
Abstract
Background
Around half the US population uses dietary supplements (DS), and concomitant use with medications is common. Many DS include bioactive substances that can interact with medications; therefore, accurate tracking is critical for patient safety. Unfortunately, documentation of patients’ DS use is often missing or incomplete in the electronic medical record (EMR), leaving patients susceptible to potential adverse events. Novel approaches to assist healthcare professionals (HCPs) in capturing patients’ DS use are needed.
Objective
To assess HCPs’ perspectives on challenges and facilitators of DS documentation in the EMR and their opinions on a proposed mHealth application (app) to aid in DS capture.
Methods
HCPs, recruited from professional networks, largely in North Carolina, using purposive sampling, took part in semi-structured interviews. We inquired about HCPs’ experiences with DS documentation in the EMR and their opinions about our proposed mHealth app. Interviews were recorded, transcribed, and coded. Thematic analysis included deductive codes based on the interview guide, and inductive codes that emerged during transcript review.
Results
HCPs (N = 30) included 60% females, mean age 46 ± 10; 70% White. Pharmacists (20%), nurses (17%), and physicians (17%) were the most represented professions. Years in practice ranged from 3–35 years. Most HCPs were concerned about DS safety and potential supplement-drug interactions, and cited several barriers to accurate EMR DS documentation including time constraints, database inconsistencies, and poor patient-HCP communication about DS. HCPs’ views on our proposed mHealth app were generally positive. They expressed that our proposed mHealth app could streamline documentation processes and enhance patient-provider communication. HCPs expressed desire for a high-quality mHealth app that includes access to evidence-based DS information, integrates with the EMR, and does not increase time burdens.
Conclusion
HCPs believe documentation of patients’ DS use is important but not accurately captured in the EMR. Support was expressed for our proposed barcode-scanning DS mHealth app.
Keywords
Introduction
Dietary supplement use is common throughout the United States (US) with an estimated 58% of US adults reporting current use of supplements based on data from the 2017-2018 National Health and Nutrition Examination Survey (NHANES). 1 Concomitant use of dietary supplements and prescription medications in the US is estimated to be between 34% and 66%, and among older adults, aged 62-80 years, 15% are estimated to be at risk of potential major drug-drug, drug-dietary supplement, or drug-herb interactions.23,4 Dietary supplement use is especially common among older adults, especially people taking multiple prescription medications, 5 as well as people diagnosed with cancer, and people with multiple chronic conditions.6,7 For example, a study using NHANES data from 2003-2016 found that 70% of cancer survivors reported dietary supplement use compared with 51% of people without cancer. 2 Concomitant use of dietary supplements and prescription medications is also more common among people with chronic medical conditions (47% vs. 17%). 2
Dietary supplements are available without a prescription in the United States, leading many people to presume they have low potential for harm.8,9 However, there are safety concerns associated with dietary supplement use; these include adverse events, which were estimated to be 22% among users in one study, and the potential for serious drug-supplement interactions which were estimated in another study to be 49% among patients concomitantly using dietary supplements and tetracycline antibiotics or antihypertensive medications.10,11 There are additional safety concerns about direct toxicity, overdose, and adverse events resulting from ingestion of dietary supplements tainted with pharmaceutical drugs and/or undisclosed ingredients. For example, one woman suffered a hemorrhagic stroke while exercising after ingesting a sports supplement with an undisclosed amphetamine-like ingredient called β-Methylphenyl-ethylamine. 12 Between 2007-2016 the US Food and Drug Administration issued warnings for unapproved pharmaceutical ingredients in 776 dietary supplements. 13 There is also poor communication about dietary supplement use between patients and healthcare professionals (HCPs). For example, one study reported that during inpatient hospital stays, only 6% of patients were asked about dietary supplement use and had this documented in their medical record. 14 A 2019 systematic review and meta-analysis (N = 11,754) estimated patient disclosure rates of dietary supplement use to be 33% (95% CI: 24% to 43%). 15 Patients also often initiate dietary supplement use without consulting a HCP. For example, a study of 2772 adult cancer survivors found that 46% of participants utilized dietary supplements without consulting a HCP. 7 The Joint Commission and the American Society of Health-System Pharmacists recommend monitoring patient use of dietary supplements; however, many health systems lack policies and procedures to accurately document dietary supplement use. 16 These data highlight a gap in patient-provider communication about patients’ dietary supplement use and a lack of accurate capture of patients’ dietary supplements information in the electronic medical record (EMR); the combination of these factors make it difficult for HCPs to prevent poor safety outcomes related to patients’ use of dietary supplements.
