
Abstract
Background
Acupuncture and yoga have both been shown to be effective in chronic pain. Underrepresented populations have poorer pain outcomes with less access to effective pain care.
Objective
To assess the feasibility of bundling group acupuncture with yoga therapy for chronic neck, back or osteoarthritis pain in safety net settings.
Methods
This was a feasibility pilot in Bronx and Harlem primary care community health centers. Participants with chronic neck, back or osteoarthritis pain received acupuncture and yoga therapy over a 10-week period. Participants received 10 weekly acupuncture treatments in group setting; with Yoga therapy sessions beginning immediately following the 3rd session. Primary outcome was pain interference and pain intensity on the Brief Pain Inventory (BPI); Outcomes were measured at baseline, 10-week close of intervention, and 24-week follow-up.
Results
93 patients were determined to be eligible and completed the baseline interview. The majority of participants were non-White and Medicaid recipients. 78 (84%) completed the intervention and 10-week survey, and 58 (62%) completed the 24-week post intervention survey. Participants received an average number of 6.5 acupuncture sessions (out of a possible 10), and 4 yoga sessions (out of a possible 8) over the 10-week intervention. Patients showed statistically significant improvements in pain at the close of the intervention and at a somewhat lesser rate, at 24-weeks post intervention. Challenges included telephone outreach and site coordination integrating acupuncture with yoga therapy. The trial also had to be stopped early due to the COVID-19 pandemic.
Conclusions
Bundling acupuncture therapy and yoga therapy is feasible for an underrepresented population with chronic pain in urban community health centers with preliminary indications of acceptability and benefit to participants.
Background
Estimates of chronic pain in the US adult population have ranged from 10-40% in relevant large surveys,1-4 with a documented association of impaired physical and psychological functioning5-7 and lost work productivity.8,9 Minority populations differ both in the prevalence and outcomes of chronic pain;10-13 wherein race/ethnicity and socioeconomic factors influence access to pain care.13-16 Opioids continue to be used for chronic pain with opioid addiction, and diversion and deaths remaining an ongoing epidemic in the US. 17 By the end of 2020, accelerated by the COVID-19 pandemic, opioid overdose deaths increased by over 35% from 2019. 18 Opioid fatalities are associated with lower socioeconomic status, 19 making access to non-opioid and nonpharmacologic pain care options a priority in underserved communities. Following the Consolidated Standards of Reporting Trials (CONSORT) guidelines, 20 this paper reports on a project examining the feasibility of a novel approach to chronic pain that combines group acupuncture therapy with yoga therapy delivered in the primary care setting to an underserved patient population. 21
Acupuncture therapy is effective for chronic pain conditions, 22 including chronic low back pain (cLBP),23,24 neck pain, 24 shoulder pain and knee pain from osteoarthritis.25-28 A large individual patient data meta-analysis (39 trials) of 20,827 patients with chronic pain found acupuncture to be significantly better than sham treatment or usual care, with only a 15% loss in treatment effect after 1 year. 25 Patients with more severe pain at baseline improved more from acupuncture treatment than those with lower levels of pain, compared to sham or non-acupuncture controls. 29 Acupuncture therapy is supported or recommended as part of comprehensive pain care by the U.S. Agency for Healthcare Research and Quality (AHRQ), 30 the U.S Food and Drug Administration (FDA), 31 the National Institutes for Health (NIH) 32 and the Joint Commission (TJC). 33 A retrospective claims-based study found initial visits to chiropractors, physical therapists or acupuncturists for new onset LBP substantially decreased early and long-term use of opioids. 34 Active military service members who accessed acupuncture for chronic pain had reduced risk of long-term adverse outcomes. 35
