
Abstract
Background:
Prenatal health promotion includes the provision of evidence-based information and practical skills to optimize maternal–fetal outcomes. Increasingly, prenatal education is delivered by both healthcare professionals and allied childbirth educators, in community- or hospital-based group classes, targeted outreach programs, and online modules.
Objectives:
To better understand how prenatal health promotion relates to a diverse urban community, we assessed the perspectives of Ottawa, Canada prenatal key informants.
Design:
This is a qualitative research with key informant interviews.
Methods:
Semi-structured interviews were conducted with 11 prenatal key informants, responsible for the design, delivery, or promotion of publicly available prenatal health services. Interviews explored concepts and delivery of prenatal health promotion, strategies to address existing and emerging prenatal topics, identification of barriers to prenatal health services, and recommendations.
Results:
Key informants recommended a lifespan approach to prenatal health promotion, with an emphasis on healthy behaviors, emotional health, labor and delivery, and postpartum/early parenting. Recognizing community health disparities, key informants used community outreach, and intersectoral collaborations for Indigenous and other at-risk communities to mitigate barriers to prenatal service uptake.
Conclusions:
Ottawa key informants conceptualized prenatal health promotion as inclusive, comprehensive, and as an extension of preconception, school-based sexual education. Respondents recommended the design and delivery of prenatal interventions as culturally safe and trauma informed, using online modalities to complement in-person activities. The experience and intersectoral networks of community-based prenatal health promotion programs represent potential capacity to address emergent public health risks to pregnancy, particularly among at-risk populations.
Plain Language Summary:
A broad and diverse community of professionals deliver prenatal education to help people have healthy babies. We interviewed Ottawa, Canada experts in prenatal care/education to learn about the design and delivery of reproductive health promotion. We found that Ottawa experts emphasized healthy behaviors beginning before conception and through pregnancy. Community outreach was identified as a successful strategy to promote prenatal education to marginalized groups.
Background
Prenatal health promotion includes the provision of evidence-based health information, skills, and tools to optimize maternal health and neonatal outcomes. 1 Prenatal education is a standard component of maternity health care practice by family physicians, obstetricians, and midwives; however, it is also delivered in community settings by public health nurses and non-clinical, allied childbirth educators. 2 The diversification of prenatal health education commonly includes commercial organizations, yoga-based practices, 2 and increasingly, Internet e-classes. 3 The emergence of the COVID-19 pandemic in 2020 has shifted in-person maternity care and promotion to online or virtual formats,4–6 which prompts further consideration of the best practices of prenatal health promotion. The heterogeneity of prenatal education, in terms of instruction, delivery, and content, challenges characterization of efficacy on pregnancy outcomes, 7 although systematic reviews demonstrate associations with increased maternal self-efficacy during childbirth 8 and reduced caesarian section rates. 9
Prenatal health promotion, practiced by health professionals, reflects the interdisciplinary approaches used to encourage protective lifestyle behaviors and pregnancy risk factor mitigation, to promote healthy maternal–fetal health outcomes.10–12 Furthermore, prenatal health promotion can be used to successfully target at-risk populations, thereby bridging gaps in primary care access for marginalized communities.1,12,13 In response to the growing diversity of prenatal education modalities, we explored the perceptions, experiences, and recommendations of Ottawa, Canada prenatal key informants. Ottawa is a multicultural, bilingual (English–French) city with about 24% of residents identifying as women of reproductive age (15–49 years old). 14 Ottawa has a stable economy supported by federal government and high-tech employment sectors, which foster high family incomes and education levels. Even so, in 2018, 5% of Ottawa families screened at birth did not have a primary care physician, 4% lived in poverty, 4% required newcomer support, and 3% had not completed high school 15 —communities typically absent from prenatal interventions. 13 We assessed the perspectives and experiences of prenatal key informants to document their conceptualizations of prenatal health promotion, and their approaches to ensure content and delivery of their prenatal interventions reach both the general public and communities facing health disparities.
