
Abstract
Background:
Since 2019, the coronavirus disease-19 pandemic and its consequences from restrictions to risks have impacted our lives in all aspects. Pregnant women are especially vulnerable to the changes that were implemented as a result of the shift in healthcare priorities and the medical and social implications of the lockdown.
Objectives:
This study aimed to assess the experience of giving birth during the pandemic, how this is affected by acquiring coronavirus disease-19 infection, and its effect on postnatal mood.
Design:
A cross-sectional study was conducted which involved 490 women who gave birth during the pandemic across the Hashemite Kingdom of Jordan.
Methods:
An electronic questionnaire was distributed among women experiencing childbirth during this period in Jordan by advertising it on social media platforms targeting pregnant women and mothers. The sample size was statistically determined to be representative of the population. Statistical analysis was performed using Statistical Package for the Social Sciences for Windows v.27.
Results:
The study demonstrated that getting infected with the virus throughout the pregnancy did not affect the childbirth experience with respect to the parameters measured, but other factors during the pandemic such as the type of hospital and mode of delivery did. Positive interaction with staff in the delivery suite was a major determinant of a positive birth experience. Women associated low mood post-delivery with giving birth in pandemic circumstances, and it affected first-time mothers more than multiparous women.
Conclusion:
Although the acquisition of coronavirus disease-19 infection did not have a significant impact on women’s childbirth experience, several pandemic-related factors did. Given the importance of a woman’s perception and evaluation of events surrounding her birth experience in determining her postnatal physical and psychological well-being, having to give birth during the pandemic circumstances, especially for first-time mothers, can have potentially detrimental consequences that may affect her health and reproductive choices in the future. The results of this study offer a better understanding of the effect of pandemic and lockdown circumstances on the perceived experience of mothers during childbirth and postnatally and factors that should be taken into consideration when planning healthcare provision to this population in future similar conditions.
Introduction
The coronavirus disease 2019 (COVID-19), a potentially life-threatening infection caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was initially documented in Wuhan, China, in December 2019 and thereafter caused a worldwide pandemic. 1
Pregnant women are vulnerable to several adverse outcomes related to acquiring COVID-19 infection during pregnancy. Publications including a diversity of methods showed that complications of infection in pregnancy most commonly involved preterm delivery,2 –4 in addition to low birth weight and caesarean section (C-section).5,6 In particular, during the earlier stages of the pandemic, several studies reported significantly high rates of caesarean delivery among infected women.7 –9 Less common adversities included maternal death, stillbirth, miscarriage, preeclampsia, foetal growth restriction, coagulopathy, and premature rupture of membranes. 10
However, the impact of the pandemic was far more widespread than perinatal complications. Other, more general effects of the pandemic and its related containment strategies on healthcare, societies, and the global economy have had a significant impact on maternal health. 11 Pregnant women and new mothers have unique mental and physical healthcare needs. 12 The full effect of pandemic-related healthcare challenges is context-specific and differs according to country-specific factors. Several restrictions were applied to the provision of obstetric care during this challenging time such as the rapid move from usual direct contact to remote healthcare services, restricted access for support people during labour, and decreased or absent postnatal support.11 –13 In Jordan, for example, the lockdown measures taken in the initial phase of the pandemic had a dramatic effect on antenatal care provision to the pregnant population, as the percentage of women not receiving any antenatal care rose from 4% to 59.53% (P < 0.001). 11
A number of studies both from Jordan and other parts of the world that have been carried out since the emergence of COVID-19 reveal that the mental, social, and physical well-being of pregnant women has been compromised by the circumstance changes induced by the pandemic, as detailed below. Especially in the first phase of the pandemic, hospitals’ strict contingency plans and restrictions meant that women were frequently isolated during labour and delivery. 14 The role of support during and after giving birth is well known; therefore, these restrictions may have impacted on obstetric outcomes such as increased caesarean section rates, as well as social and psychological well-being and decreased satisfaction rates among new mothers with regard to their childbirth experience. Rapid discharge policies further contributed to this effect. 15 A study of 90 pregnant women showed that confinement due to COVID-19 led to a significant decrease in the levels of physical activity (P < 0.01) as well as in health-related quality of life (P < 0.005). 16 Postnatally, in the United Kingdom, mothers experienced a burden of constant mothering, inadequacy of virtual contact, and grief over lost social opportunities. 17 A German study also revealed that giving birth alone led to higher rates of anxiety and post-traumatic stress syndrome and can result in negative consequences for mothers and their children. 18
One of the most alarming consequences of the pandemic is its psychological impact. Pregnant women are at increased risk of mental health issues.19,20 Understanding how the pandemic may have influenced this is of utmost importance. The lockdown impacted negatively on the psychosocial well-being of pregnant women in Jordan who experienced higher degrees of psychological stress and domestic violence. 21