Acupuncture therapy - which includes palpation, the manual techniques Tui na and/or Gua sha, needling body points and needling auricular acupuncture points, and adhesive application of ear seeds for extended auricular therapy--is feasible and effective specifically for underrepresented populations at risk for health outcome disparities. 36 However, cost and access to individual acupuncture treatment continues to pose a barrier to widespread implementation in this patient population where insurance reimbursement rates remain low, and out-of-pocket expenses forbidding.37,38 To address these issues, group acupuncture, which is less costly, is being offered in many settings across the U.S. Evidence indicates that acupuncture delivered in a group setting is beneficial for chronic pain.37,39,40 Our ‘Acupuncture Approaches to Decrease Disparities in Outcomes of Pain Treatment (AADDOPT-2)’ trial compared 12 sessions of individual practitioner-patient acupuncture to group acupuncture (n = 706) 39 in the primary care setting in an underserved population demonstrated chronic pain reduction and improved function at 12 weeks in both arms. Qualitative studies to date show that acupuncture treatment in a group setting is highly acceptable to patients41-43 and that the group setting, community-based locations, and low cost of this model help eliminate some of the barriers to access. 40
Yoga therapy is an emerging healthcare profession 44 that includes the therapeutic application of attention/meditation (dhyana) and other mental practices, controlled breathing (pranayama), movement (vinyasa), physical postures (asanas), and applied philosophy/lifestyle. 17 Yoga therapy sessions differ from yoga classes in that they are delivered one-on-one or in small groups, include a thorough client intake, an individualized plan of care and ongoing assessment of progress. 45 Certified yoga therapists have training as yoga teachers (200+ hours) followed by additional specialized training (800+ hours) in clinical conditions, therapeutics, and integrative care.
Yoga practices demonstrate benefit for pain as well as pain-associated function 46 and disability, 47 in musculoskeletal pain disorders including back, neck, osteoarthritis, rheumatoid arthritis and fibromyalgia.48-50 Yoga has also been studied in underrepresented community settings,51,52 and was found to be non-inferior to physical therapy for cLBP in such patients. 52 The NIH recognizes the evidence for yoga, 32 and the AHRQ and American College of Physicians (ACP) recommend yoga for cLBP.30,53
In AADDOPT-2 39 we noted a natural progression for participants being treated with acupuncture therapy to begin to engage in more movement as their pain improved, and for acupuncturists to encourage activity and steps in movement recovery. Multiple studies and reviews have shown movement helps to reduce pain, improve function, and reduce frequency and intensity of chronic pain flare-ups. 54 We hypothesized that bundling acupuncture with an effective movement therapy may be an optimal progression for recovery. 21 Yoga therapy was chosen for this combined intervention for its contribution of movement practices, as well as its breathwork, mindfulness, and relaxation techniques that are well-aligned with acupuncture therapy and Chinese medicine principles, and relevant to chronic pain management. Broadly speaking, the model leveraged acupuncture to benefit function and reduce pain, together with yoga to provide a guided, therapeutic approach to movement; thus augmenting pain management and recovery with movement in a safe and sustainable way. No previous study has evaluated the combination of acupuncture and yoga therapy in patients with chronic pain, even though combining movement therapy with therapies like acupuncture has been an established model of rehabilitative care. 55 Both therapies are effective for chronic pain; both have been shown to be feasible in underrepresented populations.39,51,52 Given the need for patient activation in the context of chronic pain, yoga therapy combined with acupuncture therapy may offer a significant synergy for chronic pain management and recovery. We designed a pilot study to assess if it is feasible to provide these care options for this population at their primary care sites in the context of a study that could assess outcomes.
Methods
Study Design
Outcome Measures Data Collection Timeline.
