
Abstract
Good health literacy enables individuals to look after their health and wellbeing. However, deaf adults are seven times more likely to experience poor health literacy than their hearing counterparts, leading to poorer health outcomes. To improve health literacy levels in the deaf community, researchers emphasise the need for deaf children to access health-related information. When a child attends health care appointments, a qualified sign language interpreter is therefore essential. However, interpreting in this environment is a complex phenomenon. This qualitative study adopts an emic perspective to explore the challenges encountered by interpreters and some of the strategies adopted. Ten registered sign language interpreters with experience of working with deaf children in health care settings were selected to be involved in the research. Semi-structured interviews were carried out with each participant, and reflexive thematic analysis was used to identify themes in the data. This study illustrates that, in addition to linguistic skills, an interpreter needs to possess interpersonal skills to conduct themselves in a professional manner and work in collaboration with the health care practitioner, child, and parents. In addition, the research shows that in this environment, interpreters may experience intrapersonal demands, highlighting the need for them to manage their emotions and look after their own wellbeing.
1. Introduction
In a child’s health care appointment, health care practitioners (HCPs) often face challenges as they endeavour to communicate in a way that meets the needs of both parents and child (Damm et al., 2015). As Bell and Condren (2016) acknowledge, the way HCPs communicate with children requires particular attention. In the United Kingdom (UK) the General Medical Council (GMC, 2024) produced guidance to support practitioners in communicating with children under the age of 18, following which this study defines a “child” as a person under the age of 18. The guidance emphasises that HCPs must consider parents views, but they also have a responsibility to talk to the child to understand their feelings and concerns, thereby supporting collaborative, child-centred decision-making (Ong et al., 1995; United Nations, 1989). To act in the best interests of the child and promote their long-term health and wellbeing, HCPs, children and parents must communicate effectively (Silverman et al., 2013).
The National Deaf Children’s Society (NDCS, 2014) reports that deaf children often experience communication barriers during health care appointments, and struggle to express themselves effectively. This has a detrimental effect on their health literacy and long-term health (Sign Health, 2014). Researchers advocate that sign language interpreters should be provided for their health care appointments (Heap et al., 2020; Hedding & Kaufman, 2012). However, only 7% of interpreters report regularly working with deaf children in health care settings and just over 40% report doing so occasionally (Mapson et al., 2019). The reason why only a relatively small number of interpreters work with deaf children in health care settings has not been explored; however, of the ones that do, the NDCS (2014) reports that many interpreters do not possess the necessary skills to interpret these interactions effectively.
Interpreting in health care settings is complex (Hale, 2007), with added challenges when the patient is a child (Crezee, 2013). However, interpreter-mediated interactions involving children remain under-researched (Lombardi, 2023; Nilsen, 2021). This exploratory qualitative study adopts an emic perspective to examine the challenges interpreters face and the strategies they employ when working with deaf children. Drawing on 10 semi-structured interviews with registered sign language interpreters, it sheds light on the complexity of these interactions.
This article first reviews communication barriers that contribute to poorer health outcomes in the deaf community, highlighting the obstacles deaf children face in accessing interpreters and the importance of having one. It then introduces adult health care interpreting competencies as a foundation for exploring the additional skills required when working with children, their parents and the HCPs. Findings show that effective interpretation requires collaboration between the interpreter, the health care professional, the child, and the parents. The data also reveal the importance of interpreters managing intrapersonal demands (Dean & Pollard, 2013) and engaging in self-care.
1.1 The wider context
The barriers deaf children experience during childhood contribute to the poorer health outcomes experienced by the deaf community as a whole (Hedding & Kaufman, 2012). This section details the causes and manifestations of these experiences to illuminate the challenging situation in which health care interpreters work.
1.1.1 The importance of health literacy
Health literacy refers to the ability to comprehend health-related matters and understand how to look after one’s health and wellbeing (National Institute for Health and Care Research, 2022). The World Health Organisation (2022) highlights that improving health literacy empowers individuals to take preventive measures against lifestyle-related conditions and actively engage in health care consultations to make informed decisions with their HCP. Kyle and Shaw (2015) found that patients’ health literacy levels directly affect their ability to understand their choices regarding treatment. Although their study focuses on adults in orthopaedic settings, their findings highlight the broader connection between good health literacy and positive health outcomes. Conversely, poor health literacy can adversely affect a person’s health and wellbeing (Peerson & Saunders, 2009), with one study indicating that deaf people are seven times more likely to experience poor health literacy in comparison with their non-deaf counterparts (McKee et al., 2019). Consequently, the deaf community experiences poorer health than the wider population, with Sign Health (2014) reporting that in the UK the risk of a deaf person developing diabetes is quadrupled and they are twice as likely to suffer from high blood pressure. These disparities underscore the importance of accessible health education. However, deaf children often face barriers to acquiring this knowledge from an early age, which increases the complexity of interpreter-mediated health care interactions involving children.
1.1.2 Barriers to deaf children’s access to health-related information
Poor health literacy in adulthood often stems from limited health education in childhood (Hedding & Kaufman, 2012), a claim supported by Bell and Condren (2016), who emphasise that children need to learn about health matters in an age-appropriate manner, which empowers them to participate in their health appointments. However, many deaf children lack access to this information, which negatively affects their health literacy levels and overall wellbeing (Kushalnagar et al., 2018; Naseribooriabadi et al., 2017). For instance, Smith and Samar (2016) compared the health literacy of deaf and hearing children using a range of health-related assessments in their preferred language. Their findings revealed that deaf children’s health literacy levels were significantly lower than those of their hearing peers. Further validating these findings, Smith et al. (2015) employed a phenomenological approach to examine deaf children’s understanding of heart-related conditions and found notable gaps in their knowledge. These studies point to persistent inequalities in health knowledge acquisition.
Researchers argue that the disparities in health literacy arise from communication barriers experienced by deaf children from birth (Hall, 2017). Ninety-two percent of deaf children are born to hearing parents that do not sign (Mitchell & Karchmer, 2004). This often creates a linguistically inaccessible home environment, as illustrated by Meek’s (2020) phenomenological study, which described deaf individuals being excluded from family conversations. Whereas hearing children often acquire health-related knowledge incidentally in the home, deaf children are typically excluded from such learning (Pollard & Barnett, 2009). Furthermore, deaf children are often unaware of their family’s medical history, which can negatively impact their long-term health (Hedding & Kaufman, 2012). This aligns with the findings by Kushalnagar et al. (2020), who surveyed deaf and hard of hearing adults and identified a clear link between limited childhood communication and increased risk of chronic illness. Collectively, these findings confirm that early communication barriers are a significant contributor to poor health outcomes in the deaf community.
