
Abstract
Many people worldwide want to be less neurotic. As lower levels of neuroticism predict a variety of positive life outcomes, including health, success, and relationship quality, interventions that help people to become less neurotic could have wide-ranging impacts. This study protocol describes the rationale and design of the CHILL (
Neuroticism describes the tendency to frequently experience negative affect, show strong emotional reactions to stress, and perceive the world as a threatening place while doubting one’s ability to deal with such threats (Barlow et al., 2014; Goldberg, 1990; Soto & John, 2017). Neuroticism predicts a range of detrimental life outcomes (Beck & Jackson, 2022; Soto, 2019; Wright & Jackson, 2023). It has been associated with the onset of mental disorders and physical health problems, the occurrence of major life stressors such as divorce or job loss, and increased risks for long-term disability and mortality (Barlow et al., 2014; Goldstein et al., 2020; Jokela et al., 2013; Lahey, 2009; Roberts et al., 2007). Altogether, the costs associated with neuroticism exceed those of common mental disorders (Cuijpers et al., 2010). Measures that can effectively reduce neuroticism may thus offer promising ways to promote health and well-being in the general public.
With evidence that many people want to become less neurotic and are willing to invest time and money to do so (Baranski et al., 2021; Hennecke et al., 2014; Miller et al., 2019), the question of whether trait levels of neuroticism can be changed volitionally has recently gained increased attention (Bleidorn et al., 2019; Hudson & Fraley, 2015; Stieger et al., 2021). Volitional personality trait change describes self-directed personality changes in desired directions, for example, through targeted interventions (Hudson, 2022; Hudson et al., 2019; Stieger et al., 2018). Although there is initial evidence that such interventions can successfully promote desired personality changes (Haehner, Wright, et al., 2024; Roberts et al., 2017; Stieger et al., 2021), it is still unclear (1) which intervention strategies are successful in changing neuroticism, (2) whether intervention-induced neuroticism changes generalize beyond self-reports, (3) when interventions should be delivered to be most efficient, and (4) which contextual or personal characteristics moderate intervention efficacy. A thorough investigation of volitional neuroticism change is thus needed to fully realize its potential. This study protocol describes the rationale and design of the Changing How I Live Life (CHILL) Study, a smartphone-based intervention designed to reduce neuroticism in the general public.
Neuroticism as an intervention target
Neuroticism is a risk factor for many mental disorders – particularly those related to depression and anxiety – and accounts for much of the genetic vulnerability underlying these disorders (Clark & Watson, 1991; Griffith et al., 2010; Khan et al., 2005; Weinstock & Whisman, 2006). Public health experts have thus called to shift from interventions that focus on specific types of mental disorders to interventions that focus on neuroticism as the root of these problems (Barlow et al., 2014; Cuijpers et al., 2010; Widiger & Oltmanns, 2017). This suggestion is supported by recent evidence suggesting that both the levels of neuroticism and changes in neuroticism can predict important life outcomes. For example, decreases in neuroticism have been found to predict a better health status and reduced mortality risk several years later (Human et al., 2013; Mroczek & Spiro, 2007; Wright & Jackson, 2023). Together, these findings make neuroticism a prime candidate for interventions designed to improve public health and well-being (Bleidorn et al., 2019).
However, changing a personality trait like neuroticism is challenging. Contemporary theories of personality development attempt to explain why personality traits remain relatively stable over time and which conditions may lead to lasting personality trait change (Bleidorn, 2024). For example, the TESSERA Framework (Wrzus & Roberts, 2017) suggests that personality traits only change if people experience lasting shifts in the dynamic interplay of experienced situations, expectations, personality state expressions, and reactions. Thus, this model predicts that personality traits do not change if one of these elements does not change or if shifts in these dynamics are not lasting. Similarly, Whole Trait Theory (Fleeson & Jayawickreme, 2015) posits that lasting personality trait changes only occur if the explanatory mechanisms that generate personality state expressions in daily life are changed. Mechanisms like interpretation of situations, homeostatic forces, or activation of goals typically result in relatively stable distributions of personality states. Finally, the Theory of Self-Regulated Personality Change (Hennecke et al., 2014) outlines three preconditions of successful personality change. The first precondition is that people want to change their personality traits or trait-related behavior, such as being more relaxed in stressful situations. The second precondition is that people consider personality change feasible and believe that they are able to change their personality in the desired way. Then, the third precondition is that people have the capacity to show enduring changes in trait-relevant behaviors (e.g., react more relaxed in stressful situations, show efficient coping strategies) so that these behavioral changes become habitual and extend across situations and life domains.