Methods
Design
We conducted a qualitative study using semi-structured interviews to document the perspectives, experiences, and recommendations of Ottawa, Canada prenatal key informants. A qualitative study design enabled key informants to articulate their perceptions and practices about prenatal health promotion in the context of the general public as well as communities at-risk.
Participants
Key informants were drawn from healthcare practices, agencies, and organizations that deliver publicly available, free prenatal health services. This purposive sampling strategy enabled exploration of prenatal interventions targeted to both the general public along with high-risk communities. Ottawa professionals responsible for the design, delivery, or promotion of prenatal health services were identified through professional, organizational, and social media profiles to ensure a range of clinical, public health, and community-based key informants. Participant age less than 18 years, professions unrelated to prenatal health, and lack of professional experience in the Ottawa region were exclusion criteria. Prospective participants were recruited by email to participate in a single, 1-h semi-structured interview which was audio-recorded. Non-responses to our email invitations were not tracked.
Data collection
Previous prenatal studies1,16 formed the basis of the interview guide, further developed to explore concepts of prenatal health promotion. Specifically, the interview guide included the following: (1) participant role and experiences in prenatal health promotion, (2) delivery formats (in-person, online), (3) content development (standard and emerging prenatal topics, resources, collaborations), (4) access barriers/strategies for community reach, (5) recommendations, and (6) demographics. Prompts and follow-up questions were used to elicit response clarification or encourage participant to expand on their responses. Interviews were conducted in person at participants’ workplaces by female members of the research team (N.L.S., R.M.T.—undergraduate health science students) in August to October 2017, with no non-participants present. Interviewers had no prior relationship with participants. Field notes taken during the interviews, post-interview memos, and preliminary transcripts were used to confirm that thematic saturation was achieved, with emphasis on the deductive codes framed by the interview guide. 17 Interview audio-recordings and field notes were subsequently transcribed for analysis.
Data analysis
Preliminary analysis of a subset of interview transcripts by thematic content analysis 18 was first conducted by the team (N.L.S., K.P.P.) to ensure coding coherency, followed by independent transcript coding, facilitated by NVivo™ (Version 11.4.3, 2084) to organize themes. Coding meetings enabled classification of deductive themes, framed by the semi-structured interview guide, and inductive themes, which emerged throughout the interview discussion. Quotes are attributed to key informants identified by their organization type, or in the case of healthcare practice, their professional title.
Ethics
Key informants provided informed consent prior to participation in interviews. Participants were provided with the rationale for the study, roles of the interviewers in data collection, and their interest in the research topic.
Results
Demographics
Eleven (n = 11) female, prenatal health key informants (Table 1) were recruited from public health agencies, sexual and reproductive health (SRH) non-governmental organizations (NGOs), healthcare practices, Indigenous community health, and pregnant youth education/mental health centers in Ottawa, Canada. Respondents included seven clinically trained healthcare professionals and four non-clinical participants with counseling, coordination, and management roles in their respective organizations. Prenatal health promotion settings were community or healthcare practice based, with services freely available to the public. Public health, NGO, and community organizations represented here were known to participants through intersectoral collaborations, referrals, and community awareness.
Demographics.

RD: registered dietician; RN: registered nurse; MD: medical doctor; NGO: non-governmental organization.
Non-clinical administrators include program directors, managers, coordinators, and counselors.
