was sustained during crisis and contributed to VA’s response.
Methods
Qualitative interviews were conducted as part of a multi-year study of WHS transformation. A single multi-person interview was conducted with 61 WHS leaders at 18 VA Medical Centers, examining WH transformation and use during the pandemic. Data were analyzed using rapid directed content analysis.
Results
While the pandemic initially slowed transformation efforts, sites intentionally embraced a WH approach to support patients and employees during this crisis. Efforts included conducting patient wellness calls, and, for patients and employees, promoting complementary and integrative health therapies, self-care, and WH concepts to combat stress and support wellbeing. A surge in virtual technology use facilitated innovative delivery of complementary and integrative therapies and promoted continued use of WH activities.
Conclusion
The pandemic called attention to the need for healthcare systems to address the wellbeing of both patients and providers to sustain high quality care delivery. At a time of crisis, VA sites sustained WH transformation efforts, recognizing WH as one strategy to support patients and employees. This response indicates cultural transformation is taking hold, with WH serving as a promising approach for promoting wellbeing among patients and employees alike.
Keywords
Background
Since the Institute of Medicine’s seminal 2001 Crossing the Quality Chasm report, 1 healthcare systems across the United States have sought new approaches to delivering integrated, patient-centered health care while reducing costs. Examples include primary care transformations to patient-centered medical homes2,3 and integrated primary care behavioral health.4,5 This call to change service delivery models to achieve more ‘people-centered’ health care was reiterated more recently in the World Health Organization’s 2016 Working for Health and Growth report 6 yet problems with high cost, variable quality, and lack of patient-centeredness persist,7,8 while healthcare provider stress and burnout have grown. 9 The SARS-CoV-2 pandemic has further amplified a critical need for healthcare systems to systematically address healthcare worker wellbeing alongside the needs of patients. 10
Since 2017, the Veterans Health Administration (VHA), the largest integrated healthcare system in the US, has been at the forefront of demonstrating a comprehensive new approach to care that seeks to address many of the well-documented shortcomings of traditional health care7,11,12 while being responsive to recent calls to promote wellbeing among patients 13 and employees. 14 Known as the Whole Health System (WHS) of care, this approach transforms the organization and culture of health care from a disease-driven model to a patient-centered, partnership model that empowers and equips people to take charge of their health and wellbeing 15 (see Figure 1). Guided by personal health plans, 16 this approach focuses on patients’ life mission, aspiration, and purpose (i.e., what matters most to the patient) as the foundation for health care delivery, putting patients’ goals at the center of care, in addition to treatment of disease. Complementary and integrative health therapies (e.g., acupuncture, yoga, tai chi) and self-care skill building classes in core areas (e.g., personal development, healthy eating, spirituality, and physical movement) are integrated into existing primary and specialty care services to help patients achieve and maintain health, while peer specialists and health coaches support patients as they identify and work towards their goals. Employees throughout the system are trained on how to deliver a patient-centered WH approach in clinical interactions. An additional key component of the WHS is a focus on providing wellbeing services for employees to address stress and burnout and support their engagement in self-care.

The Whole Health System.
Eighteen Veterans Administration Medical Centers (VAMCs) were selected to demonstrate WHS transformation and were given significant financial resources allocated by the Comprehensive Addiction and Recovery Act 17 and regional VA offices, along with instrumental implementation support provided by VA’s Office of Patient-Centered Care and Cultural Transformation (OPCC&CT), over a three-year period. Additional funds were earmarked for evaluating the effectiveness of the WHS and the transformation efforts at these 18 sites to learn from their experiences in preparation for WHS roll-out VA-wide. 18
Two years into this demonstration effort, at the start of 2020, the SARS-CoV-2 pandemic (hereafter called the ‘pandemic’) swept across the globe, creating the potential for substantial emotional distress for both healthcare workers19,20 and vulnerable patient populations such as Veterans. 21 By March 2020, healthcare systems across the United States including the VA, were required to quickly and significantly shift operations in response to the pandemic. As part of an ongoing evaluation of how the 18 sites approached WHS transformation, we had the opportunity to examine how an exogenous shock like a pandemic intersects with system transformation efforts when competing priorities associated with the pandemic were paramount. Here, we share lessons learned about the unexpected ways in which a WH approach intersected with the pandemic response at the 18 VAMC sites.
