
Abstract
Gestational diabetes mellitus (GDM) affects many women in pregnancy and is enhanced by epidemic conditions of obesity, increasing age at the time of the first pregnancy, stressful life conditions, a sedentary lifestyle with less physical activity and unhealthy nutrition with highly processed, high-calorie food intake. GDM does not affect the mother and offspring in pregnancy alone, as there is compelling evidence of the long-term effects of the hyperglycemic state in pregnancy postpartum. Type 2 diabetes mellitus, cardiovascular disease and metabolic syndrome are more common in GDM women, and even the offspring of GDM women are reported to have higher obesity rates and a higher risk for noncommunicable diseases. Early prevention of risk factors seems to be key to overcoming the vicious cycle of cardiometabolic disease onset.
Keywords
According to WHO, cardiovascular diseases (CVDs) are the most common cause of death globally, representing 30% of all deaths [1]. A further increase in deaths from 17.3 million in 2008 to 23.3 million deriving from CVDs is expected by the year 2030, mainly due to an increase of the following risk factors: unhealthy diet, obesity or Type 2 diabetes mellitus (T2DM), hyperlipidemia and physical inactivity [1,2]. Compared with men, who are prone to suffer from CVDs approximately 10 years earlier, women face a similar or aggravated risk profile after menopause [3]. However, women face less risk during their reproductive age due to a protective effect of estrogens. In fact, recent studies show that female risk populations, such as women suffering from polycystic ovary syndrome, T2DM or gestational diabetes mellitus (GDM), have an increased risk for CVDs [4]. Prediabetes or T2DM increase the risk for women tremendously, and women with impaired glucose metabolism encounter cardiovascular mortality more frequently [3,4]. Moreover, an elevated risk of myocardial infarction and stroke was already seen many years prior to clinical diagnosis of T2DM [5]. GDM is most often reported to have a prevalence of 2–6% in Europe and is reported to be higher after switching to new International Association of the Diabetes and Pregnancy Study Groups (IADPSG) criteria and in other ethnicities, with numbers ranging from 1.7 to 11.6% in advanced economies [6–9]. Buckley
Methods
A critical review of the worldwide peer-reviewed literature was conducted relating to the cardiovascular risk of women with GDM or a history of GDM. Using Medical Subject Heading (MEsH) search terms in the MEDLINE and EMBASE databases gave a result of 157 relevant abstracts (Table 1 & Supplementary Material; see online at www.futuremedicine.com/doi/suppl/10.2217/whe.13.69). Only data derived from human studies were chosen as relevant. Material produced from 2005 onwards was sought in order to ensure that the evidence was current. Only in highly important cases was peer-reviewed literature from years prior to 2005 chosen. In addition, duplicates were removed. All abstracts were searched for relevant information regarding CVD after GDM. After careful examination of the relevant literature, a hand search was carried out in order to identify further relevant literature from the reference lists. Using the Scopus database, forward and backward literature searches were performed for highly important articles only and for literature regarding treatment and prevention methods. Forty seven relevant articles were identified. In addition, two independent literature searches were performed in order to identify literature regarding lifestyle or pharmacological interventions in women with GDM and previous GDM to prevent progression of CVD or T2DM, and to identify cytokines, adipokines, hormones and other metabolic parameters throughout pregnancy in normal glucose-tolerant and gestational diabetic women, as well as previously diabetic women and obese/diabetic subjects. Further information regarding additional searches can be found in the Supplementary Material. Because the sources of information varied widely, a narrative synthesis approach was judged to be the most appropriate method for this review, which is mainly descriptive and does not involve a systematic approach [202].
Search protocol using Medical Subject Heading search terms in the MEDLINE and EMBASE databases.

Slash symbol (/) indicates that all subheadings were selected. ‘Exp’ indicates that the term was exploded.
Results
Cardiometabolic risk factors
Increased glucose levels and diabetes mellitus are well-known cardiovascular risk factors, in addition to other modifiable and unmodifiable risk factors that are relevant for metabolic diseases and CVDs (Figure 1). Diabetic women in particular have a four- to six-fold increased risk of developing coronary artery disease [22]. Studies have shown a vast variety of modifiable risk factors in GDM women and women with mild hyperglycemia with impaired glucose tolerance, atherogenic lipid profiles, higher age, lower insulin sensitivity, impaired β-cell function, elevated highly sensitive CRP (hsCRP) and, in addition, increased carotid intima–media thickness (CIMT) at a few months postpartum (Table 2) [23–28]. Possession of two risk factors has been found to result in higher risk compared with pregnancies with only one risk factor [23]. A cutoff of 88 cm for waist circumference was shown to have a significant effect on diabetes progression [23].
Risk factors for cardiovascular disease in women previously affected by gestational diabetes mellitus.

↑ Increased; CIMT: Carotid intima–media thickness; GDM: Gestational diabetes mellitus; HDL: High-density lipoprotein; HOMA: Homeostatic model assessment; HR: Hazard ratio; hsCRP: Highly sensitive CRP; IFG: Impaired fasting glucose; IGT: Impaired glucose tolerance; IR: Insulin resistance; LDL: Low-density lipoprotein; MetSy: Metabolic syndrome; NS: Not significant; OGTT: Oral glucose tolerance test; pp: Postpartum; RRsys: Systolic blood pressure; T1DM: Type 1 diabetes mellitus; T2DM: Type 2 diabetes mellitus.

Modifiable and unmodifiable risk factors for cardiovascular disease in women with gestational diabetes mellitus and women affected by the metabolic syndrome.