Concept of prenatal health promotion
Three major themes emerged when participants were asked to define prenatal health promotion: (1) healthy outcomes; (2) lifespan approach; and (3) education. Prenatal health promotion was conceptualized by key informants as education and information sharing to optimize reproductive health even before conception, but also recognized the need for encouragement, and caring for pregnant women. . . . a reproductive health promotion framework would really include preconception health as well. So, really ensuring that individuals in their reproductive years are as healthy as possible prior to conceiving so that we can have the healthiest pregnancy possible, and ultimately have the healthiest newborn possible, as well as the transition to parenting . . . providing expecting parents with the knowledge, the skills, that they need to feel confident, comfortable and prepared for labor and birth, for breastfeeding, for parenting. (NR-05; public health agency)
Key informants were asked to comment on the local health status of pregnant people, with health disparities emerging as an inductive theme. Generally, respondents perceived that as many Ottawa citizens were of high socioeconomic status (SES), this related to good population health: I would say very good, I mean it’s mixed of course but in this practice . . . I see a lot of well-educated middle-class women-employed, Canadian in origin, and they are healthy, aside from being overweight, and very well educated and prepared, as prepared as they can be I think, to reproduce. (NR-06; family physician) The Aboriginal population obviously has more health risks and all health indicators and we tend to be doing poorer in the Aboriginal community. That’s probably influenced by younger pregnancies, more pregnancies per women in Aboriginal communities, also probably lower education status and poverty impact as well . . . I would suspect . . . for Aboriginal women just because of colonization, systemic health inequalities. (NR-01; Indigenous community health center) . . . we do have some lower-income women, new Canadians, and they have a lot more stress, often financial stress, other children, and sometimes that compromises their ability to care for themselves during their pregnancy . . . So there’s sort of a segment of our population I think that has many more challenges than the majority. And we’re aware of that, and we try to address that. (NR-06; family physician)
Prenatal health promotion—content
Key informants identified labor and delivery, postpartum/early parenting, emotional health, and health behaviors as major components of prenatal health promotion (Table 2). Community experiences, agency mandates, local need assessments, and health histories/intake forms such as the Ontario perinatal/antenatal record were used to help inform key informants’ prenatal health promotion. We purposively explored obesity in the context of prenatal care, given recent guidelines for gestational weight gain, 19 and physical activity during pregnancy. 20 Key informants were aware of overweight/obesity as risks to pregnancy and the need for communication around nutrition and physical activity. Exceptionally, prenatal youth specialists reported that obesity discussions were less relevant and potentially harmful for pregnant adolescents.
Prenatal health promotion content.

NGO: non-governmental organization.
Respondents were asked to discuss health promotion of infectious disease risks to pregnancy, including seasonal influenza and Zika virus. Although seasonal influenza vaccinations were generally promoted, some respondents perceived that influenza vaccination and emerging issues like Zika virus were better addressed by family physicians.
Prenatal health promotion—delivery
Prenatal health promotion delivery was most commonly described as in-person activities including individual prenatal counseling, small groups or “pregnancy circles” designed to target Indigenous communities, and traditional prenatal group classes. Major themes included the following: instructor–client rapport, peer socialization, and interactive experiences (Table 3). Key informants recognized that many clients experience uncertainty and seek peer validation in group classes, and reassurance from prenatal instructors. Peer socialization and support was perceived by key informants as a major benefit of group prenatal classes.
Prenatal health promotion delivery.

Even prior to COVID-19, Ottawa area prenatal education included online delivery formats, with public health agencies transitioning some of their content online in efforts to be more cost-effective. We explored key informants’ perceptions about online prenatal health promotion with key informants acknowledging increased accessibility and individualized learning pace as benefits; however, these technological platforms were perceived to limit social networking with peers and instructors, and complicated physical demonstrations of activities such as breastfeeding and labor and delivery positions. Technology barriers were identified for low SES clients and marginalized youth. Prior to the pandemic, online prenatal activities provided by public health agencies did not outcompete in-person sessions, with many participants preferring to meet in person.
Barriers to prenatal education
Participants generally understood that access barriers to prenatal health promotion and related healthcare services existed, identifying four themes: transportation, financial, stigma/shame, and language (Table 4). Intersecting social determinants of health were perceived to contribute to both lack of awareness that public health–delivered prenatal education is free, as well as compliance issues with healthy lifestyle recommendations, such as the affordability of nutritious foods and vitamin supplements. Language barriers were recognized in both immigrant communities and among Francophones who may lack French-language health service access.
