
Abstract
Background
Mindfulness-based interventions (MBIs) are supported by clinical practice guidelines as effective non-pharmacologic interventions for common symptoms experienced by cancer patients, including anxiety, depression, and fatigue. However, the evidence predominately derives from White breast cancer survivors. Racial and ethnic minority patients have less access to integrative oncology care and worse cancer outcomes. To address these gaps, we designed and piloted a series of mindfulness-based group medical visits (MB-GMVs), embedded into comprehensive cancer care, for racially and ethnically diverse patients in cancer treatment.
Methods
As a quality improvement project, we launched a telehealth MB-GMV series for patients undergoing cancer treatment, delivered as four weekly 2-hour visits billable to insurance. Content was concordant with evidence-based guidelines and established MBIs and adapted to improve cultural relevance and fit (eg, access-centered, trauma-informed, with inclusive communication practices). Program structure was adapted to address barriers to participation, with ≥50% slots per series reserved for racial and ethnic minority patients. Intake surveys incorporated a demographic questionnaire and symptom assessments. Evaluations were sent following the visits.
Results
In our first ten cohorts (n = 78), 80% of referred patients enrolled. Participants were: 22% Asian, 14% Black, 17% Latino, 45% non-Latino White; 65% female; with a median age of 54 years (range 27-79); and 80% had metastatic cancer. Common baseline symptoms included lack of energy, difficulty sleeping, and worrying. Most patients (90%) attended ≥3 visits. On final evaluations, 87% patients rated the series as “excellent”; 81% “strongly agreed” that they liked the GMV format; and 92% would “definitely” recommend the series to others. Qualitative themes included empowerment and connectedness.
Conclusion
Telehealth GMVs are a feasible, acceptable, and financially sustainable model for increasing access to MBIs. Diverse patients in active cancer treatment were able to participate and reported high levels of satisfaction with this series that was tailored to center health equity and inclusion.
Keywords
Introduction
Psychological distress has profoundly negative impacts on patients undergoing cancer treatment, particularly for racial and ethnic minority patients facing structural inequities that lead to unmet healthcare needs. Psychological symptoms, along with associated fatigue and sleep disturbance, are frequently undertreated.1,2 Moreover, access to mental health services and treatment for depression is lower among Black, Latino, and Asian American patients compared to non-Latino White patients.3,4 Psychological distress, including symptoms of anxiety and depression, is an independent predictor of increased cancer-specific mortality in multiple cancer types, notably cervical, colorectal, pancreatic, and prostate cancer – which are all correlated with racial and ethnic disparities in survival outcomes.5-9 Psychological distress is also associated with lower quality of life, social isolation, higher healthcare costs, and poor treatment adherence– underscoring the importance of managing anxiety and depression during cancer treatment.10-12
Mindfulness-based interventions (MBIs) are recommended for symptoms of anxiety and depression in adults undergoing cancer treatment by the Society for Integrative Oncology-American Society of Clinical Oncology (SIO-ASCO). 13 Common MBIs in healthcare include mindfulness-based stress reduction (MBSR), mindfulness-based cancer recovery (MBCR) and Center for Mind-Body Medicine (CMBM) training.14-17 Many MBIs were designed for and researched among primarily White, racially homogenous populations, and critiqued for neglecting cultural and historic roots of meditation practices, lack of cultural sensitivity, and cultural appropriation.18,19 Implementing evidence-based MBIs could ameliorate undertreated symptoms among racial and ethnic minorities during cancer treatment, but key challenges need to be addressed. MBIs need to be adapted for feasibility and appropriateness during cancer treatment and for cultural relevance and acceptability among racially and ethnically diverse populations. Adapted MBIs need to be embedded as part of routine oncologic care to increase uptake, particularly for patients with limited economic resources and demanding treatment schedules. Patient-level barriers also need to be considered to support equitable access to MBIs. This should include personalized mind-body medicine (MBM), described by Mishra et al. as appropriate and effective application of MBM for patients of varying backgrounds, inclinations, and abilities. 20
Group medical visits (GMVs) are an established strategy to increase access to mindfulness and other nonpharmacologic approaches for symptom management, and provide extended time for multimodal care by addressing the time constraints of usual one-on-one visits. Documented benefits of GMVs with mindfulness and other integrative therapies include improved health outcomes, 21 increased self-efficacy, 22 improved quality of life,23-25 and lower emergency room visits.26,27 GMVs may also reduce social isolation,28-30 and social isolation has been correlated with increased cancer-specific mortality.31,32 GMVs improve access by providing coordinated care to multiple patients simultaneously, reducing wait time for visits and increasing efficiency for clinicians. The ability to bill insurance for guideline-concordant care makes GMVs a financially sustainable model for clinicians without burdening patients with out-of-pocket costs that are often high when accessing MBIs outside of clinical settings. Our prior quality improvement (QI) pilot documented the feasibility of GMVs for increasing access to integrative oncology during cancer treatment. 21 Notably, patients indicated a preference for being separated by phase of care (active treatment or survivorship) but not by diagnosis (ie, cancer type). However, like with our Being Present studies of remote-delivered MBIs designed for a similar cancer population,33,34 75% of patients in our prior GMV pilot identified as non-Latino White.