Health technology may provide a solution to assist with dietary supplement capture in the clinical setting, but EMR systems do not currently support accurate dietary supplement capture and documentation. For example, medication databases within EMRs are incomplete and do not contain the estimated 85,000 different dietary supplement products available to consumers in the US; they also omit many combination products with multiple ingredients entirely. 17 It can even be difficult to find exact matches for products containing a single vitamin, herb, or mineral. Barcode scanning and product databases have advanced the accuracy and efficiency of data input across several industries including retail and shipping and hold the potential for implementation in healthcare.18,19 Many healthcare systems have already integrated barcode scanning with handheld devices into medication verification; for example, one study reported significantly higher user satisfaction and quality of information gathered compared to manual medication entry methods. 20 However, utilizing handheld devices or mobile health (mHealth) applications (apps) to capture dietary supplement information through barcode scanning, QR codes, or image recognition technology have yet to be implemented for capture of dietary supplement information in clinical care.
In a previous publication we reported results from a qualitative focus group study assessing patient perspectives on the development of a novel mHealth app to assist with dietary supplement documentation in the EMR. 21 In this study, we extended our investigation to HCPs where we sought to understand the clinical experiences, opinions, and perspectives of HCPs regarding patients’ use of dietary supplements, patient-provider communication about dietary supplements, and current challenges with accurately capturing and documenting patients’ dietary supplement use in the EMR. We also sought to obtain HCPs’ opinions and recommendations about a proposed mHealth app to improve capture and documentation of dietary supplements in the EMR.
Methods
Participants and Recruitment
Adult participants were recruited through purposive sampling with the intent of recruiting HCPs from differing job roles including physicians (e.g., internists, oncologists, infectious disease specialists, and family medicine practitioners), nurses, pharmacists, dietitians, physician assistants, naturopathic doctors, and medical assistants. A broad representation of the multiple types of HCP stakeholders involved in collecting and assessing dietary supplement information was felt to be important to understanding the challenges and potential solutions to the reconciliation of dietary supplement data. Racial and gender diversity was also considered during the recruitment of participants. For example, utilizing their collective professional networks and a “snowball” approach, the researchers made the decision to contact potential participants from minoritized groups when possible, with the aim of achieving a racial and gender distribution that reflected the larger population from which the sample was recruited. Most recruitment occurred within the University of North Carolina (UNC) Health System but also extended to other organizations across the country to ensure a wide variety of HCP types. These included the VA Health System outside NC, the University of Minnesota, a representative of the dietary supplement industry, and the Goshen Health System. Potential participants were contacted via email about their interest in the study. Participants expressing interest were provided with more information prior to the interview, including the questions that would be asked, the composition of the research team, and the goals of the research study. Many of the study participants had a pre-existing professional relationship with one of the investigators but not necessarily the researchers who conducted the interviews. All participants provided verbal informed consent for participation. This study was approved by the University of North Carolina Institutional Review Board (#18-2099).
Conceptual Model
The HCP interviews were designed to elicit stakeholder input on clinical experiences and perspectives related to dietary supplement tracking and reconciliation and for the development of a mHealth application, including desired features, that could be used to identify and track dietary supplement use. A parallel study, already reported, investigated patients’ perspectives on the proposed mHealth application and describes the conceptual model we used for both studies in detail. 21 Briefly, the conceptual model, based on the Unified Technology Acceptance and Use of Technology (UTAUT) model with added constructs from the Health Belief Model, influenced the construction of the interview guide (Appendix 1).22,24 UTAUT has been applied to studies of technology acceptance among providers. 25 Key constructs include effort expectancy (beliefs about how easy the product would be to use), performance expectancy (beliefs about product features and reliability), social influence (intent to recommend the product to patients), and behavioral intention (intent to use the product in clinical care). Health Belief Model constructs included perceived threat (safety of dietary supplements) and perceived benefit (potential advantages related to the use of the mHealth application). 24 Examples of interview questions included 1) How comfortable are you in discussing supplement use with patients? 2) How do you feel about the importance of documenting dietary supplement use in the clinical record? 3) As described, how easy do you think the proposed app would be to use? 4) If the app were available today, how likely would it be for you to use it or recommend it to your patients? 5) What risks or downsides do you see to this type of mHealth app?