Since many parents cannot converse in sign language, deaf children are often deprived of language during their formative years (Gulati, 2018), which affects neurological development (Hall, 2017), educational outcomes and reading ability (Rogers et al., 2018). Protheroe et al. (2009) assert that a good command of English is essential for health literacy. Unfortunately, poor literacy levels mean that deaf children struggle to access written health information (Naseribooriabadi et al., 2017). Hence, in the UK the “Accessible Information Standard” (NHS England, 2017), stipulates that deaf people should receive health information in their preferred language, resulting in some general health information being available on websites such as “NHS inform” (NHS, 2023). However, language deprivation, can also limit comprehension (Crump & Glickman, 2011). This can be compounded by the way that online translations are presented. Pollard et al. (2009), for example, observe that information translated online is often presented in a monologue format, whereas sign language is a dialogic language, through which information is conveyed in a conversational manner. As a result, even translated content often remains inaccessible. The connections between the experience of deaf children and the poor health outcomes of the adult deaf population are clear, making childhood health interactions a key nexus for sharing health-related information in a clear and accessible way.
While sign language interpreters cannot directly address the systemic causes contributing to poor health literacy in the deaf community, research suggests that their presence in a deaf child’s health care appointment can support the child’s understanding of health-related matters (Hedding & Kaufman, 2012). However, although UK legislation such as the Equality Act (2010) stipulates that a sign language interpreter should be provided for health care appointments, in practice, deaf children are often not provided with this support (Hedding & Kaufman, 2012; NDCS, 2014). Instead, HCPs frequently rely on parents to facilitate communication (Heap et al., 2020). This occurs despite the Royal College of Paediatrics and Child Health (2025) stipulating that family members should not interpret their child’s appointment. Parents are often unsuited to the task as they generally lack the appropriate skills and understanding of medical terminology and concepts (Crezee, 2013; De Buhr & Tannen, 2020). For deaf children the problem may be compounded by the fact that over 90% of parents are unable to communicate in sign language (Mitchell & Karchmer, 2004). Consequently, deaf children report that they are unable to speak to their HCP effectively (NDCS, 2014), which impacts how they engage with any necessary treatment (Schofield & Mapson, 2014).
Despite assertions that a sign language interpreter should be provided to facilitate health care appointments (Heap et al., 2020), the mere presence of an interpreter does not guarantee equitable access for deaf children compared to their hearing peers. This may be because initial interpreting training focuses on linguistic competence, with interpreters trained as generalists (Dean, 2021). However, researchers argue that working in health care requires specialist training, not only in medical terminology, but in ethical reasoning and contextual knowledge, to support interpreters to align themselves with the values of the setting (Angelelli, 2004b; Crezee, 2013; Hale, 2007). In addition, because interpreters are active participants who have a bearing on the dynamics of the interaction (Angelelli, 2004a; Wadensjö, 1998) and the relationships between participants (Hsieh, 2013), they require good interpersonal skills (Llewellyn-Jones & Lee, 2014; Major & Napier, 2019). Interpreting a child’s health care consultation requires the interpreter to manage complex interpersonal demands (Dean & Pollard, 2013) between the child, the parents and the HCP (Nilsen, 2021), while communicating at an age-appropriate level for that child (Ackroyd & Wright, 2018) and considering the wider context (Dean & Pollard, 2013). However, this is rarely discussed in general interpreter training, which tends to focus on adult interactions and leaves interpreters underprepared to work in specialised domains (Dean, 2021).
1.2 Interpreter-mediated adult health care interactions
To better understand the unique challenges of interpreting for deaf children in health care settings, it is important to understand the demands involved in interpreting for deaf adults. Despite these studies focusing on adult interpreter-mediated interactions, their insights provide an important foundation to understand the additional challenges when the patient is a deaf child attending a health care consultation with their parents.
Effective communication is widely recognised as the foundation of a successful health care interaction, as obtaining and conveying accurate information is essential to ensure the patient receives appropriate advice or treatment (Silverman et al., 2013). When an interpreter facilitates a conversation in this setting linguistic accuracy is a primary concern (Robb & Greenhalgh, 2006). However, interpreting medical terminology accurately can be challenging (Crezee, 2013), especially when equivalent terms do not exist in the target language. In a simulated study of medical interactions between Chin-Hakha and English, Ching (2017) found, that interpreters employed various strategies to manage gaps in terminology, such as “borrowing” terms from another language or offering explanations. While the study only gained the interpreters’ perspective, similar strategies were identified in a qualitative research study by Major et al. (2012) with native Australian Sign Language (Auslan) users, which explored how Deaf users experienced the interpretation of medical terms into Auslan. Over half the participants expressed a preference for interpreters to convey the meaning of unfamiliar terms, rather than to fingerspell the word, which was the other strategy they identified interpreters using. This is perhaps unsurprising, as fingerspelling is derived from the English language (Sutton-Spence, 1999) and relies on the clients’ existing knowledge of the English word, which may be limited due to a poor understanding of health-related matters (Naseribooriabadi et al., 2017). While these studies offer insight into how interpreters may manage linguistic challenges, they do not discuss the interpersonal demands present in health care settings. In addition, due to language deprivation in childhood, some deaf adults are also dysfluent in signed language (Glickman & Hall, 2019). Crump and Glickman (2011) offer valuable guidance on how interpreters can accommodate this dysfluency, outlining various strategies including interpreting consecutively, using drawings or objects, and interpreting in the third person. Notably, they strongly advocate for sign language interpreters to work alongside deaf interpreters in these interactions. Although their study focuses solely on mental health, the principles offer an important foundation and highlight a gap in understanding about how interpreters manage language dysfluency in broader health care contexts such as appointments involving a child.
Beyond terminology, interpreters must navigate interpersonal demands that are central to Angelelli’s (2004b) ethnographic study. She analysed over 300 medical encounters, demonstrating that interpreters are active participants in health care interactions and their behaviour and decisions significantly influence interpersonal dynamics and health outcomes. This includes working collaboratively with the HCP, managing turn-taking, and considering the power dynamics within the consultation. Hale (2007) further reinforces this through her comprehensive analysis of community interpreters, including those in health care, noting that interpreters must manage various demands, such as the time constraints of a consultation, cultural misunderstandings and the limited awareness some HCPs have of the interpreter’s role. Both Angelelli and Hale demonstrate how health care interpreting requires a combination of linguistic expertise, ethical judgement, interpersonal skills and adaptability to promote effective communication. The Demand Control Schema (DC-S) (Dean & Pollard, 2013) offers a valuable framework for navigating these complexities. It encourages interpreters to make decisions based on teleological principles by considering the situational demands and evaluating their control, or strategy, options based on their likely consequences and whether these align with the goal of the environment (Dean & Pollard, 2018).