In sum, these theoretical perspectives may explain why neuroticism remains relatively stable within individuals and the population (Bleidorn et al., 2022), despite many people wishing to become less neurotic (Baranski et al., 2021; Hudson & Fraley, 2016). Merely desiring to become less neurotic thus does not seem sufficient to promote lasting changes; rather, effective interventions may be needed to change neuroticism in the general public.
Interventions to decreases in neuroticism in the general public
To date, the best evidence that neuroticism can be changed through intervention comes from clinical studies. In a meta-analysis, Roberts et al. (2017) found that psychotherapeutic interventions can lead to lasting decreases in neuroticism (−0.57 ≤ d ≤ −0.39), illustrating that intervention-induced neuroticism change is possible in clinical populations. However, this line of research provided no evidence on how neuroticism can be changed and whether change is possible with less resource intensive interventions that can be offered to the general public.
Initial insights into these questions have been provided by volitional personality change research that examined how personality traits can be changed in nonclinical populations (Haehner, Wright et al., 2024; Hudson, 2021b). In one of the key studies on this topic (Stieger et al., 2021), participants chose how they wanted to change their personality, with one option being to decrease in neuroticism. Over 10 weeks, participants then used a smartphone app with more than 10 different intervention strategies such as resource identification, goal setting, and motivated reflection (Allemand & Flückiger, 2017). The authors found that the smartphone intervention led to a lasting decrease in participants’ neuroticism levels (d = −0.54) that also generalized to other outcomes such as well-being (Allemand et al., 2024; Olaru et al., 2023; Stieger et al., 2023). Similarly promising results were also found in a study with a personalized coaching intervention (Allan et al., 2018; Martin et al., 2014) and in a study that examined how completing behavioral challenges fosters neuroticism change (Hudson et al., 2019).
However, this initial evidence requires replication and extension as several open questions about intervention-induced neuroticism change remain unanswered: (1) What are the key components of effective neuroticism interventions? (2) Why do people differ in how they respond to interventions? (3) How can the efficacy of neuroticism interventions be optimized for the general public? (4) Under which conditions are neuroticism interventions most effective? To address these questions, novel empirical approaches are needed that move beyond one-size-fits-all approaches and that allow researchers to identify which intervention strategies are most successful in reducing neuroticism (Wright et al., 2024).
An empirically derived taxonomy of intervention strategies to reduce neuroticism
There currently exists little consensus about the most effective strategies to reduce neuroticism – possibly because a common terminology for describing and classifying neuroticism interventions is lacking (Wright et al., 2024). For example, the most common description of psychotherapeutic interventions to reduce neuroticism in the meta-analysis by Roberts et al. (2017) was “mixed” – providing little information on specific strategies to successfully change neuroticism. Similarly, existing research on volitional personality change differs significantly in its approaches (Haehner, Wright et al., 2024), precluding a systematic investigation and knowledge accumulation of the efficacy of different intervention strategies.
To overcome these limitations, Wright et al. (2024) recently proposed an empirically derived taxonomy of neuroticism interventions for the general public. In line with theoretical conceptualizations of personality traits (Allemand & Flückiger, 2017; Geukes et al., 2018; Hennecke et al., 2014; Jackson & Wright, 2024; Wilt & Revelle, 2015; Wrzus & Roberts, 2017), this taxonomy distinguishes relevant intervention strategies based on the levels and aspects of intervention targets. The level of intervention targets describes whether a strategy intervenes at the state, habit, or trait level of neuroticism. State-level interventions (e.g., relaxation) address momentary manifestations of neuroticism such as instances of stress, negative affect, or worrying. Habit-level interventions (e.g., cognitive restructuring) target domain-specific pairings of thoughts, feelings and behaviors, whereas trait-level interventions directly address stable, dispositional patterns of thoughts, feelings, and behaviors that generalize across situations (Allemand & Flückiger, 2017; Fleeson & Jayawickreme, 2015; Wrzus & Roberts, 2017). The aspect of intervention targets refers to whether an intervention strategy focuses on affective, behavioral, and/or cognitive aspects of personality (Wilt & Revelle, 2015). As personality traits like neuroticism are multifaceted constructs, each level of neuroticism is comprised of representative affective aspects (e.g., negative affect), behaviors (e.g., isolating from others), and cognitive aspects (e.g., worrying). Thus, intervention strategies can focus on different aspects of neuroticism.