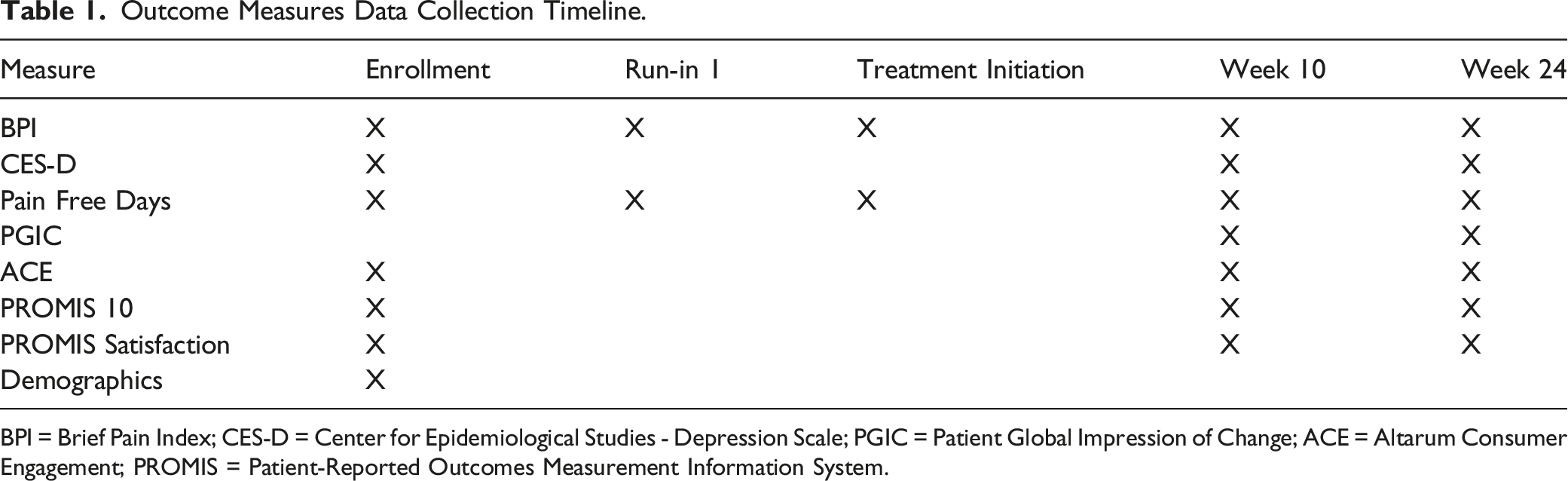
BPI = Brief Pain Index; CES-D = Center for Epidemiological Studies - Depression Scale; PGIC = Patient Global Impression of Change; ACE = Altarum Consumer Engagement; PROMIS = Patient-Reported Outcomes Measurement Information System.
Study Participants and Eligibility
Outpatients with chronic pain were receiving primary care at multiple Institute for Family Health (IFH) community health center sites in Manhattan and the Bronx, and two Montefiore Medical Group (MMG) sites in the Bronx: The Family Health Center and Williamsbridge Family Practice Center. Eligibility for participants included: • 21 years of age or older • Chronic pain (3 months or more in duration) due to a qualifying diagnosis of back pain, neck pain, and/or osteoarthritis. • Ability to provide consent in English or Spanish • Reliable phone contact • Availability for up to 10 weekly consecutive treatments and follow-up data collection up to 24 weeks.
Exclusion criteria were • Recent acupuncture treatment or yoga instruction/therapy in the 6 months prior to recruitment • Pregnancy • Severe psychiatric problems as assessed by the study team (e.g., chronic interpersonal problems, cognitive impairment or active psychosis that is uncontrolled by medication that precludes the ability to provide informed consent or complete the survey instruments).
Recruitment
Primary care providers at the IFH and MMG sites made referrals to the study team by paper referral or electronic medical record in-basket. Referring providers obtained verbal permission from the patient for a Clinical Research Coordinator (CRC) to contact them. The CRC confirmed patient eligibility and consent orally over the phone to be reviewed and confirmed in person. Participants did not receive an incentive to attend treatment sessions but did receive modest incentives to complete the research interviews. Participants were provided $25 for completing the enrollment interview, $5 for completing the Run-in 1 interview (and $5 for subsequent run-in interviews, if necessary), and $15 for completing the treatment initiation interview before the first intervention session. After the intervention, participants were provided $25 and $30 for completing study interviews at Week 10 and Week 24, respectively (Table 1 shows the interval of assessments).
