
Abstract
Introduction:
Pharmacists play an essential role as part of the multidisciplinary transplant team in providing comprehensive pharmaceutical care for kidney transplant recipients.
Methods:
A prospective, observational, single-centre study evaluated the clinical pharmacy service in a kidney transplant ambulatory clinic. At each visit, pharmacists reviewed and optimised the medication regimens of transplant recipients, which include the medication therapy management of immunosuppression, infective and non-infective complications commonly seen post-transplantation. Pharmacists also performed medication reconciliation and provided medication education during each visit. Any drug-related problems or discrepancies identified were communicated to the physicians in the clinic.
Results:
Between September 2013 and March 2015, a total of 3581 cases were reviewed. Pharmacists identified 663 drug-related problems involving 319 recipients. Most of the pharmacists’ clinical recommendations (93%) were accepted by physicians. The common drug-related problems identified were ‘inappropriate dosage regimen’ (38%), ‘omission of drug therapy’ (28%) and ‘monitoring parameters recommendation’ (9%). Common drug classes involved were immunosuppressive agents (25%), anti-infectives (14%) and anti-hypertensive agents (12%). During medication reconciliation, pharmacists identified 180 medication discrepancies. Common medication discrepancies identified include ‘incorrect dose’ (68%), ‘incorrect duration’ (17%) and ‘incorrect drug’ (13%). All drug-related problems and medication discrepancies were resolved or addressed at the same clinic visit.
Conclusions:
Pharmacists play a pivotal role in the provision of medication therapy management to ensure safe and effective use of medications in kidney transplant recipients with complex medication regimens. This was achieved through identification and resolution of drug-related problems from medication review and medication discrepancies from medication reconciliation.
Introduction
The medication therapy regimen for kidney transplant recipients (KTRs) is increasingly complex as they require life-long immunosuppressive agents to prevent organ rejection and concomitant medications for management of pre-existing or newly diagnosed disease states such as hypertension, hyperlipidaemia, diabetes mellitus, osteoporosis, infections and malignancies. KTRs may require a median of eight medications in the immediate post-transplant period and some KTRs may require 10–15 medications in the long term. 1 Some of these medications have narrow therapeutic windows, high risk for drug-drug interactions requiring therapeutic drug monitoring and multiple dosage adjustments. These factors in addition to polypharmacy increase risk for developing adverse drug effects, medication non-adherence and drug-related hospitalisations which may negatively impact graft and patient survival.2–4 These issues indicate the need for continual close monitoring and review of the medication regimens for this special population. The United States Organ Procurement Transplant Network (OPTN) recognised the importance of pharmacist involvement in the care of solid organ transplant patents and mandates that each transplant centre should have a designated transplant pharmacist to provide oversight of the medication management of all solid organ transplant recipients. In the published OPTN bylaws: ‘Each transplant program should identify at least one Clinical Transplant Pharmacist on staff who will provide pharmaceutical expertise to transplant recipients. The Clinical Transplant Pharmacist should be a member of the transplant team, providing comprehensive pharmaceutical care to transplant recipients.’ 5
In September 2013, the Singhealth Transplant Centre was opened to provide outpatient medical care for more than 800 KTRs after kidney transplantation. KTRs receive medical care from a multidisciplinary team, which comprises physicians, nurses, transplant co-ordinators and allied health professionals. Transplant pharmacists are members of the multidisciplinary team. A designated transplant pharmacist is available in the centre on weekdays to provide clinical pharmacy services. The clinical pharmacy activities include (i) review medication orders to identify, prevent and resolve drug-related problems (DRPs), (ii) perform medication reconciliation to obtain accurate drug administration by KTRs, (iii) optimise pharmacotherapy based on past medical history, medication records and laboratory results, (iv) provide therapeutic recommendations to physicians, (v) counsel KTRs to increase their knowledge on drug treatment, (vi) provide drug information for health care professionals and (vii) monitor and report adverse drug reactions.