In general, progression to T2DM is a very strong risk factor for future CVD, with a fourfold cardiovascular risk elevation even before diagnosis and a long list of equally modifiable risk factors [29,30]. An older cross-sectional study found no differences between self-reported GDM and normal glucose tolerance (NGT) groups in terms of most cardiovascular risk factors, except for greater levels of mean fasting glucose (94.0 mg/dl/5.2 mmol/l vs 106.8 mg/dl/5.9 mmol/l; p < 0.001) and mean fasting insulin (10.2 vs 14.0 IU/l; p < 0.001) [14]. After adjustment for demographic factors and waist circumference, a mitigating effect was observed. Fasting glucose and the ratio of urine microalbumin:creatinine remained significant. Increased body fat mass is often reported to be higher in GDM women compared with other groups, showing its important role in the pathogenesis of both T2DM and CVD; it is unknown whether T2DM and CVD are independent or dependently interacting with each other in this case [31,32]. Two large-scale population-based studies, together assessing more than 1.6 million participants, indicated that women with GDM have a higher risk for pre-eclampsia and pregnancy-induced hypertension (PIH), both of which are associated with CVD and hypertension in later life [33,34].
GDM & epigenetics
In addition to various environmental stressors triggering methylations, hydroxymethylations, histone modifications and RNA-based mechanisms, and causing quick adaption of cells, maternal hyperglycemia was reported to affect fetal development
Figure 1 gives an overview of the ‘common soil’ risk factors in CVDs and T2DM, but primarily focuses on postpartum findings in women with GDM. GDM and/or the metabolic syndrome are influenced by genetic background, as well as epigenetics. Post-GDM women often show hypertension and endothelial dysfunction. Furthermore, pre-eclampsia and pregnancy-induced hypertension are more often detected in GDM women. Dyslipidemia (increased free fatty acids, higher triglycerides and lower high-density lipoprotein cholesterol) and ectopic lipids (increased intramyocellular and hepatocellular lipid storage), as well as impaired body fat distribution with central obesity, are commonly seen in GDM women postpartum. This results in unfavorable changes in adipokines or cytokines. Markers of inflammation are raised and often associated with a prothrombotic state. This is often associated with lifestyle factors, such as overnutrition and physical inactivity, which further increase the risk for CVD.
Cardiovascular risk: continuous effects of mild metabolic disturbances or induction through overt T2DM
In a cross-sectional study with 995 GDM and healthy participants, women with a history of GDM had a higher prevalence of CVD (adjusted odds ratio [OR]: 1.85; 95% CI: 1.21–2.82) independent of T2DM [42]. All of these women had a family history of T2DM. Not only higher CVD events at a younger age were reported, but CVD risk factors, such as T2DM and the metabolic syndrome, were also more common. Another study confirmed these results of a higher risk for CVD events in GDM women over the course of 11.5 years [43]. A study investigating the influence of mild glucose intolerance on cardiovascular risk was performed by Retnakaran and Shah [44]. A 50-g glucose challenge test (GCT) in order to screen for abnormal glucose tolerance was carried out in a sample of nearly 450,000 women aged between 20 and 49 years followed by an oral glucose tolerance test (OGTT) if the GCT was abnormal. In total, 71,831 of the participants had an abnormal GCT but NGT, 13,888 women had an abnormal GCT and GDM, and 349,977 women had a normal GCT. The median follow-up time was 12.3 years. Primary outcomes included admission to hospital for acute myocardial infarction, coronary bypass, coronary angioplasty, stroke or carotid endarterectomy. A higher risk was seen in women with GDM, and women with abnormal GCT only compared with control women. Cardiovascular event rates per 10,000 person-years were 4.2, 2.3 and 1.9 among women with GDM, an abnormal GCT but normal OGTT and NGT, respectively. The adjusted hazard ratio (HR) for women with GDM for CVD was 1.66 (95% CI: 1.30–2.13), while for those with an oral glucose test but no GDM, the adjusted HR was 1.19 (95% CI: 1.02–1.39) compared with women with NGT. After adjustment for consecutive progression to T2DM, the relationship between CVD, GDM and mild glucose intolerance was attenuated, which corroborated previous results in which the CVD risk was mitigated from a HR of 1.71 (95% CI: 1.08–2.69) to a HR of 1.13 (95% CI: 0.67–1.89) [43]. In this study, a great proportion of the elevated risk for CVDs could be reasoned with the subsequent progression to T2DM. Nevertheless, taking into account the relatively young study population with a low-risk potential and the long onset time of diabetes-induced CVD, the authors concluded that there was no relationship between T2DM and CVD in this sample [44]. A ‘common soil hypothesis’ was discussed as the underlying mechanism for CVD and T2DM [44,45]. This study concluded an increased incidence of subsequent CVD in women with mild hyperglycemia – not affected by GDM – and presented a continuous effect of hyperglycemia on adverse cardiovascular outcomes. To date, no clear segregation can be made between CVD risk coming from GDM or mild hyperglycemia, or through the development of T2DM. Further studies need to evaluate this aspect.
Clinical relevance of 1-h glucose values
Women who are not diagnosed with GDM but instead with isolated hyperglycemia using the 1-h postpartum OGTT had a higher cardiovascular risk than women with elevated 2- or 3-h glucose levels, suggesting the clinical importance of peak glucose values for risk assessment [46]. The clinical relevance of the 1-h OGTT for postpartum risk assessment was confirmed by another study showing that, at 3–6 months postpartum, the 1-h OGTT value was a stronger predictor of insulin sensitivity than fasting or 2-h glucose values [47], thus, peak glucose levels are of clear clinical importance for the further cardiometabolic risk stratification of women with GDM.