Intervention
IFH patients received the intervention at the Family Health Center of Harlem, while Montefiore patients received the intervention at the two Bronx MMG sites. Treatment consisted of ten consecutive weekly group acupuncture therapy treatments described in detail in a previous design paper 21 and intervention manualization. 56 Yoga therapy treatments were started at week 3 and consisted of eight consecutive yoga therapy sessions that occurred immediately after acupuncture, in an adjacent room.
Usual Care
During the entire study, patients continued to receive usual care for management of chronic pain as provided by primary care providers. Usual care may include referral for specialty consultation or physical therapy, or use of medication, but does not typically include acupuncture or yoga services. We anticipated that patients would vary substantially in the duration and severity of pain and the specifics of the approach to pain management.
Acupuncture Therapy Component
During the intervention phase, each participant was given acupuncture therapy in a group setting (seated in a stationary chair) over 10 consecutive weeks. Direct practitioner/patient session time typically lasted 30-40 minutes. Session time could reach up to 60 minutes, to include time for the participants to arrive and settle in, as well as rest time after treatment. Sessions were shortened to as little as 15 minutes if participants were late to their scheduled treatment time. Three consecutive weekly sessions of acupuncture were given before yoga therapy was introduced. This allowed time for acupuncture therapy to reduce chronic pain severity, readying the participant to begin an active phase of movement and recovery provided by yoga therapy. Thereafter, patient appointments were arranged so that acupuncture treatment immediately preceded yoga therapy treatment on the same day.
Yoga Therapy Component
At week 2, a 20-25-minute yoga intake was conducted, following acupuncture therapy, to assess and inform a yoga plan of care. At week 3, that plan of care introduced the yoga therapy following the acupuncture therapy, so that week’s 3 through 10 were combined sequential interventions, as stated above. Participants’ yoga therapy sessions lasted 30-35 minutes, either individually or in dyads. To foster self-efficacy and sustained benefit, participants were further directed to practice at home via simple instructions both verbally and with handouts in patient’s preferred language of English or Spanish. Participants were guided in the yoga philosophy of mindful awareness and non-harming in order to avoid exacerbation of symptoms and ensure optimal safety in home practice.
Therapy Manualizations
Complex therapy interventions are developed for research using a consensus process also called ‘manualization’.57,58 Our acupuncture therapy was based on the pragmatic intervention manualization used in our AADDOPT-2 trial21,39,56 that allows for individualizing treatment from a pre-determined set of options adaptable to individual participant needs and in a group acupuncture setting. As acupuncture is rarely given alone, we intentionally incorporated detailed aspects of acupuncture practice to better reflect acupuncture care in real-world settings. 56 These included discussions with the participant on the history and nature of the chronic pain conditions as well as hands-on assessment and intervention. Approaches included palpation of regions of interest relative to the site of a chronic pain presentation, assessing for temperature, pain, responsivity to touch, Tui na to invigorate the body surface and regions of pain and Gua sha for inflammation and persistent or recurring focal pain. Acupuncture point options, and associated ah shi or trigger points, could be needled to obtain the de qi response with acupuncture needles then allowed to rest in place if elected. The strength of the de qi response was gauged to the patient. Either needle treatment or pressure (with affixed Vaccaria seeds) in the ear was included. A consensus-built pool of commonly used traditional acupuncture points was included for the study’s specific chronic pain problems.