Research Team and Data Collection
Data was collected through a series of investigator-facilitated HCP interviews between 2019 and 2021. At least one investigator and one interviewee took part in each HCP interview, often with a second interviewer to take notes. Interviews were conducted by members of the research team (ZK, JH, KF, AC, KN, EP, SK, and AHC), using an interview guide with scripted questions developed as part of the research protocol (Supplemental file: Interview Guide). Co-investigators JH, KF, and AHC are experienced qualitative researchers and trained the research associates (ZK, KN, EP, SK, and AC). At the time of the interview, HCPs were shown a slide deck that described the research, the proposed app, and assumptions of the research team. HCPs self-reported sociodemographic and professional characteristics from open-ended questions (e.g., “with what race and/or ethnicities do you identify?”). Interviews were conducted either in person, by telephone, or through video conference using Zoom (Zoom Video Communications, Inc., San Jose, CA). Interviews were audio-recorded and transcribed verbatim; they were supplemented by detailed notes taken at the time of the interview about responses and context. Each HCP participated in only one 20-30-minute interview, and HCPs were not re-contacted to review the transcripts. Participants received a $25 gift card as compensation for their time. Confidentiality was protected by careful data management and storage, relying on the use of the REDCap (Research Electronic Data Capture) electronic data capture tools.25,26 Interviews were conducted until the study team felt that data saturation was achieved.
Data Analysis Methods
After the interviews were transcribed, transcripts were checked by a member of the research team for accuracy and compared with the interview notes. Transcripts were uploaded into ATLAS.ti (version 8 for Windows, Scientific Software Development GmbH, Berlin, Germany). At least two team members coded each interview. Initial codes were related to the conceptual model, but more codes were generated by four team members (ZK, KF, AC, and SK) in response to the data (Supplemental Table 1. Codebook). Codes were compared through team meetings and modified by consensus. A coding tree was developed using grouped codes in Atlas.ti software and by using a virtual whiteboard in Microsoft Teams for visual representation (Supplemental Figure 1: Whiteboard). The analysis used an iterative process, based on within-interview and between-interview examinations by all four team members, to group codes into themes and subthemes using codes from within and between interviews. The team decided on final themes with associated quotations. The consolidated criteria for reporting qualitative research (COREQ) checklist guided the conduct of the study. 27
Results
Study Participant Characteristics

aHealthcare Professionals self-reported sociodemographic and professional characteristics from open-ended questions (e.g., “with what race and/or ethnicities do you identify?”).
bPlus-minus values are means ± SD (Standard Deviation).
cSociodemographic and professional characteristic data was available for most but not all HCPs: Age (n = 28), Race and/or ethnicity (n = 27), Years in practice (n = 29).
dSelf-identified as African American (n = 5), Black (n = 1).
eSelf-identified as White (n = 5), Caucasian (n = 10), White/Caucasian (n = 4).
fTotal does not add up to 100 because percentages were rounded to the nearest whole number.
gThere were n = 29 responders to the questions about the percentage of patients using dietary supplements, and n = 26 responders to the question about supplement discussions with patients and personal use of supplements.
Documentation of Dietary Supplements in the EMR
We interviewed HCPs about their clinical experiences and perspectives on patients’ use of dietary supplements and documentation of dietary supplement use in the EMR and identified five themes: 1) HCPs felt documentation of patients’ dietary supplement use in the EMR is important but not well executed for the following reasons; 2) the time required to enter dietary supplement information into the EMR; 3) the process of entering dietary supplement information into the EMR; 4) communication problems between providers, technicians, and patients about dietary supplement use; 5) provider safety concerns regarding dietary supplement use. Figure 1 illustrates the reasons for inadequate documentation of dietary supplements in the EMR identified by HCPs. Representative quotes illustrating the five themes related to HCPs' clinical experiences and perspectives on patient use of dietary supplements and the challenges of documenting patients’ dietary supplement use in the EMR are presented in Table 2. Fishbone diagram depicting themes related to healthcare professionals’ (HCPs) clinical experiences and perspectives on patients' use of dietary supplements (DS) and challenges of documenting patients’ DS use in the electronic medical record (EMR). Representative Quotes From HCPs About their Clinical Experiences and Perspectives on Patient Use of Dietary Supplements and Challenges of Documenting Patient’s Dietary Supplement Use in the EMR.
