
Abstract
Background:
A positive childbirth experience is closely associated with women’s active participation and sense of control. Although evidence supports mobility during labor as a strategy to enhance autonomy and improve outcomes, institutional practices often restrict women’s freedom of movement. Antenatal education may foster informed choices and active engagement in labor. This study aimed to assess the feasibility and preliminary effects of a woman-centered antenatal intervention on emancipated decision making, satisfaction with decision, childbirth self-efficacy, and birth beliefs, as well as its associations with labor and birth outcomes.
Methods:
This pre-experimental, pre- and posttest quantitative study was conducted in a community setting. Fifty-six women completed baseline measures (T1), 38 postintervention (T2), and 30 after childbirth (T3). The intervention included two group sessions combining experiential learning, communication strategies, and decision-making practice. Paired and nonparametric tests assessed changes in outcomes. Correlation and regression analyses explored associations with clinical and experiential outcomes.
Results:
The intervention was feasible and well accepted, with 53% overall retention and high satisfaction (mean = 9.73/10). Statistically significant improvements were observed in satisfaction with decision (p < 0.001, d = 0.60) and natural birth beliefs (p < 0.001, r = 0.61), while other outcomes showed small, nonsignificant positive trends. A modest association was found between natural birth beliefs and perceived participation in childbirth (p = 0.042). Women who reported mobility during labor tended to experience higher childbirth experience scores (p = 0.005) and a greater frequency of vaginal births (p = 0.043), though these results should be interpreted cautiously due to the small sample size.
Conclusions:
This woman-centered antenatal intervention was feasible, acceptable, and conceptually promising. Preliminary findings indicate potential benefits for women’s satisfaction with decision making, beliefs about childbirth, and birth experience; however, no definitive conclusions can be drawn. A larger, adequately powered, multisite trial is warranted to confirm these trends and further evaluate the intervention’s effects.
Keywords
Introduction
A positive childbirth experience is a key aspiration for most women and is closely associated with active involvement in decision making and a sense of personal control.1,2 Perceived control during labor has been linked to improved maternal well-being, greater satisfaction, and favorable birth outcomes. Midwifery care that promotes mobility and the use of upright positions supports women’s autonomy and aligns with international guidelines, which recommend encouraging freedom of movement and the adoption of positions that women find comfortable during labor.1,3 These practices are associated with a shorter first stage of labor, fewer interventions, and reduced neonatal intensive care admissions. 4 However, despite this evidence, hospital-based maternity care often limits mobility by favoring supine or semi-recumbent positions. This misalignment between women’s preferences and institutional practices can erode women’s self-efficacy and compromise their birth experience.5–7
Antenatal education offers an important opportunity to prepare women for active participation in labor. Evidence shows that structured education can improve self-efficacy, informed decision making, and confidence while also enhancing maternal and neonatal outcomes.8,9 Beyond the acquisition of physiological knowledge, antenatal education should also promote psychological readiness, reinforce women’s sense of agency, and build communication and decision-making skills.10,11 Empowering women to remain mobile and choose upright positions during labor requires more than encouragement from professionals; it demands preparation, self-trust, and the ability to navigate care contexts where institutional routines may conflict with evidence-based recommendations. Interventions that specifically aim to strengthen women’s autonomy in these decisions are still scarce.12,13 To address this gap, a woman-centered antenatal intervention was developed by the authors, following the UK Medical Research Council Framework for complex interventions.14,15 Designed for integration into childbirth preparation programmes in community settings, this intervention aims to support active labor and informed decision making regarding mobility and positioning. This article reports on a feasibility study that evaluates the preliminary effects of this women-centered intervention on decision making, decision satisfaction, childbirth self-efficacy, and birth experience. It also examines the feasibility of implementing and evaluating the intervention in a larger-scale trial.
Materials and Methods
Study design
This feasibility study used a preexperimental, pre and posttest quantitative design with three data collection time points. It aimed to assess the feasibility and acceptability of a woman-centered antenatal intervention and to explore its preliminary effects on birth beliefs, decision making, childbirth self-efficacy, and birth experience. Ethical approval was obtained from the Ethics Committee of the Central Regional Health Administration (CE ARSC/No. 52/2023). The study is reported in accordance with the CONSORT 2010 extension for pilot and feasibility trials. 16
Intervention protocol
I choose to move during my labor is a woman-centered, group-based antenatal program designed to empower pregnant women who plan a vaginal birth. The intervention aims to enhance women’s knowledge, skills, and confidence to make informed decisions about mobility and upright positioning during labor, thereby promoting autonomy and engagement in the childbirth experience. Grounded in the Theory of Emancipated Decision-Making in Women’s Health Care and Bandura’s Self-Efficacy Theory, the program integrates four core components: (1) structured group interaction; (2) experiential learning through hands-on practice of mobility and upright positions; (3) decision-making support using reflective prompts and the BRAIN model (Benefits, Risks, Alternatives, Intuition, Nothing); and (4) a supportive environment fostered through positive and respectful communication.
The program consisted of two sequential 2.5-hour sessions delivered face to face in community settings by experienced nurse-midwives: Session 1 (Moving during labor: my superpower!) focused on body awareness, experiential practice of positions (including feasible in-bed adaptations), relaxation and mindfulness, and group reflection; Session 2 (I choose to move during labor!) centered on decision-making skills using hypothetical labor scenarios and rehearsal with the BRAIN framework to align choices with personal values. Birth partners were invited to participate in both sessions.
