
Abstract
Background
In Iran, blood products were being delivered to healthcare centers without charge. For optimum usage and reducing wastage, the tariff was set on October 23, 2015. Thus, hospitals must pay for blood products to blood transfusion services and then the expenses are paid to healthcare centers by the insurance.
Objectives
This study aimed to explore the effects of the tariff policy on utilization pattern of blood products in healthcare centers of Fars province, Iran.
Design
This is a retrospective study which analyzes the recorded data.
Methods
Throughout this retrospective study, the number of units requested, delivered, returned, and return/delivery ratio of RBC, FFP, cryoprecipitate, and platelet were examined before and after the tariff in different cities of Fars province of Iran.
Results
After the tariff, return/delivery ratios of FFP, cryoprecipitate, and platelet increased in comparison with before tariff but were not statistically significant which means the return of unused units was increased after imposing tariff.
Conclusion
The results of this investigation showed that tariff may lead to more return of FFP, cryoprecipitate, and platelet units to the transfusion services of Fars province. More research must be performed to further approve it.
Background
Blood transfusion is a vital therapy that can save patients’ lives and is an inevitable part of healthcare services. 1 Studies have suggested that blood products are frequently overprescribed all over the world. 2 Because blood is a rare, invaluable, and expensive resource, irrational blood usage significantly increases the expenses in healthcare centers. 3 It has been reported that globally more than 50% of all medical interventions are not appropriately prescribed. 4 Inappropriate transfusion of blood products can lead to adverse events. Many investigations have demonstrated the correlation between the transfusion of blood components and the increased risk of death and diseases.5,6,7 These adverse effects are allergic reactions, hemolytic transfusion reactions, alloantibody formation, longer hospitalization period, febrile nonhemolytic transfusion reaction (FNHTR), transfusion-related acute lung injury (TRALI), and circulatory overload in patients with cardiovascular diseases. 8
Blood management refers to appropriate consumption of blood products to reduce excessive transfusion. 9 Blood consumption should be optimized, and expenses should be reduced. 3 Although blood donation is voluntary and free of charge, processing of blood products and laboratory tests such as testing for transfusion-transmitted diseases and distribution of blood products are costly and must be paid for. 10
In Iran, the blood products were being distributed to hospitals without charge until October 23, 2015. The tariff was set on October 23, 2015 for more efficient consumption pattern and diminishing wastage. After the tariff, healthcare centers must pay for supplying blood products to blood transfusion service and then the insurance will cover the expenses and give the payment to the healthcare centers. 11 Therefore, in both cases, blood products are free of charge for patients.
The objective of this investigation was to explore the influence of imposing tariff policy on management, consumption rate, and wastage of blood products in different cities of Fars province.
Materials and Methods
This is a retrospective study. All data was provided by the Blood transfusion service of Fars province, Iran. The red blood cell (RBC), fresh frozen plasma (FFP), cryoprecipitate, and platelet requests, deliveries, returns, and return/delivery ratios of five different cities of Fars province of Iran were compared in 2 years before tariff (October 23, 2015) and 2 years after tariff.
The number of units requested is defined as the number of blood units that have been requested by healthcare centers from blood transfusion service. The number of units delivered is defined as the number of blood units that have been delivered to healthcare centers. Return is defined as unused number of blood components in hospitals that are returned to the national blood transfusion services so that they will be sent to other hospitals for consumption based on their requests. 11 Request, delivery, and return values refer to total number of units in each of the centers throughout 2 years.
Blood transfusion services are available in hospitals and/or healthcare centers of all cities, and all patients are transfused without charge in all cities before and after tariff. The blood transfusion organization of Fars provides all hospitals and/or healthcare centers of all cities with blood products as they request.
Kolmogorov–Smirnov test was used to check the normal distribution of data in each group. Paired sample t-test was employed for comparison of the parameters before and after the tariff. P-value less than 0.05 was statistically significant. In addition, GraphPad Prism 9.0.0 (GraphPad software LLC, for Windows, San Diego, California, USA) was used for statistical analyses and data visualization.