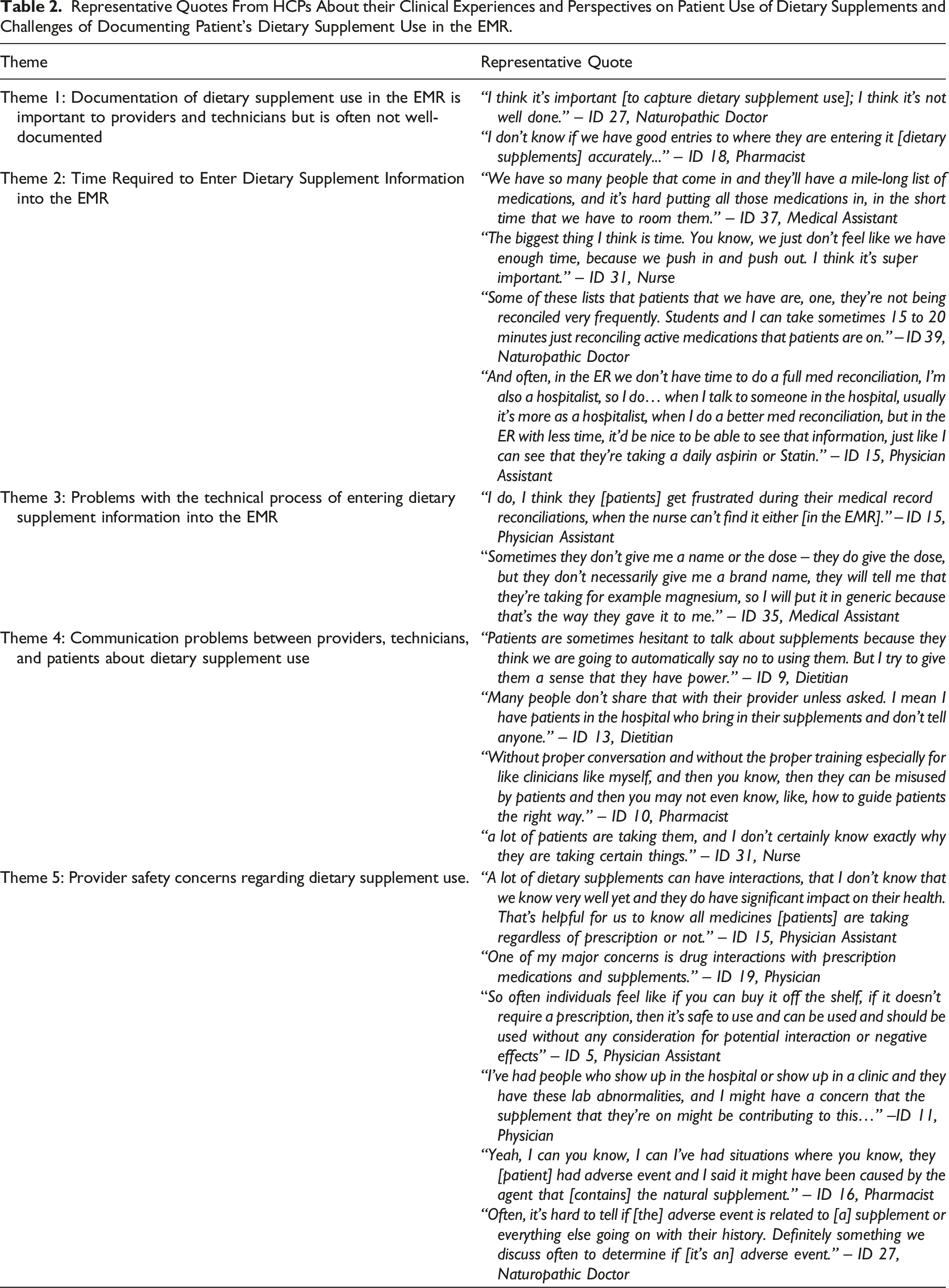
Theme 1: Documentation of Dietary Supplement use in the EMR is Important to HCPs but is Often not Well-Documented
HCPs expressed that documentation of dietary supplements in the EMR is important but also noted that its documentation, when it is done, is often inaccurate or incomplete (Figure 1 and Table 2). Reasons for the incomplete or inaccurate documentation of dietary supplements in the EMR are further explained in themes 2, 3, and 4 below, and in Figure 1 and Table 2.
Theme 2: Time Required to Enter Dietary Supplement Information into the EMR
HCPs identified time constraints of clinical visits as a hindrance to the documentation of patients’ dietary supplements in the EMR (Figure 1 and Table 2). Additionally, the manual process of entering the dietary supplement information into the EMR is time-consuming, and technical reasons for this are presented in theme 3.