The primary objectives of this QI project are to assess the feasibility and acceptability of remote-delivered, mindfulness-based group medical visits (MB-GMVs) designed for racially and ethnically diverse patients in cancer treatment. We describe two equity-focused strategies: (1) content adaptations to improve cultural relevance and fit for a multicultural population of patients in active treatment, and (2) adaptations to program structure to address barriers to GMV participation. Because the MB-GMVs are conducted as a clinical service, the goal of assessing feasibility and acceptability is to improve the quality of clinical care for all patients in cancer treatment.
Methods
Setting and Context
We conducted this QI pilot at the University of California San Francisco (UCSF) Helen Diller Family Comprehensive Cancer Center (HDFCCC), an urban, quaternary healthcare system with multiple campuses. The UCSF HDFCCC catchment area is composed of the 25 counties in Northern California that surround the Greater San Francisco Bay Area. The racial and ethnic distribution of individuals in the UCSF HDFCCC catchment area is 40% Non-Latino White, 37% Latino, 17% Asian/Pacific Islander, 6% non-Latino Black, <1.0% Native American. Our interprofessional team includes expertise in oncology, mind-body medicine, clinical operations, and integrative health research. Authors KKM and CEA were core GMV facilitators; ML and SWC were among four guest clinicians who each co-facilitated one series. A QI approach was chosen with a goal to improve the quality of clinical care available to all patients in cancer treatment. Data, de-identified and gathered during clinical activities, met criteria for UCSF Institutional Review Board-exempt QI activities. We report project findings using established SQUIRE guidelines. 35
MB-GMV Structure
“Mindfulness Practices to Promote Health During Cancer Treatment” was designed as a 4-visit synchronous telehealth GMV series. Each weekly GMV was 2 hours (8 hours total). The GMVs were designed for counseling patients on MBIs; interactive time for participation, reflection, and questions; assessment of physical, mental, and social determinants of health as appropriate; and coordination of care. During the shared appointments, clinicians spent individual time with participants: this occurred both in individual breakout rooms and in front of the group, as allowable in the GMV setting. 36 Shared decision-making and patient preferences were foundational to prescribing mindfulness strategies.
Visits were facilitated by two clinicians (two physicians or a physician and a nurse or Advanced Practice Provider). In every series, at least one facilitator identified as Black, Indigenous, or Person of Color (BIPOC). The GMVs were supported by clinic staff, including a Practice Coordinator and Medical Assistants. In addition, a clinical research coordinator was present at each session to optimize workflows, observe, and take structured field notes. Providers billed insurance for all patients present per institutional and national coding and billing guidelines based on the appropriate level of medical Evaluation and Management codes.
Electronic medical record (EMR) note templates were created for efficient documentation and billing compliance. An After-Visit-Summary was provided in the EMR’s Patient Portal after each session with a recap of the session’s content and a personalized “prescription” for mindfulness practice, including links to relevant resources. All visits were conducted via telehealth due to the COVID pandemic and to prioritize access, eliminating the need for transportation and allowing flexibility to accommodate complex cancer treatment schedules and variable health status.
MB-GMV Content and Equity Focused Strategies for Diverse Patients in Active Cancer Treatment
Mindfulness-Based GMV: General Format and Focused Patient Care by Visit Week.

aEBMC: East Bay Meditation Center and Visions Inc.: https://eastbaymeditation.org/2022/03/agreements-for-multicultural-interactions/.
bChozen Bays: https://www.shambhala.com/mindfuleating/.
cMeta analysis: Tai Chi and Qigong for Cancer-related Symptoms and Quality of Life, Wayne et al, J Cancer.
Surviv. 2018 Apr;12 (2):256-267.
dPersonalized Mind-Body Medicine in Integrative Oncology, Mishra KK, The ASCO Post, May 10, 2023. https://ascopost.com/issues/may-10-2023/personalized-mind-body-medicine-in-integrative-oncology/Abbreviations: ACSM: American College of Sports Medicine (Moving Through Cancer), AICR: American Institute for Cancer Research (Blueprint to Beat Cancer), CMBM: Center for Mind-Body Medicine, NCI: National Cancer Institute (Eating Hints Before, During and After Cancer Treatment; Fatigue; Ways to Improve Sleep; Cancer Treatment-related Symptom Clusters), NCCN: National Comprehensive Cancer Network Supportive Care Guidelines (Distress, Cancer-related Fatigue, Pain and Anticipatory Nausea), ODPHP: US Department of Health and Human Services Office of Disease Prevention and Health Promotion (Move Your Way), WCRF: World Cancer Research Fund (International Cancer Prevention Recommendations).
