
Abstract
Introduction:
To describe the orthodontic-surgical approach we used in a sample of patients affected by the horizontal type of Unilateral Condylar Hyperplasia (UCH), that is a progressive disease that leads to mandibular asymmetry and midline deviation.
Material and Methods:
A retrospective observational cohort study was designed on 29 consecutive patients affected by horizontal UCH (23 females, 6 males; mean age, 22.4 y.o. ± 7.9) treated in the Units of Orthodontics and Maxillo-Facial Surgery. Descriptive statistics was performed. Correlations were tested between type of surgery and stage of skeletal maturation, presence of Temporo-mandibular Disorders, and condylar activity, evaluated with SPECT. Duration was correlated with type of surgery, and the mean duration of therapy was compared between patients who underwent condylectomy and those who underwent orthognathic surgery.
Results:
Females were more affected than males and had higher mean age. Temporo-mandibular Disorders were present in 31% of the sample. All patients with positive SPECT (15) were treated with condylectomy, alone or associated with orthognathic surgery, followed by post-surgical orthodontics. Patients with negative SPECT were treated with orthognathic surgery if adult (12), condylectomy if in age of skeletal growth (2).
Discussion:
The choice of the therapeutic approach has depended on skeletal maturation, condylar activity, and extent of dental compensations. Early condylectomy eliminates the etiologic cause of the Hyperplasia in patients with active condylar growth. In patients in age of growth, either if positive or negative to SPECT, early TMJ surgery eliminates the asymmetric growth and leads to symmetrization of the mandibular growth rate, acting as interceptive treatment.
Keywords
Introduction
The Unilateral Condylar Hyperplasia (UCH) is a disease characterized by the excessive growth of a mandibular condyle compared to the contralateral side, that leads to a progressive facial asymmetry affecting occlusion and masticatory function.1,2 Etiology is still not clear. Among the aetiologic causes of the primary form, literature has reported over the years vascular, hormonal, traumatic, inflammatory, neoplastic, and genetic (linked to the Y chromosome with autosomal dominant factor) causes, as well as increased masticatory load. The secondary form is the result of a functional compensation that occurs in patients affected by a contralateral primary hemimandibular hypodevelopment. 3 Pathogenesis seems related to the accelerated growth of one condyle with respect to the contralateral, or to a prolonged unilateral condylar activity after the end of the period of physiological growth. 4
The UCH may develop at any age, although it was reported that the second decade is the more common age of onset; an interval of 1 to 2 years elapses between age of onset and first consultation, when the progression of the condylar activity determines a clinically evident facial asymmetry, malocclusion, or temporo-mandibular disorders. 1
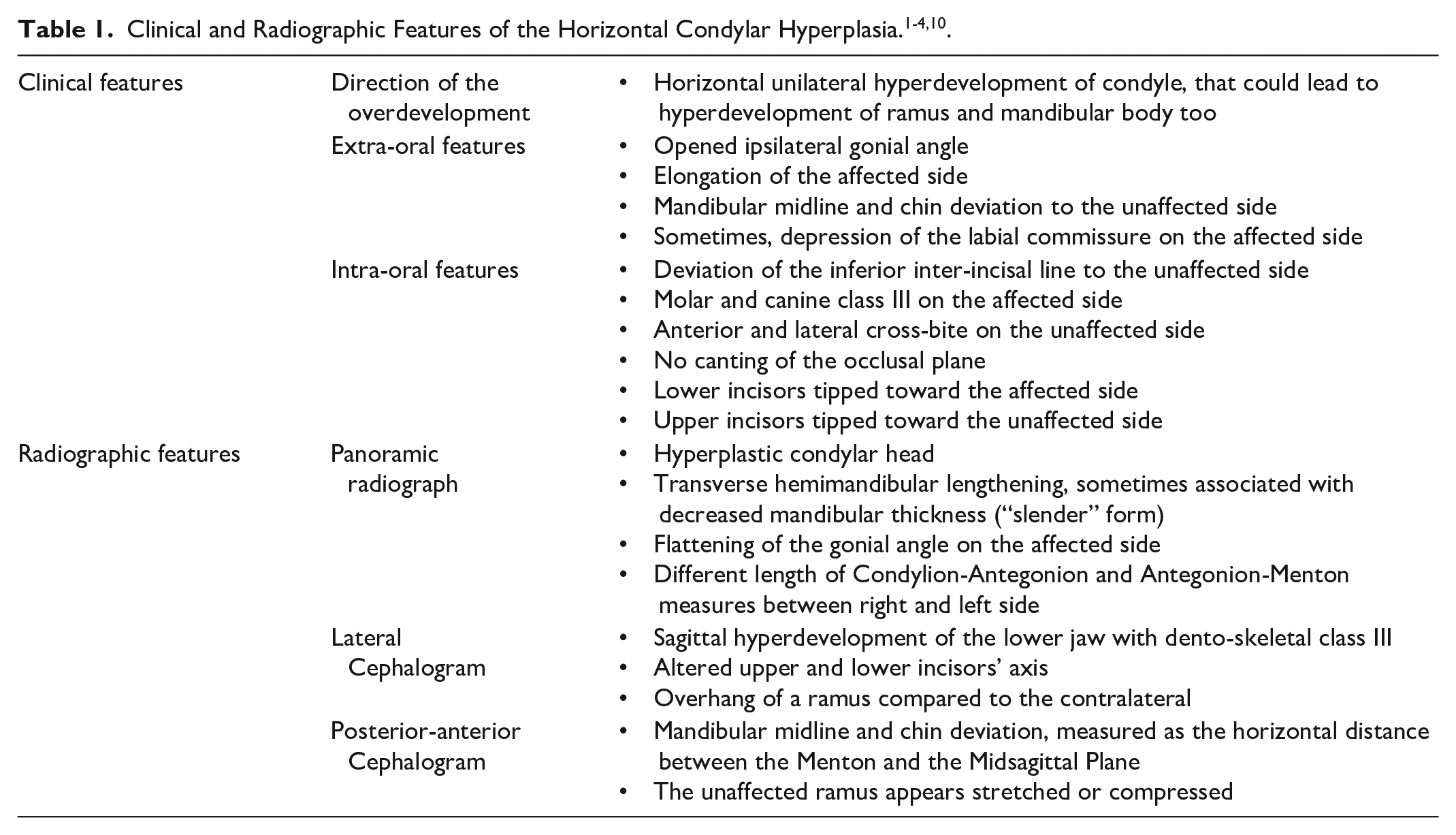
The extra- and intra-oral clinical features of the malocclusion resulting from UCH are not homogenous for all the patients at first consultation, mainly for the progressive nature of the disease and for the direction of condylar overgrowth (vertical, horizontal or hybrid, which has the clinical characteristics of both), that could determine different clinical and radiographic characteristics. 5 The horizontal pattern is characterized by a complex clinical picture related with the time elapsed from the onset of the hyperplasia, but the constant clinical feature is the “asymmetrical prognathism” with asymmetry of the facial lower third, deviation of chin and mandibular midline toward the healthy side without involvement of the maxillary occlusal plane, that not do not show canting, and class III relationships on the affected side6-8 (Figure 1A-C); the condylar hyperdevelopment could lead to elongation of both ramus and body on the affected side 9 (Table 1).

(A-C) Intra-oral features of a patient affected by right horizontal UCH.