Overview of neuroticism intervention strategies.

Note. Table adapted from Wright et al. (2024). The intervention strategies Exposure and Implicit Bias Modification are not implemented in the CHILL Study because they could not be readily implemented in a digital smartphone app. More details on the different intervention strategies and their relation to contemporary theories of personality change can be found in Wright et al. (2024).
Overall, this taxonomy of neuroticism interventions provides a systematic overview of existing intervention approaches and offers a terminology for describing and classifying relevant intervention strategies. Applying this taxonomy to practice may thus help to identify which ways of targeting neuroticism are most successful. Therefore, the implementation of intervention strategies in the CHILL Study was based on this taxonomy to allow for a closer examination of successful intervention approaches to change neuroticism. However, the efficacy of intervention strategies may vary within and between participants (Hudson, 2021b; Klasnja et al., 2015). To be able to examine such effects, another critical feature of the CHILL Study was the implementation of intervention strategies by means of a smartphone app.
Using digital interventions to promote decreases in neuroticism
Existing research on intervention-induced neuroticism change shows that effects differ across studies and participants (Haehner et al., 2024; Hudson, 2021a; Hudson et al., 2019; Stieger et al., 2021). Understanding when and why the effects of neuroticism interventions differ across people may be critical for maximizing their efficacy. One way to test these questions is using digital interventions that allow researchers to move beyond one-size-fits-all approaches and provide scalable solutions to individually tailor interventions.
Three features move digital interventions beyond traditional treatment approaches. First, the highly standardized nature of digital interventions allows for the manipulation of individual intervention aspects while controlling for others, providing researchers with an experimental paradigm to identify relevant characteristics of successful neuroticism change (Klasnja et al., 2015). Second, advances in internet and smartphone technology have made it possible to capture intensive longitudinal data on psychological change processes with limited expense for researchers or burden for participants (Moshe et al., 2021). This allows researchers to obtain large sample sizes to conduct sufficiently powered trials and ultimately make interventions available to the general population (Stieger et al., 2021). Third, the ability to adapt the timing and amount of interaction with specific intervention strategies enables the development of personalized intervention approaches, potentially boosting their efficacy (Montag et al., 2020; Nahum-Shani et al., 2015).
The CHILL Study
This protocol describes the rationale and design of the CHILL Study, which aims to test the efficacy of a digital intervention to change neuroticism in the general public. Our intervention is guided by the taxonomy of intervention strategies by Wright et al. (2024). Based on this taxonomy, we plan to create four core treatment groups (TGs) that receive different intervention strategies. Specifically, TG 1 receives trait-level interventions (e.g., psychoeducation); TG 2 receives trait- and habit-level interventions (e.g., psychoeducation and goal setting), TG 3 receives trait-level and state-level interventions (e.g., psychoeducation and physical activity), and TG 4 receives trait-, habit-, and state-level intervention (e.g., psychoeducation, goal setting, and physical activity). With the CHILL Study, we aim to address three broad research questions: Does the intervention lead to a decrease in neuroticism across TGs? Does the efficacy of intervention strategies vary across TGs? Do the effects of the intervention generalize to other life outcomes and peer-reports of neuroticism?
Methods
Transparency and openness
Data collection for the CHILL Study starts in June 2024 and is expected to be completed in December 2024. The design of the CHILL Study was preregistered at https://osf.io/mc7v3/?view_only=27cf0b64a71d4445945f6885818c8069. Data collection of the CHILL Study has been approved by local ethics committee of University of Zurich [Number 23.08.20]. After completing the data collection, we will publish an anonymized dataset on OSF. Hypotheses and specific analysis plans will be preregistered separately for subprojects that will rely on data from the CHILL Study.