Manualization of workflows and content delivery (including time allotments for each activity), along with shared note templates, enabled guest co-facilitator participation, minimizing training requirements while maintaining fidelity. The manual defines which elements were included in all cohorts and which were modifiable depending on participant needs and facilitator preferences.37,38
We tailored the MBI as a clinical service for patients in active cancer treatment by using a 4-session format and by including content on common cancer and treatment-associated symptoms, as well as mindfulness practices as evidence-based cancer risk-reduction strategies (eg, increasing activity), which still apply after a cancer diagnosis. In addition to prescribing daily meditation practice, we focused on micro-practices or “MBM snacks” 39 (eg, brief breathing techniques) for times of acute stress and mindful awareness in activities of daily life for when patients were short on energy or time. Emphasis was placed on meditation qualities of open awareness and friendliness vs concentration. As in our Being Present studies,33,34 we referred to the “body scan” as “body awareness meditation” because patients with cancer associate “body scan” with radiographic imaging, which may induce “scanxiety” (scan-provoked anxiety). Chair yoga was taught because it can be done in a range of settings without dedicated props and can be easily modified for physical limitations. For walking meditation, a seated alternative was also demonstrated, and qigong could be experienced as guided imagery. Prompts provided before movement exercises emphasized awareness, acceptance, and non-striving as mindfulness practices. For facilitated interaction, we focused on cultivating inner wisdom and self-efficacy: what the patient can do and experience now, rather than what they can no longer do or is out of their control. Facilitators were sensitive to social needs including food, housing, and income insecurities. Free resources for continued mindfulness practice were provided.
To support inclusivity in racially and ethnically diverse groups, we reviewed Communication Agreements for Multicultural Interactions at the beginning of each session. 40 Specific cultural origins of different meditative practices and harms of cultural appropriation were discussed. We addressed spirituality and alignment with individuals’ diverse religious contexts when introducing meditative practices. We included a range of practices and approaches from different cultural roots and encouraged patients to adapt MBIs based on their needs, sociocultural inclinations, spiritual/religious beliefs, and racial/ethnic backgrounds. For example, nature-based phrasing, a line from a Zen Buddhist meal chant, and saying grace in Judeo-Christian traditions were all access points into a mindful eating exercise. The facilitation teams, content, and resources shared reflected the diversity of the populations served. Because racially and ethnically diverse groups include patients for whom English is a second language, extra scheduling and technology support - including close captioning - was made available to reduce barriers to participation.
As an ongoing QI initiative, additional adaptations were made as the series evolved based on specific patient accessibility needs and feedback. For example, we offer trauma-informed meditation instructions. 41 We acknowledge that trauma is common: for individuals with a history of trauma, focusing on the breath may bring up fear or panic, rather than the feeling of calm typically associated with meditation practice. We use invitational language and endorse agency, including by offering alternatives to anchoring on the breath as an object of meditation and to taking a stationary, seated posture. Anticipating the possibility of hypervigilance, we say: “you can close your eyes, or you might choose to leave your eyes slightly open” and give a verbal cue before sounding the mindfulness bell. In individual consultations, we tailor recommendations and write referrals for additional support, as appropriate.
Providing practice options made the program more inclusive overall. Alternative focal points in lieu of concentrating on the breath were also helpful for patients with respiratory difficulties. The invitation to move during meditation was beneficial to patients experiencing pain and fatigue. Meditation with eyes open was preferred by a patient experiencing post-traumatic stress symptoms, and a deaf patient who needed to see the American Sign Language interpreter. Information presented on PowerPoint slides was also shared verbally for patients with impaired vision or those who identify as auditory learners, and recapped in an After Visit Summary, which helped a patient with mild cognitive impairment from a brain tumor. Following enrollment of a patient with known food insecurity, financial toxicity was added to a list of challenges that can make healthful eating difficult for people undergoing treatment for cancer (recognizing also the preference to be referred to as people living with cancer rather than “cancer patients”).
Patient Selection
All patients were adult, English-speaking patients in active cancer treatment at the UCSF HDFCCC. Active cancer treatment is distinct from post-cancer treatment (ie, no further planned cancer treatment, as the patient has transitioned to survivorship or palliative symptom support). Active cancer treatment includes patients receiving systemic therapy, radiation, and those on a break from treatment for metastatic disease. Half of the slots in each cohort were reserved for patients who self-identified as BIPOC.
The GMVs were introduced to patients verbally or via a message in the EMR from a known oncology or supportive care provider, followed by a formal invitation in the EMR. If a response was not sent via the EMR, clinic staff called patients to confirm interest and availability. Occasionally, patients’ treatment schedules were adjusted or space was secured in the clinic or infusion center to facilitate participation.