Several terms are used to define the horizontal pattern of growth of the UCH. “Horizontal type” is the definition used in classifications based on mechanisms of pathological development and on growth vector, like that of Nitzan et al. 1 The horizontal UCH was called “Hemimandibular Elongation” in the morphologic classification of Obwegeser and Makek, for the typical lengthening of condyle, ramus and mandibular body on the horizontal plane. 10 The Wolford et al’s classification is based on morphologic, radiographic, surgical and histopathologic features and describes the “type 1” as a unilateral or bilateral progressive self-limiting condylar hyperplasia that occurs mainly during puberty, with a predominant horizontal growth vector and an almost physiological condylar architecture. 6
Diagnosis is based on a clinical and instrumental diagnostic path that correlates clinical and radiographic signs. Panoramic radiograph is the first instrumental examination able to detect differences between the 2 sides of the lower jaw, with evidence of the hyperplastic condyle associated often with a unilateral lengthening on the transverse plane.9,11 (Table 1, Figure 2) As the horizontal UCH develops mainly on the transverse plane, the lateral cephalometric radiograph does not show specific features, while the posterior-anterior cephalometry is able to measure the mandibular midline deviation and the position of gonial angles on the coronal plane, with respect to the midline. Patients affected by facial asymmetry present a malocclusion involving the 3 planes of the space, therefore a 3-dimensional assessment performed on Cone Beam Computed Tomography is now preferred to reduce the errors caused by distortion or magnification of the 2-dimensional cephalograms.11-13

Panoramic radiograph showing the right hemimandibular lengthening and the flattening of the gonial angle on the affected side.
UCH has gained interest in the orthodontic/orthognathic literature in the recent years, especially regarding the surgical protocols. Few papers report the radiographic characterization and orthodontic considerations, therefore the treatment of this pattern of facial asymmetry is still not standardized.3,5,8,14-16 The orthodontic-surgical approach for the correction of the dento-skeletal malocclusion was based for a long time on orthognathic surgery and pre-surgical decompensation, like the other dento-skeletal malocclusions; secondary procedures were used to correct the residual asymmetry of chin and mandibular body. The improved knowledge of the pathogenetic mechanism has well established the self-limiting nature of the disease, therefore the assessment of the activity of condylar growth is critical to determine the orthodontic-surgical therapeutic strategy. The different growth activity between the 2 condyles, previously assessed with planar scintigraphy, is actually assessed with SPECT: a difference of condylar activity between affected and unaffected side greater than 10% was used as cut-off to indicate SPECT as “positive” and the UCH as “active.”3,6,17 Compared to patients affected by the vertical type, those affected by horizontal UCH showed lower difference in the radionuclide uptake between affected and healthy condyle.8,18
If a mandibular condyle is actively growing, the early condylectomy eliminates the active condyle and stops the progression of the asymmetry. To date, various surgical protocols and techniques are described in literature, and many patients may need simultaneous or subsequent orthognathic surgery as additional procedures to improve the remaining structural or esthetic asymmetry.6,12,17,19-21
To date, few papers have described the orthodontic management of UCH; the approach could vary, according to the direction of the hyperplasia, the associated occlusal compensations, the surgical approach chosen.2,22,23 Aim of this paper is to describe the population of patients affected by the horizontal form of UCH treated in our Unit, along with the Unit of Maxillo-Facial Surgery, to analyze the factors that have influenced orthodontic-surgical treatment and timing, and how the orthodontist deals with the dento-alveolar compensations proper of the disease.