What distinguishes this program from standard antenatal classes is its explicit focus on decision-making autonomy about mobility and upright positions, its use of shared decision-making tools to navigate institutional routines, and its integration of hands-on rehearsal and communication micro skills to support women’s agency during labor. A comprehensive description of the intervention’s theoretical underpinnings, development, and implementation is available in a separate publication currently under peer review. Table 1 summarizes the overall structure and key components.
Summary of the Structure and Content of the Intervention “I Choose to Move during my Labor”

Participants and recruitment
Participants were recruited from four community care units (CCUs) in Portugal offering childbirth preparation programmes. A purposive sampling strategy was used to identify eligible women who met the following inclusion criteria: age ≥18 years, low-risk pregnancy, nulliparity, and ability to communicate in Portuguese. For analytical purposes in this feasibility study, only those participants who completed both sessions and experienced an uncomplicated birth of a healthy, term newborn without postpartum complications were included in the final analysis. Exclusion criteria were Edinburgh Postnatal Depression Scale (EPDS) score ≥12 at baseline, planned elective cesarean section, or occurrence of postpartum complications.
The sample size was determined according to methodological guidance for feasibility studies, which recommend enrolling sufficient participants to assess feasibility outcomes and to estimate preliminary effect sizes for future trials. 17 A minimum target of 45 participants was established to account for an anticipated 30% attrition rate, based on previous studies of antenatal education reporting similar dropout rates.18,19 This target was set to ensure that at least 30 women would complete postintervention assessments. 16
The intervention was embedded in the routine childbirth preparation programs delivered by each CCU and was co-facilitated by the principal investigator and the local nurse-midwife. To preserve group dynamics and minimize disruption, the intervention was implemented within existing community-based groups. Women who did not meet the inclusion criteria or declined participation were still welcome to attend the sessions. A total of eight intervention groups were delivered across the four CCUs, resulting in 16 sessions conducted between November 2024 and February 2025.
Data collection
Data were collected at three time points using structured, self-administered online questionnaires. Informed consent was obtained electronically before participation. At baseline (T1), participants completed six instruments: a sociodemographic and obstetric questionnaire; the Portuguese versions of the Birth Beliefs Scale (BBS-pt) and the Revised Emancipated Decision-Making in Childbirth Scale (EDMr-pt), both cross-cultural adapted and psychometrically validated by the authors following international guidelines for cross-cultural adaptation (validation studies currently under peer review); the EPDS; the Childbirth Self-Efficacy Inventory (CBSEI-pt) 20 ; and the Satisfaction with Decision Scale (SWD-pt). 21
At posttest (T2), four instruments were completed: BBS-pt, CBSEI-pt, EDMr-pt, and SWD-pt. After childbirth (T3), women who had term, complication-free births completed two additional instruments: a short birth outcomes questionnaire and the Portuguese version of the Childbirth Experience Questionnaire (CEQ-pt). 22
Data analysis
Data analysis was performed using IBM SPSS Statistics, version 28. Descriptive statistics were calculated for all study variables. Categorical variables were summarized using frequencies and percentages, while continuous variables were described using measures of central tendency (mean, median) and dispersion (standard deviation, minimum, and maximum). Normality of continuous variables was assessed using the Shapiro–Wilk test. For paired comparisons between pre- and postintervention scores (T1 and T2), paired-samples t-tests were used when normality assumptions were met; otherwise, the Wilcoxon signed-rank test was applied. Difference scores (T2 − T1) were computed and tested for normality to guide the selection of appropriate tests. Bivariate associations between predictor variables and birth experience outcomes (T2 − T3) were examined using Spearman’s rank-order correlation coefficients. Although some variables were normally distributed, the presence of nonnormal distributions in several key variables justified the systematic use of nonparametric tests to ensure consistency. 23 Multiple linear regression analyses were conducted to explore the predictive value of emancipated decision making, decision satisfaction, childbirth self-efficacy, and natural birth beliefs on childbirth experience outcomes. Assumptions of linear regression were verified through residual analysis, and multicollinearity was assessed using variance inflation factors (VIFs).
Given the exploratory nature of this feasibility study, a significance level of p ≤ 0.05 was adopted for all inferential tests. 16 Preliminary sample size estimates for future trials were calculated based on effect sizes observed in this sample. Both post hoc power analyses and a priori sample size estimations were conducted using the observed effect sizes and standard guidance for feasibility studies. 17
Results
A total of 84 women attended the intervention sessions. Of these, 58 met the inclusion criteria and were invited to participate in the study. Two women declined participation, resulting in 56 participants completing the baseline assessment (T1). At postintervention assessment (T2), 38 participants completed the questionnaires, corresponding to an attrition rate of 32.1%. The main reasons for attrition were nonresponse to follow-up assessments and failure to attend both intervention sessions. In addition, five women scored ≥12 on the EPDS at T1. These participants were referred to their respective nurse-midwives for follow-up care and were allowed to continue attending the sessions, but their data were excluded from the analyses, in line with the exclusion criteria. At postpartum follow-up (T3), valid data were obtained from 30 participants. Three women were excluded due to elective cesarean birth or neonatal admission to the intensive care unit, and five did not respond at this stage. Figure 1 shows the flow of participants through the study.