Theme 3: Problems With the Technical Process of Entering Dietary Supplement Information into the EMR
HCPs identified problems with the technical process of dietary supplement entry into the EMR (Figure 1 and Table 2). For example, they reported that existing EMR databases do not have complete information on the full range of dietary supplement products available to consumers. This leads to inaccuracies in the patient’s medication and dietary supplement list and can contribute to patient, provider, and technician frustration. If the exact product a patient is taking is not contained in the EMR database, providers and technicians (e.g., medical assistants) will typically employ one of four strategies: 1) enter a generic product they believe is similar to what the patient is taking; 2) add the product as a free-text item in their medication list; 3) document the product in the patient’s chart note; 4) leave the product out of the patient’s record entirely. We also heard from providers and technicians that poor patient recall of detailed dietary supplement information like product names, dosage, and ingredients also hinders the technical process of their entry into the EMR.
Theme 4: Communication Problems Between Providers, Technicians, and Patients About Dietary Supplement Use
HCPs of all types recognized poor patient-provider communication about dietary supplement use as a major problem (Figure 1 and Table 2). Participants identified that this may occur because HCPs do not always ask about dietary supplement use, and because patients may not volunteer the information to providers. HCPs also expressed that some patients do not disclose their use of dietary supplements for fear of provider disapproval.
Theme 5: Provider Safety Concerns of Dietary Supplement use and Supplement-Drug Interactions (SDI)
HCPs of all types expressed concerns over the safety of dietary supplement use and the potential for interactions between dietary supplements and medications, supplement-supplement interactions, and interactions between supplements and medical conditions or disease processes. HCPs identified a common belief among patients that dietary supplements are safe because they are available without prescription; some HCPs also reported seeing abnormal lab values, symptoms, or adverse events that were suspected to be related to their patient’s dietary supplement use (Figure 1 and Table 2).
HCP Opinions About App Construction
Representative Quotes Related to the Barriers and Facilitators of App Use.

Theme 1: Benefits of the Proposed App and Facilitators of Use
Subtheme 1a—App May Improve Reconciliation
HCPs believed that the proposed app would improve reconciliation. Many HCPs felt that the app had the potential to lead to a more accurate list of the dietary supplements their patients were taking.
Subtheme 1b—App May Save Time
Most HCPs expressed a belief that the app would save time in the clinical encounter by streamlining the documentation and reconciliation process. If patients are able to generate their own dietary supplement list and upload their dietary supplement list, the HCP only needs to verify the list with them.
Subtheme 1c—App May Uncover Safety Threats
HCPs who were especially concerned about the safety of dietary supplements said that the app may be able to uncover potential safety threats, either those related to supplement-drug interactions or to adverse effects from the supplements. They saw this as an added benefit of the app.
Subtheme 1d—App May Enhance Patient-Provider Communication
HCPs who endorsed the belief that many of their patients use dietary supplements viewed the app as a tool to facilitate patient education about dietary supplements, particularly in the context of a disease process or potential for supplement-medication interactions.
Theme 2: Risks Associated With the Proposed App and Barriers to Use
Subtheme 2a—App May Have a Negative Effect on the Clinic Workflow
Although the proposed app was viewed as beneficial by most participants, not all HCPs were supportive of integrating the app into a clinical encounter. Their chief concern centered on the potential for increased HCP burden related to interacting with patients about their dietary supplement use. HCPs who stated they do not ask patients about their dietary supplement use felt that obtaining this information would add unnecessary time to visits, especially since they felt ill-prepared to judge the safety of individual products or the potential for SDI. They wondered if improved dietary supplement reconciliation would prompt patients to ask more questions about dietary supplements that would add to their workload.
Subtheme 2b—Dietary Supplement Information May be Inadequate
HCPs expressed concerns about the overall reliability of information about dietary supplements, their complexity, and rapid changes in dietary supplement product formulations. These concerns would reduce the value of the app in clinical encounters.
Subtheme 2c—App Quality Issues
HCPs also worried about the potential for technical glitches that would affect their workflow. They said that a poor-quality product may lead to more questions from patients that they are unable to answer.
Theme 3: HCP Recommendations and Performance Expectations
HCPs had specific recommendations about desired app features: 1) attention to privacy; 2) accessibility; 3) links to the dietary supplement evidence base including SDIs; and 4) seamless integration into the EMR.