Materials and Methods
A retrospective observational cohort study was designed on a population of patients affected by UCH who sought first consultation in our Unit of Orthodontics, together with the Unit of Maxillo-Facial Surgery, in a 3-years period lasting from 2017 to 2020. Patients diagnosed with horizontal UCH and who completed the entire treatment were included in this study. Patients affected by vertical UCH, other dento-skeletal diseases, congenital malformations, those who underwent previous maxillo-facial treatments, incomplete treatments, or clinical documentation, were excluded.
The diagnostic protocol we routinely use for UCH patients consists in: anamnesis and medical history, which also includes old photographs and radiographs; clinical extra-oral and intra-oral examination, photographic records; study of plaster models; radiographic study, once composed by panoramic radiograph, lateral and posterior-anterior cephalograms, and now replaced by Cone Beam CT-reconstructed images; assessment of condylar functionality with TMJ MRI and electrokinesiography, if patients were affected by Temporo-Mandibular Disorders. A CBCT-derived three-dimensional model of the skull was manufactured to simulate the eventual need of orthognathic surgery if dental malocclusion was significant. Condylar activity was assessed with SPECT tomography, while canting of the occlusal plane was assessed with plaster casts mounted on articulator or on the CBCT-reconstructed 3-dimensional image of the skull.
Two senior Authors, experienced in orthodontic-surgical diagnosis and treatment of dento-facial deformities, confirmed the diagnosis and treatment decisions, based on condylar activity and stage of craniofacial growth. All patients underwent surgery with fixed orthodontics (0.022 × 0.028 in. slot) until first or second molars if present, and were followed until the end of treatment, when they were prescribed to wear retainers for at least 1 year. The surgical technique for condylectomy was a modified proportional condylectomy, called Slice Functional Condylectomy, that consists in removing slices of the hyperplastic bone until the planned amount was removed and the mandibular midline centered, meanwhile checking the position of condyle in the fossa and the correct function between disk and condyle. In this way, the anatomical structures and the total respect of joint functionality were ensured.21,24
The data collected for this study were: age at the time of diagnosis, gender, affected side, occlusion, presence of TMJ disorders, condylar activity at time of diagnosis, type of surgery and duration of therapy. The Cervical Vertebral Maturation index (CVM) was used to detect patients in age of growth (CVM < 5) from those who were at the end. 25 Descriptive statistics was performed.
To analyze the relationship between type of surgery performed (condylectomy or orthognathic surgery) and stage of cervical vertebrae maturation, presence of TMJ disorder, positivity to SPECT, we first created a 2 × 2 table, then Fisher’s exact test was applied, indicated in samples with a small total number of observations and when some of the expected frequencies are less than 5. Spearman’s non-parametric rho test was used to analyze if duration of therapy was correlated to type of surgery performed. The null hypothesis was that variables are not correlated.
After the assessment of normality and homogeneity of variances, the Student’s t test for independent data was used, to test if the mean duration of the orthodontic therapy in the group who underwent condylectomy was significantly different from the orthognathic surgery group. Significance was set with P < .05. Data were analyzed with the R software, version 4.1.1 (https://www.rproject.org/). The protocol was approved by our Department and by the local University Ethical Board, prot. n. 4632.