Vascular abnormalities & endothelial dysfunction in GDM & prior GDM
Studies show an influence of hyperglycemia on vascular function with conflicting results [32,48–52]. In a 2-month postpartum follow-up study, arterial stiffness and endothelial function were assessed by Davenport
Changes in nitric oxide bioactivity
Impaired endothelial function was described in GDM in several studies and assessed by a decreased bioactivity of vascular nitric oxide (NO), at least in overweight women [60]. In this study, insulin resistance and increased ADMA – an endogenous NO synthase (NOS) inhibitor – contributed to endothelial dysfunction. In another study, elevated concentrations of ADMA were associated with deterioration of glucose tolerance in women with GDM after a median follow-up of 2.75 years [61]. Moreover, ADMA was described to be associated with obesity [53].
Another study anaylzed subcutaneous arterial biopsies at 2 years after pregnancy, including eight control women, 13 mild hyperglycemic women and eight women in a GDM group [32]. GDM and mild hyperglycemic women had normal vascular structure and stiffness, but also had clearly detectable impaired endothelium-dependent function. Response to carbachol in terms of maximal endothelium dilation was impaired in arteries from mild hyperglycemic women (51.7%; p = 0.04) and GDM women (43.3%; p = 0.01). Impairment in NOS activity was detected in GDM and mild hyperglycemic women after inhibition of NOS with decreased maximum endothelium-dependent dilation. Moreover, endothelial impairment was associated with BMI at biopsy in multiple regression models, but not with current glycemia. The authors concluded that vasocrine signals from adipose tissue affect glycemia and influence small vessel function [32,62]. In particular, perivascular fat seems to have a vital function in vascular integrity and local inflammation, causing anticontractile effects and mediators [63]. Whether the mechanisms behind vascular impairment are caused primarily by plasma glucose or are related to inflammatory processes in adipose tissue remains unclear.
Endothelial adhesion molecules & dysfibrinolysis
Endothelial adhesion molecules have a major role in the pathogenesis of CVD and were shown to be significantly increased in GDM and NGT women in pregnancy [52]. After delivery, circulating E-selectin and circulating VCAM-1 remained increased only in GDM women. Moreover, correlations between E-selectin and glycated hemoglobin were described before and after delivery. In a more recent study, E-selectin levels were shown to correlate with triglycerides, PAI-1 antigen and soluble ICAM-1 [51]. These findings indicate an association of GDM with atherogenic biomarkers and ICAM-1 independently of BMI and fasting glucose. Furthermore, a study of 74 GDM and 20 NGT women during and after pregnancy showed significantly elevated mean PAI-1, tissue plasminogen activator, fasting and stimulated plasma concentrations of proinsulin, C-peptide and insulin in GDM women, as well as a lower disposition index and no changes in plasma levels of fibrinogen and von Willebrand factor [31]. In prediction models for PAI-1 elevation, only fasting proinsulin and the waist:hip ratio remained significant in women with GDM with impaired insulin sensitivity, indicating a dependence of PAI-1 on plasma proinsulin and abdominal obesity.
After 6.5 years of follow-up, higher levels of E-selectin and ICAM-1, and higher intima–media thickness were observed [64]. Intima–media thickness was significantly associated with E-selectin, ICAM-1, IL-6 and hsCRP.
Inflammatory parameters
Several studies examined women with GDM aiming to measure cytokines and adipokines postpartum [55,65–80]. Glucose tolerance and insulin sensitivity are strongly influenced by inflammatory mediators, such as CRP, IL-6, PAI-1 and TNF-α, as well as mediators produced in adipose tissue – so-called adipokines (e.g., adiponectin, leptin, RBP-4, resistin, visfatin, omentin, nesfatin and chemerin) or other peptides influencing glucose homeostasis, which seem to play an important role in the subsequent pathogenesis of T2DM or subsequent CVD in women with previous GDM (Table 3).
Cytokines, adipokines, hormones and other metabolic parameters throughout pregnancy in normal glucose-tolerant and gestational diabetic women, previously gestational diabetic women and obese/diabetic subjects.
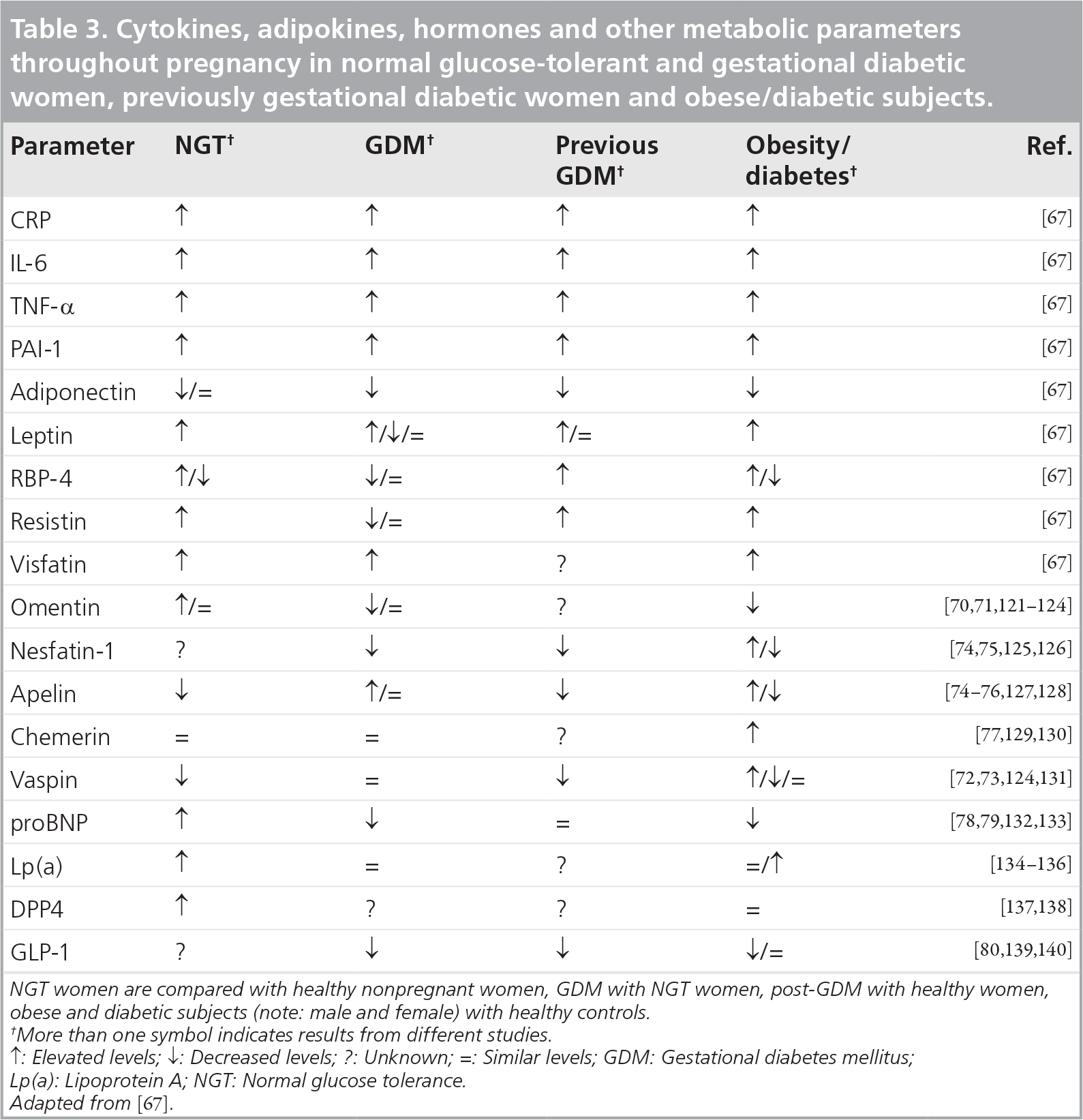
NGT women are compared with healthy nonpregnant women, GDM with NGT women, post-GDM with healthy women, obese and diabetic subjects (note: male and female) with healthy controls.
More than one symbol indicates results from different studies
↑: Elevated levels; ↓: Decreased levels; ?: Unknown; =: Similar levels; GDM: Gestational diabetes mellitus; Lp(a): Lipoprotein A; NGT: Normal glucose tolerance. Adapted from [67].
