
Abstract
Introduction:
Restoring premorbid form and function is the goal of craniofacial trauma surgery. Comminuted facial fractures are difficult to reconstruct due to bone loss and instability. Traditional fixation with plates and screws often fail due to resorption and secondary deformities. Titanium mesh is used in cranioplasty and orbital reconstruction, but its application in other facial regions is rare. This study presents a series of acute trauma patients treated with customized titanium mesh exoskeletons, molded intraoperatively using virtual planning models (VSP) to restore structure and function.
Methods:
This retrospective review (2022-2024) identified 23 patients with comminuted facial fractures treated with customized titanium exoskeletons. Craniofacial computed tomography (CT) Digital Imaging and Communications in Medicine data was used for virtual surgical planning (VSP) to achieve fracture reduction references, using mirror imaging of the uninjured contralateral side or a normal cohort image. Intraoperatively, the post-reduction models were used to shape standard titanium mesh to the patient’s craniofacial skeleton to generate a customized titanium exoskeleton that would bridge the area of comminuted fractures. Postoperative CT scans assessed anatomic reduction, and patient charts were reviewed for complications.
Results:
This technique was employed successfully in all patients with comminuted facial fractures. It was successful in several regions of the facial skeleton, including naso-orbital ethmoid (NOE), zygomaticomaxillary complex (ZMC), zygomatic arch, and mandible. This technique was more efficient and accurate in fracture reduction compared to standard plating methods. Postoperative CT scans demonstrated good anatomic reduction and VSP plan validity. Clinical assessment revealed excellent form and function long-term. One patient had partial intraoral exposure of mesh, which required limited removal. There were no known infectious, bleeding, or secondary deformity complications.
Conclusion:
This study presents the largest series of comminuted acute craniofacial fracture repairs using a customized titanium exoskeleton, demonstrating its effectiveness in stabilization, anatomical restoration, and secondary contour maintenance.
Introduction
Craniofacial injuries account for a significant proportion of injuries managed in Level 1 trauma centers. 1 The primary objective of facial trauma surgery is to restore the patient’s pre-injury form and function. Achieving this often necessitates precise anatomic reduction, which becomes particularly challenging in cases of comminuted fractures. While plates and screws are commonly used for fixation, severely comminuted fractures can be extremely challenging due to the absence of reliable anatomical landmarks and inability to effectively reduce and fixate extremely diminutive bone fragments, which can lead to difficulty restoring the 3D craniofacial skeleton structure. 2 Immediate bone grafting may be required to create a “stable construct.” Despite fixation at the time of surgery, comminuted bone and bone grafts can resorb unpredictably, leading to insufficient support of the craniofacial skeleton and secondary deformity with fragment instability, inadequate fixation, and/or persistent bony defects. 3 In certain cases, small bone fragments are left untouched or removed entirely, necessitating further reconstructive procedures to correct segmental defects. 4
Advancements in craniomaxillofacial trauma management have highlighted the potential of titanium mesh as a versatile option for fracture fixation, particularly in comminuted cases.5,6 Titanium mesh has shown promise in providing good stabilization, especially in complex fractures where traditional fixation methods may be inadequate. 6 Its applications in the maxillofacial region include osteosynthesis in traumatology, craniofacial reconstruction, and augmentation of atrophic maxilla and mandible. 6
This study introduces a novel approach that utilizes titanium mesh fabricated onto patient specific skeletal models acutely and intraoperatively to create a titanium exoskeleton to treat comminuted facial fractures. While mesh has long been used in orbital reconstruction, frontal sinus reconstruction and cranioplasty, descriptions of its use in other regions of the facial skeleton have been limited. 5 Here we describe the largest series of acute trauma patients in which standard titanium mesh was shaped intra-operatively on virtual surgical planned (VSP) models to generate a customized mesh exoskeleton. This titanium mesh exoskeleton technique was successfully performed in all regions of the facial skeleton including orbital, frontal sinus, naso-orbital ethmoid (NOE), zygomaticomaxillary complex (ZMC), zygomatic arch, and mandible, allowing for anatomic reduction, projection, and restoring 3D morphology. This approach offers a promising solution to the challenges posed by comminuted facial fractures, potentially improving outcomes and reducing the need for secondary reconstructive procedures.