Methods
Study Design
We conducted qualitative telephone interviews with key informants at 18 VAMCs transforming their sites to a WHS model. These interviews were conducted as part of an ongoing multi-year, multi-component evaluation of Whole Health focused on transformation approaches, utilization of WH-aligned services, cost of system transformation, and impacts on patients and employees.15,18 They represented one set of periodic interviews conducted over the 3-year evaluation period. The early months of the pandemic in the United States coincided with planned site interviews; therefore, we used this interview period as an opportunity to inquire about how sites were responding to challenges arising from the pandemic and supporting their patients and employees. The VA Bedford Healthcare System’s Institutional Review Board determined this work was undertaken to inform VA operations as part of program evaluation and quality improvement activities.
Participants
Participants were VA employees (clinical and non-clinical) responsible for leading WH transformation efforts in each site who had previously participated in our ongoing evaluation interviews. These individuals were encouraged to invite other pertinent WH employees from their sites to join the interview.
Data Collection
Five study team members experienced in qualitative methods conducted interviews with each site in teams of two, using a semi-structured interview guide to direct the conversation. The guide included questions to ascertain how WH transformation had been affected by the pandemic, changes made to delivery of WH services, the prioritization of WH during the pandemic, ways in which the pandemic facilitated or hindered transformation, and use of WH to support patient and employee needs during the pandemic. Interviews lasted up to one hour, were audio-recorded, and transcribed verbatim. Participants provided verbal consent prior to participating.
Data Analysis
We conducted a directed content analysis 22 using a rapid analytic approach23–25 to understand both how the pandemic affected WH transformation efforts and the role of WH in sites’ responses to the pandemic. We started with a priori coding categories based on the components of the WHS model of care. Emergent categories captured additional content relevant to sites’ responses to the pandemic. Consistent with a rapid approach, team members reviewed interview notes and transcripts and summarized information by category in a table to capture relevant content, sorted by site. We then synthesized the information across these individual summaries in each category, using constant comparison, to understand how the 18 sites adapted WH transformation efforts and used WH as part of their pandemic response.
Results
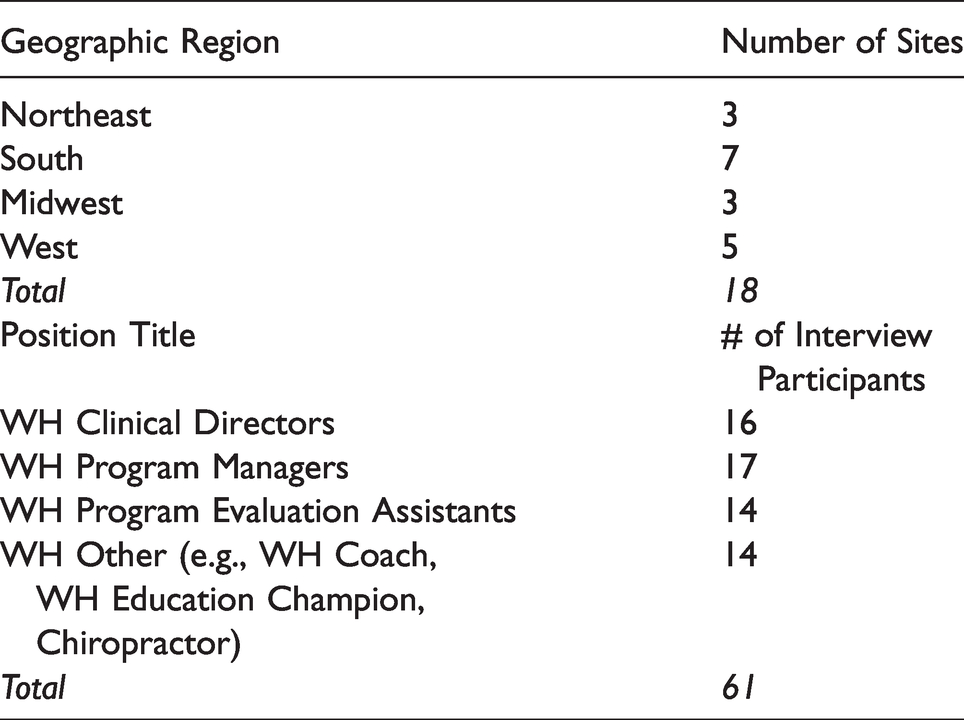
A total of 61 key informants participated in the 18 interviews, with two to nine people participating from each site. Participants comprised employees involved with WHS transformation at each site, including WH clinical directors, program managers, evaluation assistants, peer partners, administrative officers, education champions, health coaches, and complementary and integrative health practitioners. See Table 1 for site and participant details.
Site Location and Participant Role.