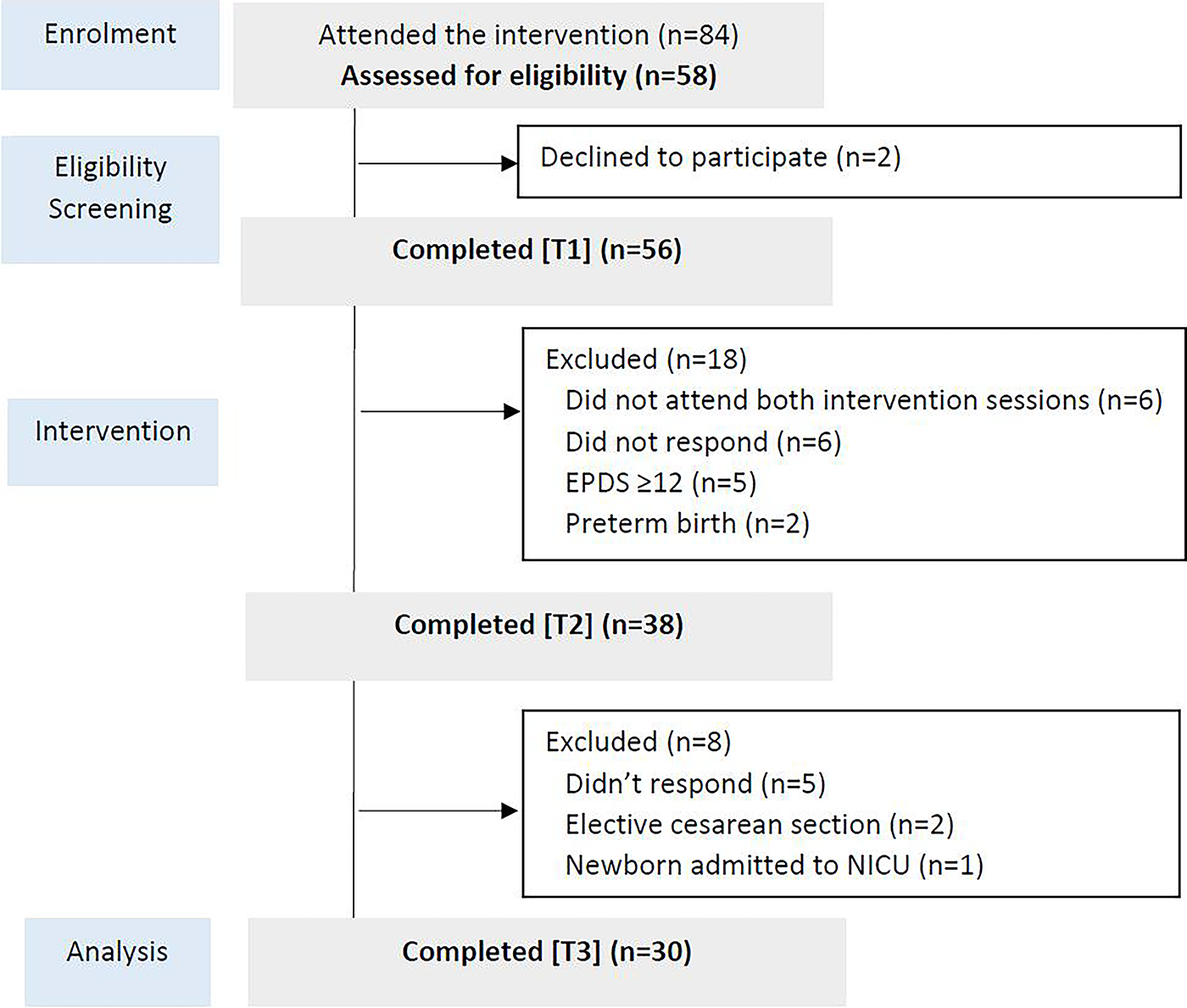
Flow diagram of participants in the feasibility study, from recruitment to postpartum follow-up.
Participants’ characteristics
The analysis of preliminary effects included 38 participants who completed data collection at both baseline (T1) and postintervention (T2). The mean age was 31.97 years (SD = 5.03), ranging from 24 to 41. At baseline, the mean gestational age was 32.3 weeks (SD = 2.65), and at T2, it was 36.5 weeks (SD = 1.41). Most participants were Portuguese (n = 33, 86.8%), held a higher education degree (n = 24, 63.2%), were employed (n = 33, 86.9%), and living with a partner (n = 35, 92.1%). Participants’ perceived partner involvement in pregnancy-related matters had a mean score of 8.92 (SD = 1.44), and perceived knowledge about mobility during labor was 6.21 (SD = 2.40), on a 10-point scale. At baseline, emotional well-being was assessed using the EPDS, with a mean score of 5.79 (SD = 2.87; range = 0–11). Table 2 summarizes the sociodemographic and obstetric characteristics of the final sample (n = 38).
Sociodemographic and Obstetric Characteristics of the Participants (n = 38)

EPDS, Edinburgh Postnatal Depression Scale; SD, standard deviation.
Internal consistency of the instruments
Internal consistency of the instruments and subscales was assessed using Cronbach’s α at each data collection point (T1, T2, and T3). Overall, the instruments demonstrated acceptable to excellent reliability. At T1, α values ranged from 0.525 (BBS-Natural) to 0.974 (CBSEI-pt Efficacy-Total). The BBS-pt showed lower internal consistency in the Natural subscale at both T1 (0.525) and T2 (0.554), while the Medical subscale demonstrated acceptable reliability (T1 = 0.712; T2 = 0.766). At T2, most instruments maintained good to high reliability, with some subscales improving. For example, the EDMr-pt subscale Sense of Pressure increased from 0.704 to 0.826, and Negative Reactions remained stable (T1 = 0.749; T2 = 0.753). In contrast, decreases were observed in the EDMr-pt subscales Feeling Supported (from 0.792 to 0.605) and Feeling Respected (from 0.778 to 0.535). The total EDMr-pt score also showed a slight reduction (from 0.852 at T1 to 0.774 at T2). At T3, CEQ-pt demonstrated excellent overall reliability (0.909), with high internal consistency across most subscales. However, the Own Threshold subscale showed limited consistency (0.439). Detailed Cronbach’s α coefficients for all scales and subscales are provided in Supplementary Table S1.