Ectopic lipid content
Kautzky-Willer
Studies examining ectopic lipid content in gestational diabetic women.

GDM: Gestational diabetes mellitus; IHCL: Intrahepatocellular lipid content; IMCL: Intramyocellular lipid content; IR: Insulin resistant; IS: Insulin sensitive; NGT: Normal glucose tolerance; S: Soleus muscle; T: Tibialis anterior muscle.
A different approach for predicting future cardiometabolic disturbances of prior GDM was derived from the calculation of a fatty liver index (FLI), as assessed by 1H-magnetic resonance spectroscopy at 3–6 months postpartum [85]. Strong positive associations with insulin resistance were shown with increasing FLI in GDM women. The high-FLI group also had elevated IL-6, PAI-1, tissue plasminogen activator, fibrinogen and hsCRP in comparison with the low-FLI group. Furthermore, the degradation of free fatty acids measured during the course of the OGTT was less pronounced in the high-FLI group. In another study, free fatty acids were higher in women with GDM, which was hypothesized to result from impairment of lipolysis inhibition caused by insulin [86]. Hyperlipidemia and ectopic lipid storage may therefore increase the risk of T2DM and CVD. Notably, the incidence of prediabetes or diabetes increased with FLI levels, and the calculation of risk for diabetes onset over 10 years in Cox proportional hazard models showed an association of FLI levels with diabetes risk [85]. Women in the high-FLI group had the highest risk compared with the low-FLI group (HR: 7.85; 95% CI: 2.02–30.5), suggesting that high liver fat content is a relevant risk factor in addition to insulin resistance or prediabetes for progression to T2DM and subsequent CVD in the near future.
Prevention factors
Many modifiable risk factors in women with previous GDM progressing to T2DM and subsequent CVD have been reported above. Disease prevention seems to be a very appropriate way to break the vicious cycle of cardiometabolic disease pathogenesis with a ‘common soil’ of risk factors. Different approaches, with impressive and promising results, have been reported throughout literature [15–18,87–105].
Lactation
A recent German study investigated long-term protective effects of breastfeeding on the development of T2DM in 304 GDM women [89]. The follow-up time was up to 19 years postpartum. The development of T2DM was dependent on treatment during pregnancy (dietary vs insulin), BMI and the detection of islet autoantibodies.
The median duration of breastfeeding was 9 weeks and was shorter in insulin-treated GDM and obese women. Breastfeeding was associated with a median onset time of T2DM of 12.2 years (95% CI: 7.7–16.8) only in autoantibody-negative GDM women, whereas in women who never breastfed, it was only 2.2 years (95% CI: 0.0–6.1; p = 0.012). A duration of more than 3 months was associated with lowest risk, with a 15-year risk of 42% (95% CI: 28.9–55.1) compared with 72% (95% CI: 60.5–84.7; p = 0.0002). This study demonstrates an easy and cost-effective method of cardiometabolic disease prevention in women affected by GDM, which was confirmed by another study examining data of 139,681 postmenopausal women and their risk for CVD in relation to lactation [90]. Women with more than 12 months of lactation in their lives reported less hypertension (OR: 0.88), diabetes (OR: 0.80), hyperlipidemia (OR: 0.81) or CVD (OR: 0.91) than never-breastfeeding women. Obesity was not affected by breastfeeding. This study clearly showed – for most risk factors – an inverse association of prevalence of hypertension, T2DM, hyperlipidemia and CVD with duration of lactation. Primiparas, who were breastfeeding for between 7 and 12 months, were significantly less affected by CVD (HR: 0.72; 95% CI: 0.53–0.97) than women who were not. In addition, a longer duration of lactation was associated with a risk reduction in incidence of the metabolic syndrome over a timespan of 20 years in women both with and without GDM [91]. Decreasing incidence rates were seen in GDM women (49.4 [95% CI: 25.8–84.7] to 8.5 [95% CI: 1.8–24.8]) and NGT women (15.8 [95% CI: 11.3–21.5] to 9.2 [95% CI: 5.3–14.6]). Despite demonstrating the effectiveness of breastfeeding in white women, black women seemed to have no or limited benefit from lactation. Lactation clearly shows benefits in pregnant women of up to an adjusted risk reduction of nearly 90% in GDM women (HR: 0.14; 95% CI: 0.04–0.55) and 60% in NGT women (HR: 0.44; 95% CI: 0.23–0.84) after 9 months or more of breastfeeding, which was intensified by physical activity in the GDM group [91]. The evidence favors a strong positive association of breastfeeding duration with a reduction of cardiometabolic disorders, starting at a duration of 1 month breastfeeding and with an increasing risk reduction with increasing duration of lactation.