Results
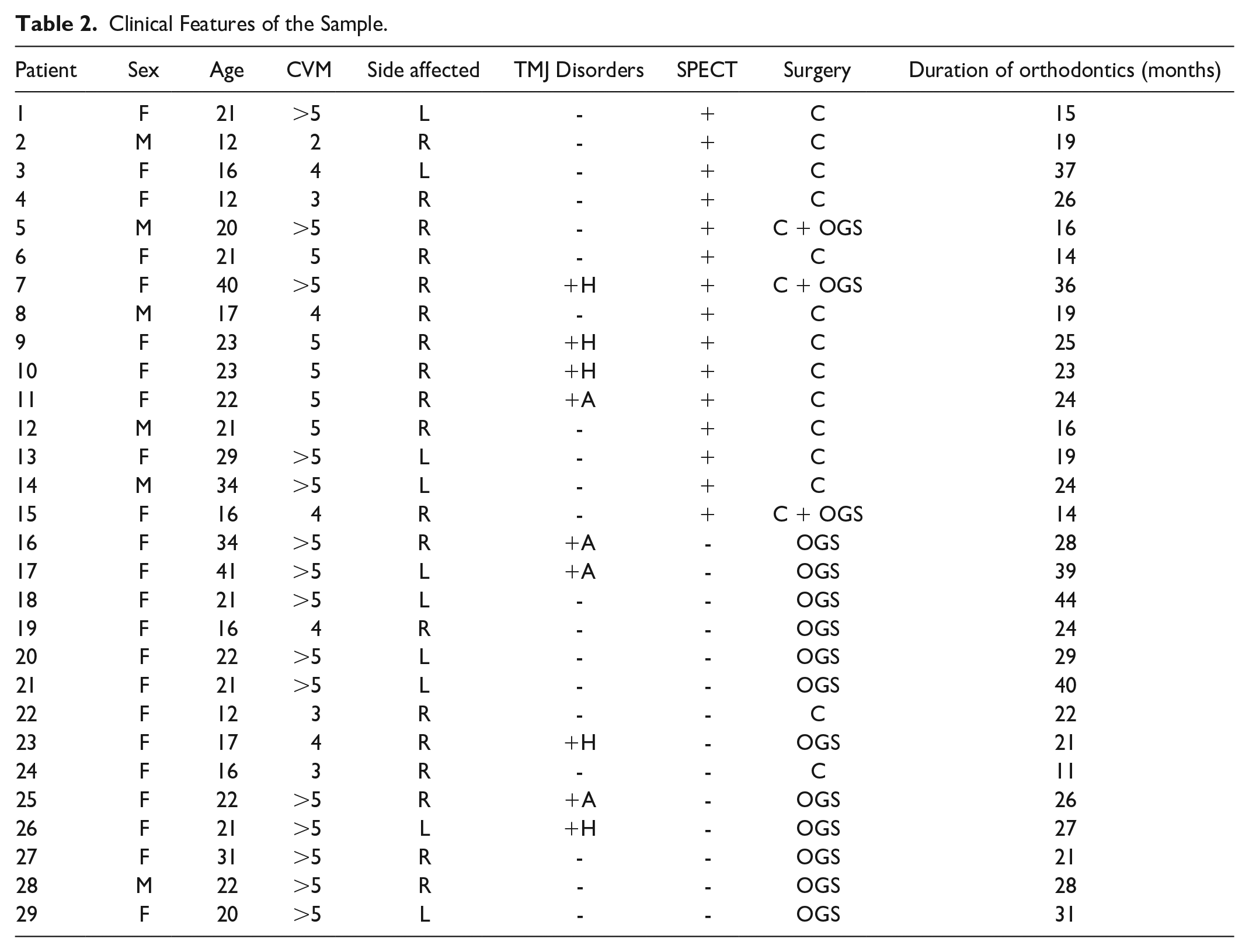
In the period considered for the study, out of a total of 67 patients diagnosed with UCH, 29 were classified as affected by horizontal UCH and included in the study, 23 female (79.3%) and 6 male (20.6%). (Table 2) The mean age at the time of diagnosis was 22.4 y.o. (S.D 7.9, minimum 12 y.o, maximum 41 y.o.), the mean was slightly higher in the female group. Nine patients were diagnosed in age of growth and 20 at the end (Table 3).
Clinical Features of the Sample.
Descriptive Analysis of the Sample.
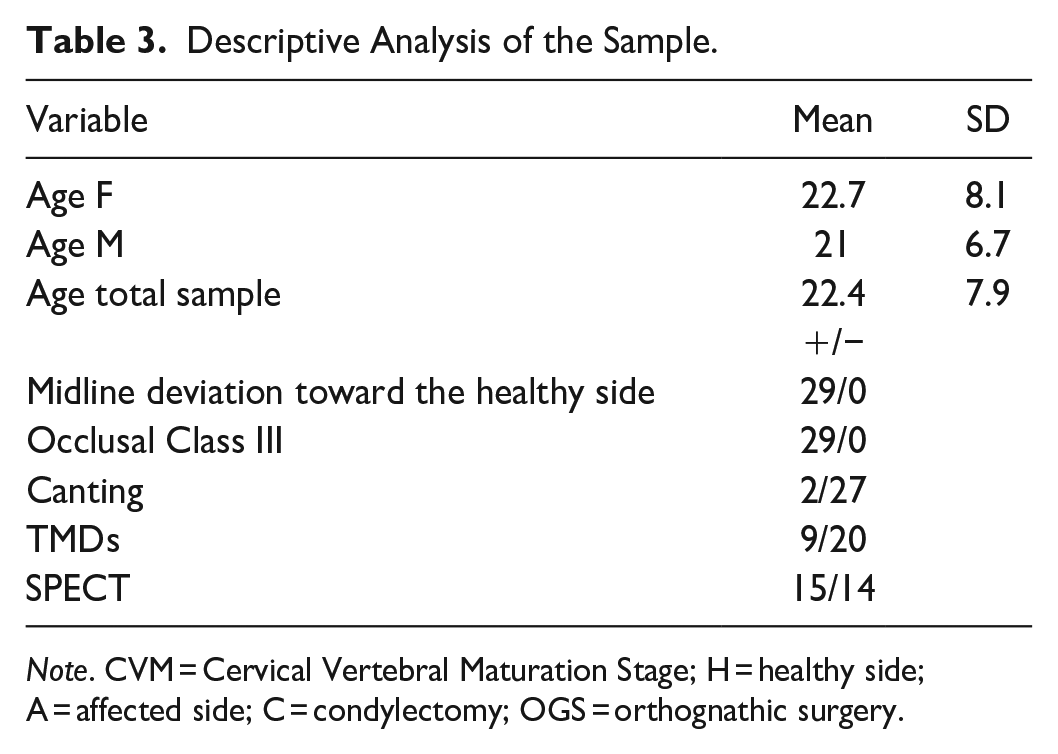
Note. CVM = Cervical Vertebral Maturation Stage; H = healthy side; A = affected side; C = condylectomy; OGS = orthognathic surgery.