Results
The total number of hospitalized patients from October 23, 2013 to October 23, 2015 (before tariff) was 454,932 while it was 517,996 from October 23, 2015 to October 23, 2017 (after tariff). Therefore, there is 12% increase in the total number of hospitalized patients. Request, delivery, return, and return/delivery ratio for RBC, FFP, platelet, and cryoprecipitate in different cities of Fars province were investigated. None of the indexes after tariff was statistically significant in comparison with before tariff.
RBC
RBC request was slightly elevated following imposing tariff policy but it was not significant (P-value = 0.19). On the other hand, RBC delivery did not show any changes. Also, RBC return decreased after the tariff (P-value = 0.11). Unexpectedly, the RBC return/delivery ratio index decreased following imposing the tariff policy however it was not significant (P-value = 0.07) (Figure 1).
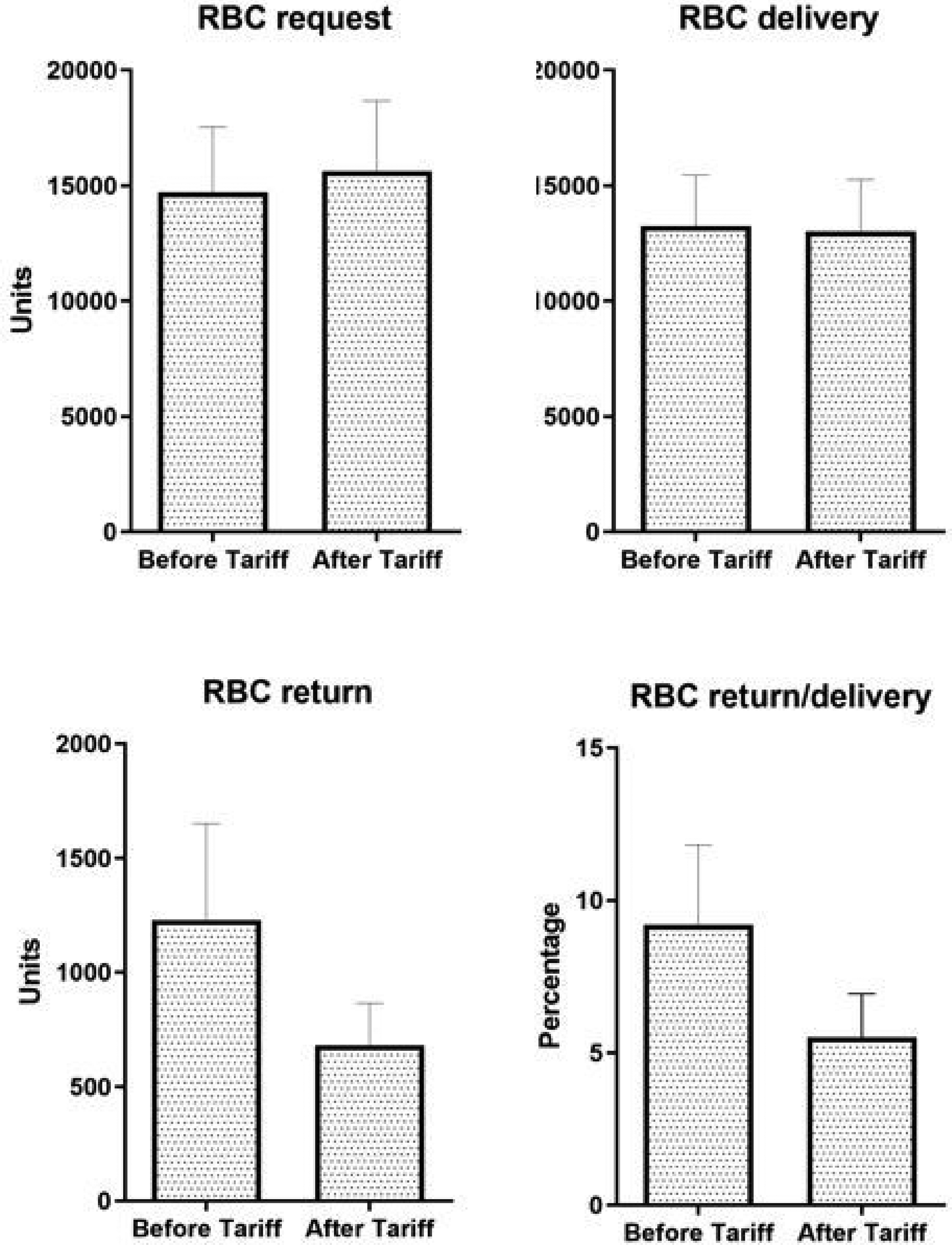
RBC request, delivery, return, and return/delivery ratio before and after imposing the tariff.