A yoga therapy manualization process was then modeled on the above experience and resulted in a consensus approach for chronic pain in an underserved multi-morbid patient population. Yoga positions (asanas) from the low back pain trial 59 were incorporated along with specific asanas used in trials for upper body/neck pain 60 and for knee Osteoarthritis pain trials. 61 To balance the individualization of yoga practices that yoga therapy provides, along with the structure necessary for research study and replication, a list of practices most relevant to the clinical population was agreed on. Yoga therapists were free to choose from the selected practices within each category, beginning with breathing practices and adding new practices at each session as appropriate to the patients’ readiness and ability. These included multiple options in the following categories of stabilizing poses, mobilizing poses, breathing practices, relaxation, mental practices, and applied philosophy. All practices could be tailored for individual needs and preferences, using yoga props (blocks, straps, pillows), chairs, the wall, or general pose variations. During and at the end of the study we encouraged participants to utilize the practices learned as part of self-management options on their own and in the context of accessing a public yoga class and modifying practices to their own needs.
Outcome Measures
Feasibility was assessed by examining study participant recruitment, compliance of the participants with the treatment protocol, and completion of pain outcome instruments. This was measured through referrals to the study from providers, acupuncture and yoga treatment attendance, and percentage assessments completed. Threshold for referrals was identified as 300; acupuncture session average threshold was 5 sessions, and yoga session average threshold was identified at 3. Minimum percentage survey completion 10-week interview (our primary outcome) was 80%. Minimum thresholds were based on our previous studies.36,37,39 The assessment of the pain outcome measures was also an integral part of our study design to assess feasibility for a larger pragmatic effectiveness trial. The primary treatment outcome was pain interference and pain intensity. Secondary treatment outcomes were pain free days, depression, functional status, patient activation, and pain medication utilization. 21 These measures were used during the pre-intervention phase, during which patients were receiving usual care only, and compared to the period after patients receive the combined acupuncture and yoga sessions. Data was collected for 10 days before acupuncture and yoga therapy, at 10 weeks post intervention initiation and at 24 weeks following the end of treatment (see Table 1, below). The multiple pre-measurement points over a ten-day run-in period allowed us to document and monitor any variable patterns of pain pre-intervention. Patient socio-demographic measures were taken at enrollment. Adverse events associated with acupuncture treatment and/or yoga sessions, both serious (deaths, illnesses leading to hospitalization) and minor, were tracked and reviewed monthly. Any serious adverse effects were to be reviewed by a designated Data Safety Monitor.
Primary Treatment Outcome Measures
The Brief Pain Inventory: Short Form (BPI) 62 provided the BPI subscales on Pain Severity and Pain Interference. The BPI is a nine-item measure that asks patients to indicate how their pain influences function: select aspects of their everyday life including mood, walking, sleep and their ability to work over the past 24 hours, as well as the level and intensity of pain. The measure was adapted for use by phone, modifying a question which asks participants to refer to a diagram of the body. Intervention responsiveness was defined as a 30% or greater improvement from baseline in pain interference and pain severity in keeping with a commonly used threshold for clinically important change in pain. 63
Secondary Treatment Outcome Measures
Secondary measures included Center for Epidemiological Studies - Depression Scale (CES-D), 64 the Altarum Consumer Engagement (ACE), 65 the Patient-Reported Outcomes Measurement Information System (PROMIS 10) measure,66,67 the PROMIS Satisfaction with Participation in Social Roles measure, 68 the Patient Global Impression of Change (PGIC), 69 and medication utilization. Pain Free Days was also collected, which is a self-report measure that has been used in previous pain research, 37 indicating the number of pain free days in the previous 2 weeks.
Data Analysis
Sample Size Calculations
Using an alpha of .05, two tailed, a power of .80, and a clinically meaningful change defined as a 30% improvement on the BPI, we estimated that we needed approximately 134 participants treated through the GAPYOGA trial. To account for attrition we based our assessment on the AADDOPT-2 trial where we had complete data at 12 weeks for 84% of the participants. Therefore, for this trial we planned to recruit 150 participants. That said, on March 13, 2020, due to the onset of the COVID pandemic, recruitment and intervention for our study was terminated, with an enrollment of 93; as a result, our power was reduced to 74%.