Lifestyle intervention
With respect to lifestyle intervention programs, there are two possibilities: either to prevent the onset of GDM in pregnancy or to prevent the onset of T2DM after a diagnosis of GDM. Indisputably, both approaches together provide the best efficacy.
Lifestyle intervention in pregnancy
Some studies examined or will examine the effectiveness of lifestyle interventions in pregnancy [15,17,18,88,93,102]. Table 5 presents recent lifestyle intervention studies in pregnancy.
Lifestyle intervention strategies in gestational diabetic women in pregnancy.
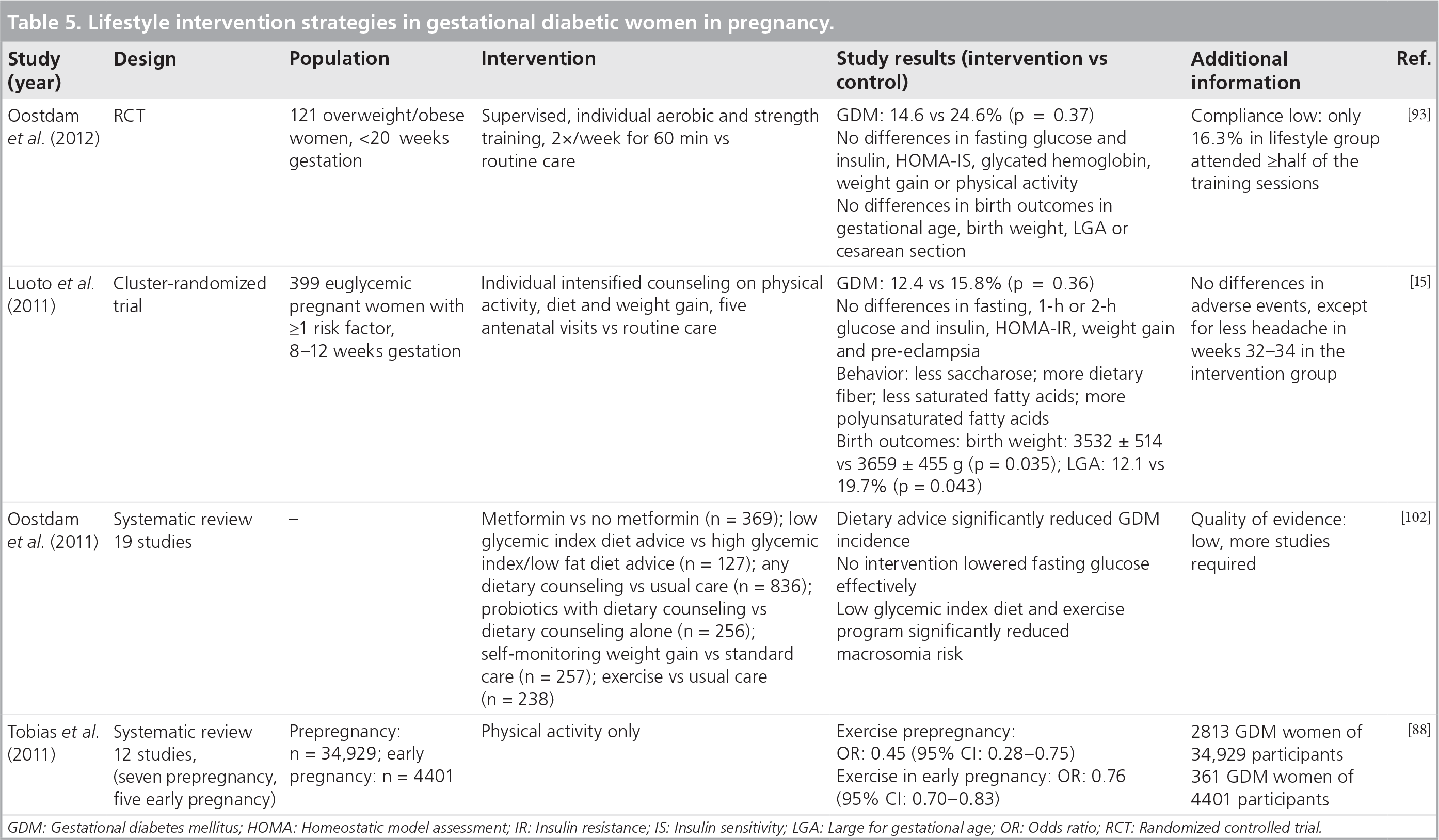
GDM: Gestational diabetes mellitus; HOMA: Homeostatic model assessment; IR: Insulin resistance; IS: Insulin sensitivity; LGA: Large for gestational age; OR: Odds ratio; RCT: Randomized controlled trial.