1.3 Interpreter-mediated child health care interactions
Although limited studies focus specifically on interpreting for children in health care settings, research from educational settings offers valuable insights into the additional challenges interpreters face. For instance, Baraldi and Ceccoli (2023) conducted a qualitative research study in Italian primary schools, using audio recordings to assess interpreter-mediated communication between Italian teachers and the native language of the children and parents, which were Chinese, Arabic and Twi. Their findings revealed that power dynamics, shaped by interpreter conduct and parental dominance, can inhibit a child’s ability to express themselves. Although this research is not situated in a health care context, similar power imbalances arise where children may adopt a passive role (Damm et al., 2015). As a result, HCPs may direct their communication solely to parents, excluding the child from discussions (Lambert et al., 2010).
Building on findings from the educational setting, Baraldi (2025) analysed 11 audio recorded interpreter-mediated child health consultations between Italian clinicians and families from Albana, Tunisia, Egypt and Cote d’Ivoire, who spoke in their respective native languages. The study explored the complex interpersonal demands interpreters face, highlighting the need for HCPs to engage both the child and parents to understand the nature of the visit and obtain the child’s history. Baraldi notes that children may feel uncomfortable in health care appointments, and interpreters play a crucial role in supporting their engagement, managing turn-taking, and facilitating the child’s responses, which works in harmony with the overall environmental goal.
There is a limited amount of literature specifically on interpreting with deaf children. Lombardi (2023) interviewed two groups of interpreters, one group working in educational settings and the other in health care. Using simulated medical scenarios, the study examined how each group conveyed medical information to deaf children. The findings highlighted that health care interpreters were more familiar with medical terminology, while educational interpreters often checked for the child’s understanding and adapted their strategies accordingly.
Ackroyd and Wright (2018) conducted qualitative research in a specialist mental health care setting for deaf children. They emphasised that while interpreters must possess strong linguistic skills, they must also adapt their approach to meet the child’s needs. A key aspect of this study is that the interpreter participants worked regularly in this setting and engaged in pre- and post-session meetings with clinical staff, which afforded the interpreter time to prepare and also debrief to manage intrapersonal demands. Interpreting for children in mental health care settings was also the focus of a study by Zafirah et al. (2020). Their semi-structured interviews with interpreters revealed that they frequently encountered emotionally challenging situations, placing them at risk of compassion fatigue. Participants were encouraged to access support by means of supervision and engage in self-care. Although both studies focus on children’s mental health care, similar emotional demands may arise in other health care contexts, potentially resulting in vicarious trauma (Bontempo & Malcolm, 2012; Lai & Heydon, 2015; Lim et al., 2022; Macdonald, 2015). Collectively, these studies highlight that interpreting for children in health care settings requires all the competences expected in adult interactions, alongside the ability to convey information in a child-friendly manner. The DC-S framework (Dean & Pollard, 2013) can assist interpreters by encouraging them to consider the “thought world” of the child. By reflecting on the child’s perspective, interpreters can evaluate their control options and select the most appropriate strategy to meet the child’s needs and achieve the overall goal of the interaction.
The impact that the interpreter has on the dynamics of health care interactions and the emotions of those involved (Angelelli, 2004b; Hale, 2007; Wadensjö, 1998) can also impact the parents who are attending the appointment with the child. When deaf children are involved, hearing parents can feel emotionally vulnerable and uncomfortable (Harvey, 1982). Many hearing parents of deaf children have low parental morale and experience negative feelings about their child being deaf (Sealy et al., 2023), and this, coupled with the fact that most are unable to communicate effectively with their child (Rowley, 2021), might lead to feeling embarrassed or inadequate (Harvey, 1982), negatively impacting the interaction. There has been limited research exploring how an interpreter’s presence specifically impacts parents. However, applying the DC-S framework can support interpreters to consider the thought worlds (Dean & Pollard, 2013) of the parents and encourage interpreters to use their interpersonal skills to mitigate threats to “face” (Monacelli, 2009).
1.4 Challenges that occur when interpreters work with HCPs
For HCPs to communicate effectively with a deaf child, they need the support of an interpreter (Du Feu & Chovaz, 2014). Numerous authors have emphasised the value of the interpreter and HCP working together collaboratively (Angelelli, 2004a, 2004b; Swabey & Faber, 2012) and for the interpreter to be considered as part of the health care team (Ackroyd & Wright, 2018; Hsieh, 2007). Unfortunately, HCPs do not always consider interpreters as team members, possibly due to their lack of medical training (Moreland & Agan, 2012).
Further challenges can relate to the need for interpersonal connection between the HCP and the patient. In a child’s consultation, the different stages of a child’s development may present various challenges for HCPs (GMC, 2024); younger children may feel nervous about being in an unfamiliar environment, while older children may be reserved and reluctant to express themselves (Bell & Condren, 2016). To support the child to feel comfortable, HCPs endeavour to use their interpersonal skills to communicate with children of all ages effectively (O’Keefe, 2001). However, Du Feu and Chovaz (2014) assert that HCPs may feel that they lack the appropriate skills that are required to treat a deaf patient. Similarly, Schofield and Mapson (2014) note that the HCP could feel apprehensive in the presence of an interpreter. This apprehension may affect how they interact with the child and parents. A qualitative study of interpreter-mediated health care interactions by Theys et al. (2022) found that HCPs may not fully utilise their interpersonal skills in an interpreted interaction, leading to a negative impact on health outcomes. For an interpreter to work in harmony with the goal of the environment, it is essential that they support the HCP to feel comfortable in their presence. This can be achieved by the interpreter using their interpersonal skills to engage in “rapport management” (Spencer-Oatey, 2008), which forms the basis of a trusting and collaborative working relationship (Hsieh et al., 2010) with the clinician. The HCP may then feel more comfortable and able to focus on using their own interpersonal skills to engage with the child.
Some HCPs worry that their interpersonal skills and the manner in which they convey information may not be relayed in an interpretation (Pugh & Vetere, 2010). This is supported by Mapson and Major (2021) who indicate that when an interpreter is unfamiliar with the HCP’s intended aims, they tend to focus predominantly on the informational content rather than the “rapport-building techniques” the HCP displays. This can be alleviated when the interpreter and HCP work collaboratively, because the interpreter is aware of the clinician’s aims and objectives (Du Feu & Chovaz, 2014), allowing the interpreter to focus on the HCP’s interpersonal skills and convey them in the interpretation (Mapson and Major, 2021). In turn, this supports the patient to feel comfortable to share information, which enables the HCP to provide the correct advice or treatment (Silverman et al., 2013). Familiarity between the interpreter and the HCP is therefore seen as positive (Mapson and Major, 2021; Schofield & Mapson, 2014) with their existing relationship, or “latent network” (Watts, 2003) facilitating a collaborative working relationship. However, the personality of the interpreter is also likely to impact on the relationship and interactional dynamics (Bontempo et al., 2014).
In summary, this literature review outlines how deaf children often face barriers that hinder their health literacy levels and health outcomes (Hedding & Kaufman, 2012; Kushalnagar et al., 2018), highlighting the need for skilled interpreters that are competent in interpreting medical language in a manner that meets the need of the child and ability to manage complex interpersonal demands (Baraldi, 2025; Dean & Pollard, 2013; Lombardi, 2023; Nilsen, 2021).
