
Abstract
With surgery-first approach, the skeletal discrepancy is corrected with orthognathic surgery at the start of treatment, but the teeth remain in their original compensated positions. This change in treatment sequence means clinicians have to determine what the occlusion immediately after the surgery, which is called transitional occlusion, should look like during the planning process. This report describes the surgical and orthodontic planning for a surgery-first case that corrected a large Cl III malocclusion. Virtual planning was used to reverse engineer the transitional postsurgical occlusion from the final ideal position. A multiplatform software can be a powerful tool for analyzing problems in finishing a surgery-first case, predicting outcomes, and improving the accuracy in planning surgery-first approach.
Introduction
Over the past few decades, the surgery-first approach has become a popular method in orthognathic surgery, particularly in Asian countries. Numerous case reports and studies have been published that point to a new paradigm shift in the field of orthodontics and orthognathic surgery treatment.1-3
The surgery-first approach has gained popularity due to several advantages. One of the most important advantages is higher patient satisfaction. Since surgery-first patients do not have to undergo a long period of presurgical orthodontic treatment, the soft and hard tissue esthetics improve immediately at the beginning of treatment. Previous studies have reported that with the surgery-first approach, quality of life related to oral health also improved immediately after surgery, whereas it worsened during the presurgical orthodontic treatment with the conventional surgical-orthodontic approach.4-6
However, some questions still remain unanswered regarding surgery first cases. Previous studies draw conflicting conclusions regarding postsurgical stability of the surgery-first approach.7,8 Also, several researchers differed on the indications, treatment protocol, and planning methods for the surgery-first approach; therefore, a consensus on the protocol has not yet been reached.
With the surgery-first approach, there is a change in treatment sequence. The skeletal discrepancy is initially corrected with orthognathic surgery at the start of treatment, but the teeth remain in their original compensated positions. The occlusion immediately after surgery is not in an ideal position, and clinicians have to determine what this temporary malocclusion, which is called transitional occlusion, should look like during the planning process. The proper transitional occlusion is the key to successful postsurgical orthodontic treatment as it ensures an ideal final occlusion. If the transitional occlusion is not planned correctly in the corrected skeletal position, then prolonged orthodontic treatment is inevitable due to unexpected tooth movements. In the worst case, compromised treatment results or even the need for additional orthognathic surgery may be needed to correct any remaining discrepancies.
Planning for a proper transitional occlusion is critical as the extent and direction of postsurgical decompensation have to be predicted beforehand. Even though some guidelines have been proposed, correct planning of the transitional occlusion can still be quite challenging.9-11 It is also the reason why the previous articles on surgery-first planning state that sufficient experience of the clinician is important for surgery-first approach planning.3,10
Virtual surgical and orthodontic planning can reduce the risk of a poor outcome due to incomplete correction and increase reproducibility by anticipating and testing the skeletal and tooth movement needed to finish the case. A few previously published articles describe the orthodontic and skeletal simulation process for the virtual treatment planning for surgery-first cases.12-14 However, the way to determine the proper transitional occlusion using virtual planning has not been discussed. Virtual planning is an important tool that can be used to reverse engineer the transitional postsurgical occlusion from the final ideal position. The treatment sequence has 3 occlusions: the initial T1 occlusion, the postsurgical T2 transitional occlusion and the final T3 occlusion. In this report, the detailed planning process for transitioning among the 3 occlusions is described. In addition, the final result is compared with the planned position to validate the treatment planning process.
Diagnosis and Etiology
A 19-year old male with a chief complaint of mandibular protrusion presented to the orthodontic clinic at. His initial records included virtual models made from an intraoral scanner (TRIOS; 3Shape, Copenhagen, Denmark), photographs, panoramic radiograph, lateral cephalogram, and cone-beam computed tomography (CBCT) scans.