Unfortunately, no effect of lifestyle intervention was found in the ambitious FitFor2 study [93]. Analysis based on the intention to treat showed no differences between groups. One reason for the lack of observed effects in this study was low compliance. Similar results were reported in other studies, suggesting that commencing intervention programs in the second semester might be too late, whereas physical activity before pregnancy and in the first trimester of pregnancy was significantly associated with lower GDM risk [88,102]. A Finnish lifestyle intervention study demonstrated fewer numbers of large-for-gestational-age newborns at birth and changes in dietary behavior in GDM women during pregnancy, and revealed a decreased risk of developing GDM in the lifestyle cohort [15].
On the other hand, in another study, dietary interventions effectively reduced the risk of GDM by 60%, as well as gestational hypertension and preterm birth [103]. The Vitamin D and Lifestyle Intervention for Gestational Diabetes Mellitus Prevention project is going to examine whether dietary intervention, physical activity or vitamin D in different combinations will be effective in the prevention of the development of GDM in overweight and obese women [106]. The Vitamin D and Lifestyle Intervention for Gestational Diabetes Mellitus Prevention study is currently being performed in 880 obese pregnant women.
Lifestyle intervention after pregnancy A lifestyle intervention pilot study delivered by telephone for 12 months in previously GDM women reported a nonsignificant but higher postpartum weight control in diet and physical activity groups compared with controls (37.5 vs 21.4%; p = 0.07) [98]. In the intervention group, a significantly decreased dietary fat intake compared with usual care was observed, in addition to not significantly increased breastfeeding. The feasibility of lifestyle interventions starting at the diagnosis of GDM in pregnancy and throughout the postpartum period was proven in this study, with retention at over 85%. Furthermore, women meeting the Institute of Medicine recommendations for weight gain in pregnancy more often met the study aims of regaining prepregnancy weight [98,107].
Several large-scale lifestyle intervention studies in order to prevent the onset of T2DM also included GDM women (~16%) and showed effectiveness (Table 6) [99–101]. In all three studies (SLIM, DPP and DPS studies), diabetes incidence was reduced significantly. Only the DPP study provided a subanalysis for women with a history of GDM [96]. Prior GDM women had a crude incidence rate of diabetes that was 71% higher than those who were unaffected during pregnancy. Lifestyle intervention reduced diabetes incidence by approximately 50%. A small Malaysian study in women with previous GDM showed that a low glycemic index diet compared with conventional dietary recommendations over 6 months was associated with significant weight reduction and improved metabolic parameters [95]. In conclusion, lifestyle intervention in GDM women postpartum is an effective approach to delaying T2DM onset and subsequent diabetic angiopathy.
Overview of lifestyle and pharmacological intervention studies.
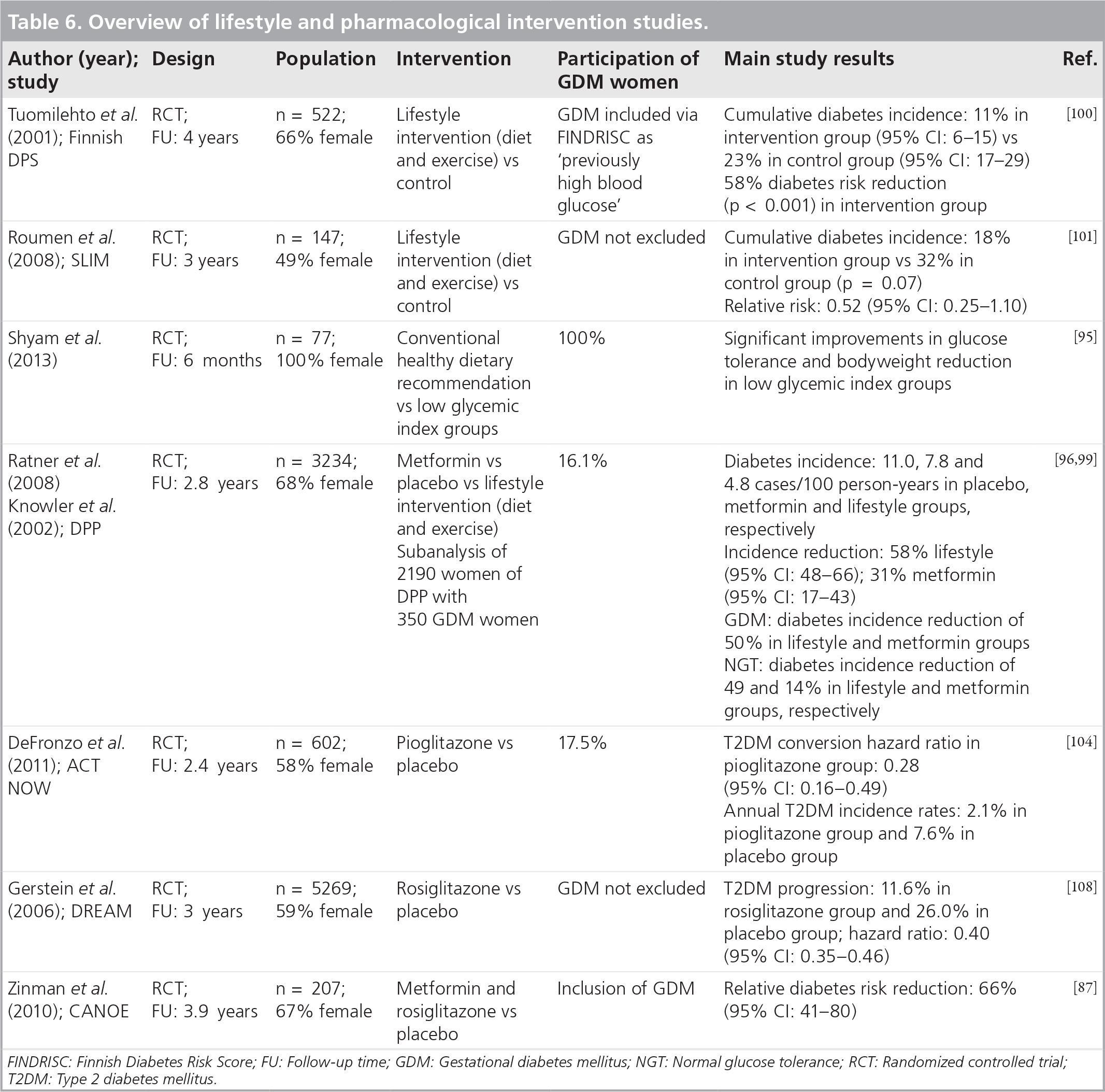
FINDRISC: Finnish Diabetes Risk Score; FU: Follow-up time; GDM: Gestational diabetes mellitus; NGT: Normal glucose tolerance; RCT: Randomized controlled trial; T2DM: Type 2 diabetes mellitus.