FFP
FFP request and delivery decreased following the policy and the changes were not statistically significant (P-value = 0.47 and 0.45, respectively) (Figure 2). Although FFP return was decreased after imposing the tariff policy (P-value = 0.46), the FFP return/delivery ratio index augmented in comparison with before the tariff (P-value = 0.74). None of these parameters were statistically significant.
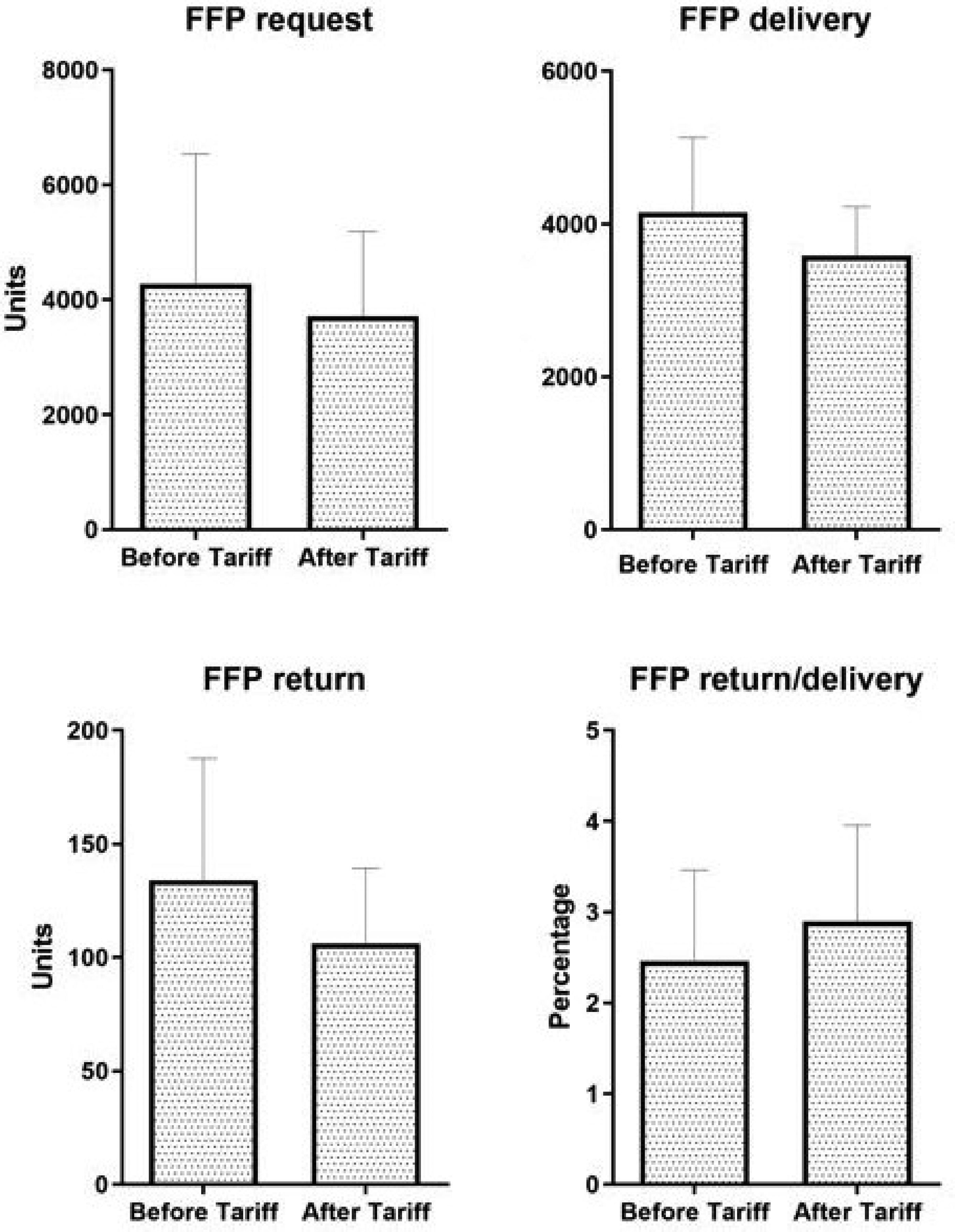
FFP request, delivery, return, and return/delivery ratio before and after imposing the tariff.