Design and procedure
The design of the CHILL Study is illustrated in Figure 1. Participants will first complete a screening that includes information about the study and questions about five inclusion criteria. Specifically, participants are required to (1) speak German, (2) be between 18 and 40 years old, (3) have a smartphone with internet access, (4) be willing to download the intervention app, and (5) desire to become less neurotic. Only people fulfilling these inclusion criteria are invited to take part in the study. Furthermore, participants are asked to invite up to three peers to support their participation in the study. To do so, participants receive unique identification numbers and registration links to send to their peers. Overview of the CHILL Study design. Participants first complete a screening to determine their eligibility to take part in the study. For eligible participants, the CHILL Study comprises four survey assessments (T0 to T3), a pre-intervention experience sampling phase, an intervention phase, and a post-intervention experience sampling phase. T0 to T3 survey assessments are conducted in formR, while all other assessments are implemented in m-Path. The intensive data collections in m-Path comprise weekly surveys, daily-diary questionnaires every evening, and experience sampling surveys three times per day. For the intervention phase, participants are randomized to four core treatment groups (TGs) that receive different intervention strategies. Furthermore, participants invite up to three peers to provide peer-reports of participants’ personality traits in four survey assessments. W = weekly assessment; D = daily assessment; ESM = experience sampling assessment.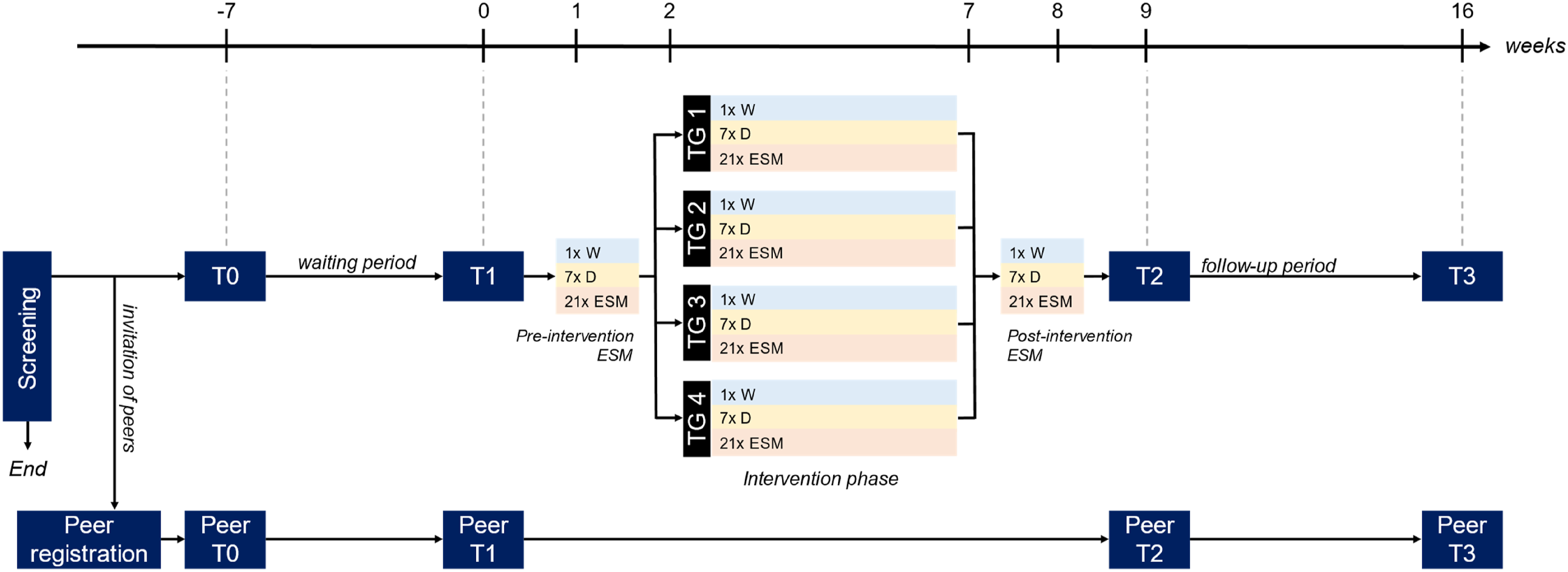
Procedure for target participants
The CHILL Study comprises four survey assessments conducted in formR (Arslan et al., 2020) and an intervention phase implemented in m-Path (Mestdagh et al., 2023). Participants are invited to the trait assessments (T0 to T3) via email and receive up to two reminders to participate in each trait assessment. At T0, participants provide informed consent and rate their neuroticism using the BFI-2 (Danner et al., 2020). After completing T0, there is a waiting period of 2–7 weeks, depending on participants’ registration dates. During this period, tutorials on how to download and set up the intervention app as well as virtual information sessions with the research team are provided to participants. The waiting period is included to compare the extent of normatively occurring changes with intervention-induced changes. After the waiting period, participants are invited to T1, which has assessments of various trait characteristics, including personality traits, self-esteem, life satisfaction, emotion regulation strategies, affect, personality change goals, and demographic information (see Measures section for details).