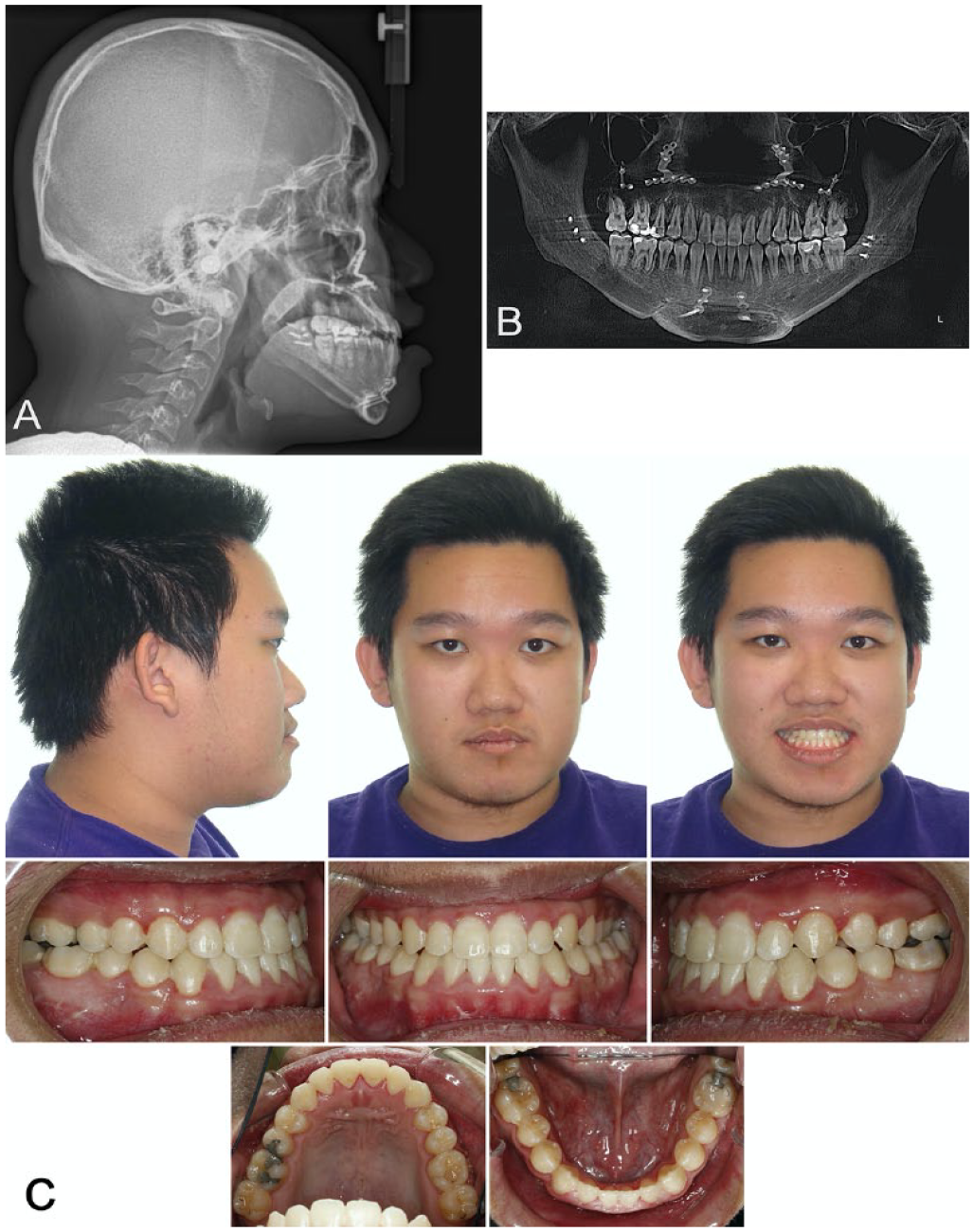
The patient was diagnosed with a skeletal class III pattern with prognathic mandible and retrusive maxilla. During the clinical intraoral exam, a class III canine and molar relationship was noted as well as a −10 mm of negative overjet and bilateral posterior crossbite. The lower incisors were in a retroclined position due to compensation to the skeletal discrepancy. Because of the lack of opposing teeth, severe extrusion of the upper second molars was also observed (Figure 1).
