
Abstract
Background:
Maxillary defects resulting from tumor resection or trauma can lead to substantial functional and esthetic impairment, including malocclusion, impaired mastication, disordered speech, and loss of midface projection. Free tissue transfer has become the primary method of reconstruction for large maxillary defects, yet flap failure and patient-specific contraindications can limit its use. Custom patient-specific implants have emerged as a potential alternative for patients who are unable to undergo or have previously failed traditional reconstruction.
Case Presentation:
We present the case of a 23-year-old man who acquired severe maxillary bone loss following childhood fibrous dysplasia treated with hemi-maxillectomy. Over 7 years, he underwent multiple reconstructive attempts at our institution, including 2 fibula free flaps that ultimately failed, prompting consideration for reconstructive alternatives. This patient was selected for custom maxillary reconstruction with a digitally planned, titanium subperiosteal implant using the IPS Implants® Preprosthetic system. The implant was successfully placed in a single-stage procedure, providing immediate, stable structural support for definitive prosthetic rehabilitation.
Conclusions:
This case highlights the role of custom patient-specific implants as a viable reconstructive option for patients with extensive maxillary loss who are poor candidates for free tissue transfer. Patient-specific subperiosteal implants may provide durable skeletal support and reliable dental rehabilitation for complex cases in which traditional methods have failed.
Keywords
Introduction
The maxilla is a crucial osseous component of the face, providing support for structures including the ocular globes, paranasal sinuses, nasal cavity, hard palate, and alveolar ridge. 1 Maxillectomies may lead to substantial morbidity due to the wide range of facial structures that the maxilla supports. Sequelae of maxillectomies include, but are not limited to, malocclusion, deficiency of the nasolabial/midface projection, and disorders of mastication, swallowing, and speech.2-5
Historically, prosthetic rehabilitation had been the principal approach for managing maxillary defects.2,6 Overtime, the approach to maxillary reconstruction has evolved alongside surgical refinement and innovation. As advancements in microsurgery have developed, free tissue transfer (FTT) has been adopted as the primary reconstructive option for complex midface defects, particularly in maxillary reconstruction. 2 Like any surgical procedure, FTT is not always successful, and when it fails, alternative reconstructive techniques are required.
Virtual surgical planning (VSP) and computer-aided design and manufacturing (CAD/CAM) are technological innovations that are advancing the landscape of maxillary reconstruction with custom patient-specific implants (PSI).3,4 Herein, we report a case of a 23-year-old male with a history of pediatric fibrous dysplasia treated with hemi-maxillectomy and subsequent failed FTT reconstruction who presented to our institution for custom PSI maxillary reconstruction.
Case
Clinical History
IB is a 23-year-old male with a past medical history of fibrous dysplasia, previously treated at an outside hospital with left hemi-maxillectomy and latissimus flap reconstruction of the palate at age 13. He subsequently presented to our institution, where he has undergone multiple reconstructive procedures. The patient initially presented to our institution at age 15 with an acquired maxillary defect following a left hemi-maxillectomy, resulting in a malpositioned residual maxilla and class III malocclusion. At that time, surgical options were discussed, and operative planning began. The patient returned 1 year later for orthodontic adjustments and finalization of the surgical plan (Figure 1A).