A Jordanian study revealed that over one-third of pregnant women (36.7%) reported depressive symptoms during the pandemic, especially those of lower socioeconomic status and those with less understanding of COVID-19 infection. 22 Another study revealed that more than half of pregnant women were feeling anxiety (58.0%) and fear (59.0%). 23 This is comparable with data from other countries. For example, in China, 26%–29% of a sample of pregnant women in China were found to have higher depression rates. 24 Furthermore, 25.3% and 13.6% of Belgian pregnant women in a study carried out during the initial lockdown experienced clinically elevated levels of depression and anxiety, respectively. 25 Canadian data from April 2020 revealed that 37% and 57% had clinically significant symptoms of depression and anxiety, respectively. 26
This leads to the realization that modifiable factors that have played a role in the aforementioned outcomes should be identified. As previous studies have demonstrated, multiple factors have affected the well-being of pregnant women during the pandemic. From here arose the question of whether women’s childbirth experiences were also affected by the pandemic, whether directly by infection during pregnancy or indirectly by the altered surrounding circumstances.
Indeed, a negative interpretation of an adverse experience adds to the severity of mental health outcomes.27 –29 Particularly, cognitive appraisal (i.e. perceived negative impact) of natural disasters, rather than objective exposure, significantly affects pregnancy and childbirth outcomes.30 –32
In this study, Jordanian women’s childbirth experiences during the COVID-19 pandemic were assessed by adapting some items from the Questionnaire for Assessing Childbirth Experience (QACE) by Carquillat et al. 33 This questionnaire was developed as a screening instrument derived from items that have been found to empirically correlate with the childbirth experience in the form of a multidimensional questionnaire aiming to identify women with negative experiences. It can be used as a whole or by adapting some of its content.
Materials and methods
Study design and sample
This research involved a cross-sectional survey of 490 women who gave birth during the COVID-19 pandemic across the Hashemite Kingdom of Jordan. The sample size was statistically determined. According to the Jordanian Department of Statistics, the crude number of deliveries per year from 2020 was 186,087 deliveries. 34 This number was taken as an estimate of the number of pregnancies per year. Due to the limited previous information regarding the effect of the pandemic circumstances on various aspects of women’s birth experiences, it was assumed that women would be affected adversely with a frequency of 50%. To achieve a 95% confidence interval, with a margin of error of 5%, and a design effect of 1.0, the desired sample size was calculated to be 384. The survey link was closed once the number of completed responses exceeded this target.
The questionnaire was distributed through an electronic link. Data were collected from the participants over a week in March 2021 by sharing the online survey on social media platforms, especially motherhood groups on Facebook in Jordan.
The survey conforms to the Checklist for Reporting Results of Internet E-Surveys. 35
The study included women who gave birth during the COVID-19 pandemic in Jordan and agreed to provide a complete response to the study’s questionnaire. Exclusion criteria were any incompletely filled responses, women residing outside Jordan, and women who gave birth prior to or after the curfew period.
Study objective
This study aimed to assess the overall childbirth experience of women in Jordan who gave birth during the pandemic, how this was influenced by acquiring COVID-19 infection, and whether this affected maternal postnatal mood.
Study tool
The survey questionnaire was developed by adapting some of the items in the QACE developed by Carquillat et al. 33 It is a multidimensional tool designed to identify women with negative childbirth experiences. It was chosen as it takes a wholistic approach to evaluating the birth experience, rather than focusing merely on mood changes and postnatal depression. The developed questionnaire was validated for content by review by a group of specialists in the field; subsequently, it was translated into Arabic language and then back-translated to English language, and several questions related to participant demographics and social circumstances, COVID-19 infection status, and a subjective feeling of low mood were added to the original items. An electronic version was designed using Google Forms and was distributed via social media platforms.
Statistical analysis
Statistical analysis was performed using Statistical Package for the Social Sciences for Windows v.27. Frequencies and mean plus standard deviation were calculated for categorical and continuous variables, respectively.
To test the association between COVID-19-infected women categories and the tested variables, we used a t-test. Association between hospital type, mode of delivery, and tested variable was performed using one-way analysis of variance (ANOVA), and post hoc comparisons were calculated using the Bonferroni test.
In addition to the correlation between post-delivery depression and the COVID-19 pandemic, the chi-square test was used to test the correlation between COVID-19 infection, hospital type, delivery way, and first delivery and the tested variable post-delivery depression.
Finally, Pearson’s correlation was calculated to assess the association between the women’s age and the tested variable. Statistical significance was considered when the P value was < 0.05.
Results
Participants’ characteristics
In total, 490 women completed the questionnaire. The mean age of participants was 28.9 ± 4.3 years. Parity ranged from 1 to 4 with a mean of 1.94 ± 0.8. The participating women gave birth in hospitals from different health sectors in Jordan, with hospitals from the private sector being most frequently sought (58.8%). Notably, 50.0% of women had normal vaginal deliveries, closely followed by caesarean section, whether elective or urgent (45.7%). Notably, 9.4% of participants got infected with coronavirus during pregnancy. A total of 52.4% reported feeling down or depressed after delivery. For further study population characteristics, refer to Table 1.
Study population characteristics.