We report here on the first 10 series, conducted between October 2021 and December 2022. Each cohort had 7-8 patients (median 8), with 78 patients total. Each patient had the option to invite one caregiver to attend with them; 16 caregivers participated.
Data Collection and Analysis
Data was collected via participant questionnaires administered using REDCap (Research Electronic Data Capture). 42 A clinical research coordinator emailed participants links for REDCap surveys at baseline, mid-series, end-of-series, and at 3-month follow-up. Reminders were sent via REDCap up to 5 times, 3 days apart, if surveys were not completed. Baseline surveys included demographics, symptoms (Memorial Symptom Assessment Scale and National Comprehensive Cancer Network Distress Thermometer [NCCN DT]), prior experience with mind-body practices, and reasons for participation. Evaluations sent during and at the end of the series requested feedback on various aspects of the intervention, such as overall satisfaction and feedback on length and frequency of sessions. The 3-month follow-up survey assessed for ongoing impact, including whether participants continued to use practices they learned during the MB-GMVs.
Descriptive statistics were used to summarize demographics, clinical characteristics, baseline symptoms, and evaluation responses, as well as feasibility (ie, ≥50% BIPOC enrollment) and acceptability variables (ie, attendance and satisfaction). Frequency distributions and percentages were used to summarize categorical measures. Means (standard deviation, SD) and medians (range) were used to describe symmetric and skewed continuous measures.
We included three sources of qualitative data: responses to questionnaires, field notes, and facilitators’ written reflections. Questionnaires included open-ended fields eliciting comments on what patients found most and least helpful about MB-GMV sessions. During GMVs, a clinical research coordinator (IL) engaged in participant observation using structured field notes with prompts on participant interactions, telehealth dynamics, what happened during each session, and any problems that arose. Additionally, core GMV facilitators documented reflections in memos written immediately after each session and guest facilitators completed exit evaluations. Team members reviewed participant responses to open-ended evaluation questions, observational field notes, and memos to identify thematic patterns across cohorts.