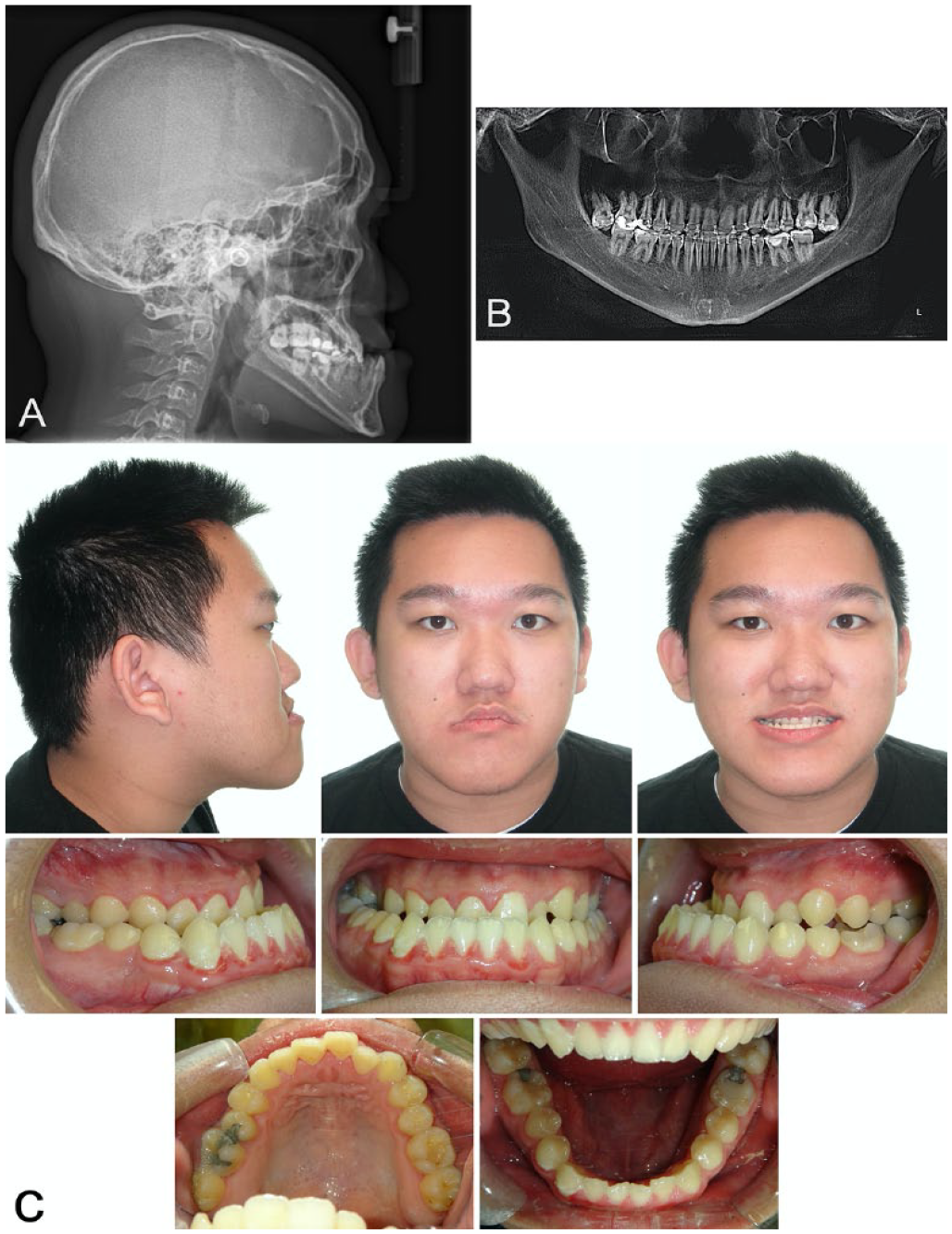
Pretreatment records: (A) lateral cephalogram, (B) panoramic radiograph, and (C) intraoral photographs.
Treatment Objectives
The treatment objectives included correction of the facial profile and skeletal discrepancy, leveling and alignment of the dentition, ideal overjet and overbite, and Class I canine and molar relationships.
Treatment Planning
Considering the amount of skeletal discrepancy, orthognathic surgery combined with orthodontic treatment was necessary. The conventional orthognathic approach consists of 3 steps: presurgical orthodontic treatment, orthognathic surgery, postsurgical orthodontic treatment.
The patient attended a college that was located over 350 miles away from. Originally, we considered collaborating with an orthodontist near his college to apply the conventional surgical-orthodontic approach; however, he asked whether it was possible to complete the treatment in one semester if he took one semester off. Given his motivation for early correction of his malocclusion and profile, we decided to apply the surgery-first approach to his case.
For prediction of orthognathic surgery and postsurgical orthodontic treatment, three-dimensional (3D) virtual treatment planning was performed using virtual planning software (Nemostudio; Nemotec, Madrid, Spain).