With the center’s extensive experience with VSP and use of surgical technology and precision-guided reconstruction, 7 a novel titanium exoskeleton technique was developed and successfully applied to address the challenges posed by complex craniofacial fractures. This investigation comprises the largest known series to date utilizing titanium mesh for acute trauma involving multiple regions of the face.
Patients and Methods
A retrospective analysis was conducted on acute craniofacial trauma patients between January 2022 and June 2024. Twenty-three patients who underwent reconstruction using this novel titanium exoskeleton surgical technique were identified. The study was conducted under the approval of the Institutional Review Boards (ID: Study00005292) at our single level 1 trauma institution.
The VSP and surgical protocol implemented in Soubra et al was used in this study. 7 Patients presenting to the emergency department with acute facial trauma underwent standard trauma evaluation and high-resolution CT imaging (1 mm axial, sagittal, and coronal views; Figure 1). Comminuted fractures were diagnosed based on CT and clinical exam findings, defined as having 2 or more free bone fragments. If VSP was deemed beneficial, DICOM CT data were uploaded to a VSP platform for segmentation and virtual reduction. This was achieved using mirrored images of the uninjured side or an anatomical overlay in bilateral cases. In patients with malocclusion, models were further adjusted to ensure proper occlusion and facial symmetry. The surgical and engineering teams then held a collaborative session to refine the reconstruction based on anatomical and clinical considerations. Finally, 3D systems produced a sterilized, anatomically reduced model, and occlusal splints for intraoperative use.
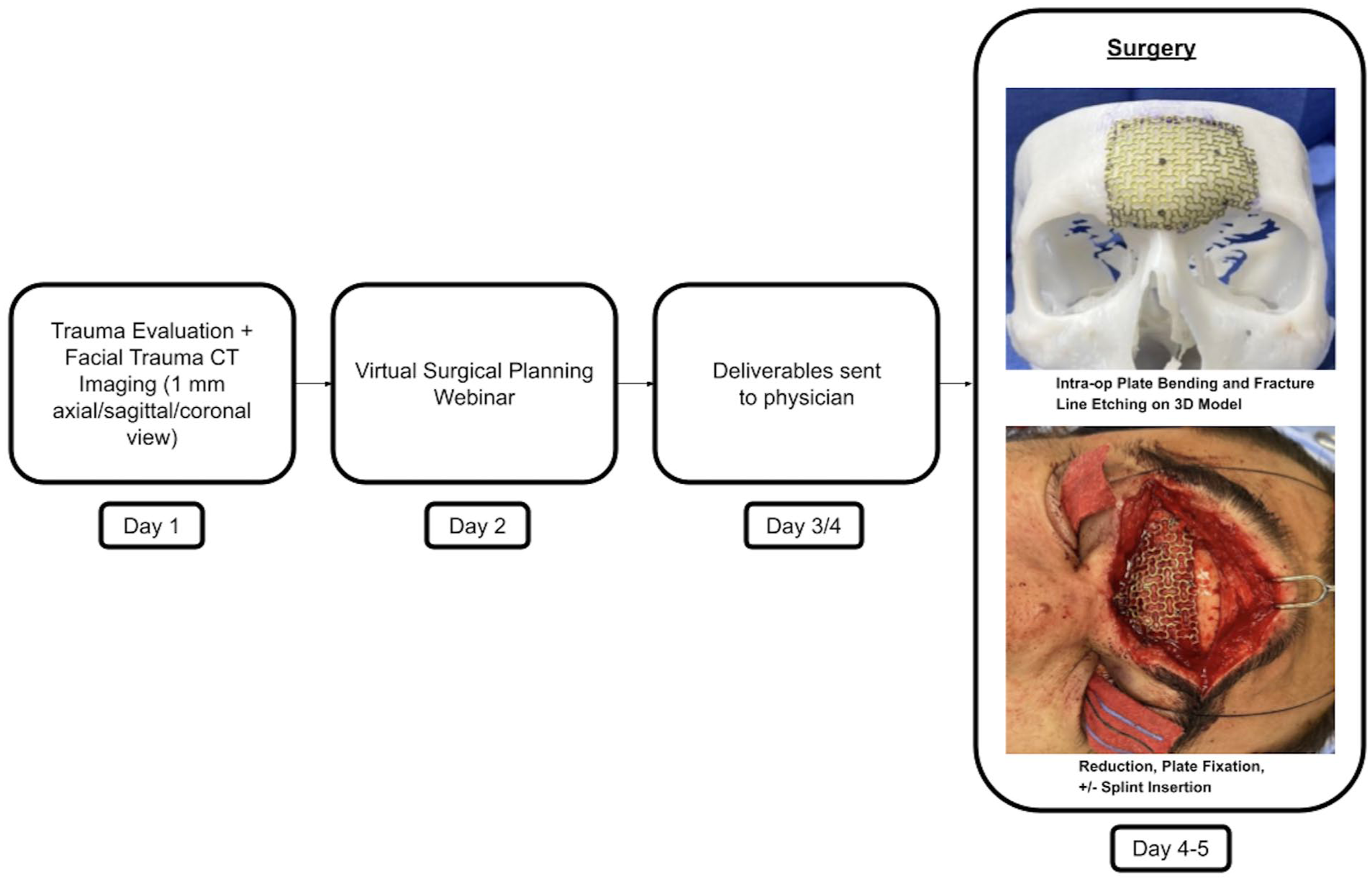
