
Abstract
Background
Cancer remains a leading chronic disease in the United States with a high burden of disease and challenging treatment protocol. Nutrition is critically linked to long-term health outcomes and recovery rates among cancer patients, but there remains a persistent gap in clinician training regarding functional nutrition. This study interviews patients to understand their experiences of nutrition support they received while in cancer treatment.
Objectives
Understand patient experiences and needs regarding cancer treatment (i.e., surgery, chemotherapy, radiation, and/or immunotherapy) and available nutrition counseling.
Methods
This was a multi-phase study incorporating survey data (n = 50) and follow-up, semi-structured interviews (n = 20) of cancer patients in the Mid-Atlantic United States. Interview participants included those undergoing active cancer treatment (n = 7) and those in remission at the time of contact (n = 13). Participants shared their experiences receiving treatment and their perspectives regarding the quality of care they received in outpatient oncology clinics. Central to this study was a discussion regarding the quality of nutrition counseling they received while in treatment.
Results
Five themes emerged through data collection and analysis: (1) patients need additional education regarding nutrition, (2) personalized resources are not readily available, (3) perceptions from patients that oncologists receive little formal nutrition training related to cancer, (4) oncologists’ attitude toward nutrition may influence patient care, and (5) patients seek nutrition information through informal sources. Commonly, patients had little access to licensed dieticians or other professionals capable of providing lifestyle recommendations.
Conclusions
The results of this study are being used to develop a clinician toolbox of resources, recommendations, and services that can be shared with patients seeking additional information regarding nutrition and diet change.
Introduction
Cancer remains a leading chronic disease in the United States, with approximately 1.9 million new diagnoses and 600 000 deaths annually. 1 According to the American Cancer Society, approximately 18% of all new cancer diagnoses and 16% of all cancer deaths are directly related to lifestyle factors, including poor nutrition. 2 For this reason, it is vital that cancer patients receive appropriate nutritional support from entire care teams during and after treatment to not only improve their quality of life, but also their treatment outcomes.3,4 Nutritional support in medical care is a crucial element of patient-centered care, an approach to treatment that empowers and enables patients to participate in shared decision-making and self-management. 5 Although patient-centered care has been implemented in many medical practices, nutritional support is still insufficiently integrated in cancer care. This practice gap persists despite evidence of nutrition improving patient-reported and clinical outcomes. 6
Cancer tumors affect patients’ resting energy expenditure and metabolism from agents produced by the cancerous tumor directly, as well as the body’s systemic response to the tumor. 7 These agents may be responsible for malnutrition and/or cachexia, a condition causing weight loss and weakness.7,8 Common cancer treatments like radiation and chemotherapy also induce taste changes and gastrointestinal symptoms that may lower patients’ appetites and directly damage healthy tissues. This, in turn, may result in malnutrition or the intensification of existing malnutrition.3,8–10
Of all hospitalized patients, cancer patients have the highest prevalence of malnutrition; according to large European surveys, 30%-50% of cancer patients are at risk of malnutrition. 11 Cancer-related malnutrition not only impairs the quality of life for cancer patients, but also causes shorter survival rates. 12 When cancer patients are malnourished, they experience faster infection rates, increased risk of postoperative complications, reduced tolerance and response to treatment due to increased toxicity, poorer adherence to treatment, and cognitive impairment. 13 Additionally, the severity of malnutrition has been found to be an independent predictor of shorter survival for patients with advanced cancer. 14 Malnutrition is also known to decrease the effectiveness of cancer treatments, further implicating the need for nutritional care and support in cancer treatment models. 15
In addition to the issues related with malnutrition and cachexia for patients during treatment, general attention to diet is important for all cancer patients, even those who are not at high risk for malnutrition. For example, while breast cancer patients are not typically at risk for malnutrition, emerging research suggests that increased adiposity may be associated with greater risk of mortality. 16 Additionally, research suggests that moderate weight loss and appropriate nutrition management can reduce the risk of all-cause mortality and cancer reoccurrence among breast cancer patients.17,18 In other words, nutrition counseling during and after treatment is critical for patients to ensure long-term quality of life and disease management.