Step 1. Virtual Orthodontic Setup
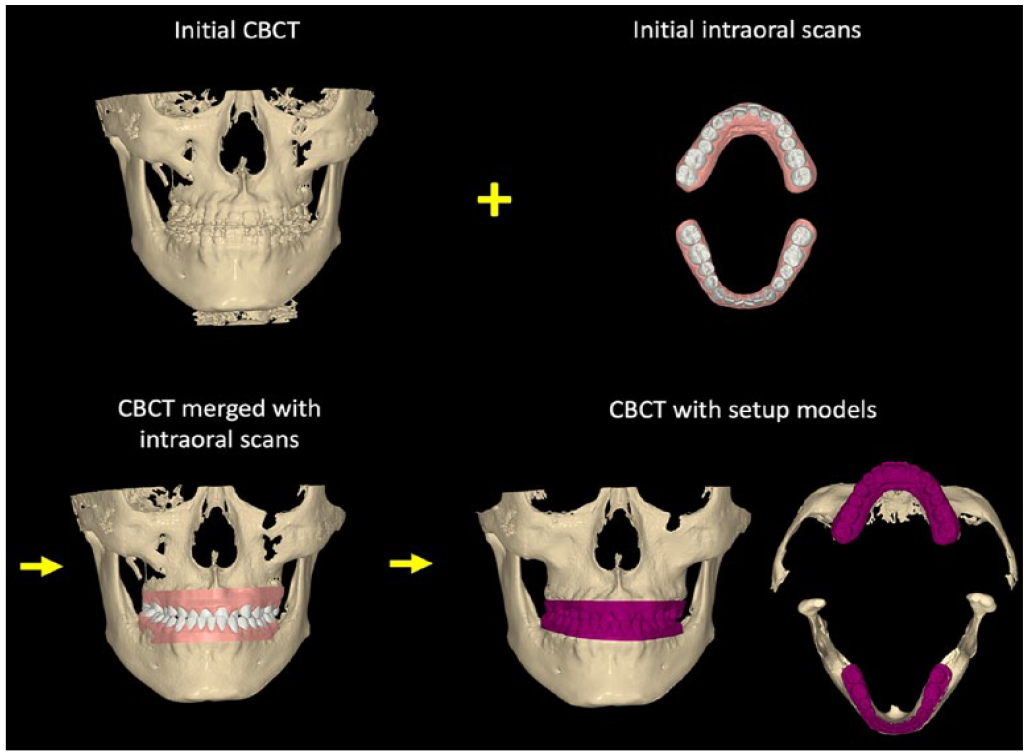
Virtual models were made from the intraoral scans and merged with reconstructed 3D images from CBCT scans. On the virtual models, each tooth was segmented for orthodontic tooth movement. The virtual orthodontic setup consisted of decompensation to achieve coordinated arch forms and ideal incisor positioning (Figure 2A). To predict and calculate the amount of movement for each tooth, both crown and root position were evaluated. The root configurations were made from CBCT scans that were superimposed to the crowns from the virtual models, enabling a precise prediction of both crown and root movement needed for decompensation (Figure 2B). The orthodontic setup was similar to the decompensation achieved with conventional presurgical orthodontic treatment. After teeth were repositioned to the ideal position, the upper and lower setup models were virtually fit together to check if they were in ideal occlusion. This check permitted fine-tuning of the setup position. Figure 3 shows the T3 final skeletal and dental positions after virtual orthodontic setup.
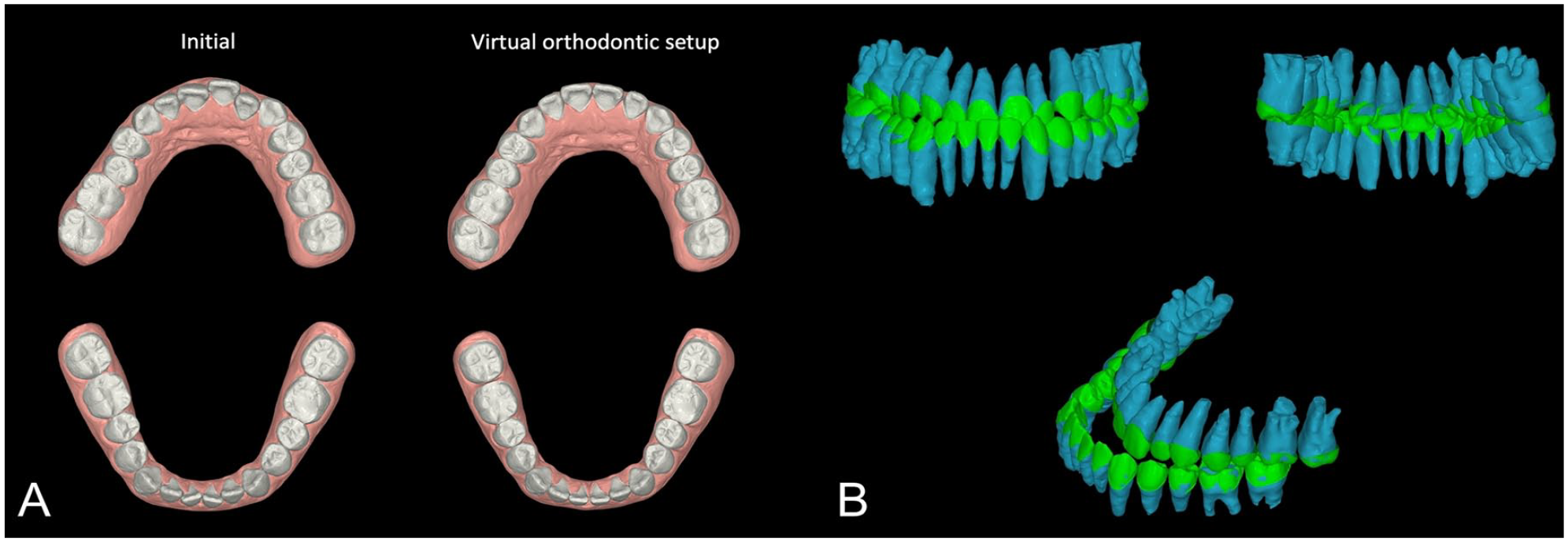
(A) Virtual orthodontic setup and (B) teeth positions including root configurations.