VSP technique flowchart.
Patients were subsequently prepared for surgery, and in the operating room, the standard titanium mesh plates were contoured acutely onto the VSP 3D printed models by the operating room team (Figure 2). Preoperative incision planning considered factors such as the exoskeleton implant size, the anatomical location of the injury, and the presence of pre-existing lacerations in the affected area. Craniofacial access was achieved using standard incisions, with or without extension, including coronal, pretrichial, transoral, and transconjunctival approaches. When feasible, existing traumatic lacerations were utilized as access points to facilitate a minimally invasive technique. Non-comminuted fractures, if present, were reduced with standard plating techniques. Comminuted bone pieces or bone grafts were placed onto the mesh for significant bone defects. Following reduction and repair, postoperative day 2 CT scans were performed to evaluate the accuracy of reduction and the fit of the reconstructed anatomical structures. All patients underwent surgical repair during their admission, typically within 5 to 7 days of injury presentation. Patients were followed up in the clinic weekly for the first 2 to 3 weeks postoperatively, then at the 1-, 3-, and 6-month marks.
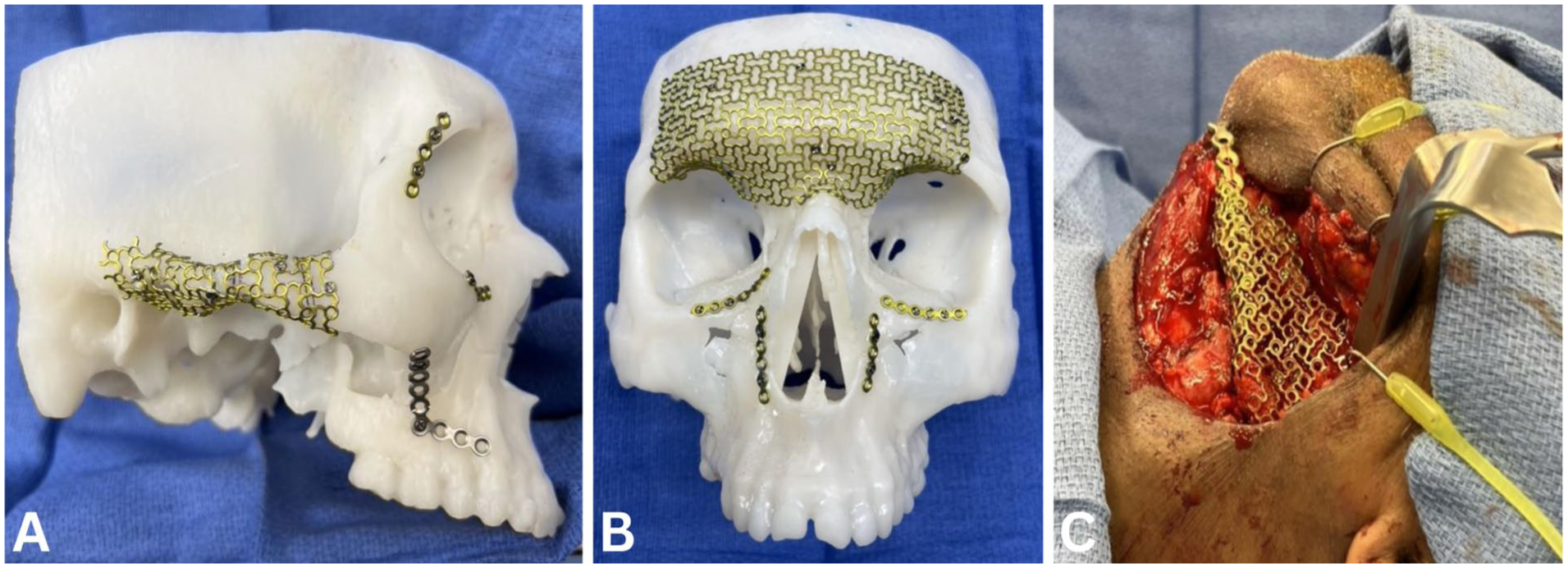
Titanium mesh exoskeleton examples. (A, B) Models and (C) in situ—mandible.
Results
Cohort Overview
A total of 23 patients with comminuted facial fractures underwent reduction and fixation using the titanium exoskeleton technique. Across these cases, 9 distinct craniofacial anatomical regions were involved. In total, 37 titanium meshes were utilized, with an average of 1.6 mesh applications per patient. Thirteen patients required intervention in multiple anatomical sites. The frontal sinus