Subtheme 3a—Attention to Privacy
Most HCPs stated they would not be concerned about privacy if the proposed app had high-level, HIPAA compliant protections common to healthcare products currently on the market.
Subtheme 3b—Accessibility
Several HCPs pointed out access issues for different patient populations. Some patients may not have a smartphone and others may not have the technical capability to use an app or to scan their information prior to their visit. HCPs also recommended an alternative method for accurate collection of the information such as a point-of-care scanner or in-clinic tablet linked to the dietary supplement database. In addition, the developers of the app should pay attention to design features that would make it easier to use for patients who are older adults (e.g., large text) or do not speak English (e.g., universal icons).
Subtheme 3c—Links to the Dietary Supplement Evidence Base
Many HCPs expressed the desire to increase access to evidence-based information about dietary supplements, especially notifications of clinically relevant SDIs. This was seen as potentially saving time, educating patients, and assisting them in becoming more knowledgeable about dietary supplements themselves.
Subtheme 3d--Seamless Integration into the EMR
Most HCPs felt that it was essential that the app could integrate into the EMR. Without the integration, they were concerned that the app would cost rather than save them time. Figure 2 Diagram depicting themes related to the app features recommended by healthcare professionals (HCPs) and technicians and the perceived facilitators and barriers to use of a dietary supplement (DS) application (app). SDI (supplement-drug interactions). EMR (electronic medical record).
More themes were generated related to the facilitators of app use compared to the barriers to app use. Therefore, the balance in Figure 2 is weighted toward facilitators.
Discussion
Summary of Results
HCPs acknowledged the importance of accurate dietary supplement documentation, but also expressed several challenges to implementation. These include inaccurate database entries, wide variations in supplement ingredients and dosing, lack of patient disclosure of supplement use, poor patient recall of dietary supplement information (e.g., brand, dosing, and ingredients), and time requirements for manually entering dietary supplement information into the EMR. Our study shows that HCPs believe there are significant gaps in accurate dietary supplement documentation, tracking, and reconciliation within the EMR. These gaps include technical issues (e.g., inadequate dietary supplement product databases, cumbersome manual dietary supplement entry), and interpersonal issues like absent or inadequate patient-provider communication about dietary supplement use.
Sampled HCPs were largely supportive of an mHealth app solution to assist with dietary supplement documentation, tracking, and reconciliation. If the mHealth app can be integrated into the EMR, most saw it as substantially improving the medication reconciliation process, both in terms of speed and accuracy of documentation. They recognized the app could rapidly reconcile a large volume of dietary supplement information allowing more time for direct patient interaction and face-to-face communication, including counseling on supplement-medication and supplement-disease interactions. However, a small subset of participants expressed concerns that the app may increase their time burden, rather than increasing efficiency. In addition, they expressed specific concerns about access; several participants suggested that patients who are older, non-English-speaking, or not technically savvy may have difficulty using the app. They also wanted assurance that the app would be linked to high-quality, rapidly accessible information about dietary supplements and their interactions with medications.
Identified barriers to the use of the app included: 1) concerns about privacy and accessibility; 2) the potential negative impact on workflow, particularly if the app is poorly constructed or maintained; 3) increase in burden due to patient questions about dietary supplements; 4) lack of high-quality research on dietary supplements; and 5) challenges integrating the app within the EMR. We believe that many of these barriers could be addressed with technical solutions to improve quality, privacy, and accessibility. In fact, digital health platforms, such as ExerciseRx, are, in practice, using a similar design of a patient app, provider dashboard, and a smart-phone system to sense and detect exercise (https://thesportsinstitute.com/our-work/exercise-rx/). Systems such as ExerciseRx are providing an example of advanced digital interfaces using technical solutions to improve tracking and prescribing of integrative and lifestyle medicine modalities, like exercise or dietary supplements.
However, other operational barriers may be more difficult to address. Implementing a new clinic workflow can be difficult, even for an outcome that could ultimately streamline care; pre-visit uploads of the information may partially mitigate this issue. In addition, increased patient questions about supplements can be both positive and negative. On the positive side, communication is enhanced, but this may contribute to increased provider burden. This barrier may be mitigated by other design strategies including appropriate patient-facing information about dietary supplement safety or utilizing other members of the care team to respond to patient communications, such as pharmacists or mid-level practitioners.