All patients showed class III dental relationship on the affected side and deviation of chin and lower inter-incisor line toward the healthy side, that are the clinical features typical of the horizontal UCH. The right side was affected in 19 patients, the left side in 10. The maxillary occlusal plane was slightly canted in 2 patients: canting of the first patient was 1 mm anteriorly and 1 posteriorly, that of the second one 0 mm anteriorly and 2 mm posteriorly.
Patients affected by Temporo-Mandibular Disorders were 9 (31%): in the hyperplastic side, 5 were affected by anterior disc displacement with reduction; in the healthy side, 3 were affected by anterior disc displacement with reduction and 1 by anterior disc displacement without reduction. Joint pain was registered in all patients affected by TMDs.
SPECT was positive in 15 patients (mean age 21.8 y.o, S.D. 7.5) and negative in 14 (mean age 22.6 y.o, S.D. 7.5). According to the results of SPECT, all patients with active condylar growth were treated with TMJ surgery (condylectomy), in order to eliminate early the hyperplastic condyle, namely the primary cause of the progression of the skeletal asymmetry. Twelve out of the 15 underwent sole condylectomy, while 3 underwent one-stage condylectomy and orthognathic surgery (Le Fort I and Bilateral Sagittal Split Osteotomy).
All patients with positive SPECT underwent a Surgery First Approach: the protocol has provided the bonding of fixed appliances 2 weeks before surgery; patients were referred to the Unit of Orthodontics 2 weeks after surgery, to correct the dento-alveolar compensations and the remaining dental malocclusion, restore the physiologic activity of the Stomatognathic Apparatus, and finalize the occlusion. Two patients started fixed orthodontics 4 months after condylectomy. Class III intermaxillary elastics (3/16 in, 2 oz. in the first 2 weeks, then 4 oz.) were applied in the operated side immediately after surgery, to early recreate the functional unit between disc and operated condyle, and to counter the neuro-muscular relapse, sometimes helped by elastics on the healthy side too. As all the orthognathic cases need a functional recovery after surgery, mild mandibular gymnastics was prescribed, to improve the symmetric function of the neuro-muscular system and support elastics to recreate the functional unit condyle-disc, at least for the first 3 months. Orthodontics in this group consisted only of the post-surgical phase, with a mean duration of 19.0 months (S.D. 7.2), a minimum of 11 and a maximum of 37.
Of the 14 patients with negative SPECT, 12 followed the conventional protocol, to eliminate the dento-alveolar compensations with pre-surgical orthodontics. Orthognathic surgery was performed once the post-surgical occlusion, checked with plaster models, was considered stable. Then, post-surgical orthodontics with intermaxillary elastics finalized the occlusion. The overall mean duration in patients treated with the classic approach was 29.8 months (S.D 7.4), a minimum of 21 and a maximum of 44. 2 patients with negative SPECT followed the same protocol used in patients with positive SPECT, which consisted in TMJ surgery despite the SPECT was negative, as they were in age of skeletal growth.
At the end of the overall treatment, 3 patients out of the 29, 2 affected by anterior disc displacement with reduction in the hyperplastic side and 1 in the healthy side, continued to suffer by the TMJ disorder, while normal function was restored in the other patients.