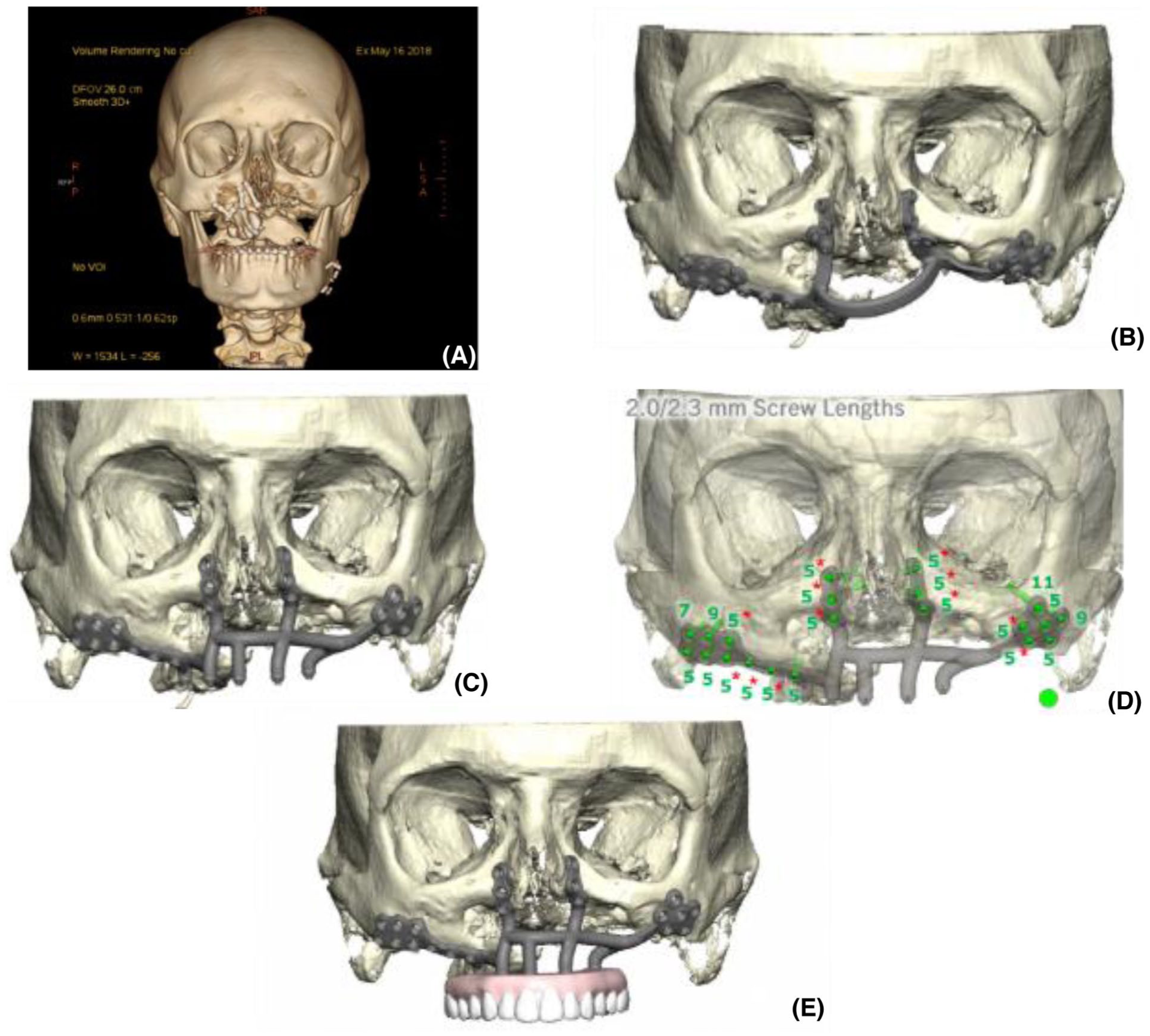
(A) Preoperative CT Scan, May 2018, (B) custom cutting guide, (C) custom IPS Implants® Preprosthetic system, (D) screw guide, and (E) final custom implant with simulated custom prosthodontic placement.
At age 16, the patient underwent his first major reconstructive procedure in June 2018: a hemi LeFort I osteotomy with maxillary fixation, left fibula free flap reconstruction, and left saphenous vein graft. Although initial flap viability was confirmed postoperatively, complications soon arose. By post-operative day (POD) 6, intraoral wound breakdown suggested flap compromise, leading to a takeback surgery the following day. Necrotic fibula was debrided, and soft tissue coverage was achieved with buccal mucosal flaps.
Over the next several months, he underwent a series of additional procedures. In August 2018, he had 2 surgeries using buccal mucosa advancement to close an oronasal fistula. Both attempts were unsuccessful, resulting in a persistent defect. In December 2018, a radial forearm flap was used as a free flap to close the oronasal fistula, with postoperative evaluations in early 2019 showing stability. Dental reconstruction was attempted with an oral and maxillofacial surgeon 18 months later in July 2020, but a nonviable fibula was recognized intraoperatively. Dental reconstruction was therefore aborted, and no implants were placed.
In October 2020, a second fibula free flap with dental implants was performed. Surgery was initially successful, and the patient was discharged home on POD 8. However, follow-up exams revealed bulky tissue, plate displacement, and eventual failure of the reconstruction, with bone and implant exposure by early 2021. This necessitated the removal of the reconstruction in January 2021. Therefore, no additional operations were required, shifting care toward prosthodontic options.