Although the need for adequate nutritional interventions in cancer has been stressed for years, oncologists’ understanding of the nutritional status of their cancer patients remains scarce. 5 According to current clinical guidelines, the diagnosis of malnutrition occurs later and less frequently in clinical practice than recommended.19,20 Sufficient patient-centered care should include the multidisciplinary approach of involving nutritionists and dieticians in cancer care paradigms to directly improve cancer patient health outcomes and survivability.
Research Questions
An extensive review of the existing scholarly literature demonstrates several significant knowledge gaps regarding nutrition knowledge among cancer patients and counseling from trained oncologists. The following research questions have been developed in response to these gaps: 1. How do cancer patients understand the role nutrition plays in managing their health conditions? 2. Where do patients receive nutrition-related information? 3. How do patients describe the counseling they receive from their oncologists related to nutrition? 4. How do oncologists describe their understanding of nutrition’s relationship to cancer outcomes? 5. How do oncologists provide nutrition counseling to their patients specifically related to their cancer treatment?
Materials and Methods
This study is the first phase of a larger project designed to develop nutrition educational programming and interventions for oncologists. This initial study sought perspectives from patients with a history of out-patient cancer care through chemotherapy, radiation, and/or immunotherapy. Data collection from this study identified five primary concerns of patients related to diet over the course of their care and will be used to inform the second phase of this study, data collection from clinical oncologists. This study received approval from George Washington University’s Institutional Review Board (NCR224709).
Recruitment and Participants
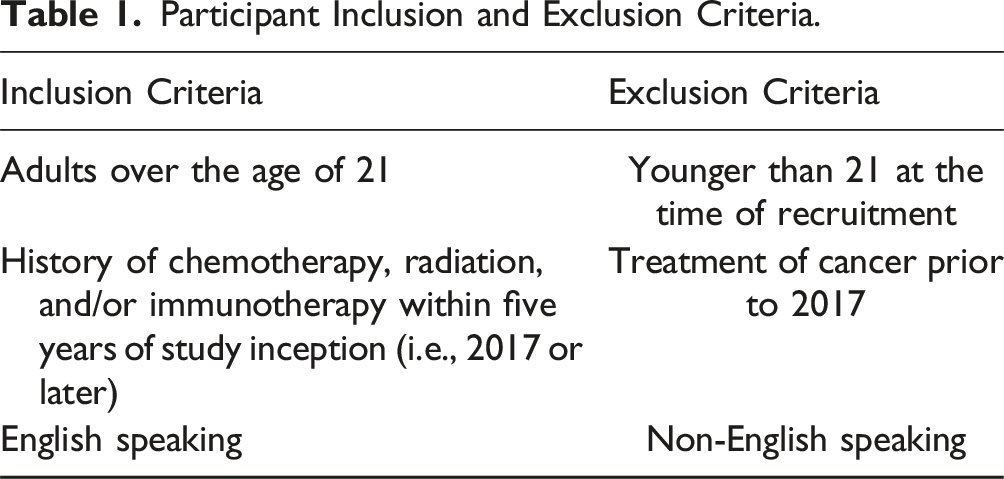
Participant Inclusion and Exclusion Criteria.