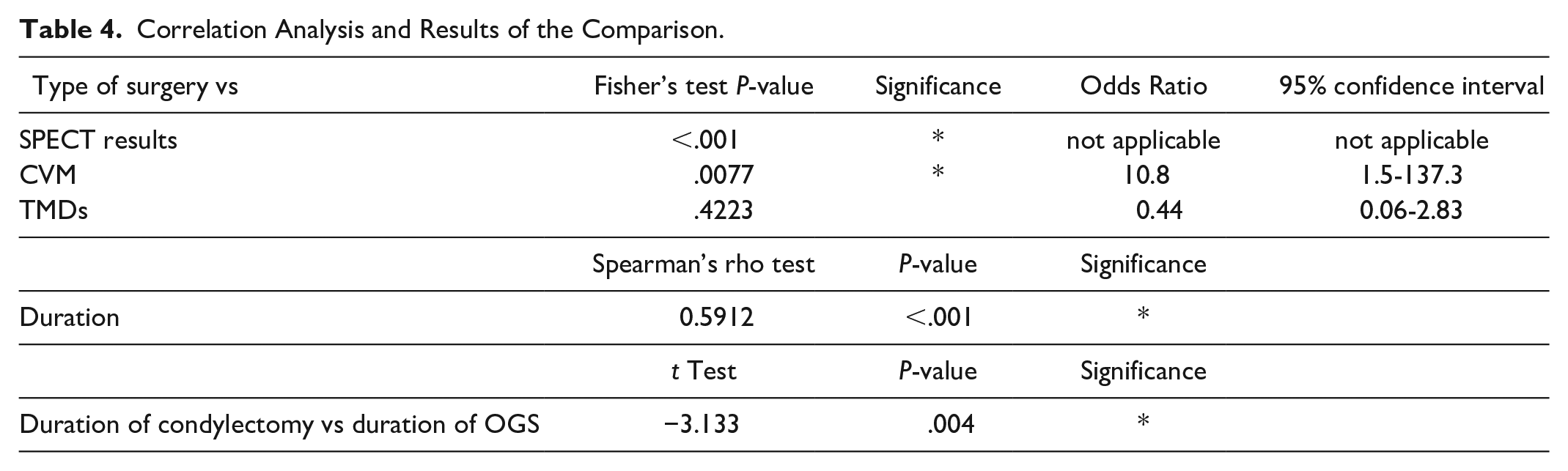
Results of the Fisher’s exact test indicate a statistically significant relationship between type of surgery performed and both SPECT results (P < .001) and stage of cervical maturation (and therefore skeletal maturation, P < .0077). The relationship between TMDs and surgery performed was not statistically significant (P = .4223). (Table 4) The Spearman’s rho test indicates statistically significant correlation between duration of orthodontics and type of surgery performed (rho = .5912, P < .001). The comparison of the mean duration of the orthodontic therapy in the condylectomy group and in the conventional orthognathic group with the Student’s t-test has evidenced a statistically significant difference (P < .001).
Correlation Analysis and Results of the Comparison.
Discussion
This study reports the experience of our Unit in diagnosis and treatment of the patients affected by the horizontal type of Unilateral Condylar Hyperplasia, and to correlate the clinical features with the orthodontic-surgical management performed.
The higher prevalence in females, also in our sample, is in line with the findings of literature. This may suggest an etiologic role of hormones, although this role is still not clear, or a stronger macro-esthetic perception of the facial asymmetry in females, that could lead to higher request of consultation.12,14,15,22,26 The mean age of the first consultation is in agreement with many studies which stated that UCH typically onsets in the second decade, when patients start to notice the asymmetric mandibular growth.7,18,22
As expected, all patients of our sample had a clinically asymmetric lower third, with chin and lower midline deviated toward the healthy side, that are the characteristic features of the horizontal type. All patients but 2 did not have an involvement of the maxillary occlusal plane, confirming that the occlusal plane is preserved in the “pure” horizontal hyperdevelopment. Therefore, the 2 patients with the slight occlusal canting should be more correctly classified as affected by the “hybrid” type, for the involvement of the occlusal plane.1,5
The ratio of patients suffering from Temporo-Mandibular Disorders agrees with the findings of Nitzan et al (38.7%) and Mouallem et al (35.6%); in our sample, TMDs occurred both on the affected and on the healthy side.1,26 The literature reports higher correlation of Temporo-Mandibular Disorders in patients affected by vertical UCH, although we would have expected higher prevalence in this pattern for the horizontal push effect of the hyperplastic condyle on the unaffected joint. 2 The TMJ surgery and symmetrization of the skeletal structure has led to better function, but more data need to be collected about how the hyperplastic TMJ affects the mandibular functions and the onset of TMJ disorders.
The therapeutic approach in our sample was highly correlated with condylar activity and skeletal maturation, while the occurrence of TMDs was not related to the type of surgery.6,27 The surgical-orthodontic approaches reported by literature include: sole orthognathic surgery; sole TMJ surgery, which could consist in high, low, or proportional condylectomy, or combination of both, in one or 2 phases.6-8,14,18-21,26,28
Early condylectomy has become the first choice for the etiological resolution of the active Condylar Hyperplasia, as it eliminates the hyperplastic growth center without waiting for the onset of dental-alveolar compensations, thus reducing the need for future orthognathic surgery, both in growing both in adult patients, at the end of growth.2,11,12,14,19 Secondary mandibular surgery may be necessary to restore the mandibular symmetry, but all patients of our sample who underwent condylectomy did not receive further surgery.11,14,22
Once the hyperplastic condyle has been removed, the post-surgical occlusion is unstable for the premature contacts on the operated side, but midlines are generally centered (Figure 3A-C). The masticatory muscles deviate the lower jaw toward the operated side and the operated condyle is repositioned upward until it reaches the maximum position allowed by the ipsilateral occlusal contacts and by the maxillo-mandibular vertical dimension of the operated side.2,19,22,27 An open bite generally occurs on the healthy side, but in the horizontal type this may not always be present: Abboud et al reported a mean post-operative open bite of 4.2 mm, a minimum of 0 and a maximum of 7 mm.2

(A-C) Immediate post-surgical occlusion after condylectomy.
