
Abstract
Background:
In response to the COVID-19 outbreak, the widespread imposition of social distancing and lockdown orders had an unintended secondary effect on reducing and changing the characteristics of facial injury presentations to tertiary referral hospitals. As the pandemic curve plateaued and indeed fell, these restrictions were periodically repealed, engendering an anticipated rise in the frequency facial injuries.
Objective:
The purpose of this study was to determine whether the frequency and characteristics of facial injury presentations to our tertiary referral hospital returned to pre-COVID levels following the repeal of COVID-19 social distancing and lockdown laws on the far side of the pandemic curve.
Methods:
The authors designed and implemented a retrospective study of patients who sustained a facial injury over 3 comparable 8-week periods in 2019 (pre-COVID), 2020 (COVID lockdown) and 2023 (post-repeal of COVID lockdown laws). The study was conducted in the Department of Maxillofacial Surgery at a level 1 tertiary referral regional trauma hospital in Newcastle, Australia.
Results:
The principal finding was an increase in facial injury frequency in the post-COVID cohort (n = 149), compared to the COVID lockdown (n = 37) and pre-COVID groups (n = 103). Across all 3 periods, males consistently outnumbered females, with a common peak in the 20 to 30 age group. Bony injuries predominated in all cohorts, with no difference in management approach. The leading cause of injury pre-COVID was interpersonal violence, which shifted to falls during lockdown and post-COVID. There was also an increase in workplace and animal-related injuries post-COVID.
Conclusion:
The frequency and characteristics of facial injury presentation finally stabilized and returned to pre-COVID levels following the repeal of social distancing laws. This was most notable as communities entered the far side of the pandemic curve. The findings are in keeping with a very small number of comparable studies sourced from literature.
Introduction
In response to the World Health Organisations (WHO) declaration on 11 March 2020, that the COVID-19 outbreak should be considered as a pandemic, a significant number of international governments simultaneously imposed a range of unprecedented and novel public health measures in an attempt to reduce the rate of country specific community coronavirus transmission. Such steps were characterized under the terms “social distancing” and “lockdown” legislation.1-3
Not unexpectedly, the widespread imposition of these initiatives had a profound effect on the usual manner in which public gatherings, sports, leisure activities, daily travel, and workplaces were conducted in the community. It is well known that a variety of personal behaviors and public encounters can be high risk settings for a range of accidental, non-accidental and recidivistic injuries.4,5 In this regard, there are a number of published papers that have investigated the epidemiology of facial injury.6-8
Our maxillofacial surgery department (along with some in China, Italy, and the United Kingdom) very quickly identified and reported that the imposition of COVID-19 social distancing measures, seemingly had an unintended secondary effect in reducing the frequency and changing the characteristics of facial injury presentations to tertiary referral hospitals.9-12 To a greater extent, this was subsequently confirmed by published data from a significant number of other international units.13-16 This was further upheld by the findings of a recent unpublished literature review on this topic, as undertaken by these authors. 17
In addition to the observation of a decline in the presentation of facial injury, the literature review also revealed evidence to suggest that as social distancing and lockdown laws were periodically repealed, and moreover, as the pandemic curve plateaued and indeed fell (as effective vaccinations and treatments became available on a widespread basis), the epidemiology of facial injury presentations returned to expectation. 17 It was this observation that engendered our interest and further research. In particular, there were no publications that sought to examine this effect on the far side of the pandemic.
After three years of enduring the catastrophic global effects of the SARS-COV-2 virus, a United Nations World Health Organisation (UN-WHO) press release on the 2nd May 2023 concluded that the health systems in most countries have begun to show signs of recovery. 18 Three days later, on the 5th May 2023, the Director General of the UN-WHO acknowledged that “the pandemic has been on a downward trend” and then declared (“with great hope”), an end to the COVID-19 pandemic as a public health emergency of international concern (PHEIC). 19
The purpose of this study was to determine whether the frequency and characteristics of facial injury presentations to our tertiary referral hospital returned to pre-COVID levels following the repeal of COVID-19 social distancing and lockdown laws on the far side of the pandemic curve.