The purpose of this study was to evaluate the clinical pharmacy service in a post-kidney transplant ambulatory clinic in Singapore General Hospital. The study aimed to (i) document the number and categorise DRPs identified by the transplant pharmacists in the transplant centre; (ii) document the number and categorise medication discrepancies identified during medication reconciliation; and (iii) evaluate the rate of acceptance of the therapeutic recommendations provided by the transplant pharmacists.
Methods
This was a prospective, observational study conducted in Singapore General Hospital from September 2013 to March 2015 to evaluate the clinical pharmacy service in a post-kidney transplant ambulatory clinic. At each visit, the KTR was seen by the transplant pharmacist after consultation with the physician. The transplant pharmacist at the clinic reviewed and optimised the medication regimens of the KTRs which include the medication therapy management of immunosuppression, appropriate anti-infective prophylaxis and management of comorbidities such as diabetes, hypertension and hyperlipidaemia. The transplant pharmacist also performed medication reconciliation with the KTRs and provided medication education during each visit. A DRP is ‘an event or circumstance involving drug therapy that actually or potentially interferes with desired health outcomes’ as defined by the Pharmaceutical Care Network Europe Foundation. 6 A medication discrepancy is any difference between the medication use history or the intended medication order and the medication order in the prescription.
Any DRPs or medication discrepancies identified during the consultation were discussed with the physicians-in-charge at the same clinic visit and they were either resolved or resulted in actions taken to address the specific issues. All DRPs and discrepancies were documented in the electronic medical record. The outcomes of the recommendations, namely ‘accepted’, ‘accepted with modification’ and ‘not accepted’, were also documented.
All DRPs and medication discrepancies documented at the clinic from September 2013 to March 2015 were retrieved from the system for analysis. DRPs were categorised according to ‘omission of drug therapy’, ‘no indication for drug ordered’, ‘therapeutic duplication’, ‘improper drug selection’, ‘therapeutic substitution’, ‘inappropriate drug dosage regimen’, ‘avoidance of adverse drug event’, ‘drug interaction’, ‘monitoring parameters recommendation’ and ‘non-adherence’. These DRP categories were adapted from Strand criteria and American College of Clinical Pharmacy guidelines for therapeutic interchange.7,8 Medication discrepancies were categorised according to ‘incorrect drug’, ‘incorrect dose’, ‘incorrect frequency’ and ‘incorrect duration’. The drugs involved in the DRPs and discrepancies were analysed according to their therapeutic classes.
Results
A total of 1271 KTRs accounting for 3581 reviews were performed by transplant pharmacists from September 2013 to March 2015. Transplant pharmacists identified a total of 663 DRPs and 180 discrepancies in approximately 24% of the reviews performed during the study period. Of the overall recommendations addressing DRPs and discrepancies, 753 recommendations provided by transplant pharmacists were accepted by the physicians, and 33 recommendations were accepted with modifications translating to an overall acceptance rate of 93%. The DRPs identified were ‘inappropriate dosage regimen’ (38.3%), ‘omission of drug therapy’ (27.9%), ‘monitoring parameters recommendation’ (9.2%), ‘no indication of drug ordered’ (7.2%), ‘avoidance of adverse drug event’ (6.8%), ‘non-adherence’ (5.1%), ‘therapeutic substitution’ (2.4%), ‘improper drug selection’ (1.7%), ‘therapeutic duplication’ (0.9%) and ‘drug interaction’ (0.5% ) as presented in Figure 1. From the medication reconciliation performed with the KTRs, transplant pharmacists identified 180 medication discrepancies. The medication discrepancies (Figure 2) that were identified include ‘incorrect dose’ (67.8%), ‘incorrect duration’ (17.2%), ‘incorrect drug’ (12.8%) and ‘incorrect frequency’ (2.2%). An analysis on the drug classes implicated in the recommendations was performed and they are presented in Figure 3; the three most common drug classes involved were immunosuppressive agents (25.3%), anti-infectives (14.1%) and anti-hypertensive agents (12.0%). All DRPs and medication discrepancies that were identified by the transplant pharmacists during consultation were discussed with the physicians-in-charge at the same clinic visit and they were either resolved or resulted in actions taken to address the specific issues.