After T1, participants receive an individualized invitation to the smartphone intervention app m-Path. On the Monday after registering in m-Path, participants complete a 1-week baseline phase of experience sampling method (ESM) surveys. On each day, participants complete three ESM assessments and one end-of-day diary assessment, consisting of questions about their personality, environment, and experiences of stress and negative affect. Furthermore, for the next 8 weeks, participants receive a weekly questionnaire that, among other things, assesses change goals and perceived personality changes.
Overview of treatment groups.

Note. This table summarizes the allocation and dosage of intervention strategies across treatment groups (TG). Trait-level interventions are continuously presented in the CHILL Area. TG 2 is split into TG 2a and TG 2b to distinguish cognitive and behavioral intervention strategies. TG 4 is split into TG 4a and TG 4b to distinguish between state-level intervention strategies that require participants to perform purely behavioral activities (e.g., Behavioral Activation) and strategies that also target cognitive and/or affective aspects (e.g., Mindfulness and Meditation Training).
aAlthough this strategy primarily targets neuroticism at the habit level, it is accessible continuously for all TGs to fulfill ethical requirements.
Then, 8 weeks after the T1 assessment, all participants are invited to the post-intervention survey assessment (T2) that contains the same measures as the pre-intervention assessments. Another 7 weeks later – approximately 15 weeks after T1 – participants receive an invitation for the fourth and final survey assessment (T3), which serves as a follow-up to examine the longevity of the intervention effects.
Procedure for peers
Peers who are nominated by the target participants enter the study via links provided to the target participants. As a first step, peers complete a brief registration which includes information on the study design and determination of eligibility: (1) German-speaking, (2) age of at least 18 years, and (3) not a target participant in the CHILL Study. Eligible peers are invited to the four survey assessments of the CHILL Study that take place in parallel to the trait assessments of the targets. These peer assessments include questions about their relationship to the target as well as peer-reports of targets’ personality traits and perceived personality changes.
Participants and recruitment
We intend to recruit German-speaking adults between the ages of 18 and 40 who are willing to take part in a digital intervention study and who are motivated to decrease their neuroticism. We selected the age range of 18–40 years because personality traits are generally believed to be more malleable in early adulthood than they are during other developmental periods like middle adulthood (Bleidorn et al., 2022; Schwaba & Bleidorn, 2018). Furthermore, in line with theoretical and ethical considerations on volitional personality change, we restrict our sample to people who are motivated to decrease their neuroticism (Hennecke et al., 2014).
Participants will be recruited using convenience sampling methods, including social media platforms, newspapers, mailing lists, flyers, and websites. Participants can receive up to CHF 200 for participation in the study, with compensation being contingent upon completion of different questionnaires across the study period. Participants will also receive a personalized personality feedback report after the study is completed. Finally, peers will be entered into a raffle for 10 vouchers for Galaxus or Amazon worth CHF 50 each.
We aim for a final sample size of N = 390 participants. With this sample size, we will have 80% power at α = .05 to detect an effect of TG assignment on changes in neuroticism across the study period equal to d = 0.44 (f = .222, η2 = .047) in line with effect size estimates in existing research on volitional change in neuroticism (Haehner, Wright et al., 2024; Roberts et al., 2017; Stieger et al., 2021).
Measures
Survey assessments and peer-reports (T0 to T3)
Overview of constructs assessed at the trait assessments T0 to T3 (self-report).

Note. Unless not otherwise indicated, constructs are assessed on a 5-point scale.
Overview of constructs assessed at the trait assessments T0 to T3 (peer-report).

ESM assessments, daily-diary assessments, and weekly assessments
Overview of constructs assessed at the ESM, daily diary, and weekly assessments.

Note. Unless not otherwise indicated, constructs of the weekly assessment are assessed on a 5-point scale.
Mobile sensing
In addition to the questionnaires, participants are given the opportunity to activate mobile sensing. If the necessary permissions are provided, data are collected directly after participants complete interactions in the m-Path app (i.e., no continuous assessment). The types of data collected are: GPS location, app usage, step count, noise level, and nearby Bluetooth devices. Participants can agree to the collection of all types, some types, or no mobile sensing data at all.