The hypothesis was that there was a return to expectation, with the null hypothesis being that numbers continued to remain lower than expected, and that there was no observed difference between the 2 timeframes.
The aims of the study were to:
(I) Calculate the frequency of facial injury over a matched 8-week period (2019 pre-COVID and 2020 COVID lockdown) with the same 8-week period in 2023 (post-repeal of COVID-19 lockdown laws).
(II) Identify any variations that might exist in demographic and injury characteristics in the group.
Materials and Methods
Study Design, Sample and Setting
To address the research purpose, the authors designed and implemented a retrospective study (conducted over 3comparable 8-week periods in 2019[pre-COVID 19], 2020 [COVID lockdown] and 2023 [post-repeal of COVID-19 lockdown laws], commencing on 16th March and ending on 11th May) of the clinical records of a cohort of patients who sustained a facial injury. The study was conducted in the Department of Maxillofacial Surgery at the John Hunter Hospital, Newcastle, Australia.
The study population was derived from all maxillofacial trauma patients who attended our level 1 tertiary referral regional trauma hospital and who were assessed or managed by the Department of Maxillofacial Surgery. Exclusion criteria were imposed on patients who had insufficient clinical data.
Local health district population estimates were obtained for the study years 2019 (n = 942 374), 2020 (n = 952 381) and 2023 (n = 962 390).
Variables
The primary predictor variable was an 8-week period of COVID-19 social distancing. The primary outcome variable was the sustaining of a facial injury. Other variables that were studied included demographic (age and gender) and injury characteristics (mechanism, site, and treatment).
Data Collection
The relevant data that were required to undertake the study was retrieved from the unit logbooks and cross-checked against the hospitals digital medical record system (DMR). The relevant data were entered onto a password protected spreadsheet by a single author, which was shared in a de-identified manner between the authors.
Censorship
Censorship was within a matched 8-week study period in each of the years: 2019, 2020, and 2023.
Statistical Methods
Descriptive statistics were presented as count percentages and compared between 2019, 2020, and 2023 using the Pearson x 2 test (or Fisher’s exact test if small cell counts). The change in count of facial injuries per week over the 8-week period for 2019, 2020, and 2023 was analyzed using the Poisson regression (count outcome). Modeling included week (continuous), year, and the interaction term. Estimates presented include the estimated change per week for each year with 95% confidence interval. Statistical analyses were programed using SAS v9.4 (SAS Institute, Cary, North Carolina, USA). A priori, P < .05 (2-tailed) was used to indicate statistical significance.
Ethics
The study was designated as a retrospective continuation review of patient records and was therefore granted an exemption from review by the human ethics research committee (HREC) by the local institutional review board (IRB), authorized as negligible risk: AU202305-11. The authors adhered to the privacy and confidentiality of all clinical information in the conduct of this research as espoused by the World Medical Association’s Helsinki Declaration.
The authors have no funding, sponsorship, or conflicts of interest to declare.
Results
Frequency of Facial Injuries
Patients were recruited for the same 8-week period (March 16th to May 11th) in 2019 (pre-COVID), 2020 (COVID lockdown) and 2023 (post-COVID).