We found that the pandemic intersected with WHS transformation efforts in several important ways: (1) transformation efforts and WH service provision were initially hindered by the pandemic; (2) many sites simultaneously embraced a WH approach to engage and support patients during this time; (3) sites addressed concerns of the pandemic’s impact on employee wellness by offering an extensive variety of employee WH activities that were both solicited and endorsed by hospital leadership; and (4) two key changes catalyzed by the pandemic facilitated these efforts - the surge in the acceptance and use of technology to offer healthcare services virtually (i.e., telehealth) and the innovative delivery of complementary and integrative therapies through telehealth modalities.
Impact of the Pandemic on Transformation
Participants across all sites reported that early pandemic-related restrictions on in-person meetings and rapidly changing guidance initially slowed WH implementation efforts. In-person WH services were canceled, and many WH employees were pulled away from their transformation duties and detailed to other areas of the hospital to address pressing pandemic-related needs (e.g., patient and employee screening). These changes initially curtailed transformation efforts and the provision of WH services and seemed to have a greater impact on smaller hospital systems and sites with fewer WH employees. After this initial curtailing, many sites reported shifting to online provision of many WHS components, including health coaching, CIH therapies, and self-care skill-building classes. Some sites were able to rely on existing remote delivery infrastructure, while others had to develop infrastructure before they could continue offering WH services to patients. “Well, I would say overall, we have been dramatically affected by COVID-19 precautions… one of the first actions that occurred was cancellation of all groups… (…) I would say roughly 65 to 70 percent of our services are in groups, so that was a pretty big hit. We really weren’t, unfortunately, doing very much with regard to telephone or [virtual visits] at all previously, (…) when I compare us to some of our other sites (…) who, you know, maybe were more rural and were already offering [virtual] services and kind of just ramped that up. We had zero in place. (…). So, I think our first, I would say, three to four weeks actually were spent mostly dealing with the administrative burden of canceling groups, and then for individual services, migrating them over from face-to-face to virtual care.” [Site 14, Whole Health Clinical Director] “Also, I will just tell you we got a pat on the back, because (…) Whole Health is willing to roll their sleeves up and to participate, and because of that, it opened that door for better integration, you know.” [Site 12, WH Partner Lead]
The Whole Health Approach and Support of Patients During the COVID-19 Pandemic
As the pandemic progressed, the wellbeing of patients was paramount for sites. Efforts to support patients included widespread use of “check-in” calls, also described as “wellness” and “compassion” calls. Across most sites, a range of WH employees including coaches, peer specialists, and clinicians, reached out to thousands of patients to inquire about their wellbeing. These calls took a distinctly WH approach, seeking to understand patient needs and inquiring about their support systems at home, food security, ability to obtain needed medication, and levels of stress and anxiety. During these calls, WH employees discussed with patients the ways CIH therapies (e.g., yoga, mindfulness meditation) could help relieve stress and emphasized the importance of self-care; they also connected patients to innovative remote WH offerings (described below) as well as other services for which patients expressed a need (e.g., primary care, cardiology). For example, as one participant described: “You know, checking in. Are they connecting with people? Are they feeling isolated? Are they moving their body? (…) What are their surroundings like? Are they lacking food? And then being able to connect them to the resources that they needed was invaluable. Especially if folks were saying, you know, “I need my medications, what do I do now?” or “I'm feeling sick, what am I supposed to do?”, and being able to connect them with that care.” [Site 18, Whole Health Program Manager]

Whole Health Circle of Health.
Participants reported that most patients were appreciative of these calls and remarked on the relevance of the WH approach, noting how this approach acknowledged the isolation and anxiety many patients experienced during the pandemic. The outreach calls were so successful that some sites planned to continue them beyond the pandemic time frame.