This study addresses a critical research gap by examining sign language interpreters’ perspectives on the challenges and strategies involved in interpreting the complex interactions that comprise deaf children’s health care appointments.
2. Methodology
This qualitative study was designed and conducted within a constructivist paradigm underpinned by a relativist ontology (Lincoln & Guba, 2013). Our approach fits with our multiple identities (Breen, 2007) as both interpreters and researchers, and our emic perspective as interpreters who have also interpreted for children in health care settings. For an exploratory study such as this, we generated data through semi-structured interviews for multiple reasons. First, due to the inappropriateness of bringing additional adults or video cameras into children’s health care appointments for observational purposes, and the challenges involved in obtaining ethical consent, which were beyond the scope and timescale of this study. Second, because this type of interview is considered to be effective in generating broad perspectives around a professional adult’s perspective of working with children (Pyle et al., 2023). Third, due to their flexibility and suitability for novice researchers (Kvale & Brinkmann, 2014; Ruslin et al., 2022). Moreover, Braun et al. (2015) describe how thematic analysis, which we apply to our data, is a useful analytical tool for those new to research.
2.1 Participants
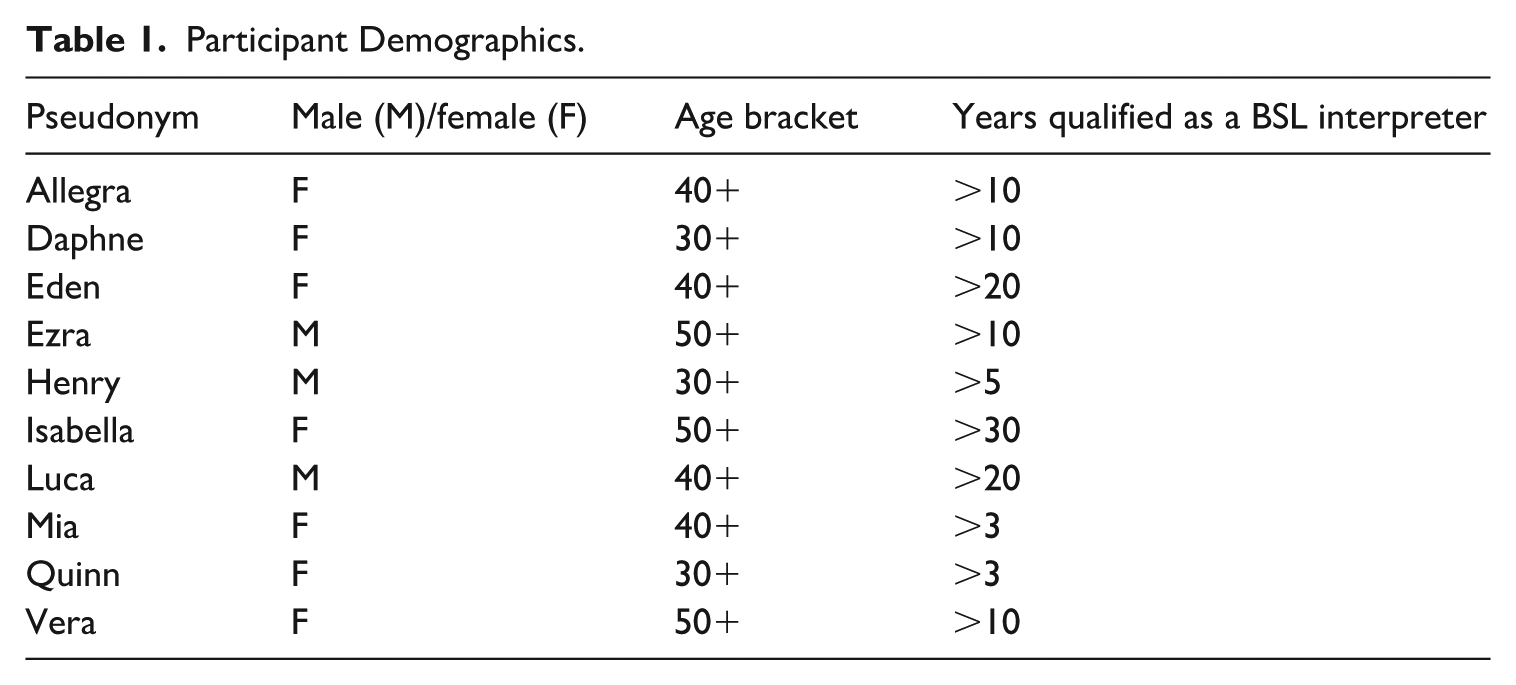
Participation in this study was open to registered sign language interpreters in the UK that had been qualified for at least three years and had experience of interpreting for deaf children in health care settings. To recruit suitable participants, an invitation was emailed to interpreters registered with the National Register of Communication Professionals Working with Deaf and Deafblind People (NRCPD) and interpreters in other interpreting networks in which the authors are involved. Three male and seven female interpreters were recruited for the study, which broadly aligns with the demographic of the profession in the UK (Napier et al., 2021). These interpreters varied in age and interpreting experience (see Table 1) and came from a large geographical area across the UK. Participants were sent an information sheet which provided details about the research, had the opportunity to ask questions and seek clarification. They were reminded that their participation in this study was voluntary and that they could withdraw from the research, at any time, without providing a reason. The participants were then required to sign a consent form, and a suitable time and date for a remote interview was arranged.
Participant Demographics.
2.2 Data generation
Each participant took part in a semi-structured interview using the Zoom platform to accommodate the geographic spread of interviewees. Each interview lasted about 1 hr and was video recorded. The participants were asked a series of open-ended questions and encouraged to convey their experiences of working with children in health care settings (Appendix). The transcription feature in Zoom was used to generate an initial transcript which was manually checked for accuracy against the video recordings before the recordings were deleted. The data were then de-identified: Personal information was redacted, and pseudonyms were allocated to each participant to maintain confidentiality.
Reflexive Thematic Analysis (RTA) was used to collate and identify themes in the data (Braun & Clarke, 2022), with the researchers playing an active role in this process. Our emic perspective informed both the questions that we asked the participants and our analysis of their responses. The process of analysis initially involved the researchers becoming “immersed” in the data (Braun & Clarke, 2022), which occurred while reviewing the recorded interview and correcting the transcripts. Thereafter, we used Quirkos software to code the data and systematically provide meaning to each chunk of information (Terry & Hayfield, 2021). Coding was inductive but necessarily informed by our emic perspectives. The process allowed for different codes to be assigned to the same data extract. For example, the codes, “interpreter’s identity rapport,” “introductions,” “child’s perspective,” were assigned to the quote: I’m acutely aware sometimes because, you know, I’m a guy, and I’m tall, I can be a bit scary to a little child. So sometimes it’s good to break that ice and have a little chat beforehand.