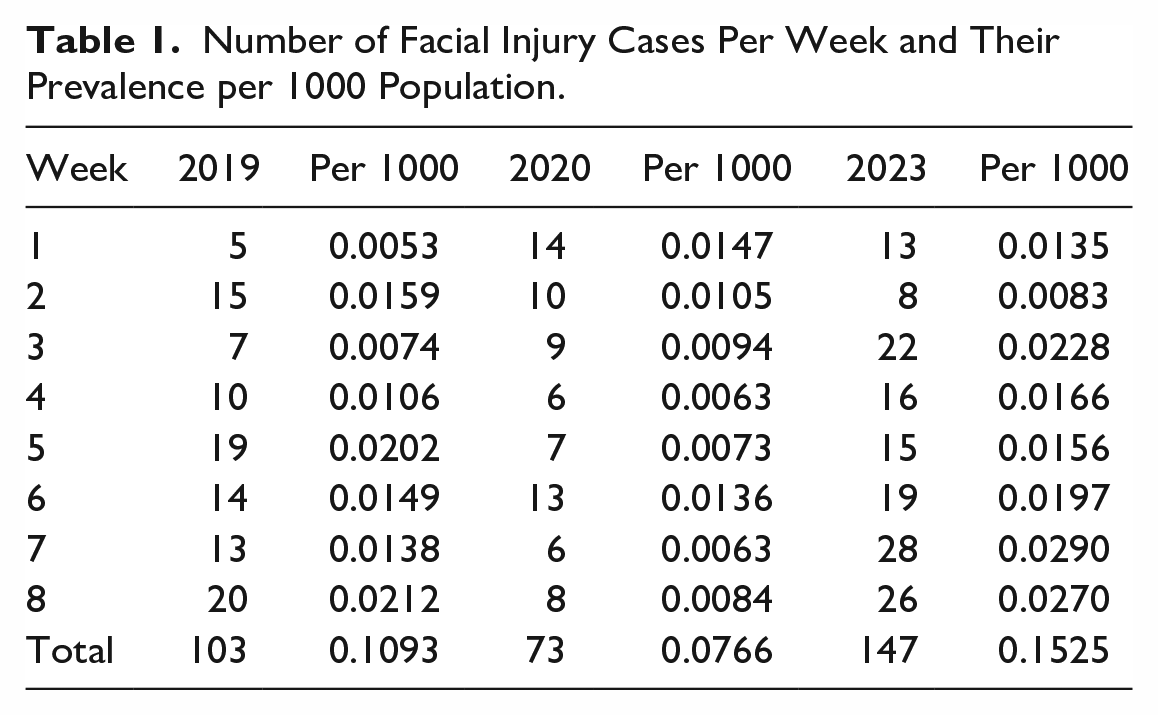
In total, 147 patients presented with facial injuries during the 2023 study period. There was a twofold increase in the incidence of injuries between the COVID lockdown and post-COVID groups, with an approximate 1.5 times increase between the pre-COVID and post-COVID cohorts.
Overall, the prevalence in the post-COVID group was highest at 0.15/1000 population, followed by 0.11 pre-COVID and 0.08 during COVID lockdown (Table 1).
Number of Facial Injury Cases Per Week and Their Prevalence per 1000 Population.
Variation in Demographics and Injury Characteristics
The demographic and injury characteristics of the 3 cohorts are reflected in Table 2.
Comparison of Demographics, Injury Type, Mechanisms, and Management Between 2019, 2020, and 2023.