Preliminary effects of the intervention
To assess the preliminary effects of the intervention on emancipated decision making, satisfaction with decision making, childbirth self-efficacy, and childbirth beliefs, difference scores (T2 − T1) were analyzed. Normality of the difference scores was tested using the Shapiro–Wilk test. Assumptions of normality were met for the decision making, satisfaction, and self-efficacy variables (p > 0.05). For childbirth beliefs, the BBS-Natural subscale violated the normality assumption (p = 0.004), while the BBS-Medical subscale did not (p = 0.126).
Paired-samples t-tests revealed no statistically significant changes in emancipated decision making or childbirth self-efficacy from T1 to T2. Although mean scores increased slightly, the differences were not significant, EDMr-pt: t(37) = −0.637, p = 0.528, d = 0.10; CBSEI-pt Efficacy: t(37) = −0.854, p = 0.399, d = 0.14. In contrast, satisfaction with decision improved significantly, SWD-pt: t(37) = −3.675, p < 0.001, with a moderate effect size (d = 0.60). For birth beliefs, the Wilcoxon signed-rank test indicated a significant increase in natural birth beliefs (Z = 3.764, p < 0.001), with a large effect size (r = 0.61). Beliefs about birth as a medical event decreased significantly, BBS-Medical: t(37) = 2.229, p = 0.032, with a small-to-moderate effect size (d = 0.36).
Table 3 summarizes descriptive statistics and effect sizes. Effect sizes for nonparametric tests were calculated as r = Z/√N, 23 with interpretation based on Cohen’s criteria (small = 0.10; medium = 0.30; large = 0.50). 24
Changes in Decision Making, Satisfaction, Self-Efficacy, and Birth Beliefs from Pre- to Postintervention (n = 38)

Δ Mean = T2 − T1. Effect sizes interpreted according to Cohen’s thresholds: small = 0.10; medium = 0.30; large = 0.50.
Labor and birth-related characteristics (T3)
At the time of labor, the mean gestational age was 39.4 weeks (SD = 1.10; range = 37–41). Spontaneous onset of labor occurred in 19 women (63.3%), while 11 (36.7%) underwent induction. The mean cervical dilation at admission to the birth room was 3.57 cm (SD = 2.05), increasing to 4.72 cm (SD = 1.73) at the time of epidural analgesia administration. Most participants (n = 27; 90.0%) reported being able to move during the dilatation phase of labor in the hospital setting. Among them, 14 women (51.9%) were mobile in the labor ward, 12 (44.4%) in the birth room, and 1 woman (3.7%) in both settings. Epidural analgesia was administered to 29 participants (96.7%) following their informed choice, while one participant chose not to receive it. The mean cervical dilatation at the time of epidural initiation was 4.72 cm (range = 1–8). Although most women reported being able to move, over half (52%) experienced reduced mobility after transfer to the birth room. Regarding mode of birth, 15 women (50.0%) had a spontaneous vaginal birth, 10 (33.3%) had an instrumental vaginal birth, and 5 (16.7%) had a cesarean section. Among those with vaginal births (n = 25), the mean duration of the dilation phase was 8.72 hours (SD = 5.49), and the expulsion phase lasted an average of 63.20 minutes (SD = 48.28). Episiotomy was performed in 14 cases (56.0%).
Although not a direct measure of satisfaction, the likelihood of recommending the intervention was high, with an average rating of 9.73 (SD = 0.74; range = 7–10), indicating a positive perception of the intervention experience. Table 4 presents detailed labor and birth-related characteristics.
Labor and Birth-Related Characteristics at T3 (Postpartum Follow-Up, n = 30)

Data available for n = 25 vaginal births.
Associations between childbirth experience and predictor variables
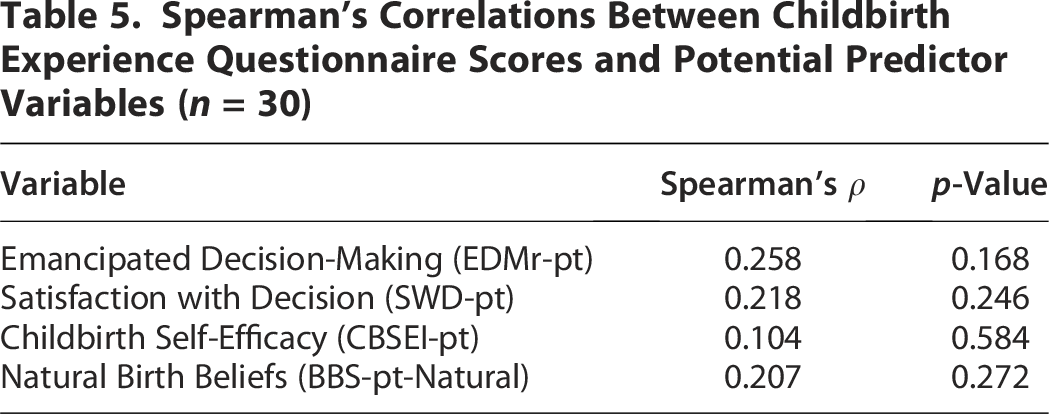
Spearman’s rank-order correlations were conducted to explore associations between women’s reported childbirth experience (measured by the CEQ-pt at T3) and selected variables measured after the intervention (T2), considered as potential predictors. These included emancipated decision making, satisfaction with decision making, childbirth self-efficacy, and natural birth beliefs. No significant correlations were observed. Although higher scores in all four variables tended to be associated with more positive childbirth experiences, the associations were weak and did not reach statistical significance (Table 5).