was the most reconstructed region (10 patients), followed by the naso-orbital ethmoid (NOE) complex (8 patients; Figure 3). Other frequently involved areas included the zygomatic arch (4), orbit (3), temporal fossa (3), zygoma (3), mandible (2), maxillary sinus (2), and frontal bone (2). Importantly, even in regions with higher risk of contamination such as the frontal sinus, where mesh contact with sinus cavities is common, no infectious complications were observed.
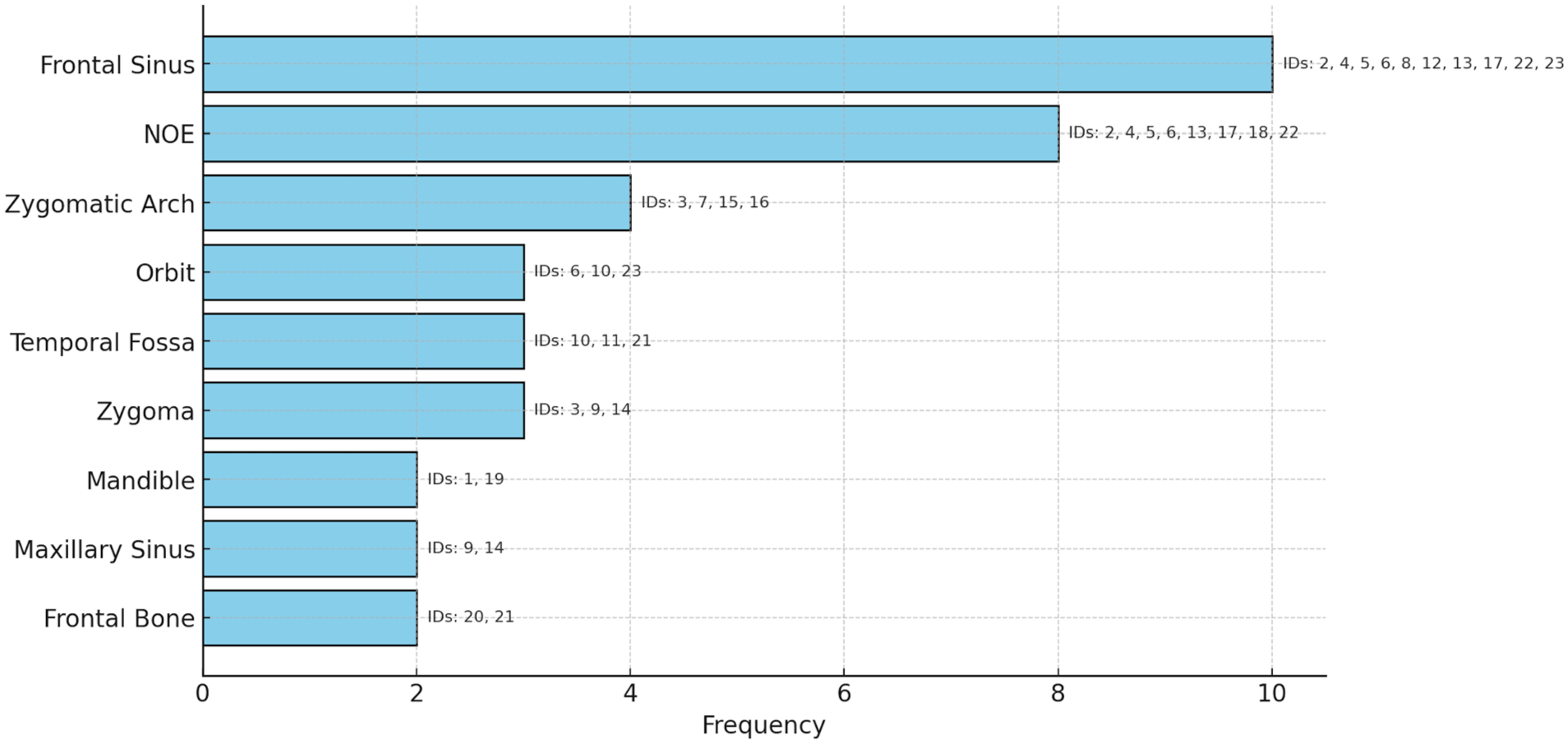
Region and frequency of 3D shaped titanium mesh.
Clinical Outcomes and Complications
The titanium mesh exoskeleton technique was successfully applied in all 23 cases, facilitating reliable intraoperative reconstruction aligned with VSP-based planning. Postoperative day 2 CT scans confirmed appropriate anatomic reduction and mesh positioning consistent with preoperative virtual models. Clinical assessments throughout follow-up indicated satisfactory restoration of form and function. Complications were minimal. All patients demonstrated primary wound healing without evidence of infection, hematoma, or mesh exposure, except for 1 patient who experienced partial intraoral exposure of his right maxillary mesh. This was addressed through minor revision surgery involving limited segmental mesh removal using right buccal incision. No cases of mesh loss, sinus-related complications, or secondary deformities were reported during follow-up.
Discussion
This study highlights the successful intraoperative application of a customized titanium exoskeleton technique for acute management of comminuted craniofacial fractures. By utilizing VSP 3D model creation, and intraoperative titanium mesh shaping, the technique achieved precise anatomical restoration, structural stability, and maintenance of secondary contours in all 23 patients that were treated, with postoperative imaging confirming accurate fracture reduction and alignment with preoperative plans. The results showed minimal complications, with only 1 case requiring minor revision for intraoral mesh exposure.
This technique offers reliable outcomes in cases involving severe comminution and bone loss, addressing complexities in the acute fracture fixation period and preventing secondary deformities related to an unstable, partially resorbed skeleton. In comparison to traditional fixation methods such as standard plates with or without immediate bone grafting—which carry risks of resorption, deformity, or secondary surgery, this approach provided anatomically correct 3-dimensional skeletal morphology and enhanced structural support while preserving native bone fragments. The exoskeleton acts as both a scaffold and fixator, enabling stabilization of diminutive and/or free-floating bone segments that would otherwise be discarded or inadequately secured. Bone fragments will have less tendency to resorb if fixated. 8
The titanium mesh used in all patients was thinner than a typical reconstructive midface or mandible fixation plate. Traditional methods of bone stabilization/stabilization utilize titanium with a single plane/vector load sharing or in the case of the mandible sometimes load bearing. As 3-dimensional strength increases when converting from a single vector plate to a chain plate, a comprehensive 3D titanium mesh provides stability across multiple vectors, and thus rigidity despite the lower profile nature. Of note, we have not seen any loss of 3D morphology in the postoperative period. Once the bone heals after 2 months, the absolute strength of the mesh is less important, but will, however, maintain contour in areas of decreased or absent bone support long term.