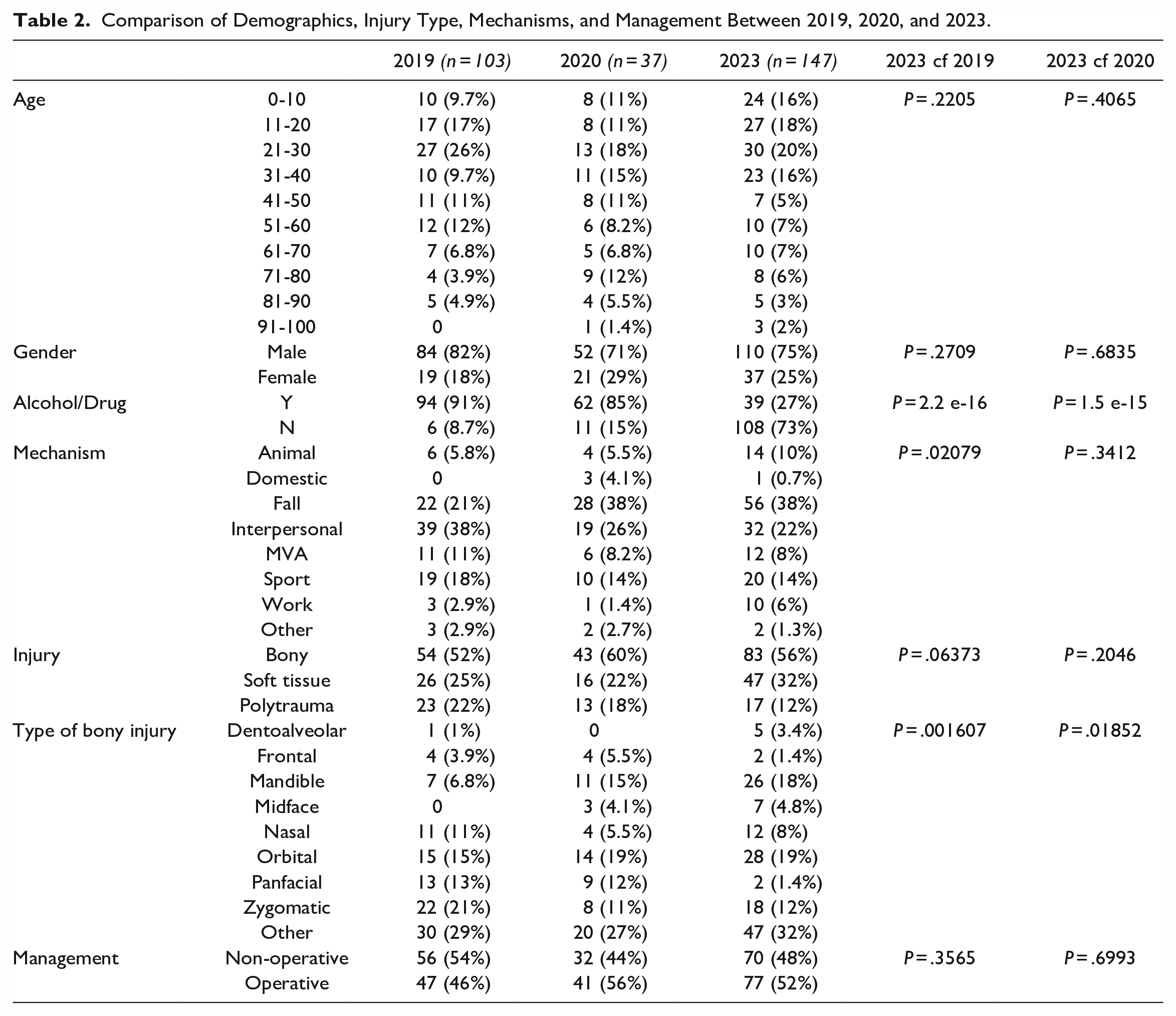
Across all 3 periods, males consistently outnumbered females and the 20 to 30 cohort was the peak age group for facial injuries, although the proportions were not statistically significant. This trend is depicted in Figure 1 which highlights the peak in frequency of that age-group.