Spearman’s Correlations Between Childbirth Experience Questionnaire Scores and Potential Predictor Variables (n = 30)
Prediction of overall childbirth experience
A multiple linear regression model was tested to assess whether the four variables measured at T2 predicted overall childbirth experience at T3 (CEQ-pt total score). The model was not statistically significant, F(4, 25) = 0.865, p = 0.498, explaining 12.2% of the variance (R2 = 0.122, adjusted R2 = −0.019). None of the predictors reached statistical significance. Multicollinearity diagnostics indicated no concerns (all VIF <2.5) (Table 6).
Multiple Linear Regression Model Predicting Childbirth Experience Questionnaire Scores (n = 30)

Model summary: R2 = 0.122, adjusted R2 = –0.019, F(4, 25) = 0.865, p = 0.498. VIF, variance inflation factor.
Associations with specific dimensions of childbirth experience
To explore associations with specific aspects of women’s childbirth experiences, Spearman’s rank-order correlations were performed between T2 predictor variables and each CEQ-pt subscale. A significant positive correlation was found between natural birth beliefs and the CEQ Participation subscale (ρ = 0.373, p = 0.042). No other statistically significant associations were observed (Supplementary Table S2).
Prediction of CEQ subscales
Four multiple linear regression models were tested to determine whether T2 variables predicted each CEQ-pt subscale. None of the models was statistically significant. For the CEQ Participation subscale, natural birth beliefs emerged as the strongest predictor, approaching statistical significance (β = 0.447, p = 0.062). All other predictors were nonsignificant across subscales (Supplementary Table S3).
Associations between mobility during labor and birth outcomes
Analyses were conducted according to the nature of each outcome. For the duration of labor phases (dilation and expulsion), comparisons were limited to women who had vaginal births (spontaneous or instrumental). All other comparisons (type of birth, use and timing of epidural analgesia, and childbirth experience) included the full postpartum sample (n = 30).
Given the nonnormal distribution of most variables, nonparametric tests were used. Mann–Whitney U tests revealed no significant differences in the duration of the dilation phase (U = 3.50, p = 0.234) or the expulsion phase (U = 9.50, p = 0.726) between women who were mobile during labor and those who were not. Although the use of epidural analgesia did not differ significantly between groups (Fisher’s exact test, p = 1.000), a trend toward later administration was observed in the mobility group, with higher cervical dilation at the time of epidural (U = 12.50, p = 0.056). A significant association was observed between mobility during labor and type of birth, χ2(2) = 6.296, p = 0.043, with vaginal births being more frequent among women who reported mobility. These results should be interpreted with caution due to the small size of the nonmobility group (n = 3). Childbirth experience scores were significantly higher among women who moved during labor compared with those who did not. Significant group differences were found for the CEQ total score (U = 4.00, p = 0.005), as well as for the subscales Own Performance (U = 6.50, p = 0.011), Participation (U = 6.50, p = 0.011), and Professional Support (U = 7.00, p = 0.015). No significant difference was observed for the Own Threshold subscale (U = 16.00, p = 0.100) (Table 7).
Comparison of Obstetric and Childbirth Experience Outcomes by Mobility During Labor

Analyses restricted to women who had vaginal births (n = 25).
CEQ, Childbirth Experience Questionnaire; CS, cesarean section; IV, instrumental vaginal; IQR, interquartile range; SV, spontaneous vaginal.
Associations between satisfaction with the intervention, mode of birth, and childbirth experience
The association between participants’ satisfaction with the intervention and their childbirth experience was examined using Pearson’s or Spearman’s correlation coefficients, depending on the distribution of each CEQ-pt subscale. Significant positive associations were observed for the overall CEQ score (r = 0.444, p = 0.014), the Own Performance subscale (r = 0.469, p = 0.009), and the Professional Support subscale (ρ = 0.376, p = 0.041). No significant correlations were found for the Participation or Own Threshold subscales. Mode of birth (vaginal vs. cesarean section) was also examined in relation to childbirth experience. A statistically significant difference was found for the CEQ Professional Support subscale, with higher scores among women who had a vaginal birth (U = 26.50, p = 0.041). No significant differences were observed for the other subscales or for the total CEQ score. However, moderate effect sizes were identified for CEQ-pt total (d = 0.43), Own Threshold (d = 0.54), and Own Performance (d = 0.65), suggesting clinically meaningful trends that may not have reached statistical significance due to the small number of participants in the cesarean group (n = 5). Full results are available in Supplementary Table S4.
Post hoc power and sample size estimation
Post hoc and a priori power analyses were conducted for key outcome variables based on the effect sizes observed in this feasibility sample (n = 30). The analyses revealed that statistical power was limited for most outcomes. For instance, observed power was 31.9% for the overall childbirth experience (CEQ-pt) and 61.5% for the Participation subscale. For other variables, observed power ranged from 16.3% to 28.3%. To achieve 80% power in future studies, estimated total sample sizes would range from 76 to 402 participants, depending on the outcome and effect sizes observed in this study, calculated using standard methods. 25 Full details are provided in Supplementary Table S5.