Process of virtual presurgical orthodontics.
Step 2. Virtual Surgical Repositioning
The next step was a surgical plan based on the physical examination, the cephalometric analysis and the virtual 3D setup. During the physical examination, the dental and facial midlines, canting of dental arches, maxillary and mandibular incisor position relative to a vertical line from glabella, incisor display on smiling and repose, maxillary yaw seen from a bird’s eye view and mandibular yaw from a worm’s eye view were recorded. The cephalometric analysis started with a proportionate analysis that can give the location of the maxillary central incisors in a well-proportioned face as well as evaluate the need for rotations of the occlusal plane. 15 The analysis and surgical simulation was checked against standard surgical cephalometric lines and angles. 16 During the simulated 3D virtual surgery, the computer-generated midline was checked against the midline from our physical examination before the surgical segments were moved into their target positions. Yaw and any angulation of the midfacial plane were checked as well. During the 3D virtual surgery, surgeons could modify the surgical plan before it was finalized for splint fabrication. The surgical plan consisted of combined LeFort I maxillary advancement, mandibular setback (bilateral sagittal split osteotomy), and genioplasty. Once the skeletal movements were done virtually, the skeletal positions were fine-tuned by placing the maxilla and mandible in an ideal occlusion with positive overjet, positive overbite, and class I canine/molar relationship (Figure 4B). The objective of this step was to start by generating the T3 final outcome. Figure 4C shows the T3 final skeletal and dental positions at the end of treatment as defined by the software. This position would be used to reverse engineer the transitional occlusion for the surgical splint.
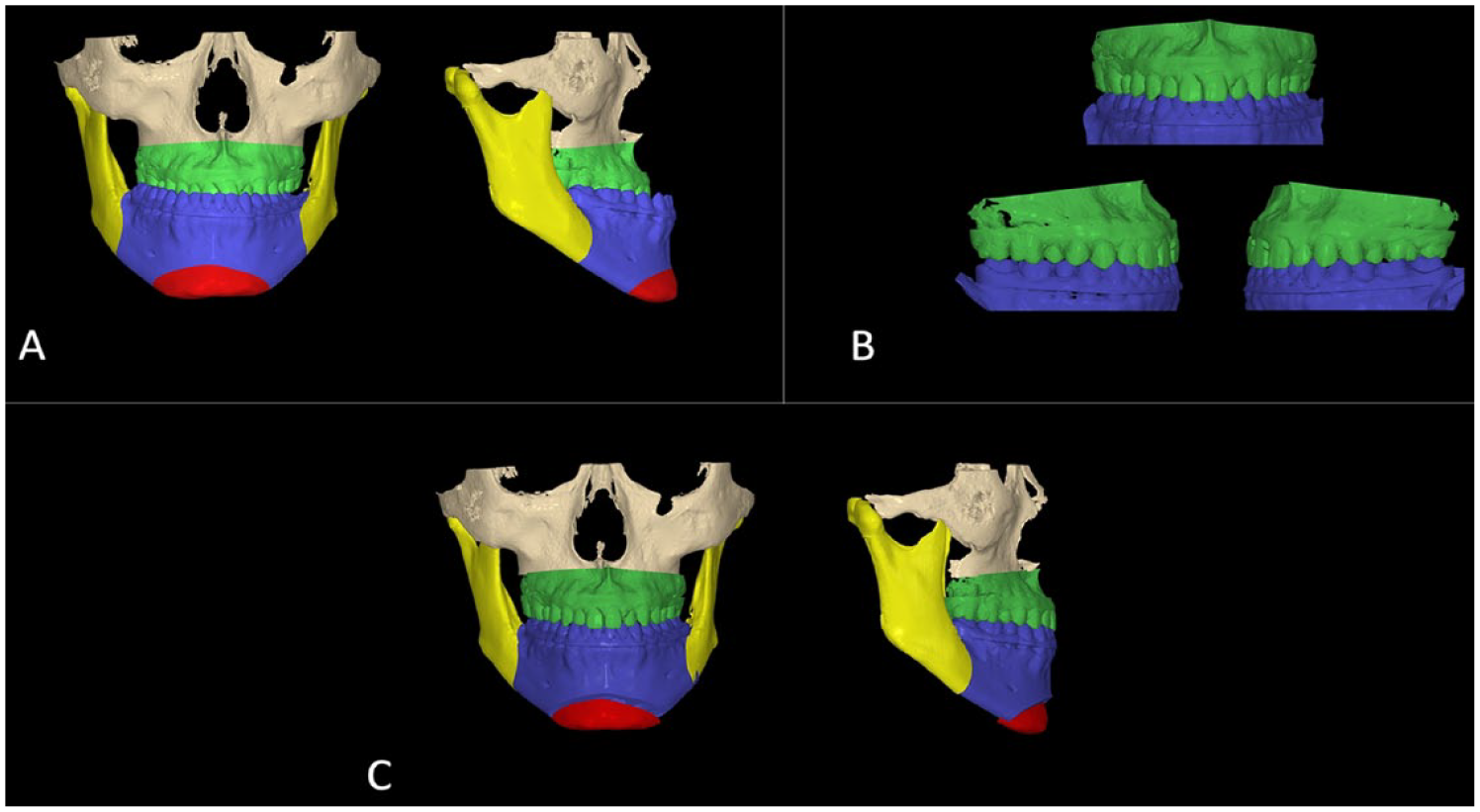
Process of virtual surgical repositioning: (A) initial skeletal positions with osteotomy, (B) setup models fitted to the ideal occlusion, and (C) final skeletal and dental positions.
Step 3: Determining the Transitional Occlusion
The T2 transitional occlusion was made from initial models placed in their postsurgical position. The reverse engineering step required swapping the idealized T3 final models with the initial, untreated T1 models while maintaining the ideal skeletal positions (Figure 5B). The T2 transitional occlusion captured the skeletal movements during the surgery and was needed to make the surgical splints for orthognathic surgery. In this case, both