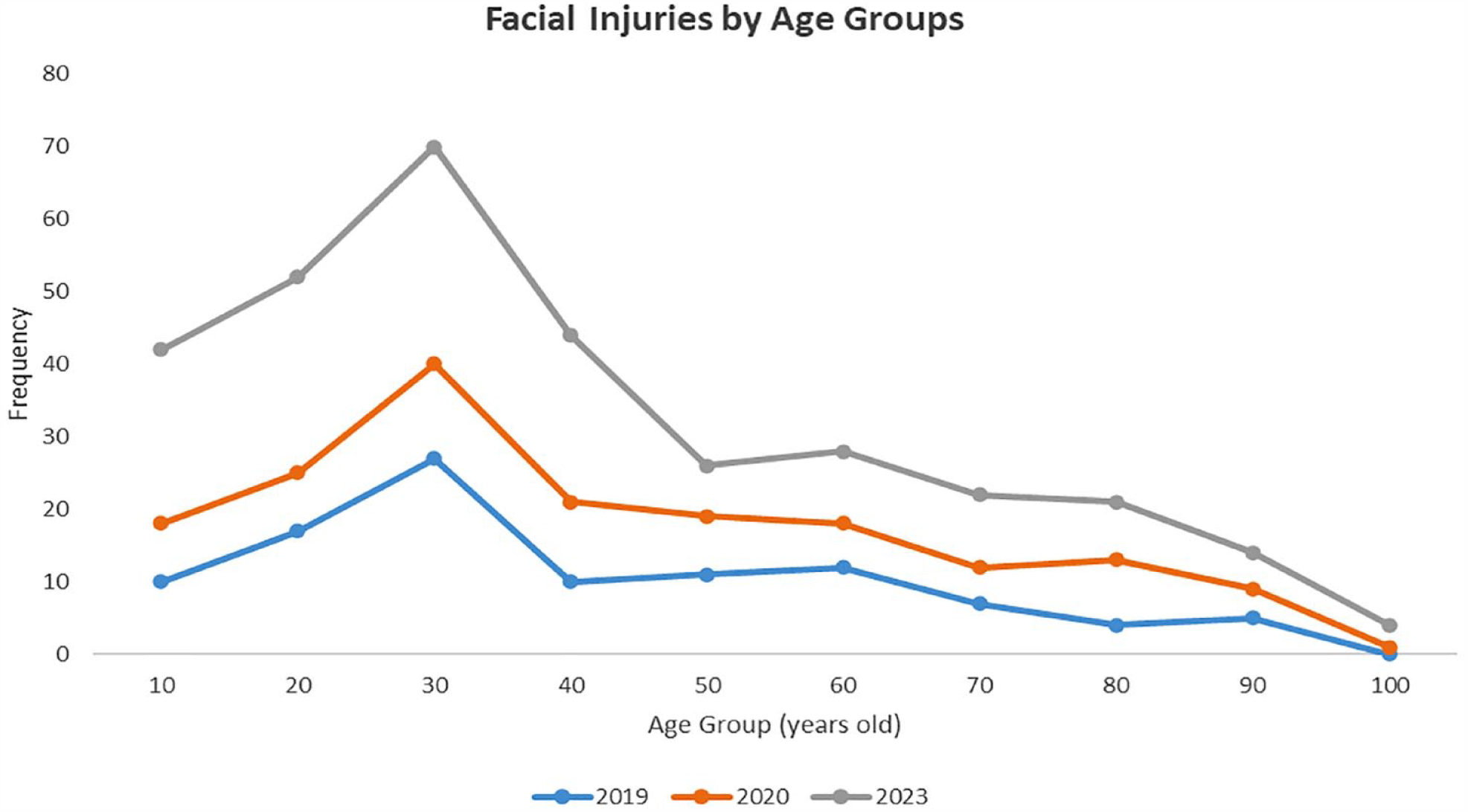
Frequency of facial injuries by age group between 2019, 2020, and 2023.
The mechanism of injury has significantly changed pre- and post-COVID with an increased proportion of workplace injuries and injuries involving animals post-COVID. Fall was the leading cause for injuries during lockdown and post-COVID whilst interpersonal violence predominated pre-COVID.
Patients presenting with facial injuries were significantly more likely to be under influence of drugs and alcohol pre-COVID and during the lockdown. The proportions were diametrically opposed post-COVID.
The majority of facial injuries were bony in all 3 periods. The type of facial fracture was quite variable, and interestingly there was a higher proportion of more severe bony fractures (ie, panfacial) during the lockdown period. The treatment of these injuries remained much the same across the cohorts.