By May 2023, following years of multiple reconstructions and flap failures, the patient had a stable intraoral environment and was considered a candidate for a custom implant-based maxillary reconstruction with full upper arch restoration. With a history of multiple graft complications and a thrombophilic family history, the patient was evaluated by hematology/oncology in August 2024 to rule out the presence of an underlying clotting disorder. Laboratory evaluation was found to be significant for an elevated Anti-Cardiolipin IgG, suggesting an underlying blood dyscrasia.
Custom Implant-Based Maxillary Reconstruction
Our craniofacial surgeon (E.B.) and maxillofacial prosthodontist (S.O.) decided to proceed with a patient-specific implant in collaboration with the KLS Martin group, IPS Implants® Preprosthetic (KLS Martin Group, Tuttlingen, Germany). A digitally backward planned subperiosteal implant was designed for 1-step reconstruction of the maxilla (Figure 1B-E). In January 2025, 7 years after the patient’s initial reconstruction, the custom implant was placed.
Through an upper gingivobuccal incision, the zygomas and nasomaxillary region were exposed. A premade guide was used to align drill holes (Figure 1B) followed by introduction of the custom implant (Figure 1C). The implant was secured in place with 6- and 7 mm screws (Figure 1D). Access holes were created for the 5 posts, the palate was closed with Vicryl sutures, and caps were placed without difficulty. The patient was discharged the following day.
At early follow-up, the implant remained stable with minor mucosal sloughing. By POD 8, all posts were visible and no oronasal fistula was noted. Shortly after, the patient was evaluated by our maxillofacial prosthodontist and reported the sensation of a fistula in the upper right area. Examination showed palatal tissue now covering 2 implants as well as the presence of a new soft tissue defect.
At his third postoperative visit in March 2025, 4 out of the 5 posts were visible, and a small anterior oronasal fistula was confirmed. The patient underwent an additional operation for fistula closure and exposure of the fifth post. The nasal oral lining was closed using 4-0 Vicryl suture in interrupted fashion, and the fistula was repaired with an adjacent tissue transfer. Tissue overlying the left posterior post was debrided for full exposure, and the patient was discharged on the same day of surgery with no concerns. Screw-retained temporary prosthetics were applied the following week. Due to the prosthesis intaglio and contours not matching with the soft tissues, the distal abutment was not engaged, and only 3 support posts were used (Figure 2A and B).

(A and B) KLS provisional connection to MUA abutments, March 2025, (C and D) final fixed prosthesis, August 2025, (E) final panoramic x-ray, August 2025, and (F) Final fixed restorations with titanium substructure and zirconia suprastructure, August 2025.
In May 2025, the right posterior post became accessible, allowing a 4-post temporary prosthetic. The left posterior post remained inaccessible due to partial coverage by the buccinator muscle. A new screw-retained prosthesis was then placed using the 4 available posts. In October of 2025, the upper screw-retained teeth were delivered to the patient’s satisfaction (Figure 2C-F), and the patient was scheduled to follow up with S.O. in 6 months.
Discussion
Objectives of maxillary reconstruction include support of midface soft tissues, separation of oral and nasal cavities, and establishment of bony support for dental implants. 2 Soft tissue and bone augmentation procedures, often by FTT, still remain the standard for maxillary reconstruction of large defects.2,4,7-9 The free fibula flap provides excellent versatility, combining sufficient bone for structural support with a long pedicle and flexible soft tissue for contouring.2,7
Not all patients are ideal candidates for maxillary reconstruction with FTT and bone augmentation. We presented the case of a patient who acquired severe maxillary bone loss and suffered 2 failed fibula flaps. Sweeny et al found that 84% of free flap failures in head and neck reconstruction were attributed to vascular compromise involving the arterial and or venous systems. 10 Due to the history of multiple flap losses, our senior author E.B. recommended hematologic workup for the patient which revealed elevated anti-cardiolipin IgG antibodies, suggestive of an underlying clotting disorder. Our patient’s course prompted consideration of available options for patients needing major maxillary reconstruction who cannot undergo or have failed free tissue transfer.
Subperiosteal implants for dental rehabilitation have been described in the literature for over 80 years.11-13 This technique has been replaced by FTT as the primary option for complex maxillary reconstruction and implant dentistry. With advances in VSP and CAD/CAM, new strategies for complex facial reconstruction have emerged.3,4,12 These tools allow refinement of older techniques such as subperiosteal implants, although current planning still prioritizes bony contours over soft-tissue thickness, which can limit postoperative access to implant components. In our patient, this contributed to a post that remained buried beneath the palatal flap, limiting postoperative accessibility. These challenges underscore the importance of precise preoperative planning and frame the rationale for selecting a customized patient-specific implant.