Barriers to prenatal health promotion and mitigation strategies.

NGO: non-governmental organization.
Stigma, shame, and mistrust barriers were perceived to impact pregnant adolescents and women from low-income, Indigenous, immigrant, and racialized communities. Key informants discussed the interrelationships between mistrust of the medical system and feelings of stigma/shame, which ultimately disincentivized some people from accessing prenatal health services, including health promotion. Poverty, past-trauma, addiction, and mental illness were perceived by participants to contribute to stigma and shame. Mitigation strategies included community outreach, trauma-informed care, and warm handovers, the latter a strategy to ensure continuity of care, and reflecting the intersectoral collaborations within the city.
Recommendations
Key informants recommended preconception health promotion (Table 5), echoing back to their lifespan conceptualization of health promotion. Respondents considered that many prenatal risks are difficult to mitigate during pregnancy, supporting the need for preconception health promotion. The second major recommendation to improve prenatal health in the region was more inclusive prenatal health promotion. Most respondents had worked in multiple community sectors throughout the region and were very mindful of community health disparities. Although Indigenous communities were most commonly mentioned, pregnant people from queer communities and language minority groups were also identified as typically absent from general health promotion activities.
Strategies and recommendations for prenatal health promotion.
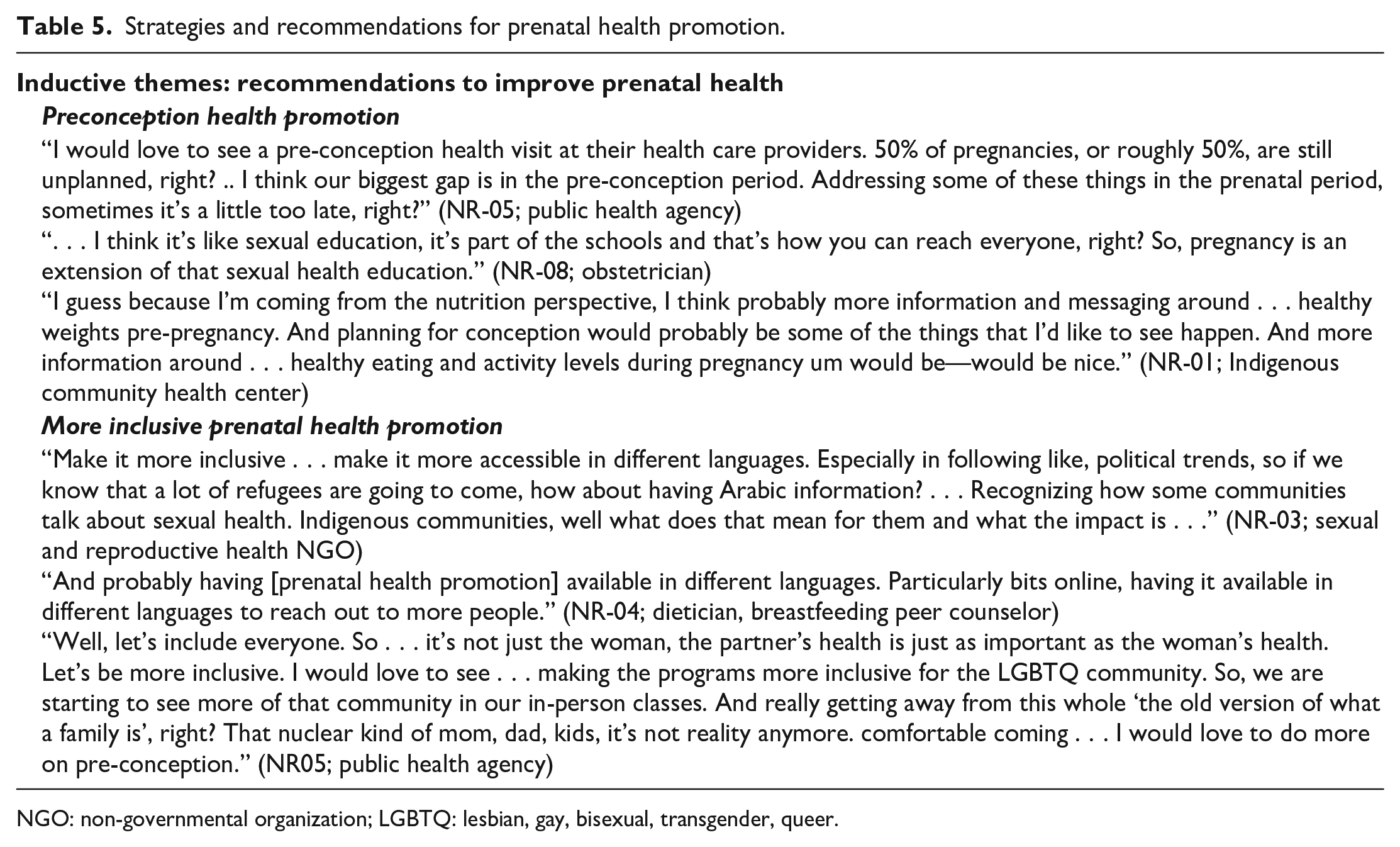
NGO: non-governmental organization; LGBTQ: lesbian, gay, bisexual, transgender, queer.
Discussion
Ottawa key informants were aware of the social determinants which informed pregnancy experiences, and contributed to the health disparities among Indigenous, immigrant, and low-income communities. To ensure health equity, participants recommended that prenatal health promotion should provide tailored, culturally safe, and trauma-informed care using a range of modalities such as community outreach, in-person classes, individual sessions, and as a supplementary option, virtual or online platforms. Despite the heterogeneity of our key informants in terms of training and practice domains, participants were remarkably consistent in their framing of prenatal health promotion, and perceptions of reproductive health challenges for pregnant people in Ottawa. Respondents recommended that mitigation of modifiable prenatal health risks was best achieved prior to conception, emphasizing the need for preconception health promotion as an extension of school-based sexual health education programs. As almost half of the Canadian pregnancies are unplanned, and the most critical period of fetal organ development occurs before the first prenatal healthcare visit, 21 a proactive, lifespan approach, the cornerstone of prenatal programs in the United States,22–24 would optimize maternal–fetal health outcomes.21,25,26