Discussion
COVID-19 Synopsis
It is universally known that in the first quarter of 2020, the world bore witness to the outbreak of “an unprecedented,” “once in a generation” severe viral respiratory illness. This culminated in the declaration by the World Health Organization on 11 March 2020 of COVID-19 as a pandemic. The nominal virus (SARS-CoV-2) was exceptionally virulent, highly transmissible, catastrophically comorbid and contemporaneously associated with the lack of both an effective vaccine and treatment.1,2
The emerging mortality left multiple national governments with little alternative other than to rely on the imposition of a range of non-pharmacological public health isolation measures, typified by “social distancing” and “stay-at-home”/“lockdown” laws, in an attempt to curtail the community spread of the virus.3,20
These measures were variously imposed and then periodically relaxed only to be re-imposed in accordance with multiple resurgents of viral transmission due to, in particular, the progressive emergence of a number of highly virulent variant strains. As targeted vaccines and specific antiviral medications became available and were widely adopted, the so-called pandemic curves plateaued and then started to fall.3,20
At the present time, the virus is considered endemic, and remains under a “watch and wait” policy, being monitored by virologists and public health officials.18,19 As a result, “social distancing” and “lockdown” laws have, to all intents and purposes, been repealed, and we are simply living with an apparent, less virulent disease in the context of an increasing herd immunity.
Impact of COVID-19 Social Distancing/Lockdowns on the Epidemiology of Facial Injury: Lockdown and Unlock Cycles
There is a demonstrable literature that has been identified that supports the view that the implementation of COVID-19 social distancing and lockdown public health measures serendipitously altered the frequency and characteristics of facial injuries that presented to tertiary referral, speciality surgical units. In this regard, a total of 54 studies from various parts of the world have identified, on average, a 44% reduction in frequency (range: 4%-82%), which was associated with a 65% increase in falls and an 83% increase of such injuries occurring in the home. 17
There is however, little, “if any,” information available on what happened to the epidemiology of facial injury following the permanent repeal of these laws and arguably none which additionally investigated what happened as the SARS-Cov-2 virus became endemic and notably as communities reached the far side of the COVID-19 pandemic curve.
Our study assessed the status of facial injury presentation and the variation on etiology that was evident following the repeal of social distancing. We did this by comparing the same 8-week periods (16th March to 11th May) in each of the study years in 2019 (pre-COVID), 2020 (COVID lockdown) and 2023 (post repeal of social distancing laws).
We identified that in the pre-COVID 2019 period 103 patients attended our department with a facial injury which decreased to 73 patients during the COVID (2020) lockdown period. The number that was identified in the post-repeal of social distancing 2023 period was 147 patients. This was also seasonally comparable to the figures of 120 (pre-COVID 2019) and 129 (post-lockdown 2020) that were derived from a subsequent period May 12 to July 6. 21
We found that the etiology of facial injury significantly changed between the pre-COVID and COVID lockdown cohorts. The fall in interpersonal violence, sporting related injuries and motor vehicle accidents was all reasonably explained by lockdown laws and social distancing measures. During lockdown, cabin fever likely precipitated the rising trends of “DIY” home tasks which resulted in a predominance of injuries secondary to falls. As mentioned, this was consistent with the general observations seen across most studies globally.
Whilst some injury etiologies returned to the norm in the post-COVID era, there were also some distinct differences. Compared to the pre-covid cohort, there was essentially an equal number of cases due to interpersonal violence, sports, and motor vehicle accidents. However, falls continued to persist as the leading cause of injury and we saw a rise in animal and work-related injuries. This is likely a comment on the greater societal impact that COVID-19 espoused, which includes the rise in “pandemic pets” for psychological support and the new employment paradigm of working from home. 22
We have only been able to identify 4 studies in the literature that have similarly considered the basis of our study. However, the most important distinction is that our study has been conducted in a period where not only lockdown or social distancing laws were repealed but there were global signs of recovery from coronavirus and de-escalation of its status as a pandemic. As such, this paper provides unique insight into epidemiological trends in the immediate recovery/post-pandemic phase, that will be more applicable to support policy making in the event of another global health crisis.