There is truth to the belief among HCPs that sufficient high-quality evidence and information pertaining to safety and efficacy of dietary supplements is lacking. However, our proposed app could contribute to solving this issue by providing information about available evidence-based dietary supplement resources, structure-function claims, and qualified and approved health claims for supplements. For example, an entry for a product containing calcium and vitamin D could include the FDA-approved health claim that “adequate calcium and vitamin D throughout life, along with physical activity, may reduce the risk of osteoporosis in later life”. 28 In addition, the app can include a tool to help providers assess the safety of a particular supplement product such as the US Department of Defense “Operation Supplement Safety” tool. 29
Additional barriers include the challenge of integrating mHealth apps with EMR systems. Most often, data can be exported from EMR systems, but importing external data is often prohibited by governance decisions at the level of the institution. Also, to ensure that the data are integrated into the EMR in a way that is most useful to HCPs, the EMR itself will need to incorporate a dietary supplement database such as the one maintained by the National Institutes of Health Office of Dietary Supplements (ODS). The ODS Dietary Supplements Label Database is updated monthly and can be automatically imported into an EMR, making it a key tool to improve the quality of dietary supplement reconciliation. The database can be searched by ingredient name and/or by product brand name.
Comparisons with Similar Studies
The problem of poor dietary supplement documentation has been known for many years and has been attributed to a lack of provider inquiries and patient disclosures. 12 Both published literature and hospital regulations prompt providers to document dietary supplement use, yet documentation is still poor, possibly due to the challenges identified by our participants. Lee et al., identified supplement-drug interactions as one problem that contributes to the need for adequate dietary supplement documentation. In this study, breast and prostate cancer patients who had completed chemotherapy were questioned about their dietary supplement use. They discovered 1,747 potential medication interactions among 67 participants, 56% of which were related to herbs and dietary supplements. 30
The aim of our study was to gather stakeholder input on the dietary supplement documentation process and the potential use of a mHealth app to improve reconciliation. We are aware that a few other supplement apps have been developed, but none address EMR integration and accurate reconciliation, and few include product-level databases. We feel that the latter is important due to the variability in multi-constituent supplements. For example, a multivitamin-multimineral supplement may contain amino acids, botanicals, metabolites, and proprietary blends that contain additional herbs and nutrients, but not the amount of each ingredient in the blend. If the app had a product-level database, the ingredient information, including the components of a proprietary blend, would be available to the clinician for review.
Study Limitations and Strengths
Most HCPs we interviewed were affiliated with an academic medical center in North Carolina, which limits generalizability to private practices, particularly those in resource-limited areas. In addition, because most of the HCPs worked in North Carolina, generalizability to other parts of the country where practice patterns may differ is yet uncertain. Although we used theory to guide our interview questions, valuable information may have been omitted by our process or by our participants. A strength of our study was that we aimed for broad participation by a variety of provider types, not only physicians and pharmacists, but also other HCPs involved in the dietary supplement documentation process who could have had different perspectives on the barriers and facilitators, e.g., naturopathic doctors, dietitians, nurses, and medical assistants. We also talked to providers that work in a variety of specialties and practice settings; for example, providers working in oncology, emergency medicine, family practice, and infectious disease. However, this strategy had some limitations. Due to limited funding and time constraints, we were not able to ensure that we achieved data saturation within each HCP category, especially regarding differences by specialty. Additional research may be needed to address this issue in a larger population of HCPs. Although we did not target saturation within each HCP category, we feel that saturation was achieved across the sample.
Impact and Future Directions
Accurate dietary supplement documentation is essential to setting the stage for understanding the risks and benefits of dietary supplement use at the population level. In the current regulatory environment, which does not require pre-market establishment of safety and efficacy, post-marketing surveillance of dietary supplements is critical. Post-marketing surveillance relies on passive capture of adverse events including disclosure by the manufacturer and reports made by both patients and providers. Hence, current methods only capture a small fraction of the adverse events related to dietary supplement use. It is only through demand for more active data surveillance and high-quality phase II and III clinical trials that dietary supplement product safety and effectiveness can be established. Future development could include direct reporting of adverse events to the FDA either through the electronic record or the mHealth app.
More robust safety monitoring and identification of adverse events would facilitate research into the impact of dietary supplement documentation on certain endpoints including improved or maintained control of chronic diseases, adherence, and protocol compliance. Synchronization of this data with EMRs would also allow for further research into patient and provider experiences, minimization of data silos, and pharmacoepidemiologic analysis, collectively leading to important implications for patients, payers, and providers.