SD: standard deviation.
Impact of COVID-19 infection on delivery process
A total of 46 women were infected with COVID-19 during their last pregnancy (9.4%); however, none of them had complications related to the infection. We tested the relationship between being infected with COVID-19 during pregnancy and the women’s delivery experience, positive interaction with the medical staff, pain during delivery, fear of future delivery, satisfaction level regarding delivery during the COVID-19 pandemic, and what they perceived as an ideal delivery. The results shown in Table 2 show that getting infected during pregnancy did not affect any of the tested parameters significantly.
Impact of COVID-19 infection on delivery process.

Data are represented as mean ± standard deviation. All P values were calculated using an independent-sample t-test.
As shown in Table 3, acquiring COVID-19 did not significantly affect whether women reported feeling of low mood after delivery (P value = 0.786).
Association between COVID-19 infection and post-delivery depression.

Data are represented in n (%).
Mode of delivery during the pandemic
The delivery categories were normal vaginal delivery, forceps, vacuum, urgent caesarean section, and elective caesarean section.
Forceps as a mode of delivery was excluded since only one woman was delivered by this method. One-way ANOVA was performed to compare the mean of women’s responses in every category. The Bonferroni test was used for post hoc comparisons.
We tested the effect of mode of delivery on the women’s delivery experience, the interaction with the medical staff, the fear of future delivery, the satisfaction level regarding delivery during the COVID-19 pandemic, and the delivery circumstances perceived by them as ideal. The results are shown in Table 4.
Effect of mode of delivery on the process.

ANOVA: analysis of variance.
Data are represented as mean ± standard deviation. All P values were calculated using one-way ANOVA.
For delivery-related pain, post hoc comparisons revealed that women who had a spontaneous vaginal or vacuum delivery had experienced similar and significantly higher levels of pain than those who delivered by caesarean section. In addition, urgent caesarean section was related to significantly higher levels of pain than elective caesarean section (P value < 0.0001).
The post hoc analysis also showed that the women who underwent both types of caesarean sections were significantly less satisfied from giving birth during COVID-19 pandemic compared with other groups (P value = 0.002). However, women who delivered via elective caesarean section reported significantly higher levels of positive interaction with the medical staff compared with the other groups (P value = 0.044).
The results also demonstrate that normal vaginal delivery and elective caesarean section resulted in a more positive delivery experience compared with other types of deliveries (P value < 0.0001).
The analysis of perceived ideal delivery showed that women who had caesarean section reported that they perceived having a normal vaginal delivery as ideal, in contrast to women who had natural or vacuum delivery, who thought the ideal way to give birth is by caesarean section, implying that none considered their delivery circumstances to be ideal.
All participants apart from women who had elective caesarean section ideally would prefer to choose the obstetrician who performs the delivery.
Finally, women delivered via elective caesarean section did not consider being able to choose the delivery date an issue that makes for a more ideal delivery.
Table 5 demonstrates that there is no significant correlation between the mode of delivery and post-delivery self-reported feeling of low mood (P value = 0.060).
Effect of mode of delivery on post-delivery self-reported feeling of low mood.

Data are represented in n (%).
Type of the hospital
Hospitals in Jordan belong to four main health sectors, namely, teaching, private, military, and public hospitals. We tested the effect of the hospital type on the women’s delivery experience, the interaction with medical staff, fear of future delivery, satisfaction level regarding delivery during the COVID-19 pandemic, and what they perceived as an ideal delivery. The results are shown in Table 6.
Type of the hospital on the delivery experience.