Discussion
This feasibility study aimed to explore the preliminary effects of a woman-centered antenatal intervention designed to promote mobility and upright positions during labor, with particular emphasis on decision making. The three-phase longitudinal design enabled not only the evaluation of changes in decision making, birth beliefs, and self-efficacy but also the assessment of instrument performance over time. Most instruments demonstrated acceptable to excellent internal consistency. The CEQ-pt showed high reliability overall, but the Own Threshold subscale presented limited internal consistency (α = 0.439). This is consistent with findings from the Portuguese validation study, 22 suggesting that this subscale may capture a more heterogeneous or context-sensitive construct. Own Threshold reflects perceived vulnerability during labor, often shaped by fear, exhaustion, pain, lack of control, and environmental discomforts, which may vary considerably between women and be difficult to capture with only a few items. Thus, the lower alpha is likely related to the inherent variability of these experiences, rather than to a psychometric flaw in the subscale itself. Regarding the EDMr-pt, internal consistency was generally stable or improved. The Sense of Pressure subscale increased from α = 0.704 to α = 0.826, possibly indicating greater clarity or shared understanding of social norms following the intervention. In contrast, a decline was observed in the Feeling Supported and Feeling Respected subscales at T2. This may be explained by the relatively small sample or by increased variability in responses due to heightened awareness of care quality. Exposure to the intervention may have encouraged more critical appraisal of clinical interactions, leading to more diverse interpretations and reduced internal consistency. These findings underscore the importance of monitoring not only mean scores but also internal reliability across time points, particularly when interventions are expected to influence women’s perceptions, expectations, or critical engagement with maternity care.
Preliminary effects of the intervention
The intervention led to a statistically significant increase in satisfaction with decision making, while only small, nonsignificant improvements were observed in emancipated decision making and self-efficacy scores at T2. Several factors may explain this pattern. Satisfaction with decision making reflects women’s confidence in their choices at the moment they are made, before the consequences are known. This construct is associated with behavioral intention and is considered a relevant predictor of health outcomes. 26 In contrast, emancipated decision making involves a deeper sense of agency, ownership, and control, shaped by the broader sociocultural and organizational context of childbirth care. 11 It is likely that a short antenatal program, even when focused on experiential learning and decision-making support, is insufficient to activate structural empowerment processes. The intervention consisted of two sessions and was embedded in community antenatal education. Although it incorporated key components such as group interaction and positive communication, the development of emancipated decision making may require longer exposure, repeated practice, and reinforcement across the perinatal continuum. As noted by Watkins et al., 27 systemic barriers such as limited access to woman-centered care, risk-averse institutional norms, and inadequate provider communication continue to constrain women’s autonomy in maternity care. These structural constraints are often compounded by assumptions about women’s capacities during labor, including the presumption of vulnerability or incapacity to participate actively in decision making. 28 Such assumptions may lead to disempowering practices and reduce responsiveness to women’s preferences, even when well prepared during the antenatal period. Furthermore, there may be a mismatch between what women learn during childbirth preparation and what they encounter during labor. Sutcliffe et al. 29 highlight how hospital routines and provider behaviors may hinder the application of techniques taught in antenatal programmes, leading to frustration or reduced confidence. This incongruence may help explain why satisfaction with decision making improved, possibly due to increased clarity and preparedness, but deeper changes in emancipatory processes were not yet evident. These findings suggest that while decision satisfaction may respond to brief educational interventions, fostering emancipated decision making likely requires broader changes in care models, provider attitudes, and institutional practices to enable women’s full participation in labor and birth.
No statistically significant changes were observed in childbirth self-efficacy scores between pre- and postintervention assessments. While this finding contrasts with several studies reporting positive effects of antenatal education on self-efficacy,8,30–32 several factors may account for this result. One possibility is a ceiling effect, as participants already reported relatively high levels of self-efficacy at baseline. Consistent with existing evidence, self-efficacy has been positively associated with higher educational attainment, engagement in antenatal programmes, and access to information. 33 In this sample of nulliparous women, limited prior birth experience and potential social desirability bias may have contributed to inflated baseline scores, reducing the likelihood of detecting meaningful postintervention improvements. Additionally, previous research suggests that small-group antenatal education may increase women’s confidence in managing early labor and navigating the birth process, but may have limited impact on their confidence in shaping birth into a positive experience. 34 Childbirth self-efficacy is a multidimensional and dynamic construct, encompassing domains such as pain management, emotional regulation, and communication with health care professionals. These domains are shaped not only by antenatal preparation but also by the nature and quality of intrapartum support. As such, gains in self-efficacy may be context-sensitive and may manifest during labor, in behaviural responses, or retrospectively in women’s appraisals, rather than being fully captured by antenatal self-report measures.
In contrast, the intervention was associated with significant changes in birth beliefs. Women reported stronger beliefs in childbirth as a natural and physiological process and weaker beliefs in birth as a medical event. These findings align with those of Sucu et al., 35 who also reported enhanced natural birth beliefs following antenatal education. Shifts in birth beliefs are particularly meaningful, as previous research has highlighted their influence on women’s preferences, decision making, and birth experiences. Preis et al. 36 demonstrated that natural birth beliefs are associated with a preference for low-intervention options, while medicalized beliefs are linked to a greater preference for technological or interventionist care. Furthermore, preferences have been shown to mediate the relationship between beliefs and actual birth outcomes, although this effect may be diminished in highly medicalized systems, where access to physiological birth options often requires active negotiation by women. Vogels-Broeke et al. 37 further identified key factors shaping birth beliefs, including sociodemographic, psychological, and care-related characteristics. Stronger natural birth beliefs have been associated with higher educational levels, previous positive birth experiences, and participation in antenatal education. In contrast, medicalized beliefs have been linked to older maternal age, elevated anxiety or depressive symptoms, and predominant care by obstetricians. These findings suggest that addressing birth beliefs in antenatal education may be an effective strategy to enhance women’s agency and autonomy, particularly in maternity care systems where medicalized models of birth prevail.