Cryoprecipitate
Cryoprecipitate requests showed a statistically insignificant increase after the tariff (P-value = 0.09) (Figure 3). As a result of such more demand, Cryoprecipitate delivery was increased (P-value = 0.06) although it was not significant as well. Cryoprecipitate return (P-value = 0.34) and return/delivery ratio (P-value = 0.72) indices were also increased following imposing the policy, but they were not significant.

Cryoprecipitate request, delivery, return, and return/delivery ratio before and after imposing the tariff.
Platelet
Platelet request (P-value = 0.23) and delivery (P-value = 0.24) were decreased after the policy and they were not significant (Figure 4). Resultantly, platelet return was decreased which was not significant (P-value = 0.62). In addition, platelet return/delivery ratio index was decreased following imposing the policy (P-value = 0.78).
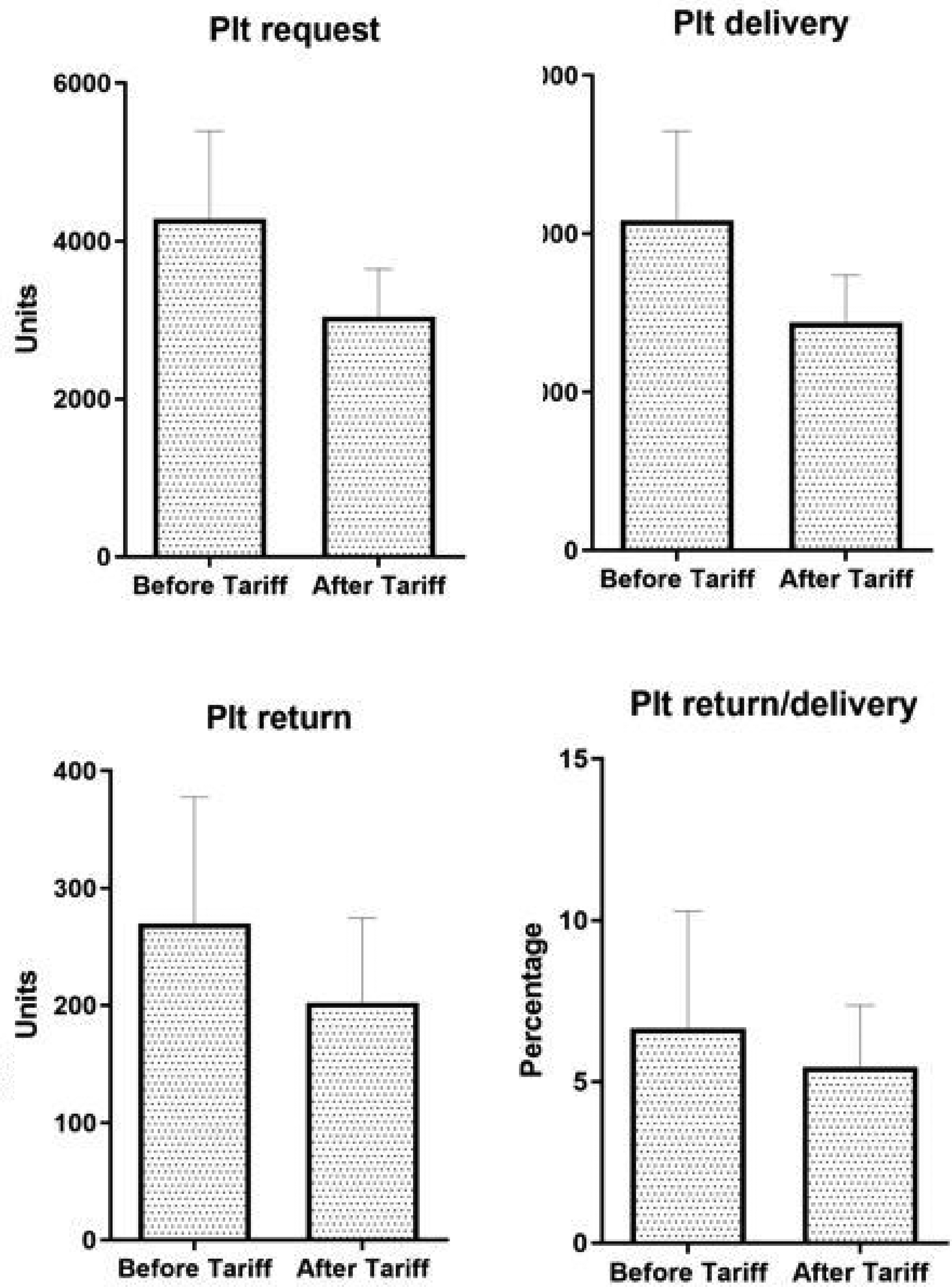
Platelet request, delivery, return, and return/delivery ratio before and after imposing the tariff.
Discussion
This is the second study that investigates the effect of tariff policy on consumption pattern of blood products. This study was performed in Fars province of Iran. According to our study, RBC request was slightly elevated following imposing tariff policy, but RBC delivery did not change. In addition, RBC return and return/delivery ratio index decreased after the tariff. Therefore, it might show an efficient request pattern. FFP request, delivery, and return decreased following the policy and FFP return/delivery ratio index increased after tariff. Decreased FFP delivery despite the increasing need, to some extent may explain the decreased FFP return. Increased return/delivery ratio index for FFP was the result of the return of unused FFP units after the tariff. Cryoprecipitate request, delivery, return, and return/delivery ratio increased after the tariff. Also, platelet request, delivery, return, and return/delivery ratio index were decreased after the policy. Decreased platelet delivery may be the reason for decreased platelet return.
These parameters were not statistically significant, despite that more research must be carried out to further approve it. The number of hospitalized patients two years before the tariff was 454,932, while 2 years later it reached 517,996, which means that the figure for hospitalized patients has augmented by 12%. Increasing the number of hospital admission—regardless of the etiology of the disease—increases blood consumption and may be associated with decreased return of unused units from healthcare centers to blood transfusion services.
The reason for reduction in RBC return might be the increase in the number of patients and unchanged RBC distribution. It may be a sign of better RBC management. In case of RBC, it might also be possible that the hospitals are wasting RBC units and further research is needed to unveil the underlying reason.