Distribution of drug-related problems (DRPs) identified during medication review (n = 663).
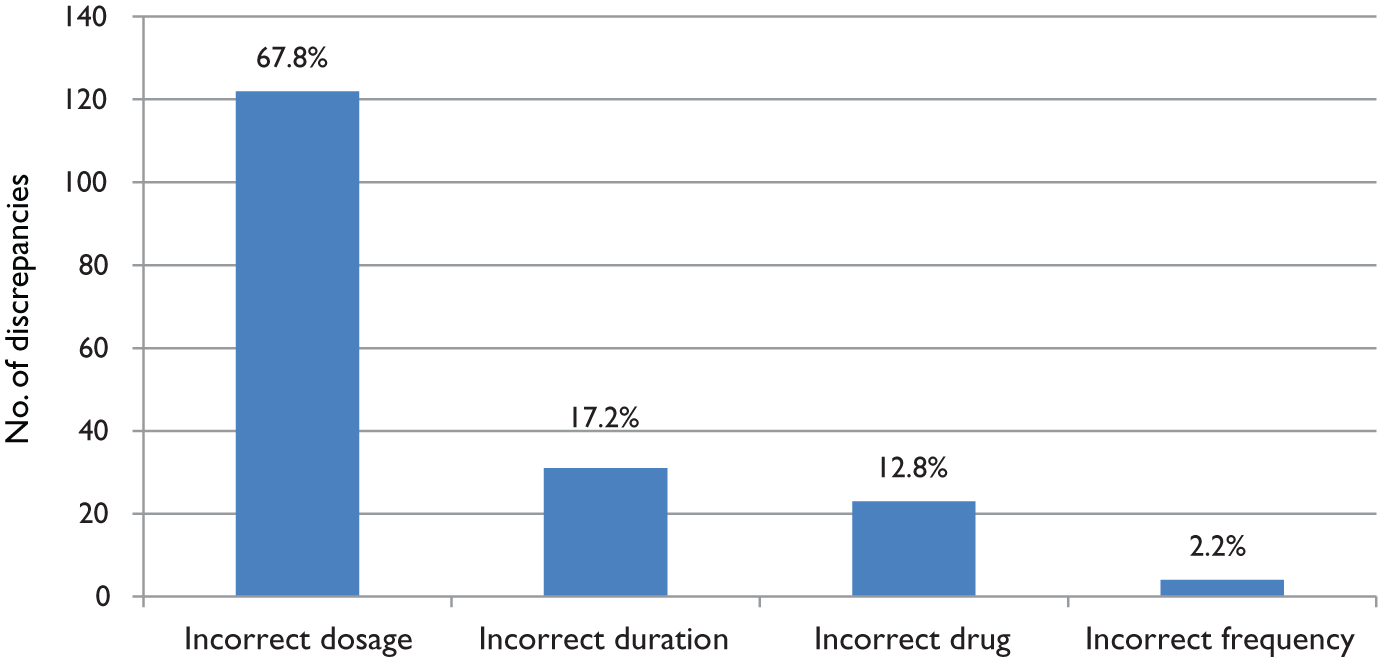
Distribution of medication discrepancies identified during medication reconciliation (n = 180).