Associations with childbirth experience
No significant associations were observed between emancipated decision making, satisfaction with decision, childbirth self-efficacy, or natural birth beliefs and women’s overall childbirth experience. These findings suggest that, within this sample, psychological variables assessed during late pregnancy were not direct predictors of women’s postnatal evaluations of their birth experience. However, analysis of individual subscales revealed that stronger beliefs in childbirth as a natural process were significantly associated with greater perceived participation during labor. This is consistent with previous research indicating that women who endorse natural birth beliefs may feel more empowered to engage actively in decision making during labor.36,38 A similar, although nonsignificant, trend was noted between natural birth beliefs and the CEQ Own Performance subscale, suggesting a possible link with women’s perceived coping and competence during childbirth. These results are particularly relevant given that the Participation and Own Performance dimensions were directly aligned with the aims of the intervention. The Participation domain reflects women’s sense of agency and involvement during labor. The intervention actively promoted this through decision-making support, the encouragement of mobility and upright positions as informed choices, and the use of decision-making scenarios. By increasing awareness of options and fostering confidence to act on them, the intervention may have enhanced women’s perception of being active participants in their care. Similarly, the Own Performance dimension relates to women’s retrospective assessment of their ability to manage the challenges of labor. The intervention’s experiential components, such as bodily rehearsal of positions and active movement strategies, may have contributed to an increased sense of competence and preparedness, ultimately enhancing self-perceived performance. Positive self-assessment in this domain is associated with greater confidence and empowerment, even when labor presents difficulties. 22
In contrast, emancipated decision making, satisfaction with decision, and self-efficacy did not demonstrate direct associations with childbirth experience. This may reflect the complex and multifactorial nature of birth experience, which is shaped by a combination of individual, interpersonal, and clinical factors, including expectations, perceived control, quality of intrapartum care, type of delivery, and neonatal outcomes. 39 As McKelvin et al. 40 emphasize, birth experience is influenced by both salutogenic and pathogenic factors, and the relationship between antenatal psychological constructs and postnatal outcomes may be indirect, potentially moderated or mediated by intrapartum care experiences. Nonetheless, these findings underscore the potential value of targeting modifiable beliefs during childbirth preparation. Promoting natural birth beliefs may offer a feasible pathway to enhance women’s engagement and sense of participation during labor, even within medicalized care environments.
Associations between mobility and birth outcomes
The majority of women in this sample reported being able to move during labor while in hospital. However, over half (52%) were unable to continue moving once transferred to the birth room, a reduction that appeared to coincide with the initiation of epidural analgesia or continuous fetal monitoring. This finding is consistent with previous studies,6,7,41,42 highlighting how institutional routines and clinical practices may restrict women’s mobility during labor.
Women who remained mobile during labor were significantly more likely to have a vaginal birth compared with those who did not. This supports earlier evidence suggesting that mobility may reduce the likelihood of cesarean section. 4 However, no significant differences were observed in the duration of either the dilation or expulsion phases between women with and without mobility. While some studies have reported shorter labor durations associated with upright positions, 4 more recent meta-analyses have shown inconsistent results, particularly among women receiving epidural analgesia. Inconsistencies in how mobility is defined and operationalized across studies may contribute to these mixed findings. 43
A nonsignificant trend toward later administration of epidural analgesia was noted among women who remained mobile. This aligns with the rationale of mobility-promoting strategies, such as the Labor Hopscotch Framework, which aim to encourage activity and delay early epidural use to support physiological progression. 12 Although modern epidural techniques may have a reduced impact on birth outcomes, 44 some evidence suggests that delayed epidural administration, after at least 3 cm of cervical dilation, may be associated with more favorable labor progression. 45
Importantly, mobility was significantly associated with more positive birth experiences. Women who remained mobile reported higher scores for overall childbirth experience, as well as for the Own Performance, Participation, and Professional Support subscales. These results echo prior findings suggesting that freedom of movement and upright positions may enhance women’s sense of control, autonomy, and active involvement in labor.2,7,12 These experiential and relational dimensions were explicitly targeted by the intervention, which included practical training in movement strategies and structured decision-making scenarios to foster preparedness and autonomy. In addition, women who reported higher satisfaction with the intervention also reported more positive birth experiences, particularly in terms of self-assessed performance and perceived professional support. This suggests that the intervention may have contributed not only to increased informational readiness but also to improved interactions with health care professionals. The group-based format, experiential learning, and supportive discussions may have reinforced both confidence and expectations for collaborative care. 46 Such expectations, shaped during childbirth preparation, may have influenced women’s perceptions of intrapartum care quality. Women who gave birth vaginally reported significantly higher perceived professional support compared with those who underwent cesarean section. This is consistent with previous studies suggesting that although clinical outcomes influence birth satisfaction, perceptions of autonomy, involvement in decision making, and the quality of professional support are particularly influential, and often more pronounced, in vaginal births.47,48
The findings from this feasibility study provide preliminary evidence supporting the integration of woman-centered interventions into antenatal education. The intervention, which incorporated experiential learning, decision-making scenarios, and communication strategies, was associated with improvements in birth beliefs and decision satisfaction. Although some effects did not reach statistical significance, likely due to limited sample size and reduced statistical power, these trends suggest that such interventions may contribute to more positive and empowering birth experiences. The intervention’s impact on women’s beliefs about childbirth, particularly the shift toward perceiving labor as a natural process, is a noteworthy outcome. In addition, the significant associations between mobility and more favorable birth experiences support the relevance of promoting movement and upright positions during labor.