Table 6 gives an overview of lifestyle and pharmacological studies, which included or were carried out in women with a history of GDM. Figure 2 shows the treatment options for women with previous GDM.

Prevention options in women with gestational diabetes mellitus.
Pharmacological intervention studies
Several studies investigated pharmaceutical treatment options and included GDM women at postpartum (Table 1) [87,96,97,104,108]. An approximately 50% reduction in diabetes incidence was observed in the GDM group treated with metformin in the DPP study [96]. Higher effectiveness of metformin in women with a history of GDM compared with those without was also reported. In the ACT NoW study, the risk of progression to T2DM was significantly reduced, but a higher prevalence of side effects, such as weight gain and edema, was also observed [104]. The PIPOD study determined the progression of CIMT in premenopausal Hispanic women with previous GDM [97]. The CIMT rate in women receiving pioglitazone was 69% lower after 3 years of therapy. Furthermore, other diabetes prevention studies, such as DREAM or CANOE, using pharmacological interventions showed high effectiveness in the total study groups, but did not report effectiveness in subgroups, such as GDM women (Table 6).
Figure 2 presents the prevention options for stopping the subsequent progression of CVD. Different approaches have been shown to be effective (e.g., increased physical activity or a healthy diet in order to maintain normal weight or reduce weight [5–10%] if overweight or perfroming a randomized controlled trial showing a positive effect of pioglitazone or metformin) [15,17,18,87,88,93,95–97,99–102,104,108]. The data currently available indicates that incretin-based therapies might be of relevance in CVD prevention in the future [109], but further studies need to prove this. Other lifestyle factors, as well as other ameliorating factors, are also of importance. Regular follow-up visits are recommended in order to control for metabolic or other risk factors in patients who are at high risk.
Subsequent pregnancy & contraception
The influence of a subsequent pregnancy was examined in a Canadian sample of women with a 4.5-year follow-up time [110]. The hypothesis that physiological insulin resistance of a subsequent pregnancy accelerates the pathogenesis of T2DM was discussed. In this sample, 16.2% of participants developed GDM. After adjustment, an association between reduced diabetes risk and subsequent pregnancy was found (adjusted HR: 0.68; 95% CI: 0.60–0.76). Above all, a modestly increased risk of T2DM was seen in subsequent GDM pregnancies (adjusted HR: 1.16; 95% CI: 1.01–1.34), as well as a decrease in risk with each nondiabetic pregnancy (adjusted HR: 0.34; 95% CI: 0.27–0.41). In subsequent pregnancies with recurrent GDM, we could not find any association with either impairment of glucose metabolism or cardiovascular risk [111].
There is a lack of information in terms of choice of best contraceptive method after GDM, with there only being a few published studies. No significant changes in carbohydrate metabolism were described with hormonal contraception [112]. If obesity, hypertension or dyslipidemia are present, either a hormonal contraceptive with no vascular effects or a mechanical method is recommended [112]. In addition, the use of gestagen-only contraceptives was described to lead to an increased risk for T2DM in Hispanic populations [113].
Conclusion & future perspective
As GDM, obesity, T2DM and CVD prevalence is growing, further randomized controlled trials focusing on intervention methods in pregnancy and thereafter – or, even better, involving both periods – are needed in order to shed light on the pathogenesis of these diseases. We need evidence of specific treatment strategies that are able to reduce obesity and the metabolic syndrome postpartum, and subsequent CVD.
Health economies all around the world are called to invest in primary preventative approaches, as the costs of cardiometabolic diseases are rapidly increasing and are more expensive if diseases have fully progressed. Cost–effectiveness analyses revealed that new International Association of Diabetes and Pregnancy Study Group (IADPSG) criteria are effective when postpartum monitoring is able to prevent diabetes progression [114]. International consensus on GDM diagnosis, as recently presented by WHO [115], screening methods, treatment options and treatment after delivery is urgently needed, as this disease affects not just the mother, but also the child. Furthermore, screening rates are reported to be far from optimal, with only approximately half of all women attending a postpartum retest [116].
Lifelong monitoring is recommended for all diagnosed abnormalities of glucose metabolism, starting at the detection of prediabetes. Moreover, screening for glycemic abnormalities after GDM in pregnancy helps to identify women who are at high risk for T2DM and CVD, and might help to reduce complications in following pregnancies, as well as discovering women who might benefit from lifestyle and pharmacological interventions. With regards to the prevention of the development of GDM, many studies suggest a major role of hyperglycemia in pregnancy on outcomes, cardiometabolic parameters and disease progression in the offspring. Intrahepatocellular lipid content at 1–3 weeks of age measured by magnetic resonance spectroscopy was 68% higher in children born to obese or GDM mothers compared with normal-weight mothers, suggesting a fetal origin of nonalcoholic fatty liver disease [117]. In 587 Caucasian offspring of mothers with a diabetic pregnancy, the effects of intrauterine hyperglycemia were examined at 18–27 years after their delivery [118]. This study showed a higher risk for glucose intolerance in the offspring of diabetic mothers, as insulin sensitivity and β-cell functions were impaired. Placental dysfunction is triggered by hyperglycemia, which causes vascular impairment, misbalance of vasoactive molecules and enhanced oxidative stress, and affects both the mother and fetus [119]. Substrates playing key roles in angiogenesis are proven to be impaired due to hyperglycemia triggered by the growth factors insulin and IGF-II [120].