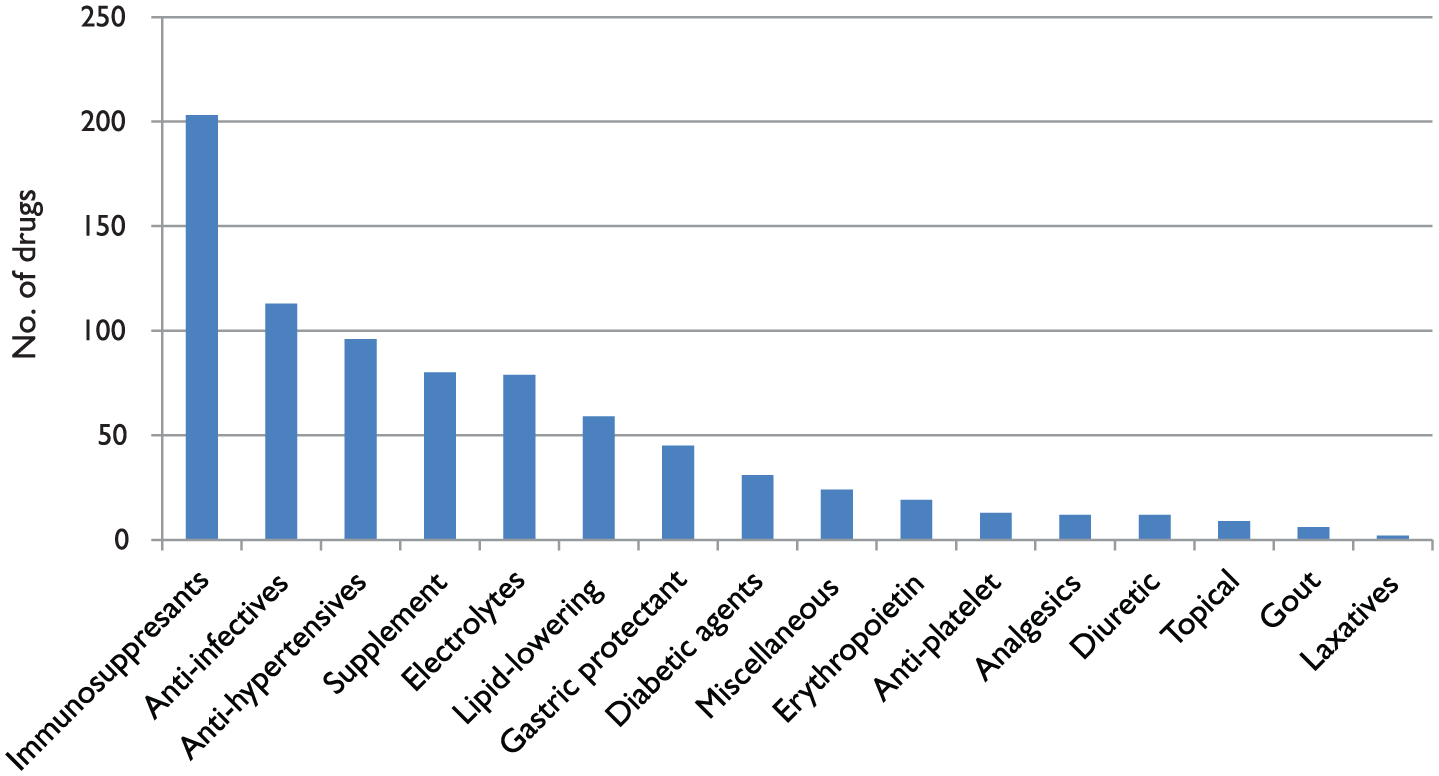
Drug classes involved in drug-related problems (DRPs) and medication discrepancies.
Discussion
Transplant pharmacists have been recognised as a valuable member of the multidisciplinary team in the care of solid organ transplant recipients. Several reports have highlighted the positive impact of transplant pharmacists in the ambulatory transplant clinics.3,9,10 Chisholm et al. 3 reported an overall pharmacists’ recommendation acceptance rate of 96% by physicians. Most of the recommendations they reported addressed issues on untreated indication, over-dosage and subtherapeutic dosage. These reported results were similar to those observed in our study, which reported an overall acceptance rate of 93% by our physicians. The two most common DRPs identified in our study were inappropriate dosage regimen and omission of drug therapy, which were similar to those in other studies.3,9,10 From our analysis, the most common DRP identified was inappropriate dosage regimen involving mainly immunosuppressive agents and anti-infectives. During the immediate post-transplant period, transplant pharmacists made multiple dosage adjustments for immunosuppressive agents to achieve their desired target therapeutic level. Similarly, multiple dosage adjustments of anti-infectives were required in view of changing renal function in KTRs as the anti-infectives used were mainly eliminated by the kidneys. Omission of drug therapy is the second most common DRP identified through medication review. The three most common drug classes involved in omission of drug therapy were anti-infectives, diuretics and electrolyte supplements. Prophylaxis against opportunistic infections is an important consideration in KTRs but KTRs require different anti-infectives for varying durations based on their risk profile, which was likely to lead to physicians omitting appropriate anti-infectives when required. During the immediate post-transplant period, KTR often have fluid and electrolyte imbalances due to their changing renal function, as such they do require diuretics and supplementation for electrolytes such as magnesium, potassium and phosphate to manage these issues. As KTRs require multiple courses of supplementation for the electrolytes, transplant pharmacists often suggest the need for repeated courses of supplementation to avoid the complications associated with electrolyte imbalances.