The findings of this study align with prior research on the use of titanium mesh craniofacial reconstruction. Titanium mesh use in reconstruction has versatility and biocompatibility for VSP technology, which has shown to improve surgical precision and reduce operative time.9,10 Compared to traditional methods like stock titanium plates or bone grafts, this customized approach offers superior anatomical accuracy and reduces the effects of complications like graft resorption or implant failure. 11 The intraoperative use of standard mesh, shaped to fit VSP-generated models, offers a cost-effective and reproducible method without requiring premade custom implants, combining the flexibility of intraoperative decision-making with the precision of digital planning.
Incision planning is essential in craniofacial reconstruction, especially when using large or complex implants. Common approaches like coronal, transconjunctival, and intraoral incisions are reliable access points with minimal scar noticeability. However, incorporating existing traumatic lacerations, as used in this study in combination with common approaches, can help the ability to place mesh, minimize soft tissue damage, and shorten operative time. Other studies have emphasized the impact of proper incision choice on surgical outcomes and complication rates, especially when mesh reconstruction is used for comminuted fractures.6,12 Achieving close contact between mesh and bony defect edges is key to promoting stability and integration long term. Literature on facial trauma shows that securing titanium mesh helps limit micromotion, improves alignment, and lowers risk of mesh exposure or infection.11,13 In our approach, using VSP-generated 3D models to shape the mesh intraoperatively allowed for more precise fit and a more secure fit to the defects.
An unexpected finding was the absence of infectious complications despite using mesh in high-risk areas such as the frontal sinus. This may be due to the nature of titanium mesh, which has been shown in other craniofacial mesh studies as being associated with a lower risk of infections than other materials like polyetheretherketone (PEEK).14-16 Other studies that investigated titanium mesh shaping in comminuted mandibular fractures emphasized the material’s ability to secure bone fragments with minimal infection rates and preserve morphology. 13 Additionally, the meticulous preoperative planning enabled by VSP and precise acute intraoperative adaptation of the sterile titanium mesh might be what minimized tissue disruption and infection rates in our patients. Our technique maintains sterility throughout the modification process because all sterile mesh contouring and trimming is performed intraoperatively on a pre-sterilized patient specific model within the surgical field. This minimizes handling, multiple OR procedures, and may contribute to the low infection rate seen in our series. This is significant as it suggests that customized titanium exoskeletons molded intraoperatively may reduce infection risks traditionally associated with implant use in anatomically challenging or contaminated regions.
Despite these promising results, some limitations merit discussion. This was a retrospective study at a single institution with a relatively small sample size. Long-term outcomes, including effects on soft tissue remodeling, mesh integration, and need for secondary interventions, require further evaluation. Additionally, while this study relied on in-house surgical expertise and established VSP protocols, widespread adoption may be limited by resource availability, team training, and cost considerations.
Conclusion
This study presents the largest series to date demonstrating the feasibility and effectiveness of a novel titanium exoskeleton technique for acute management of comminuted craniofacial fractures. By combining virtual surgical planning with intraoperative molding of standard titanium mesh on patient-specific models, this approach offers a precise, customizable, and structurally stable method for reconstructing complex facial injuries. The technique proved versatile across multiple anatomical regions and was associated with excellent clinical outcomes, minimal complications, and no implant-related infections—even in high-risk areas such as the frontal sinus.
Footnotes
Ethical Considerations
The study was conducted under the approval of the Institutional Review Boards (IRB) at Dell Medical School at The University of Texas at Austin (ID: Study00005292).
Consent to Participate
Informed consent was obtained from all individual participants included in the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Raymond J. Harshbarger III is a member of the Editorial Board of FACE and did not take part in the peer review or decision making process for this submission.
Data Availability Statement
Due to the nature of this study involving patient-specific surgical care, data are not publicly available to protect patient privacy.