This process allowed us to generate themes that captured “meaningful patterns” (Terry & Hayfield, 2021), which reflects our deep engagement with the data.
The research gained ethical approval from Queen Margaret University, and we endeavoured to be reflexive throughout, by critically reflecting on our research decisions. We maintained the confidentiality and anonymity of the participants through use of pseudonyms to ensure that they could not be identified from the reported data.
3. Results and discussion
The participants had experience of interpreting for deaf children in both physical and mental health settings. They acknowledged that interpreting in any health care setting is often challenging, but when the patient is a deaf child, it adds another layer of complexity, a point echoed in the literature (Crezee, 2013). To manage the array of demands that interpreters encounter, a wide range of strategies or “control options” (Dean & Pollard, 2013) were identified in the data. To determine the most appropriate control in any given situation, the participants often used the phrase “it depends” and then relayed a list of factors that would influence their choice. This falls in line with DC-S which is underpinned by the assumption that interpreters are practice professionals (Dean & Pollard, 2013, 2018) and which promotes an approach whereby, rather than following a “deontological” or rule-based approach, interpreters need to take into consideration the concurrent demands in the situation and consider how their interpreting decisions impact the interaction (Dean, 2021; Dean & Pollard, 2018). The purpose of this research study is therefore not to give a list of rules as to what interpreters should or should not do in any one situation, but rather to explore the challenges that interpreters face and understand the various strategies that are available to them.
Two salient themes were identified in the data. The first is “Do everything with a spirit of collaboration,” which highlights the need for participants to all work together and the ways in which interpreters facilitate this. The second theme is “They are kids; It’s emotionally hard sometimes,” which concerns the intrapersonal demands that interpreters can face, and how they mitigate these demands. Within each theme, we report on various challenges that occur and the strategies that can be employed in a child’s health care appointment, illustrating these with data extracts, and relating the findings to existing literature.
3.1 Theme 1: do everything with a spirit of collaboration
This theme concerns the ways in which interpreters work collaboratively with everyone involved in the interaction, the challenges this involves and the strategies they employ to ensure that the interaction is as effective as possible. It has four sub-themes, (1) establishing a collaborative working relationship with the health care practitioner, (2) working with the child and their parents, (3) supporting the child to trust the health care practitioner, and (4) conveying information.
3.1.1 Establishing a collaborative working relationship with the health care practitioner
A central theme identified in the data is the need for interpreters to work collaboratively with all the individuals involved in the child’s health care appointment. In a health care environment, professionals from a variety of disciplines often work together to look after the health and wellbeing of the patient (Department of Health and Social Care, 2023; Rosen et al., 2018). When a HCP has a deaf child as a patient, they require the specialist skills of a qualified sign language interpreter (Du Feu & Chovaz, 2014) and, as noted in the literature, the interpreter should be considered as an essential part of the health care team (Angelelli, 2004a, 2004b; Swabey & Faber, 2012) to support the HCP to treat and diagnose the child effectively (Ackroyd & Wright, 2018; Hsieh, 2007). Ezra illustrates this collaborative approach in the following comment: We would have meetings, where we would talk about the children, try and understand their background, we would talk about the reason why they’re coming in . . . it was great preparation, because I knew what I was going in to interpret.
Ezra’s use of the word “we” indicates that he felt part of the mental health care team, and that the information that was provided to him, enabled him to understand the aims of the appointment and ascertain exactly what was expected of him. Ezra’s comments echoed those of other participants that regularly worked with a particular HCP and who mentioned that they were able to employ preparation strategies of reading case notes or referral forms which enabled them to prepare for the appointment. Researchers assert that to work together effectively, it is important that professionals understand the roles and responsibilities of each team member (Ndoro, 2014), obtain background information about the patient, and understand the proposed treatment plan, which enables them to work towards the same goal (Swallow et al., 2013). The research data suggests that when interpreters had a “latent network” (Watts, 2003) with a HCP there appeared to be a mutual understanding of roles and responsibilities. This occurred most frequently in specialist mental health care settings. In addition, these interpreters were more likely to have a pre-meeting with the HCP, to obtain relevant information as Eden explains: I will get briefed . . . so my preparation is then getting myself in the right mindset and making sure that I have things up my sleeve just in case things don’t go as planned . . . But I know what he, [the consultant psychiatrist] is wanting. He trusts me . . . so I can go, okay, he wants to know this, this and this for this child . . . . so, I am used as quite an integral part of the team.
This comment highlights that collaborative working fosters trust, as the participant reports being provided with information that supported her to know exactly what was needed to employ the appropriate strategies and work in harmony with the overall goal of the interaction. Ezra’s and Eden’s comments align with Ackroyd and Wright’s (2018) observation that when interpreters work regularly in specialist child mental health settings, they become part of the health care team, and engage in meetings, which enable alignment with the intended aims.
Participants’ experiences indicate that inclusion within the clinical team was far more likely to occur within specialist mental health care provisions. However, in a physical health care environment, interpreters were less likely to be able to have a pre-meeting with the HCP, as Quinn comments: During my [interpreter] training, we were advised to speak to the medical practitioner beforehand. . .so when I first started, I was really keen and very green and I thought to myself, I am going to speak to the practitioner beforehand; but it has never ever been possible. Possibly because they are back-to-back with appointments, so it’s just never been possible.
Isabella illustrates some of the other challenges that arise from the lack of a latent network with the HCP: I was interpreting . . . for a deaf child, waiting for the clinicians to come in at various points . . . there was an OT . . . a physio . . . the consultant . . . the ward nurses . . . I think for me it was an unsuccessful interaction because . . . there was no handover from the team . . . I found that I had to think on my feet . . . I was more conservative in my interpretation and in my controls . . . to the point of being very reserved, because I thought, I can’t do anything that’s going to upset what’s already gone before.
This comment indicates that in this interaction there were several professionals who worked together as a team and carried out work within their specialisms. Within a hospital, prior to commencing work with a patient, a handover is always given between the clinicians (Ghosh et al., 2021). However, Isabella was not afforded the benefit of a handover or a pre-meeting and, consequently, this impacted on the way that she conducted herself and her interpreting decisions and strategy choices. Mapson and Major (2021) highlight that when an interpreter is not aware of the aims and intentions of an interaction, their cognitive load increases. In Isabella’s example she had to “think on her feet” and rather than feeling confident about her interpreting decisions, she remained cautious so as not to have a negative impact on the interaction. This evidences how a lack of collaboration can cause the interpreter to feel unprepared and have less confidence in their interpreting decisions.