Boom et al evaluated the impact that COVID-19 lockdown had on the incidence, type and mechanism of facial injury. 23 They compared 3 phases: pre-COVID (2018 and 2019), intra-COVID (2020) and post-COVID (2021) over the same 15-week periods. They identified a statistically significant (P = .007) 49% decline (naverage = 38.5 to n = 19) in the presentation of facial injury in the 2020 lockdown. This increased (from n = 19 to n = 34) in the post-lockdown period (78.95%) and with n = 34 being comparable to the pre-COVID figure, n = 38.5. They also observed statistically significant changes in the various etiologies of facial injury over the duration of their study.
A similar study was conducted by Shenoi et al who investigated pre (Group A)—intra (Group B)—post (Group C) COVID “lockdown effects” in relation to the presentation of facial injury. 24 Mathematically considering their results, Group A -pre COVID- identified 217 cases over 166 days (1.3/day), Group B—COVID lockdown—identified 30 cases over 70 days (0.39/day) and Group C—COVID-unlock—identified 95 cases over 92 days (1.03/day).
As a proportion, Road Traffic accidents in Group A comprised 72.5%, decreased in Group B to 47.37% and returned to approach mean normal levels at 63.83% in Group C. Falls increased from 22.5% to 31.58% and then returned to near expected at 26.6%. Assaults comprised 2.5% of their cohort, increased to 15.79% and then fell to 6.38%.
A third study that we identified was undertaken by Press. 25 He investigated similar trends over a comparable time in 2020 (COVID: n = 212) compared to 2019 (pre-COVID: n = 203). Two individual time frames from the respective years were selected: March 1 (2019 and 2020) to May 31 (2019 and 2020) and June 1 (2019 and 2020) to August 31 (2019 and 2020). These were consistent with (initial) “lockdown phase” and (re-opening) “unlock phase” periods. “Lockdowns” figures decreased by 24.5% (n = 106 to n = 80) and following “unlock,” rebounded by 36.1% (n = 97 to n = 102). In particular, instances of interpersonal violence decreased by 52.4% in lockdown and rose by 30% in unlock.
The last of the 4 studies was undertaken by Qiu and Hoffman. 21 They investigated 2020 lockdown / post-lockdown periods. The 8-week figure for 2019 (control) was n = 103, which reduced to n = 73 (30% reduction) for the 2020 lockdown and then rose to n = 120 (64% increase) in the post lockdown period.
Strengths and Weaknesses
In principle, our study was a single center retrospective cohort study undertaken by one specialist surgical discipline and which captured a significant proportion of facially injured patients who presented to a tertiary referral hospital. The study is subject to various limitations that are inherent in such investigations. In saying that, we attempted to account for any seasonal variability in trauma presentations by undertaking the investigation in comparable time periods. In the main, we endeavored to capture all trauma that was referred to, assessed, and managed by our department. This included both non-operative and operative cases, and the latter both under local anesthesia or general anesthesia. Unfortunately, some nasal fractures and some lacerations may have been respectively logged under Ear, Nose, Throat and Emergency Departments and therefore not included in our figures.
Conclusion
In conclusion, our study demonstrated that, following the initial imposition of COVID-19 lockdown laws in March 2020, and variably continued thereafter over 2 to 2.5 years, the frequency and characteristics of facial injury presentation finally stabilized and returned to pre-COVID levels following the repeal of social distancing laws. This was most notable as communities entered the far side of the pandemic curve. The findings are in keeping with a very small number of comparable studies sourced from literature.
The study upholds our contention that COVID-19 pandemic social distancing / lockdown laws provided a unique opportunity to witness the effect that the initial imposition and subsequent repeal of these aggressive public health isolation measures had in changing the epidemiology of facial injury presentation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study was designated as a retrospective continuation review of patient records and was therefore granted an exemption from review by the Human Ethics Research Committee (HREC) by the Local Institutional Review Board (IRB), authorized as negligible risk: AU202305-11. The authors adhered to the privacy and confidentiality of all clinical information in the conduct of this research as espoused by the World Medical Association’s Helsinki Declaration.