The Whole Health Approach and Support of Healthcare Employees During the COVID-19 Pandemic
A surge in sick and highly vulnerable patients coupled with high risk of virus transmission created substantial new physical and mental stressors for all VA employees including clinical and non-clinical providers and support staff. At many sites, executive leadership (e.g., medical center directors) and service-level leadership (e.g., mental health directors) rapidly recognized that WH activities were well suited to address stress, elevating their perceived value of WH. At these sites, leadership actively solicited WH activities for employees and endorsed them by beginning highly attended all-staff meetings with mindful moments and discussing their relevance for combatting stress and anxiety. "They (leadership) have fully embraced it (Whole Health). You can see that they put something about Whole Health and self-care in (…) daily newsletters for employees - they have something there always about Whole Health on self-care and in all the emails and the Town Halls …" [Site 13, Whole Health Clinical Director] “[Employee Whole Health] has always just been given lip service in the past. People think it's a big deal, okay we have a couple programs, but truthfully what we're seeing now is people really wanting to understand how to manage their fear, their anxiety, their stress, you know.” [Site 8, Whole Health Clinical Director] “(…) the first direction [from leadership] was [to provide] employee Whole Health help. Our people are anxious, they're very scared, they're very nervous. So we (…) partnered with mental health and the chaplain service to do this (…) and the employee assistance program. We sent out a big message to employees saying, “Hey, Whole Health is here for health and wellbeing” because that's really important. And if you need more than that, then mental health can assist with psychological first aid and if you want spiritual support, the chaplain service is here. And if you really need more help than that because some of our staff were, you know, just really afraid, then we recommend and EAP (Employee Assistance Program) for therapy…” [Site 1, Whole Health Clinical Director]
Finally, in addition to offering a variety of CIH therapies, greater attention was given to creating onsite healing environments for employees to have places to de-stress and recharge when needed. “…we’ve created two spaces just like a break room, it’s more than a break room. We’re calling it the Employee Wellness and Respite Centers and so it’s two spaces, one on each campus that folks can come in and we’ve got nice comfy chairs in there, footrests, the lights are dimmed. We’ve got soft lighting and even some of the salt lamps in there, a space with a small table that people can do some coloring if they wanted to. They’ve got aromatherapy in there, ambient music, nature scenes up on the screens…it’s open 24 hours a day.” [Site 4, Whole Health Program Manager]
Catalysts for the Use of WH Approaches During the Pandemic
We found that two key changes catalyzed by the pandemic helped to facilitate the use of WH approaches during this time.
Surge in Use and Acceptance of Telehealth – Soon after the pandemic began, routine healthcare delivery in the VA had to either halt or shift to being offered virtually, increasing the use of telehealth for all types of care. Many participants reported that in their sites, the use of telehealth (e.g., real-time video platforms, telephone) for WH approaches such as CIH and coaching also surged at this time and was essential for being able to offer WH support for patients and employees during the pandemic. However, smaller hospital systems, and those with relatively small WH teams found it more challenging to make a quick pivot from face-to-face care to telehealth. Many interviewees also noted that attitudinal (both patients and employees) and administrative barriers they had encountered when previously trying to develop and promote WH telehealth services were rapidly removed and addressed. These included restrictions on approved virtual technology platforms and the need to address privacy concerns. Employees and patients were rapidly trained on the use of various virtual technology platforms, and many began to make more use of traditional conference and one-on-one phone calls, too. “Before we were basically a face-to-face program and now, you know, we've really expanded our whole virtual presence. Which we just never had the time to do or the support, frankly, and there's been so much support and so many tutorials on how to use this stuff (…) it was really, I felt, a struggle before.” [Site 16, WH Clinical Director]
Innovative Delivery of Complementary and Integrative Health Therapies – Facilities also adapted several CIH therapies that, at first glance, may not seem amenable to being delivered through telehealth. At many sites, practitioners creatively adapted massage, acupuncture, chiropractic, and biofeedback services to virtual formats adjusting these traditionally ‘hands-on’ approaches to ones that could be carried out remotely to continue to address patients’ physical issues. One WH Administrative Support Staff noted that it, "is very surprising that we have Veterans that are asking for it (telehealth massage). That are asking to show them how to do self-care. And so (the massage therapist) is actually filling up with (virtual visits).” [Site 1] As the quote below indicates, at least some patients were quite satisfied with this mode of care: “Biofeedback, I'll just say, is also one that's not real conducive to virtual but they found it works really well (…) if the patient has had at least one face-to-face visit. (…) In fact, one of our psychologists that does biofeedback in (X city) had a great compliment [from a patient] yesterday. (…) it was something like, ‘This has been tremendous, it's been life-changing, you're a godsend.’” [Site 1, WH Clinical Director] “So, the physical therapist on our team said, “Well, take your computer, the laptop, and walk me up to your sewing room and show me what you’re doing.” So, this lady, this was (…) semi mass-producing these things. (…) this was very healing for her. And so, the therapist (…) had the patient go through each station as if she was doing that activity and was able to make some small tweaks ergonomically, and you know, at the end of it, the patient said, ‘Well, you know, I’m not having the pain with this modification that I was the way I was doing it.’ (…) I think using virtual technology has really opened the doors to remove space and time as a barrier.” [Site 11, Chiropractic Supervisor]
Discussion
Like other healthcare systems, the VA faced great challenges to providing health and wellbeing services to patients and employees during the pandemic. Our findings show that as VA sites working towards WHS transformation rapidly pivoted to address pandemic-related challenges, instead of setting aside their WH work, they largely embraced it as a mechanism through which to support the wellbeing of patients and employees. This may evidence maturity in sites’ transformation efforts. When faced with a crisis, sites recognized the WH approach they had been working towards and leaned into Whole Health rather than retreating to former processes and practices. This finding indicates that transformation is taking hold and sites are indeed moving towards a new model of care. Further, by aligning transformation with crisis-related needs, these organizations ensured progress even when immediate priorities temporarily lay elsewhere.