Ottawa prenatal professionals strongly endorsed in-person prenatal health promotion, with emphasis on activities, social networking among participants, and interactions with provider/instructor. The provision of in-person maternity care was perceived to foster the development of trust and understanding between client and provider/instructor. Pre-pandemic online prenatal health promotion, in contrast, was perceived as failing to provide social connectivity among peers and instructors/healthcare providers. In-person prenatal health promotion provides opportunities for the provider/instructor to address both verbal and non-verbal expressions of pregnancy/parenting uncertainty and insecurity, to promote patient self-efficacy and empowerment. 27 Our discussions with Ottawa prenatal key informants about online health promotion in 2017 proved timely, as many in-person SRH services were later canceled, reduced, or moved online during the COVID-19 pandemic.4,28 Before the pandemic, online prenatal education platforms were developed by commercial organizations and adopted/refined by public health agencies throughout North America, representing a cost-effective prenatal health service delivery model. 3 Online prenatal health interventions and telehealth services are vital strategies for rural and remote communities in Canada which lack consistent maternity care. 4 The emergence of new virtual technology platforms during the pandemic, coupled with social media, may have overcome some of the challenges of traditional online prenatal education modules to provide peer socialization, with benefits reported by pregnant women participating in Zoom group physical activity, 29 online pregnancy circles, 6 and social media/website/radio–TV prenatal classes in remote communities. 4 Migrant and refugee women in Canada expressed the desire for multiple SRH messaging modalities, with some preferring one-on-one consultations and others preferring group-based format with supplemented online information. 30 Although prenatal telehealth models may be appropriate for low-risk pregnancies, virtual maternity care may exacerbate existing health disparities. 31 Lessons learned from the global experience of virtual delivery of education, health services, and physical activity programs may further increase the use of online prenatal health promotion as a complementary strategy post-pandemic.