an intermediate and final splint were made from the T2 position. The software could 3D print the surgical splints. Since no orthodontics had been done prior to surgery, the maxillary and mandibular dentition would not fit into an ideal intercuspated relationship. Malpositioned teeth caused maxillary and mandibular dental cusps to collide and interfere in the transitional occlusion. To compensate for occlusal interferences (Figure 5C), the mandible was rotated clockwise to open the bite in order to avoid any posterior interferences in the antero-posterior and transverse dimension (Figure 5D). Eventually, this open bite would be closed in a clockwise direction between the T2 transitional occlusion and the T3 final occlusion during active orthodontic tooth movement.
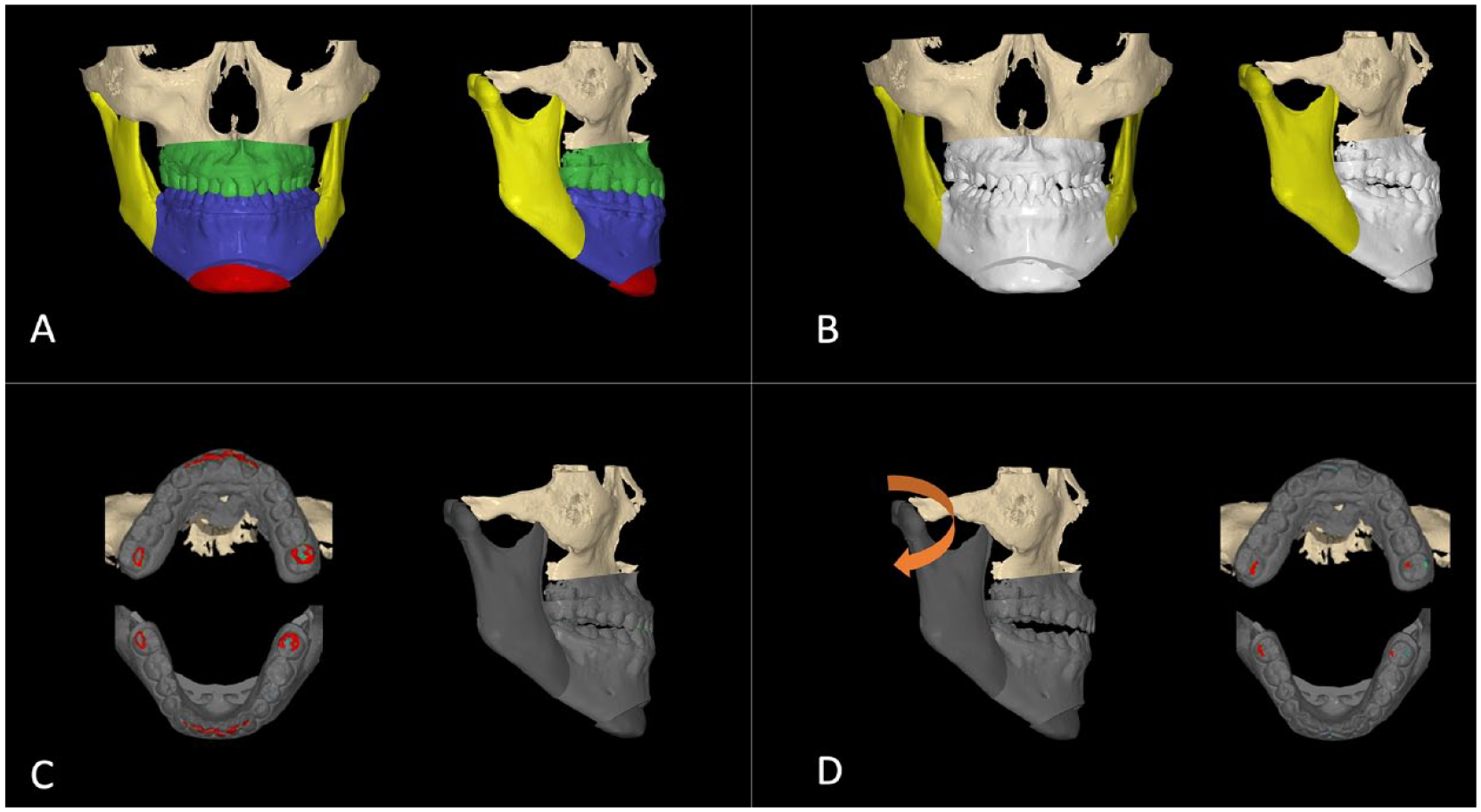
Process of determining the transitional occlusion: (A) the T3 final skeletal position with setup models, (B) initial models were substituted for setup models, (C) dental collisions, and (D) mandible rotated clockwise to avoid the dental collisions.
The patient underwent orthognathic surgery as planned and postsurgical orthodontic treatment was initiated 6 weeks after surgery. Minor crowding was corrected, the dentition was decompensated, and a 5 mm of lateral open bite was closed during the postsurgical orthodontic phase.
Treatment Results
The final result was shown in Figure 6. The orthodontic treatment time was 4 months from bonding to debonding. The total treatment time for surgery and orthodontic treatment was 5.5 months.
Posttreatment records: (A) lateral cephalogram, (B) panoramic radiograph, and (C) intraoral photographs.
Discussion
This report describes the surgical and orthodontic planning for a surgery-first case that corrected a large Cl III malocclusion. The main difference between the conventional orthognathic approach and the surgery-first approach is the sequence for decompensating the untreated malocclusion. In the conventional approach, decompensation occurs prior to surgery during the presurgical orthodontic phase of treatment. Therefore, the occlusion with ideal overjet, overbite, and canine/molar relationship is set up to guide surgical segmental movements. 17 On the other hand, with the surgery-first approach, the orthodontic decompensation occurs after the surgery has taken place. Thus, the transitional occlusion with untreated initial models is used to plan surgical movement. Orthodontic bonding occurs after surgery in order to move teeth from the T2 transitional occlusion into the ideal T3 final occlusion.3,10,11