Conclusions
Most participants expressed the belief that dietary supplement documentation is important but inaccurately represented in the EMR. Support was expressed for our proposed barcode-scanning dietary supplement mHealth app. Accurate tracking and reporting of dietary supplements may improve patient safety and quality of care by helping patients and providers make evidence-informed decisions about dietary supplement use and avoid unwanted supplement-drug interactions.
Supplemental Material
Supplemental Material - Healthcare Professional’s Perspectives on Improving Dietary Supplement Documentation in the Electronic Medical Record: Current Challenges and Opportunities to Enhance Quality of Care and Patient Safety
Supplemental Material for Healthcare Professional’s Perspectives on Improving Dietary Supplement Documentation in the Electronic Medical Record: Current Challenges and Opportunities to Enhance Quality of Care and Patient Safety by Zachary O. Kadro, ND, MPH, Aisha Chilcoat, ND, MPH, Jacob Hill, ND, MS, Stephanie Kenney, PharmD, Catharine Nguyen, PharmD, Elana Post, PharmD, Amanda H. Corbett, PharmD, Gary N. Asher, MD, MPH, and Keturah Faurot, PhD, MPH, PA in Global Advances in Integrative Medicine and Health.
Supplemental Material
Supplemental Material - Healthcare Professional’s Perspectives on Improving Dietary Supplement Documentation in the Electronic Medical Record: Current Challenges and Opportunities to Enhance Quality of Care and Patient Safety
Supplemental Material for Healthcare Professional’s Perspectives on Improving Dietary Supplement Documentation in the Electronic Medical Record: Current Challenges and Opportunities to Enhance Quality of Care and Patient Safety by Zachary O. Kadro, ND, MPH, Aisha Chilcoat, ND, MPH, Jacob Hill, ND, MS, Stephanie Kenney, PharmD, Catharine Nguyen, PharmD, Elana Post, PharmD, Amanda H. Corbett, PharmD, Gary N. Asher, MD, MPH, and Keturah Faurot, PhD, MPH, PA in Global Advances in Integrative Medicine and Health.
Supplemental Material
Supplemental Material - Healthcare Professionals’ Perspectives on Improving Dietary Supplement Documentation in the Electronic Medical Record: Current Challenges and Opportunities to Enhance Quality of Care and Patient Safety
Supplemental Material for Healthcare Professionals’ Perspectives on Improving Dietary Supplement Documentation in the Electronic Medical Record: Current Challenges and Opportunities to Enhance Quality of Care and Patient Safety by Zachary O. Kadro, ND, MPH, Aisha Chilcoat, ND, MPH, Jacob Hill, ND, MS, Stephanie Kenney, PharmD, Catharine Nguyen, PharmD, Elana Post, PharmD, Amanda H. Corbett, PharmD, Gary N. Asher, MD, MPH, and Keturah Faurot, PhD, MPH, PA in Global Advances in Integrative Medicine and Health.
Footnotes
Acknowledgements
The authors would like to thank Kelly Eason from the UNC Program on Integrative Medicine for her role in management of the interview transcripts.
Author Contributions
Concept and design: Faurot, Corbett, Asher, Hill
Acquisition, analysis, or interpretation of data: All authors
Drafting of the manuscript: Kadro, Faurot, Chilcoat, Kenney, Hill
Critical revision of the manuscript for important intellectual content: All authors
Statistical analysis: Kadro, Faurot
Qualitative analysis: Kadro, Faurot, Chilcoat, Kenney
Obtained funding: Asher, Hill.
Administrative, technical, or material support: Faurot, Corbett, Asher.
Supervision: Faurot, Asher, Corbett.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported through # 2KR1151904, NC Translational and Clinical Sciences Center (NCATS). We acknowledge the data management assistance of the NC Translational and Clinical Sciences (NC TraCS) Institute, which is supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health (NIH), through Grant Award Number UL1TR002489. The authors would also like to acknowledge funding from UNC Family Medicine Innovation Award Funding. Drs Chilcoat, Hill, and Kadro were supported by the National Center for Complementary and Integrative Health National Research Service Award (NRSA) Institutional Research Training Program (T32) at University of North Carolina, grants (T32-AT003378), 5T32AT003378-13, 5T32AT003378-14, and 5T32AT003378-15.
Ethical Statement
Supplemental Material
Supplemental material for this article is available online.
Data Availability Statement
Deidentified data from this study are available upon request from the corresponding author subject to a data use agreement with the University of North Carolina at Chapel Hill.
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.