Participant Remuneration
All individuals who completed an interview were given a $20 Visa gift card in recognition of their time and labor in supporting this study. Participants did not receive any form of payment for completing the initial questionnaire. Participant remuneration is a complicated issue with a long history of discussion and disagreement in the research community, particularly due to concerns over coercion and fairness. 22 It was important for us to provide remuneration for our participants as it showed respect for the time and expertise of our participants and aligned with our understanding of justice in research ethics. 22
Instruments and Methods of Data Collection
This study utilized data collection instruments consistent with inductive qualitative research. Participants initially completed a questionnaire to ensure eligibility and to capture patients’ personal characteristics, their experiences through care, and their perceptions of their oncologists’ nutrition knowledge. Questionnaires in health research are common and can be useful but they are often misused and are not wholly appropriate for all research questions.22,23 Given the subjective nature of our research questions, we elected to follow the questionnaire with optional, semi-structured interviews. Data was collected between December 2022 and May 2023. We conducted an initial questionnaire (n = 50) followed by individual interviews (n = 20) of individuals with a history of cancer.
Initial Questionnaire
Initial Questionnaire Results, Likert Questions (n = 50).

Individual Interviews
Initial Questionnaire Results, Continued (n = 50).

Interview Participant Self-Reported Demographics (n = 20).

Credibility, Trustworthiness, and Rigor in Qualitative Research
To establish rigor and ensure methodologically sound results, we incorporated multiple safeguards into the research process. First, we pursued a two-phase process of peer debriefing and member checking. In peer debriefing, we engaged two external qualitative researchers to discuss our process of data analysis, review initial codes, and discuss the process of thematic analysis. By engaging external methodologists, this study introduced a layer of independent review that ensured more critical reflection on our behalf. Next, we ensured intercoder reliability by independently coding data and coming together to discuss agreements, disagreements, and to clarify emerging questions. 29 The next process, that of member checking invited all participants to review transcripts of their interviews to ensure that their language and experiences were accurately captured prior to data analysis. We further invited participants to review an early draft of our findings to ensure that our personal assumption did not influence our findings over the perceptions of participants. Furthermore, the data was carefully triangulated; the initial questionnaire data was reviewed against results from the semi-structured interviews, and we consistently returned literature to identify alignment, or deviation, from previous work in cancer nutrition. Throughout this process we maintained a clear audit trail of the work, including detailed memos to ensure the timeline of the study was well established and to capture decision points related to the study.
Data Analysis and Results
Data analysis occurred concurrent with data collection, and we followed a process of inductive initial coding followed by thematic coding. 30 Upon the completion of initial coding, the senior researcher (PC) reviewed all transcripts for completion and consistency. Following this process, we conducted a series of meetings to review initial codes, manually sort them into relevant categories to identify relationships and used these categories to identify themes.
Ultimately, five themes emerged through data collection and analysis: (1) patients need additional education regarding nutrition, (2) personalized resources are not readily available, (3) oncologists receive little formal nutrition training related to cancer & patients identify this as a significant knowledge gap, (4) oncologists’ attitude toward nutrition may influence patient care, and (5) patients seek nutrition information through informal sources. While it did not rise to a level of thematic significance, four participants felt that their oncologists dismissed their concerns regarding lifestyle interventions and alternative methods of symptom management (i.e., non-pharmacologic management of side-effects).
Theme One: Patients Need Additional Education Regarding Nutrition
Data from the initial questionnaire affirms that most participants perceive themselves slightly more knowledgeable than the average person regarding general nutrition knowledge. Everyone who responded to the question considered themselves at least as knowledgeable as the general population, with nobody selecting “slightly less knowledgeable” or “Not at all knowledgeable.” Figure 1 represents self-reported nutrition knowledge. Nutrition knowledge survey results.
Despite the common confidence in nutritional knowledge, participants consistently cited a desire for more education from their healthcare providers that was specific to their treatment protocol and disease type. Instead, participants were consistently provided with guidance to either eat a lot to increase their overall energy intake or otherwise to “exercise more, eat less.” The nuance that multiple participants expressed was that they wanted nutritional recommendations specific to their course of treatment and the treatment side-effects that they were experiencing. One participant specifically noted how they expected a greater focus on nutrition from their oncology team to improve her overall quality of life. I wish that nutrition education and a really healthy diet plan was actually part of my treatment. I think that it would give cancer patients something else they could be in control of. And it could also make them feel better… the goal of cancer treatment is to… give you more quality years and we’re missing out on this big piece by not [getting] nutrition counseling that that matters (Chele).