Culturally competent health promotion
Ottawa prenatal health promotion encompassed both general interventions aimed at the general public, but also tailored strategies to meet the needs of communities marginalized by poverty, systemic racism, colonialism, or xenophobia. Key informants with generalized practices relied on community organizations to target prenatal services for youth or Indigenous pregnant people, demonstrating intersectoral collaborations. For public health sector key informants, differential programming approaches, including in-person interventions, small groups or pregnancy circles, and outreach strategies, were mandated and considered essential to build connections and overcome mistrust of the healthcare system. Culturally competent care is increasingly a fundamental tenet in best practices for prenatal health promotion,24,32,33 ensuring providers recognize cultural diversity and how culture shapes behaviors. 34 Examining the provider–patient relationship in the context of Indigenous health, the concept of cultural safety further considers the establishment of shared respect, dignity, and recognition of the Indigenous patient as a person of value. 34 The incorporation of community elders and use of the medicine wheel—an Indigenous conceptualization of holistic health and wellness—in Ottawa prenatal interventions are consistent with recommended strategies to reduce maternal and newborn health disparities through uptake of interventions, and improve healthcare provider–client relationship satisfaction.4,34,35 Furthermore, Indigenous community investment–ownership–activation with the initiation, development, and implementation of prenatal–infant–toddler health promotion programs is a critical pathway for the success of these interventions. 36 Ottawa prenatal key informants promoted personal empowerment through knowledge, tools, and development of self-efficacy to mitigate most pregnancy-related concerns. Development of cultural safety requires some time for connection and experience sharing, which may be possible virtually, 4 though perhaps better fostered by in-person interactions. Migrant and refugee women in Canada identified empathetic, women-centered care as essential for discussions related to SRH, with providers taking time to establish environments of trust. 30
Pregnant adolescents experience high rates of poverty, abuse, and mental illness, further complicated by substance abuse. 37 Recognizing this, Ottawa youth specialists described trauma-informed approaches that focussed on resiliency, safety, and promotion of attachment. These key informants further acknowledged adolescents’ history of trauma as the foundation of their mistrust of healthcare professionals, reluctance to share information and experiences about pregnancy, and as potentially affecting their capacity for maternal attachment. Prenatal care models incorporating cultural competence and trauma-informed care may be relevant for pregnancy interventions for at-risk adolescents, Indigenous, racialized, refugee, and other minority communities.35,38
Empathetic health promotion
Key informants identified essential components of prenatal health promotion such as lifestyle/healthy behaviors, labor and delivery, emotional health, and postpartum/parenting—consistent with recommended guidelines.1,12,13,3 Lifestyle/healthy behaviors, particularly nutrition and physical activity, were often discussed by key informants as risk mitigation strategies to prevent adverse maternal (e.g. gestational diabetes, hypertension) and fetal health outcomes, as well as strategies to improve labor and delivery experiences, consistent with the literature.25,26 Participants described appropriate gestational weight gain targets 19 and acknowledged that overweight/obesity was an issue for the Ottawa general population. Physical activity guidelines during pregnancy 20 can be incorporated in all prenatal health promotion activities, with emphasis on gestational weight gain targets 19 but also as a means to mitigate stress and improve emotional health and wellbeing. 29 As weight stigma is a barrier to healthy behaviors, Ontario pregnant women living with obesity articulated that exercise recommendations tailored to different body sizes and visual representations of pregnant people living with obesity in health promotion would be helpful. 39
Health promotion as risk communication
It is well established that exposures to infectious pathogens such as severe acute respiratory syndrome coronavirus 1 (SARS-CoV-1) and SARS-CoV-2 (COVID-19), H1N1, H5N1, and Zika virus during pregnancy cause adverse maternal and offspring health outcomes.40–42 Ottawa key informants were generally hesitant about introducing emergent pregnancy risks such as Zika virus, preferring to maintain an optimistic tone about positive topics such as healthy baby outcomes. Although Zika virus was never endemic in Canada, with cases in North America limited to local transmission in Florida and Texas, 43 travelers did pose Zika-related risk questions to their Ottawa maternity care providers. Given that many infectious diseases and/or treatments have risk implications for pregnancy, prenatal health promotion should develop strategies to amplify scientific messaging and to counter myths and misinformation. 42 During infectious disease outbreaks and other emergent public health threats to pregnancy, prenatal health specialists can play a central role in the promotion of evidence-based, pregnancy risk mitigation communication, and as public health advocates.