From the reports on clinical pharmacy services in KTRs, antihypertensive, antimicrobial and immunosuppressants were the most common medications accounting for the majority of the DRPs reported in KTR.3,11 Immunosuppressive agents are the most common drug class implicated in DRPs in our analysis, as they have a narrow therapeutic drug window requiring close monitoring and multiple dose titrations to achieve the desired target therapeutic level to maximise immunosuppression and minimise infections and adverse effects. Transplant pharmacists, who are equipped with the knowledge of pharmacokinetics and skills in dose titration of immunosuppressants, are in the position to utilise their clinical expertise in the management of immunosuppressive agents.
Anti-infectives for prophylaxis against opportunistic infections in KTRs are a standard part of their medication regimen. 12 Valganciclovir used for cytomegalovirus prophylaxis and co-trimoxazole for Pneumocystis jiroveci prophylaxis are eliminated by the kidneys, requiring dosage adjustment in KTRs with varying renal function. Hence transplant pharmacists play an important role in providing appropriate dosage adjustments for these anti-infectives to prevent under- or over-dosing.
Hypertension is a common comorbidity which affects more than half of the KTR population, sometimes requiring multiple anti-hypertensive agents. 13 Transplant pharmacists identified DRPs and discrepancies during medication reconciliation involving anti-hypertensive agents, where the dosages administered to KTRs were often lower than prescribed. The common reasons for the discrepancies were reported symptomatic hypotension or adverse effects such as pedal oedema with calcium channel blockers. Transplant pharmacists would educate KTRs on the management of hypertension including blood pressure monitoring, symptoms of hypotension, hypertension and appropriate titration of their anti-hypertensive agents.
In our analysis, non-adherence to medications in KTRs accounted for 5.1% of the DRPs. Transplant pharmacists identified non-adherence to medications during their consultation with KTRs and found out the reasons for non-adherence through their interview. The two most common reasons reported by KTR for medication non-adherence were adverse effects associated with drug therapy and lack of understanding on the indication of drugs. For KTRs who experienced adverse effects with their drug therapy, transplant pharmacists would highlight the issue to physicians and recommend either dose modification, change in drug therapy or symptomatic treatment for adverse effects if a causative drug was required. Transplant pharmacists would reinforce the need for drug therapy through patient education if a lack of understanding on the indication of drugs was identified.
For every recommendation, transplant pharmacists assigned a level of significance as ‘no significance’, ‘somewhat significant’, “significant’, ‘very significant’ or ‘extremely significant’. One limitation of our study is the lack of an expert panel to rate the level of significance for the recommendations independently; as such we did not report the level of significance for the recommendations in our study.
In conclusion, pharmacists play a pivotal role in the provision of medication therapy management to ensure safe and effective use of medications in kidney transplant patients with complex medication regimens. This was achieved through identification and resolution of DRPs from medication review; and medication discrepancies from medication reconciliation. Issues of medication non-adherence were also addressed through identification of reasons for non-adherence with strategies to overcome them and reinforcement of patient education.
Footnotes
Acknowledgements
This work was presented at the World Transplant Congress, 26–31 July 2014, at the Moscone West Convention Center, San Francisco, CA, USA.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.