Blood transfusion is an important part of various therapeutic guidelines that must be manipulated with special precautions because blood transfusion as a treatment strategy may have many complications, such as the transmission of viral infections, transfusion reactions, and alloimmunization.12,13
Because of the expensive technologies for the preparation of different cellular and plasma products, and the limitation of alternative sources, researchers put blood transfusion medicine in line with guidelines and standards for proper use to save as much blood resources as possible. 14
Unnecessary transfusion reduces the storage of blood products in blood banks, and increases blood supply costs and workload of blood transfusion services. 15
In many hospitals, the request of blood products is significantly higher than transfusion, and such an inefficient blood product utilization poses significant financial and moral losses. 16 Blood products are transfused to patients without any profit and exactly at the cost of their preparation expenses. 17 In Iran, blood products are distributed without charge to patients. In line with the evolution of healthcare reforming, tariff policy was imposed on blood products on October 23, 2015. In Iran, blood transfusion service provide hospitals with required blood units. Before tariff, blood products were being delivered free of charge from blood transfusion service to hospitals. After tariff, hospitals must pay for blood products to blood transfusion service and later insurance will pay the expenses to hospitals. 11
Gharehbaghian and colleagues demonstrated that the problems associated with blood consumption are lack of transfusion committees in hospitals, inexperienced physicians, lack of external audition on blood banks in hospitals, lack of software matching between healthcare centers and blood services, lack of type and screening before admission, and more specifically free blood transfusion in hospitals. 16 To minimize blood wastage and improve blood saving, more attention should be paid to blood ordering. 18
The first study on the effects of Tariff on consumption of blood products carried out in Kerman province of Iran by Anani and colleagues showed that imposing tariff policy on blood products increased the return and return/delivery ratios for FFP and platelet. Their findings showed that the tariff led to more return of unused FFP and platelet to blood transfusion service thereby less wastage but it was not statistically significant. On the other hand, the return and return/delivery ratio indices for RBC significantly increased following imposing the tariff policy. 11 Inconsistent with their findings, tariff led to a statistically insignificant return of unused FFP, cryoprecipitate, and platelet units to the blood transfusion services of Fars province, Iran. Although, the number of admitted patients and the need for blood products increased after the policy, more efficient requests for blood products may explain the insignificant return.
This paper investigated the effects of imposing tariff policy on the management and consumption of blood products. It is inferred from this study that the RBC return and return/delivery ratio indices were decreased following tariff policy. Noteworthy, a 12% increase in the number of patients and yet unchanged RBC delivery is an important reason for it which shows that consumption pattern has been more efficient. In contrast, FFP and Cryoprecipitate return/delivery ratios were increased following the tariff policy. Current investigation highlights that in terms of health care reforming, tariff policy may be effective on the return and request of unused FFP, cryoprecipitate, and platelets in addition to better management of RBC; however further investigation is needed to validate our findings.
Limitations
The limitations of the current study are lack of access to the exact number of wasted blood products and multitude of confounding variables affecting the analysis including illness severity of the patients etc.
Conclusion
The return of unused units of FFP and Cryoprecipitate has been increased after tariff but the increase was not statistically significant. Further research is required to validate the efficacy of tariff on consumption patterns of blood products to minimize wastage through ensuring efficient blood ordering and consumption, and more return of unused blood products.
Footnotes
Acknowledgment
We appreciate the blood transfusion organization of Fars province for providing us with the data.
Author Contributions
Rohollah Baktashi: Formal analysis, Writing – original draft. Fariba Rad: Methodology. Masoud Torabi Ardekani: Investigation. Alireza Salah: Conceptualization. Hossein Anani: Data curation, Methodology. Roohollah Mirzaee Khalilabadi: Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
Author Contributions
RB contributed to investigation, writing the original draft, conceptualization, data collection. FR contributed to investigation, review and editing. MTA contributed to investigation, review and editing. AS contributed to investigation, review and editing. HA contributed to writing original draft, review and editing, methodology, data analysis. RMK contributed to supervision, final editing and review, methodology and conceptualization.
Availability of Data and Materials
The raw data will be available by the corresponding author upon logical request.
Consent for Publication
Not applicable.
Consent Statement
Current study was performed according to the ethics rules and regulations. It was performed analyzing the recorded data of centers. Our study did not require ethical board approval because no humans or animals were used in this study. No human data was used in this study. In addition, data of centers were only used for this paper.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not applicable. Current study was performed according to the ethics rules and regulations. It was performed analyzing the recorded data of centers. Our study did not require ethical board approval because no humans or animals were used in this study. No human data was used in this study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.