To manage the lack of an existing relationship with the HCP and a pre-briefing with them, the participants explain that they must rely on their own knowledge and experience to predict the aims of the interaction. However, Quinn and Vera both feel that, as Angelelli (2004b) and Hale (2007) have previously highlighted, some HCPs have a lack of awareness about the role of the interpreter, which hinders collaborative working relations. Henry echoes these sentiments as he reveals that on many occasions some HCPs assumed that he was a friend or family member. In addition, another participant reports being asked by a HCP to leave because they expected the parents to facilitate communication in the child’s appointment and they did not feel that her presence could add any value. This evidence supports the wider debate regarding the barriers deaf children face to obtaining an appropriately trained interpreter (Heap et al., 2020; Hedding & Kaufman, 2012). Moreland and Agan (2012) offer insight into the potential thought world of some practitioners as they explain that, despite interpreters undergoing extensive training and viewing themselves on par with the practitioner, the interpreter’s status is often not recognised because they are not medically trained, which can act as a barrier to a collaborative working relationship. Participants explained how they try to compensate for this by endeavouring to introduce themselves, explain their role, and conduct themselves in a professional manner by displaying the appropriate interpersonal skills. This mirrors arguments made by Llewellyn-Jones and Lee (2014) according to which the way interpreters introduce and conduct themselves can affect how they are viewed by the HCP. For example, Luca had positive experiences of working with HCPs and was often able to obtain the information that he needed prior to an appointment. This reflects the broader literature emphasising the role of interpersonal skills in fostering trust and building a positive rapport, with researchers such as Spencer-Oatey (2008) and Hsieh et al. (2010) underscoring how relational behaviours directly contribute to the success of collaborative interactions. Therefore, when an interpreter displays positive professional behaviours, it can promote a collaborative working relationship with the clinician, as together they support the health needs of the child.
3.1.2 Working with the child and their parents
Luca and Quinn both explained that when a child and their parents attend a health care appointment the parents may naturally “worry about the health of the child.” In addition to these feelings, while some deaf children are proficient BSL users and feel confident about being deaf, Mia recognised that others may feel embarrassed about signing and struggle to accept their deaf identity. As a consequence, they may feel self-conscious in the presence of an interpreter. Furthermore, the participants noted that some parents may feel embarrassed that they are not able to communicate effectively with their child and perhaps have not explained what the health care appointment is about, which could cause the child to feel anxious and frustrated. Therefore, while some parents may feel grateful that there is an interpreter present, others may feel defensive and say that one is not needed. Silverman et al. (2013) assert that it is important that the child and their parents feel comfortable so that they can express themselves in the health care appointment. Ezra’s comment reinforces this: If everybody . . . likes each other and gets on, then the communication is going to be successful or at least more effective.
This is why it is important that an interpreter engages in “rapport management” (Spencer-Oatey, 2008), which helps the child and their parents to feel comfortable in the interpreter’s presence. For this reason, Mia endeavours to use her interpersonal skills to introduce herself and have a conversation with both the child and their parents. Isabella acknowledges that some interpreters believe that this interaction is inappropriate, reflecting the traditional view of interpreters as conduits and the idea of engaging in a conversation as unprofessional (Hsieh, 2007; Solow, 1981). However, Isabella asserts that this cannot be the case when working with children as she says, “there has to be something of yourself that you give.” Luca makes a similar point: I’m not afraid to say a little bit about myself . . . I think that you may need to say a bit about yourself to get people to trust you.
Engaging in a conversation prior to interpreting the health care appointment can foster trust in the interpreter and support a child and parents to feel comfortable. However, the participants note that an interpreter’s identity could hinder them from establishing a rapport. For instance, Vera highlights that as “an older lady” it can be difficult to engage in a conversation about something that may interest the child, and Eden asserts that she does not have a lot of access to “youth culture.” As a coping strategy the participants use humour and their lack of knowledge on various topics to engage with the child, which Allegra describes as “having a bit of banter and just being kind, being nice.” The male participants also highlight how their identity could impact the child as Luca explains: I have to have my eyes open to . . . general intersectional stuff and around who I am and who they are . . .
To manage this type of challenge, Ezra explained that, at times, depending on the situation, he may suggest that a female interpreter replaces him to help the child feel more comfortable; but generally, the male participants state that they endeavour to introduce themselves and use their interpersonal skills to support the relationship. This suggests that the personality of an interpreter can impact the interaction, which is why both Ezra and Eden believe that not all interpreters are suited to work in this domain. This is because while a person can be taught about the technical aspects of the job, Eden argues: If you’re giving off vibes that the child doesn’t connect with, or the parents don’t connect with, it ain’t gonna work.
The data resonate with the work of Bontempo et al. (2014), who argue that the personality of the interpreter is important because it can impact on the dynamics of an interaction. The data show that displaying qualities that are warm, empathetic, kind, pleasant and respectful, supports a positive relationship with the child. In addition, these interpersonal skills can aid an interpreter to develop a positive rapport and trust with the parents, as Luca highlights: Building some relationship with the adult because they need to know that I am alright, and I may need them for the information that they hold about the child and the situation . . . the people that know them best can be really good informants.
This comment indicates that establishing a positive rapport with the parents may support them to feel comfortable to share information with the interpreter, which can aid the interpretation process. Here the interpreter’s conduct is a strategy to mitigate the face threat of their presence (Monacelli, 2009), enabling the interpreter and the parents to work together in harmony with the overall goal of the environment.
3.1.3 Supporting the child to trust the health care practitioner
The child is central to their health care appointment (Wangmo et al., 2016) and has a right to express their views and opinions (Baraldi & Ceccoli, 2023). However, Ezra explained that this can be a challenge for a deaf child because in an interpreter-mediated health care appointment, they are the “only child in a room full of four or five adults,” which could cause them to feel intimidated and hold back from expressing themselves. Allegra believed that the HCP should have the responsibility and necessary skills to support the child to feel comfortable and gain their trust. Mapson and Major (2021) assert that it is essential that the interpreter conveys the HCP’s skills and techniques in their interpretation. Consequently, Daphne feels that, as an interpreter, she has to “be in tune” with the HCP and understand what they are trying to achieve. For instance, the HCP will often use their interpersonal skills to develop a rapport and build trust with the child; the participants say they mirror this in their interpretation by using the appropriate body language and facial expressions.
Another strategy that was identified to support the child to trust the HCP was the use of consecutive interpreting. Luca explained that this mode of interpreting allows the child time to look at the body language and note the rapport-building strategies that the HCP is attempting to display, which he believed is an effective strategy as deaf children are often very good at reading body language. Furthermore, this strategy can also encourage direct communication on the part of the HCP as Isabella illustrates: If the doctor is trying to use gestures in some way . . ., if they are, kind of doing the thumbs up, I wouldn’t repeat that . . . I look at the clinician too so that the child is then engaging directly with the clinician where appropriate.