After condylectomy, the functional matrices and the increased muscular strength of the masticatory muscles, shorter after surgery, and the increased masticatory load on the operated side have an intrusive action on molars, and, together with the simultaneous increase of the maxillary dento-alveolar height on the unaffected side, help the spontaneous closure of the open bite.22,26 It is unclear what is the best moment to start orthodontics. Literature has stated that orthodontic treatment accelerates the spontaneous dento-alveolar remodeling, and facilitates the achievement of a more precise intercuspation, compared to patients who did not undergo post-surgical orthodontics.2,22,26 Abboud et al delay any dental treatment that could influence the occlusion for at least 6 months, Kim et al start the orthodontic finishing 1 year after surgery.2,29 All patients of our group were treated with active orthodontics except 2 patients, who started orthodontics 4 months after surgery, because the post-surgical occlusion was clinically stable.
The main purpose of intermaxillary elastics on the operated side, generally with class III vector, is to restore the condyle-disc functional unit, while on the healthy side they extrude teeth to close the open bite; alignment, leveling of teeth over the basal bone and correction of dental compensations were the main goals to reach (Figure 4). Although the effects of the extrusion on the healthy side are probably greater than intrusive effects on the molars of the operated side, this feature is poorly analyzed in the literature. Fariña et al found an intrusion of the dento-alveolar sector on the affected side of 0.12 mm on the maxilla and 0.9 on the lower jaw, while on the healthy side they found an upper extrusion of 0.3 mm and on the lower sector of 0.6 mm, demonstrating that the effects of the orthodontic therapy are on the dento-alveolar sector both of the upper and the lower jaw. 30 Also Abboud et al reported that the maxillary occlusal plane results nearly unchanged after the orthodontic mechanics.2,19

Occlusion at the end of treatment.
Duration of the post-surgical orthodontics was highly related with the type of surgery performed; the difference of the means between the 2 groups was statistically significant. The mean duration of the group treated with condylectomy was in line with the study of Kim et al who reported a mean duration of 22.4 months. 29
The elastic-driven change of the masticatory forces, associated with the rapid change of the tone of lips, tongue e masticatory muscles and with the “Regional Acceleratory Phenomenon,” well-known to explain the efficiency of Surgery First protocols, speeds up the post-surgical orthodontic movements, even if, in this case, the site of surgery is far from occlusion. Amongst the various features that need a more thorough study in the surgical-orthodontic research of UCH, the clinical evaluation of the postoperative mandibular function (eg, Range of Motion, lateral movements) with numeric data is actually one of the less known: the correction of the mandibular asymmetry and the restore of the condyle-disc unit with condylectomy require the early restore of a symmetric function of facial muscles. The function of intermaxillary elastics on fixed appliance acting on teeth may be supported with daily exercises of light mandibular gymnastics to achieve complete rehabilitation and symmetric function. Severe pre-treatment mandibular asymmetry, or dysfunctional cases, may need postoperative manual therapy.
As a lot of time is required for the orthodontic correction of the posterior torque, the early use of rectangular archwires should be useful to address the posterior compensation with the torque correction. The important standard deviation in both groups indicate high variability in the duration of treatment, that may be related to the occlusal characteristics of the initial malocclusion and to the amount of dental compensations.
According to the functional matrices’ hypothesis, the facial asymmetry in growing patients could keep on stimulate the asymmetric growth on the 2 sides. All patients in age of growth, even those negative to SPECT, were treated with early condylectomy followed by post-surgical orthodontics, because condylectomy prevents the longer side from receiving further functional stimuli during growth that could worsen the mandibular asymmetry, even in negative SPECT patients. The early condylectomy also leads to symmetrize the rate of residual growth in the 2 halves, gradually restoring the functional balancing and the joint function as the growth continues. Occlusion too, following the skeletal rebalancing, undergoes to spontaneous remodeling. 11 This treatment should be considered as an interceptive and conservative treatment of the UCH.
Adult patients with negative SPECT were treated with conventional 2-jaws orthognathic surgery, because the condylar/hemimandibular hyperactivity has finished, therefore the skeletal and occlusal compensations should be considered stable. 18 This approach is preferred by many Authors in patients at the end of growth, because it preserves the temporo-mandibular joint and achieves favorable and stable long-term occlusion over time.2,6,7,19 Condylectomy may be useful when the difference of length of the condylar head leads to severe functional imbalances.
Pre-surgical orthodontics on the transverse plane should correct the skeletal discrepancy of the dental midlines in relation with the chin and the transverse molar discrepancy in relation with the transverse position of the gonial angles, maximizing the results of orthognathic surgery and allowing the normalization of the stomatognathic functions. 18 On the sagittal plane, the orthodontic preparation should create adequate negative overjet, to correct the lower jaw in the proper esthetical and structural position, with proclination of the lower incisors and correction of the lower incisal tip.