ANOVA: analysis of variance.
Data are represented as mean ± standard deviation. All P values were calculated using one-way ANOVA.
The results showed that the type of the hospital has effects on women in the following aspects: fear of future delivery (post hoc), satisfaction level regarding giving birth during COVID-19(post hoc), positive interaction with the medical staff (post hoc), and delivery as positive experience (post hoc). Significant differences in the perceived ideal delivery were found only regarding being able to choose the specialist supervising the delivery.
Post hoc analysis shows that satisfaction levels regarding delivery during the COVID-19 pandemic were reported to be significantly higher among women who gave birth in private hospitals compared with public hospitals (P value = 0.006). Similarly, private hospitals together with teaching hospitals were associated with more positive interaction with the medical staff and with a positive delivery experience (P value < 0.0001).
Women who delivered in public hospitals were more likely to report that choosing the specialist was considered the most important factor for ideal delivery (P value < 0.0001).
The results showed no significant association between the hospital type and post-delivery self-reported feeling of low mood (Table 7) (P value = 0.521).
Effect of hospital type on post-delivery self-reported feeling of low mood.

Data are represented in n (%).
Results revealed that women after their first delivery had higher rates of post-delivery self-reported feeling of low mood than those who have had previous deliveries (Table 8) (P value = 0.002).
Association between first delivery and post-delivery self-reported feeling of low mood.

Data are represented in n (%).
Is postpartum depression COVID-19 related?
Women were asked whether feeling down after delivery was related to giving birth during the pandemic. The chi-square test was used to test the association between feeling down or depressed after delivery and having to give birth in pandemic circumstances. The results revealed that women who experienced those feelings connected it to giving birth during COVID-19 pandemic conditions (P value < 0.001). Table 9 summarizes the results.
Association between low mood after the delivery and delivery under the COVID-19 pandemic.
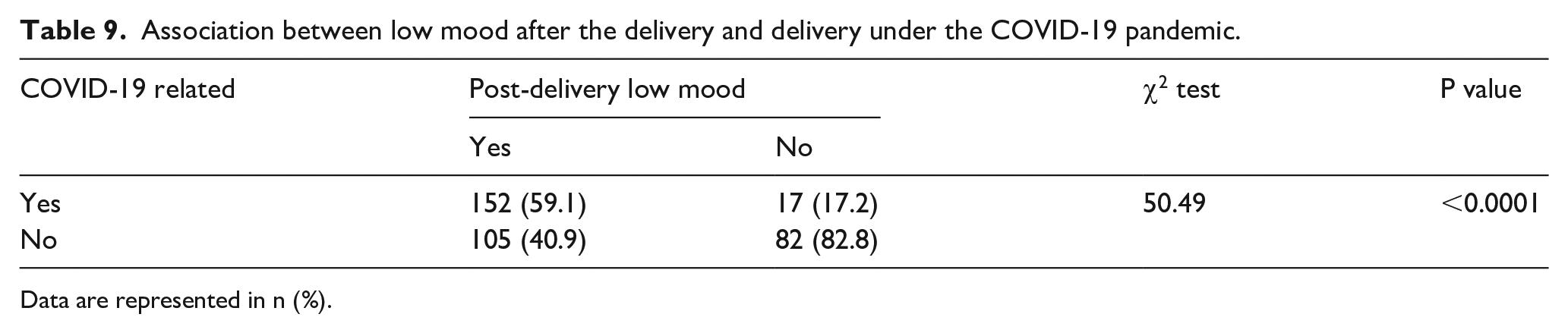
Data are represented in n (%).
Association between positive interaction with the medical staff and satisfaction from the process
A significant positive correlation was found between positive interaction with the medical staff and satisfaction regarding the delivery process. Women who had positive interaction with the medical staff reported higher levels of satisfaction from delivery under COVID-19 (P value < 0.001) (Table 10).
Correlation between interaction with medical staff and women satisfaction.