Quantitative Analysis
Prior to any univariate or multivariate analysis, all data was reviewed to make sure values were in range and that outliers did not reflect typographical or data entry problems. Missing responses for any index measure were imputed using the average values from completed measures within the same index. Data was described univariate at baseline, 10 weeks and 24 weeks to assess loss to follow-up. Each primary and secondary outcome, pain interference and pain severity, were examined separately using repeated measures t-tests.
Results
Retention, Feasibility and Engagement
Demographics at Baseline, 10 Weeks and 24 Weeks.

Primary Outcomes
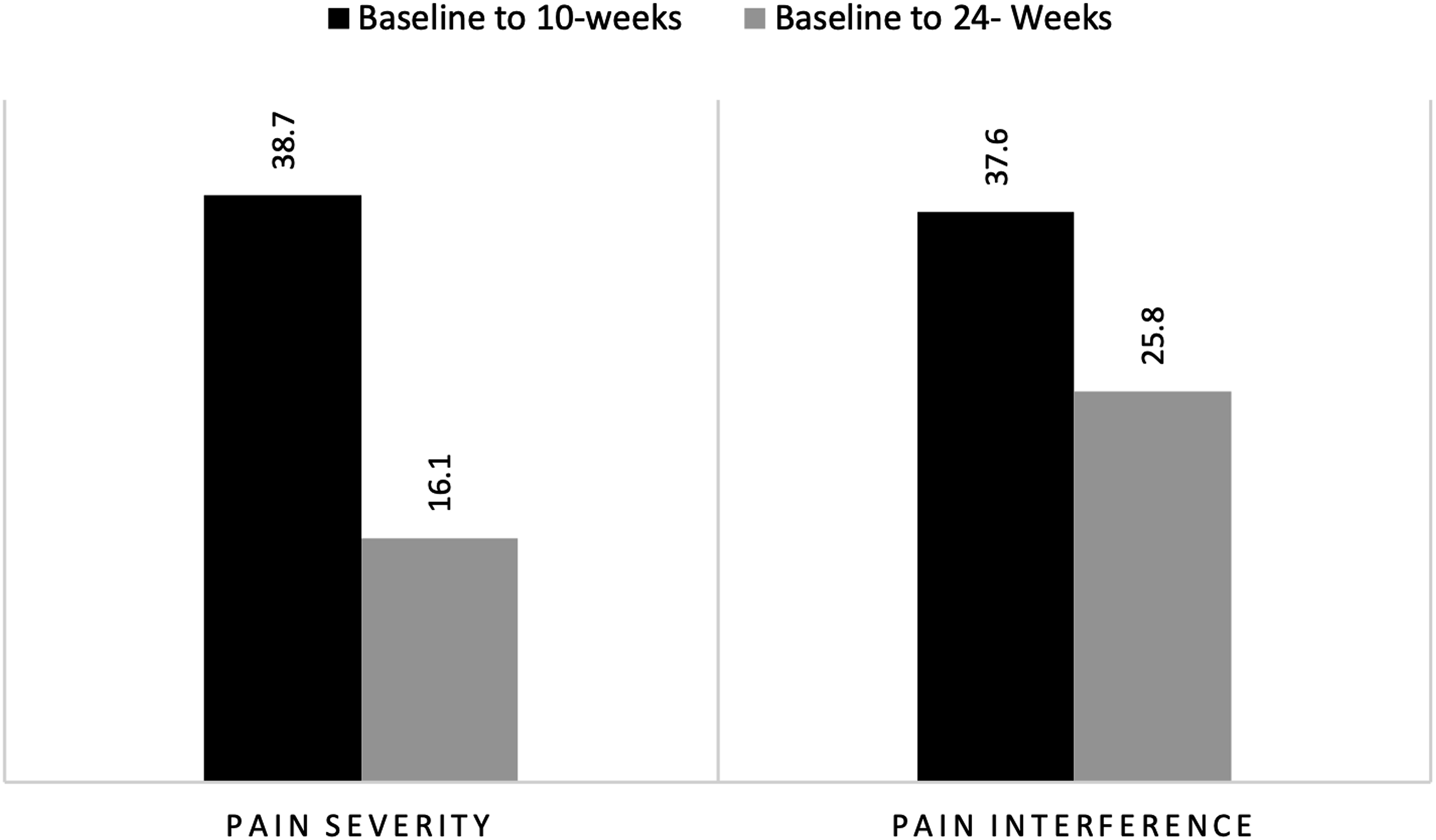
Both pain interference and pain severity show statistically significant improvement from baseline to 10-weeks (mean difference -2.1, P < .01) and baseline to 24-weeks (mean difference −1.62, P < .01) (Figure 1). Improvement was strongest from baseline to 10-weeks, at the close of the intervention. While improvement diminished somewhat at 24-week post intervention, significant improvement was maintained. In regard to pain responsiveness, using a 30% decrease as the benchmark for clinically meaningful improvement, at the 10-week end of intervention period, over one-third of the patients showed a 30% or greater improvement in both pain interference (37.5%) and pain severity (38.7%) (See Figure 2). At the 24-week follow-up, this proportion decreased to 25% for pain interference and 16% for pain severity. Mean Changes in Primary and Secondary Outcomes. * Significant improvement baseline to midpoint (10 weeks) and baseline to endpoint (24 weeks); ** Significant improvement baseline to midpoint; *** Significant baseline to endpoint (all assessed at P < .05). Proportion of Patients improving by 30% or Better.
Secondary Outcomes
Pain-free days and general pain showed a similar pattern of greatest improvement at 10-weeks with a reduction of effect at 24-weeks but still maintenance of significant improvement from baseline. Average pain and patient impression of physical change (PCIG Physical) showed significant improvement from baseline to the 10-week term of the intervention. However, by 24-weeks these improvements nullified. The patient impression of mental change (PCIG Mental), and engagement (ACE inform) showed no significant improvement at 10-weeks, but at the 24-week follow-up these showed significant improvements from baseline. The PROMIS 10 and PROMIS Satisfaction showed no significant change over the study period.