Interestingly, many participants could not tell us where they received their nutritional knowledge. They cited a friend, spouse, or lessons they learned through their childhood; none of our participants had formal education in nutrition. Two mentioned employing intuitive cooking, as described by Bee: …I think I know just from cooking for years. I think I know intuitively how to cook some things. So, if I'm making rice and it’s the third or fourth day of the week I’ve made rice, I just kind of know how to add veggies to it or I kind of know what would be good with rice. So, some of it is just the experience of cooking (Bee).
Participants felt generally informed about nutrition but wanted a more holistic and tailored approach considering their specific needs. Multiple participants identified feeling overwhelmed at the amount of information to navigate in addition to physical and emotional exhaustion. These participants said they wanted to know exactly which varieties of food to eat, how often to eat, and what foods might positively impact their conditions. Participants wanted information that would make their course of treatment easier, while recognizing that they were experiencing significant personal stress. In other words, cancer patients want guidance from their medical team that has room for some personalization based on personal preference.
Theme Two: Personalized Resources are Not Readily Available
Only half of participants—even among those who had access to nutritionists during treatment—felt they had individualized recommendations in their care plans. Those who did feel they had individualized nutrition advice were often receiving care at large, well-funded institutions with a multidisciplinary team who had access to their existing medical records. In other words, these patients had access to comprehensive healthcare systems that are not accessible by all.
Some patients received personalized nutrition resources through their involvement with large clinical trials; two of whom participants in studies through the National Institutes of Health (NIH). Despite access to personalized nutrition, both patients reported seeking additional contextual information and wanting more specific information about the food they were recommended. One participant discussed her experience seeking treatment at a major, internationally recognized center of excellence in cancer care. Even in this state-of-the-art facility, the information was impersonal and delivered as part of a larger packet of resources. they [the oncologist office staff] give you this big folder and it’s like, here’s a business card for the dietician and here’s a business card for a social worker… but it wasn’t like, “we have a class I want you to go to…” So, it seemed like just a small part of the whole treatment of the diet, the dietary part (Bee).
Nine of our participants were higher income earners (>$125,000 annually) and supplemented their treatment through their social network (e.g., multiple participants had friends who are physicians who advised on nutrition during treatment), through other fee-for-service healthcare providers who could provide personalized recommendations, or through bespoke food delivery services. One participant credited her lack of adverse treatment symptoms to nutrition advice she received from her holistic chiropractor. The chiropractor recommended many leafy greens, Brussels sprouts, and kale to specifically combat the adverse effects of chemotherapy. … my husband ended up purchasing a Vitamix… But I did a lot of juicing [with] heavy greens and fruit smoothies… and [it was] probably the best nutrition of my life during my year of treatment for cancer. Because I just really felt like my body was being depleted because of the conventional treatment [chemotherapy]… (Monica).
Monica elaborated further that “… outside of some fatigue, I felt really good the year of my cancer treatment. And I do think that the nutritional way that I was handling it had a big impact on that.” She also noted her oncologist did not provide her with nutritional guidance other than to “eat a regular healthy diet.” A common concern among participants was that personalized nutrition during cancer treatments comes at a financial cost and often requires a network to leverage diet. Not all participants had that level of financial flexibility. One participant discussed his ongoing difficulty in accessing the type of food that he was recommended in treatment. it’s a bit of a challenge, because my oncologist can suggest a certain food … But, you know, currently my family is not really that well off. So, we have some financial problems to accessing some specific foods that I'm recommended to take (Mikey).
This experience is common among cancer patients who do not have disposable income or similar access to health resources as those with a higher income. Given the diversity of people who are experiencing cancer and the varying level of resources available to individuals, it is important for clinical teams to identify resources and recommendations that can support the complex needs of such a heterogenous population.