Through collaboration between our craniofacial surgeon and maxillofacial prosthodontist, a custom patient-specific implant was selected. The team used the IPS Implants® Preprosthetic system (KLS Martin Group, Tuttlingen, Germany). The design protocol, known as “IPS-Dental,” was described by Gellrich et al12-14 Planning begins with high-resolution CT imaging and wax-up models used to define ideal dental position and occlusion. The data is then converted into stereolithographic (STL) files for digital reconstruction of the defect. The skeletal framework and prosthodontic connection system are planned individually then merged into a single titanium implant produced by laser melting, resulting in a substantial 1-piece implant. To ensure accurate placement, this large implant requires wide exposure with appropriately sized incisions to allow precise fixation along stable bony buttresses and facilitate single-stage placement. In this case, access was achieved through an upper gingivobuccal incision, as other approaches would not have provided adequate exposure. However, in cases with severely hypoplastic maxillary bone stock, additional surgical approaches may be necessary.
Applying IPS Implants® for maxillary reconstruction has multiple benefits when compared to existing surgical techniques. Korn et al hypothesized that since the posts are not anchored to bone but rather part of the subperiosteal framework itself, there is a reduced risk of peri-implantitis and local infection. 12 Additionally, the rigid fixation is completely customizable to the patient’s anatomy, with emphasis of fixation onto the buttresses of the maxilla. 14 In the past, the use of non-rigid subperiosteal implants often resulted in progressive bone loss due to movement of the framework. 14 In contrast, the rigid fixation in IPS Implants® provide the stability needed to prevent the occurrence of bone loss. The denture connection system is built into the implant, and this integrated unit passes through the overlying soft tissues on the day of surgery, thus eliminating the need for 2 procedures. 13 These properties offer meaningful advantages in reconstructive efficacy and complication reduction when compared to conventional approaches.
While the integrated design aims to eliminate the need for a second procedure, select cases may necessitate a staged intervention. Surgeons who consider performing this operation must therefore balance adequate soft-tissue clearance to allow the posts to emerge, without over-resection that increases fistula risk. In cases requiring concomitant free tissue transfer, IPS Preprosthetic reconstruction may be staged to preserve flap viability, with initial burial of posts and delayed exposure after vascular integration. In such cases, careful staging is essential. At our institution, we favor performing soft tissue reconstruction first, allowing for confirmation of negative margins and complete intraoral healing prior to implant placement through the gingivobuccal incision. Immediate placement at the time of free flap reconstruction should be approached cautiously, as the reliability of residual bone for anchorage is variable and dependent on factors such as tumor characteristics, required margins, and the ablative surgery. Surgeons and patients should be counseled accordingly, as staged intervention may be required even when single-stage reconstruction is the intent.
Conclusions
IPS Implants®, particularly in patients who have significant contraindications to or have previously failed FTT for maxillary reconstruction, provide an exciting new treatment modality. This promising surgical option may provide a new opportunity for maxillary reconstruction and dental rehabilitation in patients who have exhausted conventional approaches. Our case builds upon previous reports by Gellrich and Korn showing that patient-specific implants are a reliable and stable option for prosthodontic restoration in patients with large maxillary defects.12,13,15 This case also illustrates the essential role of coordinated care between the craniofacial surgeon and maxillofacial prosthodontist in guiding both surgical planning and prosthetic rehabilitation. Future studies are warranted to focus on the long-term outcomes and stability of subperiosteal IPS Implants® in patients with large maxillary defects. Notably, current FDA approval restricts use of this system to patients 18 years of age and older, which may limit access for younger patients who could otherwise benefit from intervention. Because maxillary growth typically completes in mid-to-late adolescence, select skeletally mature patients younger than 18, including those with craniofacial syndromes, oncologic defects, or severe maxillary deficiency, may be appropriate candidates. Therefore, broadening the approved age indication to include skeletally mature adolescents could allow for earlier definitive reconstruction in this population.
Footnotes
Ethical Considerations
Our institution does not require ethical approval for reporting individual cases or case series.
Consent to Participate
Informed consent for information published in this article was not obtained because all patient information was de-identified and patient consent was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.