Discussion
This study was conducted during the COVID-19 pandemic in Jordan and aimed to assess the overall childbirth experience of women in Jordan who gave birth during the pandemic, how this was influenced by acquiring COVID-19 infection, and whether this affected maternal postnatal mood.
Our results showed that getting infected with coronavirus during pregnancy did not affect the experience of delivery, the satisfaction of the mother, or reported postpartum low mood. The infection rate among pregnant women in the study population was 9.4% with no COVID-19 complication. The fact that women who acquired infection in this study had an uncomplicated disease course may play a role in these findings.
Mode of delivery affected several aspects of the childbirth experience during the pandemic. Women who underwent caesarean section reported less pain related to delivery than normal vaginal delivery and instrumental delivery. Consistent with previous studies, our results demonstrated that normal vaginal delivery and elective caesarean section resulted in a more positive delivery experience compared with other types of deliveries. This may indicate that any divergence from the planned intervention, such as urgent caesarean sections or operative vaginal interventions, particularly if these procedures are carried out in emergency circumstances, may have a traumatic influence. 36 This is particularly important when the delivery occurs in an atmosphere of general uncertainty such as a global pandemic.
In Jordan, socioeconomic status and type of insurance are important factors in determining the type of hospital where a woman will give birth. Private hospitals were associated with a more positive experience than public, military, and academic hospitals. In this study, significantly higher levels of satisfaction about giving birth during COVID-19, positive interaction with the medical staff, and higher levels of delivery as positive experience were found to be in private and academic hospitals rather than public and military hospitals. Public and military health sectors took on the main role of providing care for COVID-19 patients in Jordan during the pandemic, and resources were under significant strain, from both a staffing and a financial point of view, which had implications on the services provided to other patient groups, such as pregnant women. 11
Women were significantly more satisfied with their childbirth experience when they had a positive interaction with the staff involved in their care. As the restrictions of the pandemic, isolation policies, reduced staffing, and fear of infection can all impede good rapport between patient and caregiver, this is likely to contribute to the negative impact of the pandemic on new mothers’ satisfaction levels. Satisfaction with the delivery is related to how supported women felt by the staff, the quality of their relationship with the delivery team, and how involved they were made to feel in the decisions surrounding their care.37 –39
This may also explain why women associated low mood after delivery with experiencing childbirth in pandemic conditions. The pandemic circumstances have created considerable anxiety, adversity, and fear, which has a negative emotional effect on pregnant women. 40 Previous studies reported significant levels of depression and anxiety among pregnant women in a number of countries.22 –26 These high levels of depression may be explained by the fact that the formal postnatal health services, usually available to support women and their families were reduced, or in some cases, not available.11,41 In this study, postnatal low mood was reported significantly more frequently in first-time mothers.
Strengths and limitations
This is one of the first studies to examine the childbirth experience in Jordan in a multidimensional fashion taking into consideration multiple social, obstetric, psychological, and COVID-19-related factors, which offers a better understanding of many obstacles that prevented women from having a satisfactory intrapartum and postnatal experience. However, it is not without limitations. The different health sectors were not equally represented in the study, with most women giving birth in private sector hospitals, likely as access to those was easier and other sectors were overwhelmed with COVID-19 patients. Adding to this, the survey was only available to those women who have access to social media; hence, the most deprived could potentially be under-represented. Furthermore, the postnatal psychological impact was based on self-reported symptoms, which could lead to a lack of objectivity and recall bias. Further research of larger samples in regions with similar circumstances is required for the results to be generalized.
Conclusion
Although the acquisition of COVID-19 infection did not have a significant impact on women’s childbirth experience, several pandemic-related factors did. Importantly, positive interaction with medical staff during childbirth, which was likely a challenge due to contact restrictions, wearing of personal protective equipment, and staff shortages during the pandemic, was found to be a major determinant of how satisfactory a woman’s delivery experience was. Those who delivered in private hospitals were more satisfied with their birth experience, highlighting that the strains put on public, military, and teaching hospitals during the pandemic, related to the majority of COVID patients being treated in those facilities, and the resulting in the redistribution of services provided there, may have led to suboptimal support for labouring women. Women who felt that they suffered depression or low mood after delivery attributed this to giving birth during pandemic circumstances. Given the importance of a woman’s appraisal of the events surrounding her delivery in determining her postnatal physical and psychological well-being, having to give birth during the pandemic circumstances, especially for first-time mothers, can have potentially detrimental consequences that may affect her health and reproductive choices in the future. The results of this study offer a better understanding of the effect of pandemic and lockdown circumstances on the perceived experience of mothers during childbirth and postnatally and factors that should be taken into consideration when planning healthcare provision to this population in future similar conditions.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231199038 – Supplemental material for Insights into women’s experiences of giving birth during the coronavirus disease-19 pandemic in Jordan, a cross-sectional survey
Supplemental material, sj-docx-1-whe-10.1177_17455057231199038 for Insights into women’s experiences of giving birth during the coronavirus disease-19 pandemic in Jordan, a cross-sectional survey by Nadia Muhaidat, Batool AlQuabeh and Waed AbdulGhani in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231199038 – Supplemental material for Insights into women’s experiences of giving birth during the coronavirus disease-19 pandemic in Jordan, a cross-sectional survey
Supplemental material, sj-docx-2-whe-10.1177_17455057231199038 for Insights into women’s experiences of giving birth during the coronavirus disease-19 pandemic in Jordan, a cross-sectional survey by Nadia Muhaidat, Batool AlQuabeh and Waed AbdulGhani in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.