To complement the quantitative findings, a qualitative component was conducted and will be reported separately. The qualitative data are expected to provide further insight into women’s subjective experiences, the perceived value of the intervention, and the contextual factors that may have influenced their capacity for emancipated decision making during labor. This study also assessed the feasibility of conducting a larger trial. Recruitment in a community-based setting was successful, and participants responded positively to data collection procedures. Retention rates were acceptable for a feasibility study, with 65.5% at postintervention and 52.7% at postbirth follow-up. These results indicate the need to strengthen follow-up strategies in future trials, such as offering flexible contact methods or integrating follow-up into routine postnatal appointments. The acceptability of the measures was also supported, with no major issues reported regarding instrument completion or understanding. The current results can inform future sample size calculations and methodological refinements. Larger, adequately powered trials will allow for subgroup analyses to examine whether intervention effects vary by sociodemographic, clinical, or psychological characteristics. Longitudinal designs could also explore the sustainability of intervention effects, including their impact on maternal mental health, satisfaction with care, and retrospective evaluations of the birth experience.
Based on recruitment and retention rates observed in this feasibility study (overall T1–T3 retention 53%), achieving approximately 400 analyzable participants would require enrolling around 750 women. Given the current recruitment rate (an average of about 2 analyzable participants per site per month across four CCUs), such a sample would be feasible within 18–24 months by expanding to approximately 9–12 participating sites. This scaling appears realistic, provided that enhanced follow-up procedures, flexible session scheduling, and standardized training for intervention delivery are implemented to support participant adherence and data completeness.
Strengths and limitations
This study has several limitations. First, the small sample size limited the ability to detect small-to-moderate effects, particularly in multivariate analyses. As this was a feasibility study, not designed to test efficacy, post hoc power analyses confirmed that larger samples will be required in future confirmatory trials. Second, the sample comprised nulliparous women with low-risk pregnancies recruited from community care settings, which may limit generalizability to broader obstetric populations and more medicalized care models. Third, the high educational level of participants may have influenced psychological variables, including childbirth self-efficacy, potentially reducing the intervention’s observable impact. Fourth, although validated Portuguese instruments were used, some subscales, particularly in the EDMr-pt and CEQ-pt, showed lower internal consistency at specific time points, raising concerns about the measurement precision of constructs. Fifth, outcomes such as decision satisfaction and childbirth experience were self-reported and may be subject to recall or social desirability bias, especially when measured postnatally. Sixth, while the inclusion of a control group is not mandatory in feasibility studies, the absence of a comparison group in this study prevents causal inferences regarding the effects of the intervention. The observed changes may reflect the combined influence of the intervention, routine antenatal care, or other contextual factors. Last, because women gave birth in different hospital settings, some outcomes, particularly those related to mobility during labor and the childbirth experience, may have been influenced by institutional practices and the degree to which each facility supports movement and autonomy during labor. Although all participants received the same antenatal intervention, variations in intrapartum care routines, such as epidural protocols or monitoring policies, could have contributed to differences in outcomes. Future studies should consider collecting data on institutional characteristics or adopting a cluster design to better account for these contextual influences.
Despite these limitations, the study provides preliminary insights into the potential benefits of a woman-centered antenatal intervention focused on promoting mobility, enhancing decision-making autonomy, and strengthening women’s agency during labor. The findings offer a solid foundation for designing larger, adequately powered trials aimed at improving maternal autonomy and birth experience.
Conclusion
This feasibility study supports the acceptability and potential value of a structured, group-based, woman-centered antenatal intervention aimed at promoting mobility, upright positions, and emancipated decision making during labor. Preliminary findings suggest that the intervention may reinforce natural birth beliefs, increase satisfaction with decision making, and contribute to more positive perceptions of the birth experience, particularly when mobility is supported during labor. While no significant effects were found for emancipated decision making or self-efficacy, the direction of change was consistent with the intervention’s theoretical assumptions. These results should be interpreted as exploratory given the limited statistical power of this feasibility sample. Future research should evaluate this intervention in a larger, adequately powered, multisite trial to confirm its effects and explore subgroup variations. Based on current recruitment and retention rates, a study involving approximately 9–12 CCUs over 18–24 months appears feasible. Such work could clarify the intervention’s impact on women’s autonomy, confidence, and satisfaction with childbirth while informing scalable strategies for promoting active, woman-centered labor care.
Authors’ Contributions
M.I.L.: Conceptualization, methodology, investigation, data curation, formal analysis, validation, writing—original draft, and writing—review and editing. M.V.: Conceptualization, methodology, supervision, and writing—review and editing. A.C.: Conceptualization, methodology, formal analysis, validation, supervision, and writing—review and editing.
Footnotes
Acknowledgments
The authors gratefully acknowledge the nurse-midwives from the CCUs for their active engagement and valuable support during the implementation of the intervention. They are especially thankful to the women who generously contributed their time to complete the questionnaires and share their experiences. The authors also acknowledge the support of the Health Sciences Research Unit: Nursing (UICISA: E), hosted by the Nursing School of Coimbra (ESEnfC) and funded by the Foundation for Science and Technology.
Author Disclosure Statement
The authors declare no competing interests.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.