Adverse Events
There were no serious events during the course of this study. There were four minor adverse events: dizziness during an acupuncture session, retained needle from acupuncture (but discovered by yoga therapist), worsening of leg pain attributed to acupuncture by the participant, and dizziness and weakness after intervention attributed by participant to intervention. Our experience is in line with the safety literature for acupuncture therapy70,71 and yoga.72,73
Discussion
Combining and individualizing beneficial therapies as part of chronic pain rehabilitation is an established feature of comprehensive, multidisciplinary pain care.74-76 In our study we aimed to leverage the decreased pain from acupuncture and then build upon it together with yoga therapy - addressing not only the chronic pain but also initial barriers to movement that chronic pain can entail. Bundling acupuncture therapy and yoga therapy is feasible for underrepresented population with chronic pain in urban community health centers with indications of acceptability and benefit to participants. Participants completed an average of 6.5 acupuncture and 4 yoga sessions, above our average thresholds, again demonstrating engagement and commitment to the intervention in this patient population. Further supporting feasibility in primary care, we found that providers at these safety net health centers readily referred patients with chronic pain for this intervention. Referrals to the study numbered 467, above our threshold. Significant improvement was seen in participants’ pain score at the end of the intervention, especially in pain interference. In addition, though the degree of pain improvement declined at 24 weeks, there was only minimal ‘decay’, with statistical significance continuing for pain interference and pain free days. This improvement was evident despite the likelihood that the challenges of the pandemic in NYC—including social isolation, increased anxiety and financial strain—might have been expected to have a negative impact on outcomes.