Precise evaluation of the initial dental and skeletal problems is the first step for planning the transitional occlusion. In individuals with Class III skeletal patterns, teeth are usually compensated to adapt to the current skeletally discrepant position due to an altered balance of tongue and lip pressure. 18 In the transverse dimension, maxillary molars tend to incline buccally, and mandibular molars tend to incline lingually. 19 Also, in the antero-posterior dimension of a Class III malocclusion, the maxillary incisors are usually proclined and the mandibular incisors are retroclined. 20 In this case, the amount and direction of compensation were carefully defined by evaluating virtual tooth positions containing root configurations (Figure 2B).
In this case, the transitional occlusion was reverse engineered using virtual orthodontic treatment planning combined with virtual surgical planning utilizing Nemostudio software. Swapping the T3 final models which were used to plan surgical movement with the initial T1 models provided the exact position of the T2 transitional occlusion following surgery.
Another issue that needs to be considered when planning the surgery-first approach is changes to the skeletal position after surgery as the occlusion is corrected. Several studies comparing postsurgical skeletal positions between a surgery-first approach group and a conventional surgery group showed that the mandible tended to rotate in a counterclockwise direction after surgery in the surgery-first approach group.7,8,21 It was also reported that the chin point of the mandible was positioned forward as the mandibular plane angle decreased with the counterclockwise rotation. 22
The transitional occlusion usually has a tendency for anterior open bite due to a scissors effect from posterior crown interferences and few occlusal contacts. This clockwise mandibular rotation can be amplified when upper second molar extrusion is present. In this case, transverse interference was noted in the surgically corrected setup due to presurgical buccal tipping. As teeth are leveled and decompensated during the postsurgical orthodontic phase, these teeth uprighted and relieved the occlusal interferences. Concomitantly, the bite closed in a counterclockwise direction, decreasing the vertical dimension as the maxillary molars went from a buccally tipped transverse position to an upright position.22-24 In other words, the transitional T2 skeletal position and occlusion with the temporary bite opening from transverse interferences differed from the final skeletal position and occlusion,10,25 and it complicates a precise prediction of the treatment outcome.