Among the patients who did receive nutritional guidance, many felt their physicians lacked personal attention. One such patient, Bee, described her physician’s recommendations as being broad and not particularly helpful. … [the care team] never said anything really firm [about nutrition]. [The advice has] always been, you know, you should eat more vegetables. Well, I don’t eat very much meat… and [they’re] like, you should exercise. Okay. I exercise every day. So, I never felt it was a very in-depth thing (Bee).
The same interviewee also summarized the feeling of several participants in saying that while she was provided a nutritionist as a resource, “it seemed like just a small part of the whole treatment” (Bee).
Another interviewee reported similar frustration and experience with broad advice and lack of personal attention placed in her patient notes. They’re not asking, they’re just saying, eat a healthy, well-balanced diet, Mediterranean being the best… get away from processed foods and watch that alcohol consumption. And that’s just like standard verbiage at the end of the MyChart report. (Betsy)
Though her care team advised a Mediterranean diet as the best nutritional option, she wanted more concrete guidance tailored to her needs, her treatment, and her active lifestyle that requires she maintain muscle strength. The interviewee did note, however, that her oncologist was knowledgeable about alcohol consumption. This physician encouraged her to eliminate hard liquor, recommended a pinot noir for the resveratrol benefits, and counseled the patient to limit herself to four ounces of wine a day.
Theme Three: Perceptions From Patients that Oncologists Receive Little Formal Nutrition Training Related to Cancer
An important aspect of patient-centered care is the utilization of multidisciplinary teams as well as an awareness of other determinants of health and wellness beyond the traditional disease-focused model of care. 5 While comprehensive whole-person care is multifactorial and requires consideration of many factors, nutrition is foundational for many of the patients in this study.
A disproportionate number of questionnaire participants indicated that they were rarely asked (n = 15) or never asked (n = 18) about their dietary habits by their oncologist. Most participants felt that their oncologist was only somewhat prepared in addressing their nutrition concerns (n = 15). From the data, it can be inferred that this significant knowledge gap is of concern for cancer patients. Most participants (74%) rated nutrition during their cancer treatment as extremely important (n = 14; 28%) or very important (n = 23; 46%). The significant difference between patient perceptions of the importance of nutritional information and patient perceptions of the nutritional care and knowledge of their oncologists is highlighted in Figures 2-4. Frequency of nutrition counseling with oncologists. Patient perception of oncologists’ nutrition knowledge. Patient perception regarding the importance of nutrition in treatment.


Multiple participants in our interviews also described the need for improved nutritional support from their oncologists. The message from Nick highlights both his perception of this importance as well as his current misunderstanding of nutrition. If there were any way that the medical profession[al] could give more detailed guidance, not on the foods to eat, but more on the moderation required for all of the foods and the things to monitor on the food pyramid is woefully pitiful (Nick).
This understanding of healthy nutrition aligning with the food pyramid suggests that the average patients’ knowledge of nutrition is not necessarily current. Another participant expressed their knowledge about medical school curricula and described the inadequacy of nutrition training: “They [oncologists] don’t get much nutrition in school. They get… they just basically get a three- or four-hour lecture and that’s it. (Betsy)”
These patient perspectives on the nutrition knowledge gap of their oncologists are important and highlight the need for improved nutrition training related to cancer. Oncologist recommendations are extremely influential in patients’ decision-making processes. With inadequate oncologist knowledge on nutrition, patients may not make the appropriate dietary choices for optimal cancer care.
Theme Four: Oncologists Attitude Toward Nutrition May Influence Patient Care
Participants highlighted the attitudes of their oncologists when faced with questions about nutrition. Specifically, a third of participants felt as if their oncologists deprioritized nutrition in their recommendations. This experience varied from participant to participant, with some patients discussing their oncologists’ goals of keeping their calorie intake high, while other were encouraged to eat less. Debbie specifically noted that her oncologist was more concerned that she was eating at all while disregarding the quality of food. “You know, a lot of physicians don’t really want to talk about that stuff [nutrition]. I mean, they just want you to eat, and I get that. Like they just want you to eat” (Debbie).