Even prior to the pandemic, healthcare institutions were becoming increasingly focused on promoting stress and burnout reduction techniques for their employees26,27 as a way to improve overall health and engagement in their work. The pandemic quickly created an environment that stoked fear among employees, amplifying their feelings of stress, anxiety, and isolation,19,28 and highlighting the need for healthcare organizations to develop a “proactive, comprehensive wellness strategy” for their employees. 10 Similarly, the general public also faced significant stress and uncertainty during the pandemic29,30 with Veterans in particular facing a high risk of increased anxiety and stress due to pre-existing trauma31–34 and greater economic insecurity. 35 Given the inherent alignment between the principles of WH and the needs of Veterans and employees whose lives had been deeply affected by the pandemic, sites in our study found that the pandemic presented a unique opportunity to showcase the value of a proactive WH approach to care. By turning towards WH, sites demonstrated the enormous potential of this approach to promote wellbeing and address stress among patients and employees during unprecedented times. The need for an approach such as this may be even more pertinent now given that recent studies have shown a marked increase in substance use among the US adults during the pandemic,36,37 including among health care workers. 38 As calls urgently grow for healthcare systems to address employee burnout, the VHA’s WH model provides a system-wide example of how healthcare organizations can attend to employee wellbeing while simultaneously transforming the delivery system.
In practical terms, sites’ use of the WH approach to support its patients and employees during the pandemic was facilitated by the surge in acceptance and use of telehealth 39 and the creative adaptations of numerous CIH therapies to virtual formats. While long-term shifts in payment and other policies are still needed, high levels of telehealth utilization are expected to be sustained post-pandemic.40,41 In this environment, it is likely that many of the ideas for how to better deliver WH that were inspired by COVID-related restrictions and concerns will persist beyond the pandemic as sites continue to provide virtual as well as in-person health and wellbeing services for patients and employees. It is unclear what the balance of in-person versus telehealth offerings will be in each facility but the decision will most certainly be impacted by staffing levels (i.e., having enough staff to offer multiple format options) and perceptions of the most appropriate and effective modality for delivering each type of service. For example, while video platforms may be useful for sustaining engagement in hands-on therapies such as chiropractic, acupuncture, and massage when in-person treatment options are not available, their effectiveness is unknown. The perceived greater effectiveness of in-person treatments will likely cause a shift away from the virtual towards in-person offerings once they become available. However, the comparative effectiveness of something like virtual meditation may be perceived as just as appropriate and effective as in-person meditation, leading to more virtual options being offered.
This study has several limitations. First, we chose to use a rapid analysis approach which, while having been shown to generate timely and valid findings, also has tradeoffs including limiting our ability to produce complex and nuanced interpretations of the data. 42 Second, the observations were limited to one moment in time early in the pandemic and to a limited number of medical centers across the large VHA network of facilities. They also represent the perceptions of employees leading WH transformation efforts only. We do not know, for example, the extent to which these services and spaces were utilized nor how they may have been maintained hygienically or added to the burden of some employees during the pandemic (e.g. respite rooms may increase housekeeping staff workload). Research on the perceptions of other healthcare employees at these facilities and patients would add important insight into the value of a using a Whole Health approach to support patients and employees during the SARS-CoV-2 pandemic.
Conclusion
Nevertheless, this study provides a unique view of a healthcare system facing a crisis while undergoing large scale transformation to a new model of care. A WH approach to health care, which recognizes health and wellness as being comprised of many aspects of a person’s life, was perceived to be valuable for patients and employees working in healthcare systems that are stressed and caring for people who are anxious and unable to access usual care. The unprecedented shock of SARS-CoV-2 did not significantly derail the work of transformation and, in fact, sparked creative thinking and development of new ways to apply this approach while demonstrating its value to leadership and staff. As the US healthcare system continues to seek ways to improve patient care, VHA’s WHS model exemplifies an approach that can support the wellbeing of patients and employees alike even in the face of crisis.
Footnotes
Disclaimer
The views in this paper are the views of the authors and do not represent the views of the Department of Veterans Affairs or the United States Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding provided by the Department of Veterans Affairs, Office of Patient-Centered Care and Cultural Transformation, and Quality Enhancement Research Initiative [PEC 13-001].