Intervention phase and treatment groups
At the beginning of the intervention phase, participants download the CHILL Area applet in m-Path – an app within the m-Path app. This applet accompanies participants’ navigation through the intervention phase (see Figure 2), with some intervention strategies, such as Psychoeducation or Structural Support, being continuously available in the CHILL Area. However, most intervention strategies are prompted at specific times throughout the day, with different intervention strategies being implemented across the four core treatment groups (TGs 1 to 4; see Table 2). This randomization of intervention strategies across TGs allows us to investigate which intervention strategies are most effective in changing neuroticism. TG 1 only receives trait-level interventions that are continuously accessible in the CHILL Area, such as Psychoeducation and Information Feedback. This group may thus be seen as an active control group that allows to evaluate how minimal intervention efforts are related to personality changes. TG 2 receives trait-level and habit-level interventions. TG 2 is further split into two subgroups (TG 2a and TG 2b) to distinguish cognitive and behavioral intervention strategies. Comparing these two subgroups allows researchers to evaluate whether behavioral or cognitive strategies are more effective in changing neuroticism. TG 3 receives trait-level and state-level interventions. Finally, TG 4 receives intervention strategies that target all levels of neuroticism. TG 4 is again split into two subgroups (TG 4a and TG 4b) to distinguish between state-level intervention strategies that require participants to perform purely behavioral activities (e.g., Behavioral Activation) and strategies that also target cognitive and/or affective aspects (e.g., Mindfulness and Meditation Training). Illustration of the CHILL Area applet in m-Path. At the beginning of the intervention phase, participants download the CHILL Area applet as their intervention companion. The CHILL Area includes, for example, psychoeducational content on neuroticism and personality development.
Intervention strategies
In total, 17 different intervention strategies are examined in the CHILL Study. In the following sections, we describe the implementation of each intervention strategy in more detail. Further details on the taxonomy of intervention strategies can be retrieved from https://personalitychange.shinyapps.io/NeurTaxonomyShinyApp/.
Trait-level interventions and continuously presented strategies
Information feedback
Information Feedback is an intervention strategy that primarily addresses cognitive aspects of neuroticism. This strategy is continuously presented to participants with the goal of increasing their intervention adherence (e.g., Biesen et al., 2024). For example, after completing a questionnaire, participants receive a message stating the amount of compensation they have earned so far. In addition, participants can see a progress bar on their app homepage, allowing them to track how many questionnaires and tasks they have completed and how many remain for each day.
Psychoeducation
Psychoeducation (Walsh, 2009) is an intervention strategy that primarily addresses cognitive aspects of neuroticism. Information on the definition of personality, the costs of neuroticism, and personality development are sent out as notifications during the first intervention week and subsequently provided in the CHILL Area (based, for example, on Bleidorn et al., 2022).
Structural or practical support
Structural or Practical Support is an intervention strategy that addresses cognitive and behavioral aspects of neuroticism. Information on mental health services and counselling are continuously accessible in the CHILL Area.
Habit-level interventions
Habit-level interventions strategies are provided to TGs 2 and 4. These intervention strategies are presented twice per week.
Cognitive restructuring
Cognitive Restructuring (Clark, 2013) is an intervention strategy that primarily addresses cognitive aspects of neuroticism. When receiving this strategy, participants are provided with information on cognitive biases and asked to describe one negative thought that they would like to change. Then, they are guided to reflect on how cognitive biases may have influenced this thought and prompted to develop a more adaptive alternative.
Goal setting
Goal Setting is an intervention strategy that primarily addresses cognitive aspects of neuroticism. Participants receive instructions on how to formulate specific, concrete, and realistic goals to become less neurotic (e.g., Hudson & Fraley, 2015). They are then guided to develop one “if-then” plan for the following days (e.g., “When I come back from work, I will put on my running shoes and go for a 20 min run”).
Motivated reflection
Motivated Reflection is an intervention strategy that primarily addresses cognitive aspects of neuroticism (e.g., Stieger et al., 2021). When receiving this strategy, participants are guided to reflect on their experiences of the day, week, or on how they have changed since starting the study (e.g., “How have you changed since you started the CHILL Study? Write down the areas in which you have or have not noticed a change. How does this make you feel?”).