Seasonal influenza prevention programs, including annual vaccines and risk messaging, represent an opportunity to establish community-level interventions for the general public and at-risk groups. It is well established that influenza infections during pregnancy increase risk of maternal morbidity and mortality, preterm delivery, low birthweight, and neonatal death.41,44 Despite the World Health Organization’s identification of pregnant people as the highest priority population for influenza vaccination, 45 national vaccine uptake during pregnancy in developed countries is generally less than 50%.41,46,47 Ottawa key informants generally supported influenza vaccinations, but many questioned their relevancy as a prenatal topic. Influenza vaccine hesitancy by pregnant people may be due to perceived concerns about vaccine safety, gaps in vaccine promotion from maternity care providers, and lack of awareness.41,48 Given that history of influenza vaccine uptake along with education and awareness is now known to be predictive of COVID-19 vaccine uptake during pregnancy, 49 it is evident that seasonal influenza vaccine community programming provides an essential foundation for future emergent infectious disease risks, in terms of prenatal education, community outreach, and social media communication.
Limitations
Our recruitment of key informants emphasized engagement with prenatal health promotion within community/public health sectors, excluding allied childbirth educators engaged in commercial organizations. Despite our small sample size, thematic saturation was achieved, and the population reach of the agencies/organizations represented in this study is considerable, given free service provision and established community/healthcare mandates. The breadth of organizations represented here is a strength of this study as they reflect health promotion for the general public along with targeted services for high-risk communities. The findings are not generalizable but do provide valuable best practices for the delivery of prenatal health promotion in diverse urban environments.
Conclusion
Best practices in prenatal health promotion should include early preconception interventions that are culturally safe and trauma informed, both in design and delivery. Given the heterogeneity of pregnant people in our urban communities, multiple modalities for prenatal health promotion are required, ensuring tailored, small group, and individualized options, supported by community outreach for at-risk groups. Gaps remain, however, in the recognition that prenatal health promotion must be readily adaptable to include emergent public health risks to pregnancy, and grounded by evidence-based communication strategies to refute misinformation and promote pregnancy risk mitigation.
Supplemental Material
sj-docx-1-whe-10.1177_17455057231158223 – Supplemental material for Best practices in prenatal health promotion: Perceptions, experiences, and recommendations of Ottawa, Canada, prenatal key informants
Supplemental material, sj-docx-1-whe-10.1177_17455057231158223 for Best practices in prenatal health promotion: Perceptions, experiences, and recommendations of Ottawa, Canada, prenatal key informants by Nura L Soucy, Rowan M Terrell, Rebecca A Chedid and Karen P Phillips in Women’s Health
Supplemental Material
sj-docx-2-whe-10.1177_17455057231158223 – Supplemental material for Best practices in prenatal health promotion: Perceptions, experiences, and recommendations of Ottawa, Canada, prenatal key informants
Supplemental material, sj-docx-2-whe-10.1177_17455057231158223 for Best practices in prenatal health promotion: Perceptions, experiences, and recommendations of Ottawa, Canada, prenatal key informants by Nura L Soucy, Rowan M Terrell, Rebecca A Chedid and Karen P Phillips in Women’s Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.