If the counterclockwise rotation is not considered during the surgical planning step, the final skeletal position will not be the same as the planned final outcome. This potential issue was addressed in this case by using reverse engineering during treatment planning. After substituting the setup models with initial models, dental collisions in the incisor and molar areas were noticed (Figure 5C). The transitional occlusion was determined after rotating the mandible clockwise by 2.4 degrees until occlusal collisions were relieved (Figure 5D). By this method, postsurgical skeletal changes due to changes in the occlusal vertical dimension during postsurgical orthodontic treatment could be fully predicted and incorporated in the planning process.
For the virtual treatment planning to be reproducible in actual treatment, predicted virtual tooth movement should correlate with actual tooth movement. To confirm whether the mandibular position changed as predicted, lateral cephalograms at T1, T2, and T3 were superimposed. Comparison of T2 and T3 lateral cephalograms showed that the mandible rotated counterclockwise during the postsurgical orthodontic treatment. The amount of rotation that occurred was 2.3 degrees, which was similar to the planned amount. Anterior movement of the chin point due to the counterclockwise rotation was also observed as predicted. Superimposition of the planned final skeletal position and the actual final CBCT images showed the overall treatment planning was precisely reproduced.
Virtually planned setup models and final virtual models made with an intraoral scanner (Itero element; Align technologies, San Jose, Calif) were also superimposed to verify whether orthodontic tooth movement occurred as predicted. Some differences were noticed, especially in the transverse width in the mandibular arch, which led to a slight posterior crossbite tendency on the left side in the final occlusion. Baan et al described possible differences between diagnostic virtual presurgical orthodontic setup and the actual final outcome with presurgical orthodontics. 26
The surgical and orthodontic planning software may improve predicted and final dentition outcomes by precisely planning the T3 final tooth and bracket positions and transferring those positions during initial bonding of brackets by using by 3D printed indirect bonding trays. In addition, the same surgical and orthodontic planning could be used with prefabricated sequential clear aligners. Clear aligners could be 3D printed during the planning process before surgery and delivered right after surgery; thereby reducing chair time at future appointments. Although some types of tooth movement are reported to be less reliable with clear aligners,27,28 digital setups are the basis for aligner treatment planning. All of the orthodontic tooth movement can be reliably reverse engineered and incorporated into the overall treatment plan.29,30
One reason for using conventional orthodontic brackets in this case was the postsurgical closure of lateral open bite. The orthodontic plan is based on what types of mechanics, appliances and skeletal anchorage devices an orthodontist may use in postsurgical orthodontic treatment. The patient had 5 mm of lateral open bite in his transitional occlusion. In the virtual orthodontic setup step, the open bite was planned to be mainly closed by posterior teeth extrusion. Therefore, posterior box elastics was used to close the open bite during the actual postsurgical treatment process. In cases with large amounts of lateral bite opening, temporary anchorage devices (TAD) with extrusion springs can be used for extrusion as well. 31 Although we did not used TADs in this case, molar intrusion using TADs can also be considered as an option for treating the open bite caused by over-erupted maxillary second molars. In such cases, molar intrusion will cause more mandibular counterclockwise rotation and shortening of the lower face height. The exact amount of bite closure and counterclockwise rotation of the mandible can be calculated with virtual planning.
The postsurgical orthodontic treatment time was 4 months. It was reported that the surgery-first approach can shorten treatment time32,33 One mechanism for accelerated tooth movement proposed by Liou et al is that higher osteoclastic activities and metabolic changes triggered by orthognathic surgery accelerates postsurgical orthodontic tooth movement.34,35 This accelerated orthodontic treatment can also be an important advantage in adult surgical orthodontic treatment.
Summary and Conclusions
Virtual treatment planning with the reverse engineering method was used to determine the transitional occlusion in this surgery-first approach case. A multiplatform software can be a powerful tool for analyzing problems in finishing a surgery-first case, predicting outcomes and improving the accuracy in planning surgery-first approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
All clinical information provided is in accordance with the CARE protocol for case reporting and it was written in accordance to the Helsinki Declaration. Informed consent was obtained from the patient for scientific purposes.