Positive reinforcement
Positive Reinforcement is an intervention strategy that primarily addresses behavioral aspects of neuroticism. This strategy is incorporated as a companion strategy to the other intervention strategies (e.g., Yeo et al., 2016). After completing a task, participants receive encouraging messages (e.g., “Great! Every step outside your comfort zone is a great success!”).
Resource identification
Resource Identification (Wilson, 2017) is an intervention strategy that primarily addresses cognitive aspects of neuroticism. When receiving this strategy, participants are guided to reflect on their resources in different life domains (e.g., “Think about and research what resources are available in your environment. For example, find out what psychological support services are available in your area or online. You can also look for group meetings on topics that concern you. After you have looked at your collected resources again, we would like to ask you to briefly consider which of them you can use at the moment”).
Skill building via modeling
Skill Building via Modeling (Ladd & Mize, 1983) is an intervention strategy that addresses cognitive and behavioral aspects of neuroticism. When receiving this strategy, participants are guided to reflect on how emotionally stable people in their environment deal with stressful situations (e.g., “Think of a person who is particularly good at dealing with stress. What behaviors do you observe in them? Describe how you could apply one of these behaviors in your everyday life”).
Skill building via practice
Skill Building via Practice (Coleman et al., 1993; Lyman et al., 2014) is an intervention strategy that primarily addresses behavioral aspects of neuroticism. Participants receive information on skills that are relevant to behave in a less neurotic way (e.g., emotion regulation, stress management, problem solving) and are then guided to implement these skills in their everyday life (e.g., “Imagine your best friend tells you about difficulties in their relationship. How would you use active listening? Give an example of how you – in your imagination – paraphrase, pay attention, and summarize at the end”).
State-level interventions
State-level interventions strategies are provided to TGs 3 and 4. These intervention strategies are presented three times per week.
Behavioral activation
Behavioral Activation (Dimidjian et al., 2011) is an intervention strategy that primarily addresses behavioral aspects of neuroticism. When receiving this strategy, participants select one of three suggestions for behavioral activation throughout the day (e.g., “Do something today that you usually avoid out of anxiety”) and reflect on their success in implementing this activity in the evening (i.e., whether they were able to implement it and how they liked it).
Discrepancy awareness
Discrepancy Awareness (Allemand & Flückiger, 2017) is an intervention strategy that primarily addresses cognitive aspects of neuroticism. When receiving this strategy, participants are guided to reflect on differences between their actual and ideal self (e.g., “What does a typical day in your life look like when you have achieved emotional stability? Which activities, habits and relationships contribute to your inner peace?”). Furthermore, participants receive feedback on their neuroticism scores and changes in their neuroticism levels once per week.
Emotional support
Emotional Support is an intervention strategy that addresses all aspects of neuroticism (e.g., Blossom et al., 2020). When receiving this strategy, participants select one of three suggestions to activate their social network (e.g., “Text a friend today and tell them about your day or about something that has moved you”). In the evening, participants then reflect on their success in implementing and experience of this suggestion.
Exposure to humor
Exposure to Humor is an intervention strategy that addresses affective and cognitive aspects of neuroticism (e.g., Berk & Nanda, 1998). This strategy is incorporated as a companion strategy to the Skill-Building via Modeling component by including humoristic elements in the videos. An example video can be found here.
Mindfulness and meditation training
Mindfulness and Meditation Training (Wielgosz et al., 2019) is an intervention strategy that addresses all aspects of neuroticism. Participants receive guided meditation or mindfulness tasks, such as an audio file with a meditation exercise. In the evening, participants then reflect on their success in implementing and experience of this task.
Physical activity
Physical activity is an intervention strategy that primarily addresses behavioral aspects of neuroticism (e.g., Dinas et al., 2011). When receiving this strategy, participants select one of three suggestions for physical activity in the morning (e.g., “Go for a walk for at least an hour today”). In the evening, participants then rate their success in implementing this strategy and whether they enjoyed it.
Relaxation
Relaxation (Jorm et al., 2008) is an intervention strategy that addresses affective and behavioral aspects of neuroticism. When receiving this strategy, participants receive a video with a guided relaxation exercise. In the evening, participants then reflect on their success in implementing and experience of this task.