Future studies should extend our current knowledge of GDM-related cardiometabolic risk to include new biomarkers that are able to predict increased risk of cardiovascular events and diabetes in the mother and offspring. Important research topics will include studies of GDM offspring and fetal programming in order to increase our understanding of the impact of the intrauterine environment on future health and enable primary prevention of cardiometabolic disease. When looking through the literature, no clear distinction could be made between CVD and T2DM, as both diseases have the same underlying risk factors, suggesting a ‘common soil’ of disease progression. A continuous effect of hyperglycemia on adverse cardiovascular outcomes is speculated and was reported in one study [44], but more studies would be needed focusing specifically on this aspect.
As at least two generations are affected by GDM (the mother and offspring), future preventative programs should either focus on finding the best modalities to prevent the onset of GDM or on finding treatment possibilities as soon as possible. Lifestyle intervention programs for the mother and child affected by GDM, or ideally for the whole family, are needed, as nearly all family members face similar risk factors. Mostly, women at high risk suffer from GDM by the first trimester and experience untreated hyperglycemia for several weeks until GDM screening at 24–28 weeks of pregnancy. Thus, screening for women who are at high risk should take place as early as possible, ideally using a WHO 75-g OGTT, or at least an assessment of fasting glucose or glycated hemoglobin. With an epidemic of obesity, T2DM and CVD in mind, disease prevention programs are key to stopping disease progression in patients who are at risk, and these may be able to save enormous costs for economic systems, as disease onset is stopped or delayed. Taking into account the idea that, for all noncommunicable diseases, the predicted future numbers will rapidly increase, actions to stop the onset of disease will have to start now, not in future.
Executive summary
Women with polycystic ovary syndrome, Type 2 diabetes mellitus (T2DM) or gestational diabetes mellitus (GDM) have an increased risk for cardiovascular diseases (CVDs). Women with impaired glucose metabolism encounter cardiovascular mortality more frequently.
Progression to T2DM based from previous GDM is a very strong risk factor for future CVD, with a fourfold cardiovascular and coronary artery disease risk elevation.
Women with previous GDM are at higher risk for CVD at a younger age compared with their healthy peers.
GDM progresses to T2DM in 2.6–70% of cases after 6 weeks to 28 years postpartum.
An association between metabolic disturbances and CVDs in the mother and offspring has been reported.
A higher risk of T2DM onset was found in black women. Furthermore, Asian–Indian and African-Caribbean ethnicities were described to have impaired glucose tolerance more often.
Insulin sensitivity and glycemic state seem to play key roles in progression to CVD.
Screening of women who are at high risk for T2DM should take place as early as possible after a GDM pregnancy, or at least a measurement of fasting glucose and glycated hemoglobin should be taken.
A continuous effect of hyperglycemia on adverse cardiovascular outcome has been speculated.
Early derangement of endothelial function is directly influenced by hyperglycemia in pregnancy and thereafter.
In GDM, endothelial function is impaired, as determined by a decreased bioavailability of nitric oxide and nitric oxide synthase activity.
Perivascular fat seems to have a vital function in vascular integrity and local inflammation.
Endothelial adhesion molecules play a major role in the pathogenesis of CVD.
GDM women have higher body fat mass and lower insulin sensitivity.
Mean intramyocellular lipid contents in soleus and tibialis anterior muscles are higher in GDM women. Intramyocellular lipid content of the tibialis reflects insulin sensitivity, whereas intramyocellular lipid content of the soleus is related to obesity.
Women treated with insulin shows significantly higher intramyocellular lipid contents in soleus and tibialis anterior muscles than dietary-treated women.
Intrahepatocellular lipids are twice as high in previously GDM and insulin-resistant women.
GDM women with high liver fat content have increased insulin resistance and higher fasting serum triglyceride and insulin concentrations compared with low liver fat content women.
Hyperlipidemia and ectopic lipid storage might increase the risk of T2DM and CVD.
An approximately 50% reduction of diabetes incidence was observed in a GDM group with metformin treatment.
Pioglitazone reduces the risk of progression to T2DM by 72%.
Subclinical atherosclerosis progression is decelerated by pioglitazone.
More than 3 months of breastfeeding is associated with a lower risk of T2DM progression.
More than 12 months of lactation in life results in less hypertension, diabetes, hyperlipidemia or CVD. Obesity is not affected by breastfeeding.
Lifestyle intervention reduces diabetes incidence by approximately 50%.
Dietary interventions reduces the risk of GDM by 60%, as well as bringing about a significant reduction of gestational hypertension and preterm birth.
Physical activity before and in early pregnancy is significantly associated with lower GDM risk.
Lifelong monitoring is recommended for all with diagnosed abnormalities of glucose metabolism, starting at the detection of prediabetes.
Early prevention of risk factors seems to be key to breaking the vicious cycle of cardiometabolic disease onset.
Recommendations from guidelines are conflicting, compliance for follow-up visits among women after GDM is poor and high-quality interventions are lacking. Therefore, it is necessary to establish standard guidelines for the prevention, diagnosis and correct treatment of both GDM and CVDs.
Acknowledgements
Financial & competing interests disclosure