Results
Of the 101 patients invited to participate, 81 (80%) enrolled (Figure 1). Among 20 patients who declined participation, 14 (70%) identified as male, and 11 (55%) identified as BIPOC. Reasons for declining primarily related to scheduling or lack of interest. One patient cited inability to access Zoom. Three patients enrolled but cancelled before the first visit due to cancer-associated complications. Mindfulness-Based Group Medical Visits Patient Flow Diagram. Summary of patient recruitment, attrition, attendance, and data collected. EMR: electronic medical record; BIPOC: black, indigenous, and people of color. A program goal was to enroll ≥50% patients who identify as BIPOC.
Demographic and Clinical Characteristics (N = 78 Except as Noted).
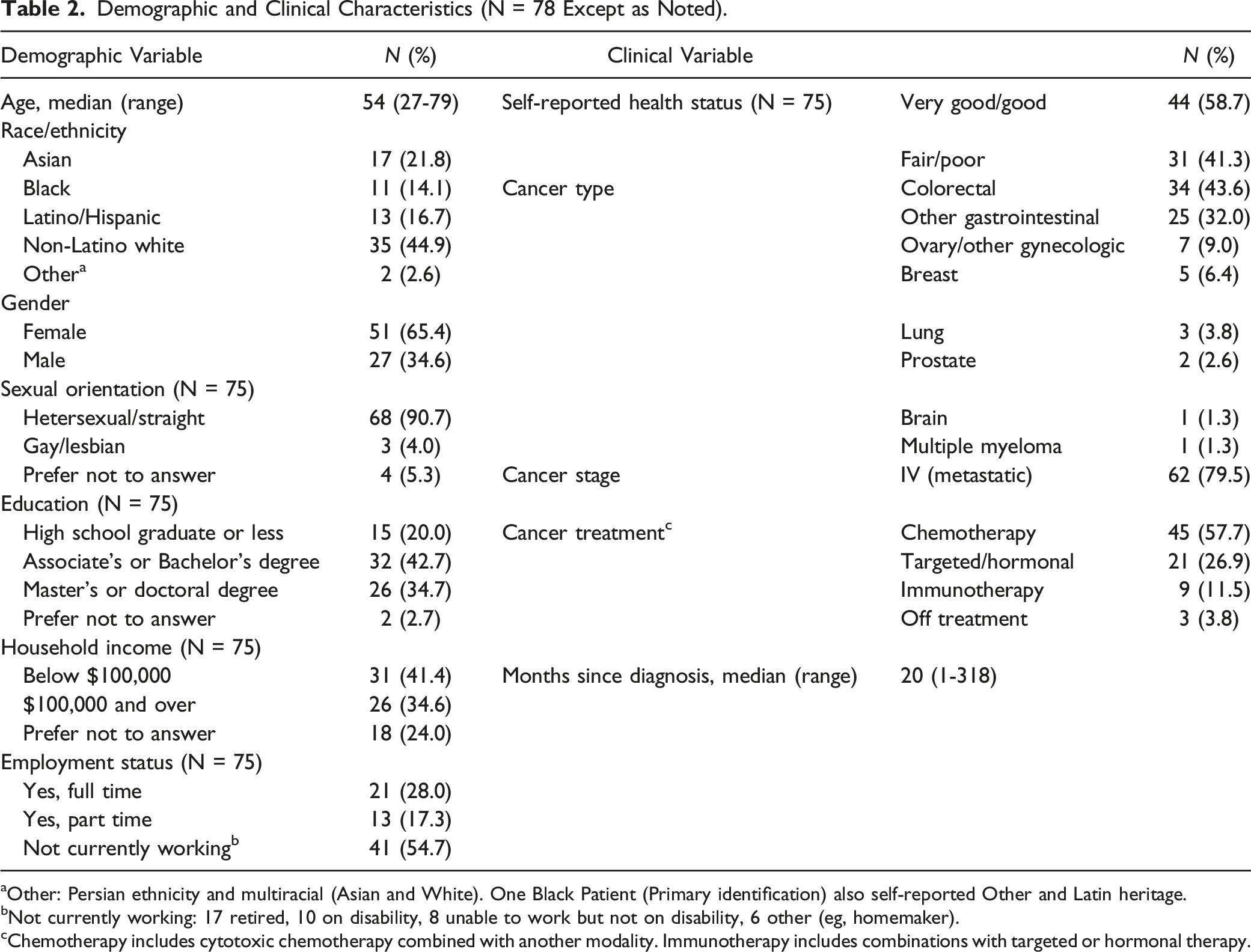
aOther: Persian ethnicity and multiracial (Asian and White). One Black Patient (Primary identification) also self-reported Other and Latin heritage.
bNot currently working: 17 retired, 10 on disability, 8 unable to work but not on disability, 6 other (eg, homemaker).
cChemotherapy includes cytotoxic chemotherapy combined with another modality. Immunotherapy includes combinations with targeted or hormonal therapy.
Memorial Symptom Assessment Scale: Burden of Symptoms With >20% Prevalence (N = 78).
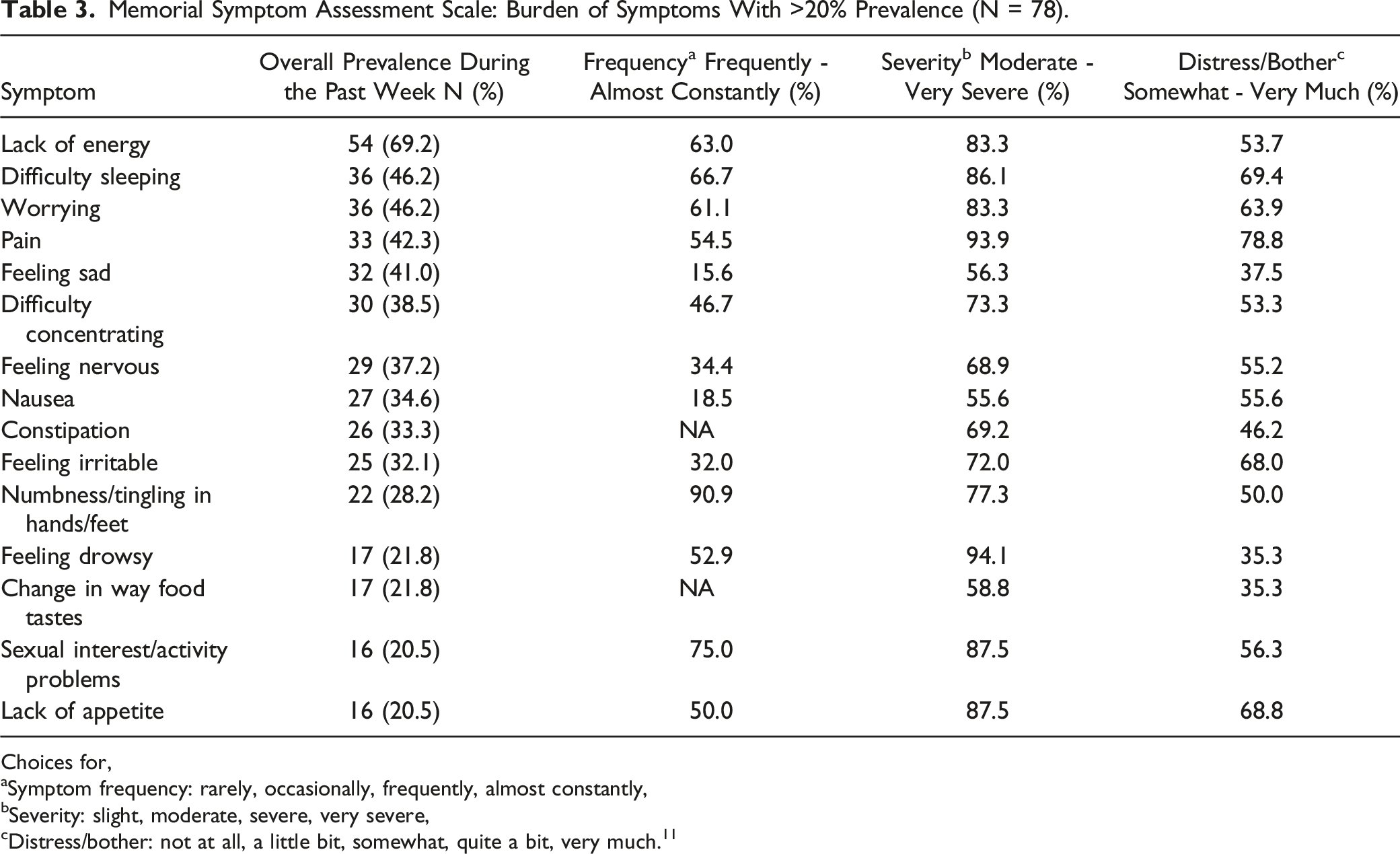
Choices for,
aSymptom frequency: rarely, occasionally, frequently, almost constantly,
bSeverity: slight, moderate, severe, very severe,
cDistress/bother: not at all, a little bit, somewhat, quite a bit, very much. 11
Attendance and Acceptability of Intervention
The missed appointment rate was 11% (33 missed visits out of 312 scheduled), with 70 (90%) patients missing one visit or less. The main reasons for missed visits were schedule conflicts or feeling unwell. Attendance was encouraged by communicating with patients and coordinating with infusion center and clinic staff to provide a private space and telehealth equipment to join visits on treatment days. Patients were invited to modify as needed, including turning their cameras off, lying down, and mostly listening if they were feeling ill. Patients regularly joined during car rides to and from medical appointments and with chemotherapy running, citing that they considered the GMVs an integral part of their cancer treatment. Sixteen (20%) patients joined with a caregiver, the majority of whom were spouses/partners (other caregiver relationships: mother, daughter, sister, and friend); dogs and cats also made frequent appearances.