Expected outcomes, analysis approaches, and practical implications
Data from the CHILL Study can be used to examine the effects of a digital smartphone intervention on self-reported, peer-reported, and implicitly assessed neuroticism, while also allowing researchers to explore spill-over effects to other constructs and investigate long-term intervention effects. Other critical questions that can be addressed with the CHILL Study concern the optimal timing and frequency of intervention components. For example, do more interventions prompts lead to more pronounced neuroticism changes? At what level may participants be overburdened with intervention prompts? Is there an optimal time point or context to prompt intervention strategies? Furthermore, the CHILL Study will provide insights into whether intervention strategies differ in their efficacy in changing neuroticism: Do different intervention approaches have comparable effect sizes (similar to the dodo bird effect; Wampold et al., 1997) or does intervention efficacy vary systematically depending on the targeted level and aspect of neuroticism? Finally, the daily diary and ESM assessments allow researchers to investigate whether and how experiences and dynamics in daily life may change in response to different types of intervention strategies.
To examine these effects, multilevel modeling and longitudinal structural equation models can be used to deal with the nested data structure. Another analysis strategy that is particularly suitable to test the efficacy of different intervention strategies in the CHILL Study involves the use of computational models (Farrell & Lewandowsky, 2010) that capture how a certain input (e.g., an intervention strategy) can alter a network of states (e.g., negative affect) to impart change in an output (e.g., neuroticism; Revelle & Condon, 2015). In contrast to variable-based models, like structural equation models, that examine covariations among variables to infer causality, computational models require researchers to articulate and test a particular conceptual model of the phenomenon under study. This requires scholars to specify assumptions that are oftentimes left implicit, such as the anticipated timescale of an effect (i.e., amount of time when a meaningful change in neuroticism can be expected, such as days, weeks, or months) and the shape of a change (e.g., gradual change vs. non-linear, stepwise effects). Thus, a core advantage of using computational models is that these models not only indicate if there is an effect, but also provide information about how that effect unfolds over time and across contexts (Riley et al., 2016). As the CHILL Study has assessments of relevant inputs and state variables across multiple timescales, its data can be combined with a computational modeling approach to advance our theoretical understanding of neuroticism change.
The practical utility of a smartphone intervention like the one examined in the CHILL Study is evident in the critical relevance of neuroticism for people’s mental health and well-being (Beck & Jackson, 2022; Cuijpers et al., 2010; Soto, 2019). Compared to psychotherapy which addresses related problems like depression and anxiety, digital smartphone interventions offer flexible and cost-effective intervention approaches that can easily be used by many people (Hardeman et al., 2019; Nahum-Shani et al., 2015). However, smartphone approaches also have important limitations, including being limited to people who have a sufficient intrinsic motivation to decrease their neuroticism. As such, the intervention tested in the CHILL Study may fill a different gap in the mental health space than psychotherapeutic approaches. Investigating the efficacy of an intervention like the one implemented in the CHILL Study is important to have efficacious treatment tools across the entire spectrum, from subclinical to clinical neuroticism.
Conclusion
As many people desire to become less neurotic (Baranski et al., 2021; Hudson & Fraley, 2016), developing an effective neuroticism intervention that can effectively reduce neuroticism in the general public is of critical practical relevance (Bleidorn et al., 2019). The CHILL Study aims to evaluate the effects of a digital intervention to promote neuroticism change. It moves beyond existing research on volitional personality change as it allows to distinguish the effects of different intervention strategies and provides insights into individual differences in intervention-induced neuroticism change. As such, the CHILL Study may facilitate the development of a comprehensive theory of neuroticism change (Bleidorn, 2024).
Supplemental Material
Supplemental Material - A smartphone-based intervention to decrease neuroticism: Protocol of the CHILL Study
Supplemental Material for A smartphone-based intervention to decrease neuroticism: Protocol of the CHILL Study by Peter Haehner, Amanda J. Wright, Rosalie Andrae, Till Lubczyk, Leyla A Rosero Betancourt, Christopher J. Hopwood and Wiebke Bleidorn in Personality Science
Footnotes
Author note
Dr Carolyn MacCann was the handling editor.
Acknowledgements
We would like to thank Mathias Allemand for sharing his insights and materials on personality interventions with us.
Author contributions
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Wiebke Bleidorn and Christopher J. Hopwood are members of the journal’s editorial board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data collection of the CHILL Study was funded by an SNSF Consolidator Grants awarded to Wiebke Bleidorn [Grant number 213696].
Data accessibility statement
Supplemental material
Supplemental material for this article is available online. Depending on the article type, these usually include a Transparency Checklist, a Transparent Peer Review File, and optional materials from the authors.
Note
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.