Patients even described certain negative attitudes displayed by oncologists when asked about nutrition that would align with their lifestyles. One participant discussed the challenge they faced in receiving guidance appropriate for their veganism. I really try to, you know, stick to a vegan diet. And they [the cancer care team] kind of rolled their eyes and laughed at me and they’re like, “you know, do whatever you need to do if that makes you happy (Debbie).
Other participants noted that their oncologists recommended that they should “eat less, exercise more.” Many participants described this advice as having little utility to their general nutritional knowledge which they deemed important. For example, Bee stressed that they only received scant information about nutrition and exercise. “She [the oncologist] just kind of said get enough sleep, get enough nutrition… it was always sleep, nutrition, … and exercise. She always said those three things in kind of a generic way” (Bee).
Oncologists are influential in their patients’ behavior, care adherence, and attitudes. 31 Various forms of oncologist communication and characteristics, like their attitudes toward nutrition, have significant effects on patients. 31 The same participants who detailed the lack of specificity of their oncologists’ nutritional recommendations also felt confident about their generic recommendations.
These negative attitudes toward cancer patients’ dietary concerns may serve to be detrimental to patients’ cancer prognosis. With increased nutritional training in medical schools and oncology residencies, providers caring for patients with cancer may develop more positive attitudes towards the role of nutrition in cancer care paradigms. 32 This is vital for cancer patients to feel acknowledged and affirmed of their dietary habits, as it is known to play an influential part in their cancer treatment and prognosis. 32
Theme Five: Patients Seek Nutrition Information Through Informal Sources
Social media and the internet serve as potential sources for misinformation and disinformation about food science and nutrition. 33 As food content has been increasingly popular on the internet, popular social media channels have established audiences that trust their nutrition advice. These channels, often designed to promote certain content or products, can disseminate inaccurate or incomplete information. Oftentimes, this content is promoted by various celebrities, “influencers,” and self-proclaimed experts. 33 This risk makes the provision of nutrition information by knowledgeable healthcare providers ever more important.
Participants who completed the questionnaire indicated that they often received information related to nutrition from the internet while undergoing cancer treatment (n = 23; 46%). Many received nutrition information from their oncologist as well (n = 22; 44%) however, our interviews highlight the gaps in oncologists’ knowledge. Several participants felt that their oncologists were skilled providers, but they also felt that they frequently needed to seek nutritional information from the internet. Five participants noted their retrieval of nutritional information as occurring exclusively through social media channels. One of these participants even noticed the informality of retrieving nutritional information online. “On the internet I did a lot of research about my mutation… you know high dose vitamin C and [other vitamins] through intravenous, I started doing that. So, it was all basically hodgepodge together on my own” (Frankie). Oncologists can directly combat this potentially risky information retrieval by directly consulting patients about their nutritional needs while undergoing cancer treatment or providing appropriate and useful referrals to qualified nutritionists.
Discussion
This study was designed to identify the needs and dietary concerns of cancer patients to provide initial data to support the development of training initiatives for oncologists. The data collected suggests that nutrition is a critical area of interest for cancer patients and part of their overall treatment plan that does not receive as much attention as they would like. Participants noted that oncologists were helpful, but often did not have the knowledge base necessary to answer specific diet related questions and that the larger care team at their outpatient clinic (e.g., nutritionists, nurses) were often so overworked that it was difficult to schedule time or receive personalized recommendations. When this happens, patients were likely to seek support outside of their clinical site, often from people online or through expensive consultation services.