Mindfulness-Based Group Medical Visit Evaluation and Follow-Up Survey Data.

GMV, group medical visit.
aRatings were the same for facilitator 1 and 2’s organization, explanations, knowledge, and attitude.
Patient Experiences with Equity-Focused MB-GMVs
Qualitative data highlighted three aspects of MB-GMVs adapted for diverse patients in active treatment: the value of offering mind-body practices from a range of cultural traditions; patient empowerment; and group interactions. Patients frequently commented on the diversity of the fellow participants and sense of comfort and safety in seeing others with diverse backgrounds in the group, as well as the diversity of practices, as critical aspects of their learning. One patient, who was reserved during the first two visits, opened up after the shaking and dancing meditation, which has African, Native American, and Asian roots. They revealed that they loved dancing in their youth and the freedom to move as the body was able without choreography or expectation. Another, who was new to qigong, discovered that it felt familiar, having seen elders practice similar movements while growing up in China.
Several patients observed that experiencing effects of the practices in their bodies and on their state of mind was impactful and surprising— redirecting their focus from what they cannot do, to opening new possibilities for what they can do. For example, one patient who had been a yoga practitioner stopped due to physical limitations after their diagnosis. They commented that chair yoga was more accessible for their current physical condition and enabled them to resume their practice. Patients also expressed that it was empowering to hear medical professionals affirm their existing spiritual traditions and self-care habits could contribute to mindfulness practice and overall health. Participants with diverse secular, spiritual and religious backgrounds (including but not limited to Buddhist, Catholic, Christian, Hindu, Jain, Jehovah’s Witness, Jewish, Muslim, Nature and Spirituality-based paths, Shinto, Sikh, and Taoist) shared a feeling of encouragement to adapt mind-body practices as appropriate and integrate them into their personal and family traditions.