These data therefore show that interpreters need to be socially aware and understand the dynamics in the room. This aligns with Major and Napier’s (2019) assertion that interpreters need social skills so that they can be perceptual and discerning. In turn, this allows the interpreter to notice and mediate the trust-building behaviours that the HCP displays to the child.
On the other hand, HCPs may feel apprehensive when working with a deaf child and an interpreter (De Feu & Chovaz (2014), which could affect how they display their interpersonal skills (Theys et al., 2022). For instance, Silverman et al. (2013) argue that when a HCP gives eye contact to a patient, they are better able to build a trusting relationship, but Mia notes: Sometimes they look at me and not the deaf child, they look at me and say, “can you tell them . . .” rather than asking them directly.
The participants relayed a variety of strategies to manage this demand, ranging from verbally instructing the HCP to look directly at the child, to using body language to direct the HCP to look at the child. Similarly, Llewellyn-Jones and Lee (2014) advise that an interpreter can redirect the eye gaze of the hearing participant by continuing to look at the deaf person, which supports the patient and HCP to build a relationship. However, Henry notes that sometimes a child, especially one that does not have access to sign language in the home, may be reluctant to engage with the HCP, preferring to engage with the interpreter. Nevertheless, Ackroyd and Wright (2018) argue that the interpreter should try to direct the child’s attention to the HCP. To do this, many of the participants reported that interpreting in the third person is a useful strategy to indicate where the information is coming from, and to promote respect and trust.
3.1.4 Conveying information
The participants all expressed a view that the child should understand what is discussed within their health care appointment. However, at times, the HCP and parents may have a conversation that excludes the child, as Isabella illustrates: It was a dental hospital . . . this particular child was only about seven . . . it got very technical between the parents and the dentist and what particular teeth they were treating . . . and the treatment plan, and I found that the child was disengaging and that was a challenge.
The conversation between the parents and HCP meant that the child disengaged in the interaction. Silverman et al. (2013) explain that, initially, the HCP will talk to the child, then engage with the parents and at the end they return their focus to the child. When an adult-to-adult conversation ensues, participants indicated that meta comments are often used to draw the HCP’s attention to the fact that the conversation is not accessible to the child. Luca acknowledged that to interpret an adult-dominated conversation in a child-appropriate manner is often incompatible. Some participants reported engaging with the child on a personal level and then at an appropriate time inviting the child to confirm their understanding of what was discussed. At the same time the interpreter still listens to the adult-dominated conversation and gives a summary to the child, which allows them to have access to the overall message and participate in their appointment if they wish to do so. These data therefore illustrate how interpreters need to be transparent and open with everyone in the interaction.
Nevertheless, even when the HCP directs their attention to the child, the language that they use can be complex. For example, Ezra recalls interpreting for a child in a situation in which the HCP explained the ramifications of a certain condition using complex terms and language. The literature emphasises that before an interpreter can interpret, they must understand the information (Napier et al., 2006) and this is borne out in the data, which show that interpreters often seek clarification to ensure that they understand the intended message. However, Mia explains that the manner in which she interprets complex information will change depending on the needs of the child. For example, the participants reported taking into consideration concurrent demands, such as the consequences of the information, the age, cognitive and linguistic abilities of the child, and whether the child has access to language in their home environment. Moreover, Luca commented that after considering the concurrent demands, he makes a professional judgement: I make judgements about whether I am going to break down the information or make suggestions, if, for example, they say something that I recognise is complicated for this kid or my experience of working with deaf people.
This comment acknowledges that some deaf children may be fluent in BSL, whereas others may be dysfluent and deprived of language (Glickman & Hall, 2019; Holmes, 2021). This prompts Luca to assess the language abilities of the child and, if necessary, break down the information and put it in a format that can meet the needs of the child. Interpreters therefore require good linguistic skills and confidence in their abilities. Furthermore, Luca’s comment exemplifies another strategy, namely, making suggestions to the HCP to support the child in their understanding. For example, the data showed that interpreters may liaise with the HCP and use diagrams, drawings, or point to real life objects to convey information. This finding echoes Crump and Glickman (2011), who also stress the importance of the interpreter and HCP working together collaboratively to accurately convey the intended message. Thereafter, the interpreter will look at the body language and facial expressions of the child to check whether the message has been understood. Mia acknowledges that this can be a challenge because deaf children often nod their head and pretend, they understand. Similarly to the educational interpreters in Lombardi’s study (2023), Ezra and Eden both adopt a further strategy of asking the child to repeat what has been said to confirm their understanding, a strategy Ezra says he would only employ when working with children. In addition, Allegra commented that involving a Deaf interpreter can be beneficial, which is also supported by Crump and Glickman (2011).
To gather information, the HCP often asks the child a series of questions. The data include examples of participants experiencing situations in which deaf children had struggled to respond. De Feu and Chovaz (2014) explain that, due to language deprivation, some deaf children struggle with open-ended questions. Consequently, the child may make a comment that is not in line with the topic. In this situation the child’s language abilities can become a significant demand for the interpreter. To manage this demand and ascertain the relevant information, Luca finds it useful to adopt a conversational manner: I use strategies around checking in such as, “so did you say this?” or just looking to have a bit more of a conversation with them as well to get the information that is being asked of them . . . It’s more like trying to find a way to maintain their comfort that means the channel is still open, when they could easily shut it down because they feel frightened or intimidated and someone is asking them questions and they are personal and they don’t know the answer, they probably want to give an answer but they can’t and that’s stressful.
Luca’s comment resonates with Pollard et al.’s (2009) observation that sign language is inherently a dialogic language, relying on a conversational exchange rather than a monologic delivery. Therefore, Luca’s strategy of “checking in” and “having a bit more of a conversation” with them, honours this linguistic form, while also helping the child to feel comfortable. Luca understands how important it is for the HCP to receive responses to their questions but also takes into consideration the “thought world” of the child and does not want to hinder them from participating in the conversation. This means that he carefully considers his interpreting decisions and works with the child to convey their message. In addition, some children are language dysfluent and may use home signs or idiosyncratic language to communicate (Hall, 2017). Consequently, Quinn says she “leans on the support of the parents” for clarification, using her interpersonal skills to engage them in a respectful and collaborative manner. This reflects literature on the communication complexities between hearing parents and deaf children in interpreter-mediated interaction (Harvey, 1982; Mitchell & Karchmer, 2004; Rowley, 2021). Quinn recognises that parents hold key information, as acknowledged in the literature (Silverman et al., 2013); therefore, her strategy promotes shared understanding and reflects a control option that encourages collaborative communication to ensure the intended message is conveyed.
3.2 Theme 2: they are kids; it’s emotionally hard sometimes
The second salient theme identified in the data concerns the emotional challenge of interpreting for deaf children in health care settings, and the strategies interpreters adopt to mitigate these emotional demands. It has two sub-themes: (1) self-care, and (2) interpreters managing their own emotions.