Importantly, our study including patients with diverse cancer diagnoses. For some individuals, malnutrition and cachexia are important concerns during treatment and can have a significant impact on disease management. For others, especially patients with a history of breast cancer, long-term nutrition planning may be critical to reduce risk of cancer reoccurance.17,18 In all cases, patients requested increased attention from the clinical teams regarding nutrition while undergoing treatment and after the completion of their therapies. Data from this study suggest that nutrition counseling should be included in treatment and incorporated in further follow-up appointments as part of further preventative care.
It is worth noting that it is infeasible for oncologists to provide comprehensive nutrition guidance or supersede the role of the oncologic nutritionist. Rather, we propose that the integration of appropriate and useful nutrition counseling must include multidisciplinary teaming and a multifaceted approach to care.34,35 Oncologists should work closely with nutritionists, nurses, and other health care professionals to provide comprehensive care that considers the multifactorial needs of their patients. That said, it is crucial that oncologists understand the immediate and long-term benefits of adequate nutrition on health outcomes.36,37 Participants in this study discussed how important diet was to their understanding of health and argued that their oncologists need additional training to answer their questions and make appropriate referrals. This is especially true in smaller, less resourced environments where dedicated nutritionists may not be readily available. This study affirms the important work that needs to be done in medical training and through continuing medical education (CME) courses to address these concerns. The next step in this study includes meeting with oncologists, discussing the results from this phase, and identifying specific training gaps and areas of interest to develop CME bearing courses or other educational material for clinicians.
This study was not without challenges and limitations that may impact the generalizable nature of our findings. First, our participant group was relatively heterogenous, representing various cancer diagnoses, treatment modalities, and geographic locations. This variety in participants may have influenced the type of treatment and treatment centers available to participants, their access to affordable resources including food and supplemental nutrition counseling, and varying levels of health literacy. On the other hand, sixteen of our interview participants have an annual income above $70,000. This income level allows many of our participants to seek resources that may not be available to others of lower income. Additionally, as this is the first phase of a larger study, it does not represent the perceptions and priorities of clinicians providing care. Without this data, the study presents a limited view of the concerns that emerge during treatment. In other words, this data represents issues that patients identify and does not consider the priorities and concerns of individuals delivering care. Lastly, because our recruitment primarily occurred using the NIH ResearchMatch program, it is likely that our participants represent a group of individuals who are familiar with medical research and invested in changing health care practice. With this participant pool, the voices and experiences of those who are not engaged in research are missed. Future research in this area should consider expanding the participant pool to include more diverse perspectives by searching for individuals through other avenues (e.g., community health clinics, academic medical centers, and other clinical spaces).
Conclusion
Cancer patients seem to appreciate the importance of good nutrition in managing their long-term health and desire more counseling from their clinicians. Many participants noted that their care teams in outpatient cancer clinics were not equipped to provide adequate nutrition counseling and that dieticians working in these settings were often overworked and unable to deliver tailored care. It is important to provide continued medical education to oncologists and others involved in caring for cancer patients. The next phase of this study seeks to explore the results from this qualitative research with oncologists to identify appropriate educational interventions (e.g., training courses, static resources, community resources) for delivery in outpatient cancer settings.
Footnotes
Acknowledgments
We wish to recognize the Emerging Scholars Fellowship and the office of the Associate Dean for Research at George Washington University’s School of Medicine and Health Sciences. This study would not be possible without the guidance of AA and members of the Collaborative for Health Education Evaluation, Research, and Scholarship (CHEERS).
Author Contributions
PC developed the concept for this study, led the development and writing of the manuscript, and trained the study personnel on qualitative data collection and analysis. NK supported the initial literature review and development of study protocol. WH refined study protocol and contributed significantly to the writing and editing of the thematic analysis section. All authors took part in data analysis and reviewed and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the “Emerging Scholars Fellowship,” a grant funded by the George Washington University’s School of Medicine and Health Sciences to provide mentorship and financial support to early-career faculty developing their research agenda. The grant funder had no role in the design of this study or the analysis of data.