On the basis of findings reported in this study, we summarized the therapeutic options in a decision algorithm for treatment of horizontal UCH, based on age and condylar activity (Figure 5).
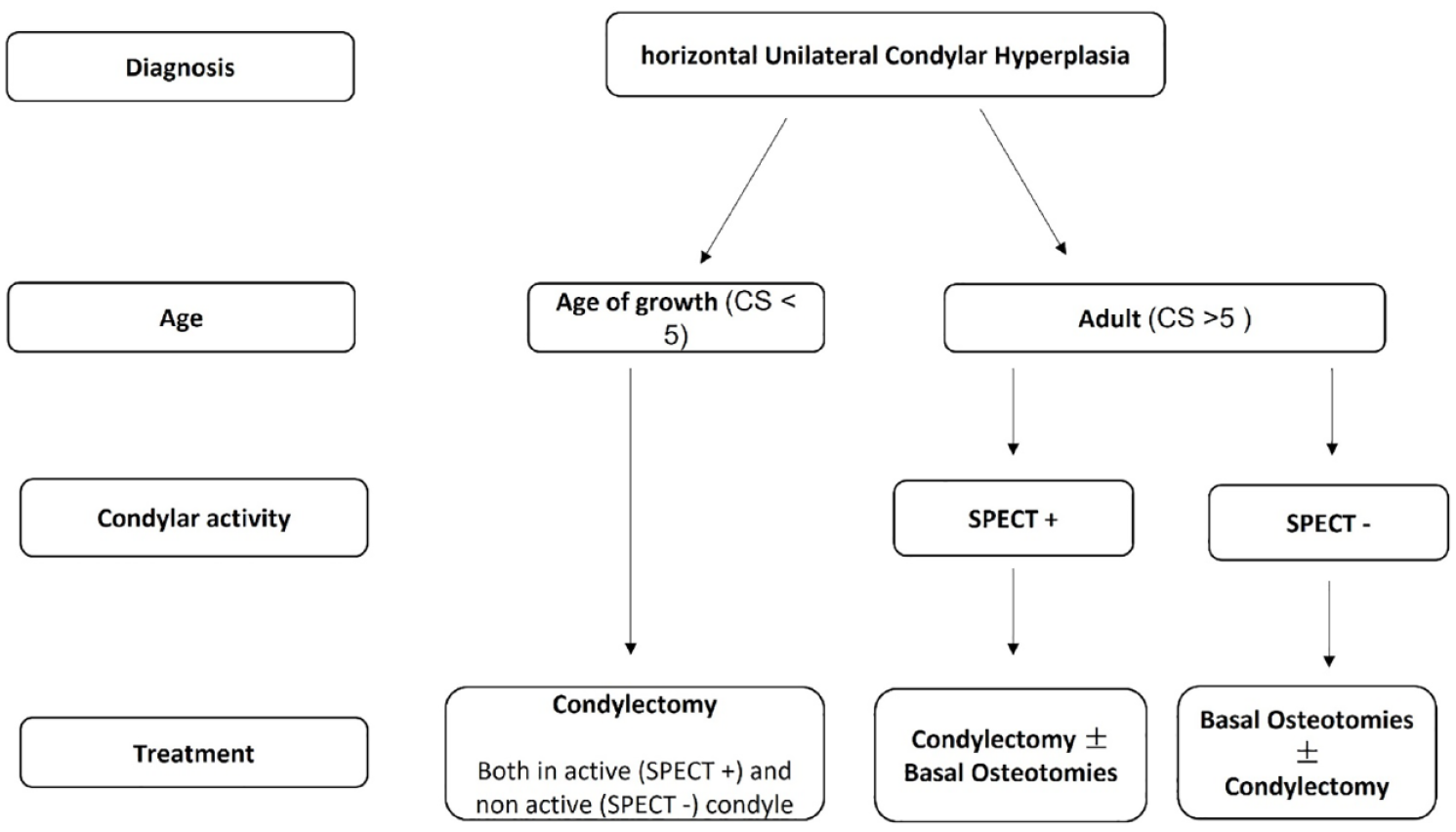
Treatment algorithm of horizontal UCH.
Despite the above said interest by the orthodontic community, this disease is not very common. So, from a methodological point of view, a study based on a cohort of patients affected requires long time to collect the data of an adequate number of patients. Another limitation to consider is the retrospective nature of this study, and the biases, depending on the several clinical pictures proper of the disease, primarily depending on the time elapsing between the onset of the disease and the first consultation.
Conclusions
The choice of the orthodontic-surgical protocol in the horizontal Condylar Hyperplasia depends on the skeletal maturation of the patient, the assessment of the condylar activity and the extent of the dental compensations.
While the pre-surgical correction of the three-dimensional dental compensations is necessary in patients with negative SPECT, patients with positive SPECT and those in age of growth, either if positive or negative SPECT, should follow TMJ surgery with a Surgery First Approach to early correct the etiological cause of the hyperplasia. Condylectomy in age of growth prevents from the progression of the malocclusion, even when condyle was not in active growth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The protocol was approved by our Department and by the local University Ethical Board, prot. n. 4632.