3.2.1 Self-care
Zafirah et al.’s (2020) exploration of the emotional toll experienced by interpreters relates to working with children in mental health care settings. However, the present data shows that interpreters experience intrapersonal demands when working with children within broader health care settings, such as surgery, palliative care or life-threatening conditions, as Quinn highlights: Working with any children in medical settings, it’s the vicarious trauma what you take away with you afterwards. You know, sometimes you think you’re managing it really well, and it’s fine, and on the day it’s fine, but then it’s afterwards.
Vicarious trauma is identified by Bontempo and Malcolm (2012) as occurring after an interpreter has been exposed to upsetting events. Participants were evidently aware of the potential for this to arise when working with children and the need for coping strategies. For example, Eden acknowledged that it is vital that interpreters working in this environment look after their own wellbeing and engage in self-care: I think interpreters going into working with children need to have a robust plan for self-care. Because you see all sorts of stuff and if you haven’t got ways of looking after yourself you are gonna burn out, because you could see stuff in a week that you’ve not seen in the whole of your life . . . Just because you’ve got a badge that says you’re a qualified interpreter does not protect you from some of the stuff you’re going to see . . .
When interpreters witness the suffering of a child this can adversely affect their mental and physical health. Gutman (2005) advocates that self-care is necessary for a professional to be ethical in their practice because they need to be able to support themselves before they can support others. In addition, Macdonald (2015) asserts that decision-making skills can be affected when a professional experiences vicarious trauma or burnout. Eden advised that interpreters should practice self-care by taking time out and doing something nice for themselves to mitigate the negative impact. In addition, Quinn explained that these difficult conversations can “stay with you,” which underlines the need for interpreters to reflect and offload in supervision (Dean & Pollard, 2013; Hetherington, 2012).
3.2.2 Interpreters managing their own emotions
In a child’s health care appointment, the data showed that interpreters experience strong intrapersonal demands (Dean & Pollard, 2013), often as a result of seeing a child that has been deprived of language. Dean and Pollard (2013) argue that it is imperative that an interpreter recognise intrapersonal demands, so that their thoughts and feelings do not impact the interaction. Many of the emotional responses that interpreters reported in this context related to the poor communication that can exist between the deaf child and their parents (Mitchell & Karchmer, 2004). Ezra candidly relates that he finds it hard when children and parents struggle to communicate because the parents do not sign. Vera recalls a parent saying to her, “can you tell my child I love them,” which caused an emotional reaction as she empathised with how upset the child may feel that they are unable to converse with their parents. This can be difficult for interpreters to witness because they know that this is indicative of language deprivation, which is preventable (Rowley, 2021). To manage this challenge, Luca makes the following comment: For me turning up to that situation, it is what it is and, I am not there to make a judgement and not there to tell them about my judgements . . .
Luca’s comment indicates that he does not cast judgement on the situation but instead endeavours to focus on the task at hand. His response reflects the ethical stance encouraged in DC-S (Dean & Pollard, 2013), which emphasises the importance of recognising and managing intrapersonal demands. By consciously setting aside personal judgements Luca demonstrates how interpreters can remain both present and professional. The NDCS (2024) asserts that it is the parent’s right to decide how they will communicate with their child. It is therefore essential that interpreters show respect to the parents and their decisions, which is in line with the ethical principles that are set out by the interpreting registration body, to “show respect” (NRCPD, 2023).
The participants also expressed how they experience interpersonal demands based on the content that they are expected to interpret. For instance, in a mental health setting, conversations about self-harm, suicidal ideation, and abuse, are common. Lai and Heydon (2015) assert that interpreting traumatic information can negatively impact upon an interpreter’s processing skills and affect their emotions. Daphne made the following observation: I think there’s a lot of that kind of internal checking that you need to do, to think about, what am I projecting here . . . and how can I modify my internal feelings.
Daphne endeavours to check in with herself, which involves being self-aware and conscious of her feelings so that she can manage her emotions during the interaction. These skills are deemed essential to avoid negatively impacting the dynamics (Dean & Pollard, 2013; Llewellyn-Jones & Lee, 2014). Furthermore, Eden revealed that when interpreting traumatic content, especially around suicide ideation, she adopts the strategy of interpreting in the third person, to protect herself, so she does not hear herself say the words “I will . . . .” Being prepared to use strategies like this is essential to help interpreters manage their emotions and protect their own wellbeing.
4. Conclusion
In conclusion, this research has highlighted the many challenges that interpreters experience when they are required to interpret for deaf children in a health care setting. While some of these challenges relate to tailoring communication to the needs of the child, and the linguistic considerations involved, many relate to the relational and interpersonal aspects of the interaction. These require interpreters to be adept at using their own interpersonal skills to establish rapport and trust with everyone involved and having a nuanced understanding of the interactional dynamics. It is these interpersonal challenges that can also have an emotional impact on interpreters, necessitating other self-care strategies to be employed in relation to their own wellbeing. Central to this is the negative experience of witnessing poor familial communication and the need to manage their emotions during the interaction, refraining from making personal judgements or giving their own opinions.
This research has several limitations. First, although the number of participants is small, the data generated in the study and the experiences of those involved resonates strongly with our own experiences of interpreting for deaf children in health care situations. Second, it has not been possible to report on the entirety of the data generated. The focus here has been on appointments involving deaf children with hearing parents. We acknowledge that some appointments will involve deaf children with deaf parents, and further research would be helpful to explore the dynamics of interpreting in that context. Further research to explore the perceptions and experiences of the parents, deaf or hearing, would also be valuable.
One significant finding from this research is that interpreters are often viewed as part of the health care team when they work with deaf children in a specialist mental health care setting. Further research to understand the extent to which a collaborative approach also occurs when working with mental health professionals that do not specialise in working with deaf children would be beneficial. Sadly, the participants note that within a physical health care environment, the HCPs often lack understanding about the role and responsibilities of the interpreter, which can hinder collaborative working relations. Therefore, further understanding of the barriers to this would be valuable to help improve relationships between HCPs and interpreters in this setting.
Another notable finding is that language deprivation and dysfluency present unique challenges for sign language interpreters, who must assess a child’s language skills to meet their communicative needs. Although research encourages working alongside a Deaf interpreter in such cases, only one participant identified this as a control option. Therefore, further research is needed to understand the perspectives and experiences of working with Deaf interpreters in health care settings and the barriers that might prevent this from happening.
Footnotes
Appendix
Acknowledgements
The authors would like to express their thanks to all the research participants for giving their time to be involved in this study and to Yvonne Waddell for her support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by Queen Margeret University on 29th February 2024. The approval number is 20240229_NC.v1
Consent to Participate
All participants provided written informed consent for publication, and they were informed that all personal information would be anonymised. Participants were informed about the purpose of the research and their right to withdraw consent at any time prior to publication.
Data availability statement
The data that support the findings of this study consist of interview transcripts and are not publicly available due to confidentiality agreements with participants.