Patients consistently shared that interacting with peers was a strength of the GMV format. They described learning from other group members and feeling supported, connected and less alone. Several patients noted prior negative experiences with support groups, and that the facilitated MB-GMVs were different because of the mind-body focus. We noted that patients with limited English proficiency shared less in the group setting. However, all responded to group prompts, questions and/or individual reflections; and most spoke very openly during individual consultations and reported benefits from participation despite language barriers. One patient who was doing well physically during the series found it difficult to see others who were sicker. For others, GMVs created an opportunity to connect through their shared experiences of cancer treatment. At the end of each series, one patient per group volunteered to be the point-person for continued interaction. Following the GMVs, two patients synchronized their infusion appointments so that they could spend time together in person. One patient shared (quote used with permission): “I found solace in the idea that my experience is both entirely unique and somewhat predictable. Hearing from others who are also experiencing the anxiety and stress of cancer, but from different backgrounds, and with different approaches to mindfulness was helpful and interesting.”
Provider Experiences
In exit evaluations, GMV facilitators universally reported gaining knowledge, practices and/or resources that were both personally helpful and useful for providing care to future patients with cancer. Reflections captured in facilitator memos indicated that the MB-GMVs were a rare opportunity in healthcare to meet patients as fellow learners and teachers. During the GMVs, unlike in a usual oncology visit, all team members responded to the check-in questions (eg, what brings you joy?) and shared personal experiences with mind-body practices. Facilitators noted increased fulfillment in leading racially and ethnically diverse groups, and working with patients who were new to mind-body practices. One nurse reported that MB-GMV facilitation was practice-changing, leading him to “look at the familiar through a different lens.” Employing techniques learned in the series, this nurse reported pausing and breathing with a distressed patient whom he was attempting to counsel over the phone, effectively deescalating a tense communication. A physician guest facilitator noted that she began using the micro-practices frequently with patients during her outpatient clinic visits, finding them to be highly accessible and effective. She also expressed feeling a sense of “rejuvenation and nourishment” while facilitating the GMVs, sharing how meaningful it felt to be in a community with colleagues and patients in this unique context. She reported that this experience increased her job satisfaction and deepened her connection to her clinical work. In addition, facilitators noted positive impacts on communication between clinicians, patients, and family members, extending beyond the group series. Several facilitators remarked that their newly learned or augmented mindfulness skills improved their day-to-day communication in their professional interactions and relationships.
Common challenges reported by the guest facilitators were difficulty initiating discussions when reflections and questions were sparse and guiding the conversation when a patient became emotional in the group setting. Holding this discomfort, a nurse observed, “helped me see that not all patients are aware that the challenges they experience during treatment are shared with other patients. It also helped me understand the emotional needs of patients and their fortitude under emotional distress.” Specific prompts and tips were added to the manual based on co-facilitator feedback. After guest facilitation, clinicians reported being able to describe the GMVs to patients with greater specificity, aiding recruitment.
Discussion
With this QI pilot of equity-focused MB-GMVs for racially and ethnically diverse patients in active cancer treatment, we demonstrated feasibility of ≥50% BIPOC enrollment in a telehealth program serving people with advanced cancer. Acceptability and appropriateness were evidenced by high attendance rates and favorable satisfaction ratings. Sustainability was achieved by billing insurance for guideline-concordant care. Qualitative observations are consistent with prior literature indicating that GMVs decrease social isolation, increase social support, and improve patient-provider relationships.30,44 Our findings indicate that MB-GMVs using inclusive strategies, embedded into standard oncologic care, are a promising approach to promote health equity by addressing unmet mental health and other symptom management needs that disproportionately impact patients from racial and ethnic minority groups.1,2 Below we discuss key learnings from this pilot project related to recruitment, retention and sustainability, as well as challenges and limitations.
Designing the MB-GMVs with half the slots reserved for BIPOC-identified patients was a pragmatic decision to balance timely access to integrative oncology care with an intention to provide a safer space for addressing cancer disparities. Our high recruitment rate (80%) depended on outreach by trusted clinicians (MDs, RNs, NPs, acupuncturists, and psychotherapists), who referred patients in greatest need of supportive care resources. Barriers to participation, including scheduling conflicts, were proactively addressed. This “high-touch” recruitment method may be less efficient than self-referral, however, it supported participation by patients who did not directly request integrative oncology services.
Our MB-GMVs had a remarkably high attendance rate (89%), especially taking into account that the majority of patients were in treatment for metastatic cancer. In contrast to our Being Present MBI which had a significantly lower participation rate in a similar population, 34 we posit that scheduling the GMVs as part of comprehensive cancer care, led by cancer center clinicians, motivated attendance. This was supported by documented reasons for participation and qualitative responses on study evaluations. Our intervention is adapted for a multicultural population, equity-focused and trauma-informed. Directly addressing trauma in an MBI for diverse patients is important, acknowledging the high prevalence of trauma in BIPOC communities, and a cancer diagnosis itself can be experienced as a trauma. Feedback received suggests that being intentional about creating inclusive experiences allowed patients to engage and feel connected to the group.