A qualitative study done with these participants also confirmed feasibility and acceptability. 43 Participants reported through the study that the combined therapy helped their pain as well as improved their psychological well-being. Additional themes that emerged as well included a transformative healing process and the importance of the relationship with the acupuncture and yoga providers.
Comprehensive pain care strategies include not only implementation of effective modalities 17 but aim to maximize their benefit through optimal combinations and bundling of care.77,78 Yoga and acupuncture therapy have inherent similarities. Both provide patients with counsel on self-care, e.g., breathing techniques to mitigate pain. Acupuncture therapy encourages participant movement as part of chronic pain recovery; Yoga not only offers specific movement strategies for pain management, but also utilizes non-movement practices that can impact pain processing, emotions associated with pain, and the impact of pain on daily life e.g., breathing, visualization techniques, and relaxation practices.
The distinction between a yoga class and yoga therapy is important to highlight here. Yoga therapy involved selection of specific movements important for strengthening and improving range of motion, maintaining gains, and promoting participant activation. Yoga therapy tailors movement to each person’s needs which can be delivered individually or in small groups and designed to accommodate differently-abled participants who may not feel safe or included in a general yoga class. The therapeutic application of yoga practices is not new, but clarification of yoga therapy as a healthcare profession in Western contexts has emerged in recent decades.
Yoga therapy instructors have advanced training to work with clinical populations and are most likely to provide safe and appropriate yoga practices for patients with chronic pain. While their services may initially be more expensive than standard yoga classes, the practices can then be continued independently at home. Our yoga intervention was not intended to create a reliance on expensive yoga services, but to empower patients to use yoga in daily life as self-care. There was an emphasis on incorporating small simple practices into existing routines. Prior research has demonstrated long-term effects from a yoga intervention beyond the treatment period when development of home practice is emphasized. 61 Yoga therapy is spreading rapidly worldwide and promises to add significantly to the long-term picture for comprehensive pain care.
Limitations
Factors associated with implementing bundled therapies at health centers that care for underserved populations are discussed in a separate paper. 79 Study challenges included difficulty reaching lower socioeconomic participants by telephone during recruitment, and site coordination to integrate group acupuncture with yoga therapy. In addition, the COVID pandemic caused the study to be stopped early before full recruitment could be achieved. The pandemic may also have added to difficulties in obtaining follow-up assessments at 24-weeks because of the overall disruption in participants’ lives during that time. Our study did not have a control group and so we could not assess whether the addition of yoga to acupuncture definitively added to treatment effect, i.e., provided synergy. Lastly, we were not able to assess feasibility associated with cost. However, even in the face of these limitations we did see significant improvement in our primary outcome measures. Lessons learned bundling care will help to inform the design and methodology of a larger pragmatic trial.
Conclusion
Access to nonpharmacologic pain care is minimal in low-resource medical centers; medical providers are seeking effective pain care options in light of the opioid crisis and welcome the ability to refer for effective nonpharmacologic options. Group acupuncture therapy was effective in our previous trial and was highly acceptable to patient participants as well as medical providers who referred patients. 39 Yoga therapy is also beneficial for chronic pain. Combining these therapies also appeared to be highly acceptable to both referring providers and patient participants. In addition, bundling these therapies at a participant’s primary care site may offer significant access benefit for patients. Further study in combining acupuncture and yoga therapy for chronic pain is warranted.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Footnotes
Author Contributions
AN, BJA, MDM, BK were investigators on AADDOPT-2 group acupuncture trial and part of original GAPYOGA design team; DMM was a research acupuncturist for AADDOPT-2; RT, SM, EW, DMM and MM joined team in transition to the pilot. SM worked with yoga team to develop yoga therapy manual. PM joined team as site co-PI for Montefiore. AN, RT, BK are responsible for article draft; each author reviewed and edited article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Private Philanthropy. Funders have no role in study design or data collection, management, analysis, or interpretation, writing of report or any study activities.
Ethical Statement
Clinicaltrial
Clinicaltrials.gov # NCT04296344.