Attendance was also supported by the GMV structure, including assistance provided by clinical and research staff. Although some patients expressed a preference for in-person groups and/or a higher number of shorter visits, four 2-hour visits on Zoom worked for most patients and had several advantages. Video visits increased access for patients in cancer treatment, hailing from a large geographic area, many of whom were also balancing work, childcare, and other responsibilities. An unexpected bonus of the video visit format was caregiver and pet participation, contributing to an atmosphere of friendliness and joint learning to establish new habits within families/social networks. With a 4-week MB-GMV series, it is easier to predict health status of patients with advanced cancer compared with a longer time span.
Sustainability is an important component of access. Co-facilitation by two MDs from different disciplines (medical oncology and radiation oncology or palliative care) allowed both providers to bill insurance. RNs were permitted by our cancer center to participate under “Education & Training” time, with float coverage provided. Clinical practice coordinators and medical assistants were supported by revenue generated by MD and/or NP facilitators. The clinical research coordinator was supported by grants and philanthropy. One challenge is that if multiple clinician-facilitators are from the same discipline, they cannot each bill independently for the same patient on the same day of service. Another challenge is that non-clinician content experts, like yoga and qigong instructors, are unable to bill insurance currently. Because our objective is to avoid passing costs onto patients, we are investing in the creation of free, high-quality video practice resources tailored to diverse patients in active cancer treatment. Finally, manualization of workflows and content has been critical to sustaining an interprofessional GMV team with fixed and rotating members, while maintaining consistent quality.
Prior literature reports benefits of mindfulness programs and GMVs for clinician wellbeing,44-46 through increased resilience and job satisfaction and reduced burnout. Our study similarly found multiple kinds of health professionals (clinicians, clinical and research staff) reported positive impacts of the MB-GMVs. These included opportunities for mindfulness practice throughout the workday, extended time with patients, improved communication, team-based care, and interdisciplinary collabration. Moreover, this GMV series has enhanced the provider experience across our center. Its unique content, structure, and emphasis on diversity and equity has inspired the creation of a number of other GMVs at our institution. Several clinicians have approached the study team to learn how to launch and sustain GMVs of their own. Engagement of multiple healthcare providers in the MB-GMVs has promoted coordination of clinical workflows, data collection, and cross-recruitment.
Limitations of our QI pilot include that it was not designed to formally assess intervention effectiveness for reducing symptoms and improving quality of life. The 3-month follow up survey return rate was low (31%), consistent with what we previously observed in a metastatic cancer population. Additionally, recruitment of Latino patients was low compared to Latino representation in our catchment area (17% vs 38%). This reflects similar underrepresentation of Latinos at UCSF HDFCCC and is related to another limitation: our MB-GMVs were only offered in English. As a next step we propose to conduct a pragmatic effectiveness trial in English and Spanish at UCSF and community-based clinics to determine the effectiveness of MB-GMVs adapted for racially and ethnically diverse patients in active cancer treatment.
Our conclusions from this MB-GMV pilot are as follows: First, MBIs need to be adapted for feasibility and appropriateness during cancer treatment and for cultural relevance and acceptability among racially, ethnically, and linguistically diverse populations. Second, effectively translating evidence-based interventions into practice requires careful attention to intervention fidelity and adaptations to ensure fit and flexibility for diverse contexts and populations. Third, adapted MBIs need to be embedded as part of routine oncologic care to increase uptake, particularly for patients with limited economic resources and demanding treatment schedules. Factors affecting implementation, such as patient-level barriers and healthcare setting, also need to be considered to support equitable access to MBIs.
Guideline-concordant symptom support should be available to all patients undergoing cancer treatment. Culturally-adapted and trauma-informed MB-GMVs embedded into standard oncologic care offer a promising approach to reduce health and healthcare inequities among BIPOC patients.
Footnotes
Acknowledgements
We gratefully acknowledge contributions from Donald Abrams, Neha Goyal, Sandy Cuevas, Julie Kesterson, Anand Parikshak, and Nicole Thompson to content development and workflows. Integrative Health Equity and Applied Research fellows Anand Parikshak and Tiffany Nereida Lopez participated in summarizing field notes. Nurses Julie Kesterson and Elizabeth Stewart served as co-facilitators. Julia Wu entered references. We also thank the Helen Diller Family Comprehensive Cancer Center, UCSF Gastrointestinal Medical Oncology and Osher Center for Integrative Health clinical and administrative teams for championing these efforts, together with patients and their families.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported in part by the National Cancer Institute [administrative supplement to award number P30CA082103], the Helen Diller Family Comprehensive Cancer Center, the Mount Zion Health Fund, and other philanthropic support. Authors received additional support from the National Institute on Minority Health and Health Disparities [ATL, K01MD015766]. The funding sources had no involvement in the design and conduct of the quality improvement project; the collection, management, analysis, or interpretation of the data; or in the preparation, review, or approval of the article. Contents are solely the responsibility of the authors and do not necessarily represent the official views of the funders.