
Abstract
Background:
Esophageal discontinuity remains a significant challenge. However, the literature lacks a comprehensive understanding of the indications for esophageal discontinuity, strategies for reversal, and long-term outcomes. This scoping review characterizes the existing evidence, identifies knowledge gaps and provides practical considerations.
Methods:
Following Arksey and O’Malley frameworks, we searched MEDLINE, EMBASE, and CENTRAL for studies from 1990 to 2023 involving patients who received a cervical esophagostomy for gastrointestinal discontinuity. Grey literature, editorials, protocols, and non-English studies were excluded. Two authors independently screened titles, abstracts, and full texts.
Results:
Of the 231 studies included, 150 (65%) were case reports, 62 (26.5%) were single-institutional observational studies, 10 (4.3%) were reviews, with few other study designs. Most studies (68%) were in the adult population. The most common geographical region was East Asia (32%), followed by North America and Western Europe (both 24.2%). The most common indications were perforation (29%), stricture/fistula (21.6%) and atresia (18.6%), with notable regional variation. Only 24.2% of studies occurred in the oncologic setting and 24.2% of studies did not report whether reversal was considered. Among 1884 patients with esophageal discontinuity, the overall reversal rate was 79.8%; excluding atresia cases, the rate was 73.2%.
Conclusion:
There are critical gaps in the literature, including a lack of multi-institutional studies, limited descriptions of reversal procedures, lack of measurement of nutritional and functional outcomes and few clinical trials. Greater international collaboration is needed to develop a longitudinal registry and define long-term quality outcomes for this complex rare disease entity which could be known as foregut failure.
Keywords
Key Learning Points
Esophageal discontinuity and cervical esophagostomy are under-studied, with limited multi-institutional data and few long-term outcome measures.
Reversal is feasible in most cases, yet strategies and outcomes are inconsistently reported.
We propose the term foregut failure to unify nomenclature and promote future research collaboration.
Introduction
Esophageal discontinuity presents a complex challenge for modern thoracic and foregut surgeons.1,2 In emergent scenarios, this condition often arises following catastrophic esophageal or gastric injury requiring a “damage control” approach to preserve life, where re-anastomosis cannot safely be performed.2 -5 In such cases, life-threatening mediastinitis or sepsis necessitates urgent source control, typically achieved by resecting the diseased segment and diverting the gastrointestinal tract through the creation of a cervical esophagostomy.1 -3 After sepsis resolves and the patient’s physiological parameters improves, delayed reconstruction may be pursued to restore intestinal continuity.1 -3 Classically, restoration is accomplished through either gastric pull-up, small bowel interposition requiring microvascular “supercharging” or colonic interposition. However, many patients present with significant challenges to the restoration of GI continuity and in some cases cannot be reconstructed with conventional methods.
In elective settings, esophageal discontinuity may occur in one of few contexts: (i) those undergoing high-risk procedures such as salvage surgery or interposition grafting who may or may not have poor performance status; (ii) catastrophic intra or post-operative complications (eg, conduit necrosis, anastomotic leak or iatrogenic perforation); and (iii) pediatric patients with significant long-gap esophageal atresia.6 -10 In the emergency setting, esophageal discontinuity may typically occur after perforation (Boerhaave’s syndrome) or caustic ingestion. 2 Regardless of etiology, the principles of esophageal discontinuity procedures include (i) cardiopulmonary resuscitation, (ii) source control, (iii) diversion (iv) nutritional support, and (v) restoration of intestinal continuity. 1 Therefore, in the surgical pathway for esophageal discontinuity, the initial operation typically results in esophageal diversion via cervical esophagostomy. 11
Originally described in 1951 as a feeding strategy for patients with advanced head and neck cancer, cervical esophagostomy is now used in both emergent and elective settings to prolong life after a catastrophic foregut event.1 -3,11 However, esophagostomy is considered a debilitating state and is associated with significant comorbidity, including weight loss, metabolic derangements, and decreased quality of life. 12 Additionally, esophagostomy may be associated with high healthcare utilization with repeated visits in the outpatient setting and potentially the emergency room such as repeated dilation and other interventions. Reconstruction remains technically challenging and requires individualized planning based on available conduits and individual patient considerations.2,3,13,14 Several studies discuss the management of esophageal perforation or delayed reconstructive options following esophagectomy, however relatively little attention has been placed on patients who have been left in discontinuity.15 -17 More specifically, the outcomes of patients with cervical esophagostomy, their healthcare utilization, and disease-specific outcomes are underreported. At present, there appears to be a gap in our understanding of the rates of reversal and reconstructive options for patients with cervical esophagostomy.
This scoping review aims to map the current evidence on cervical esophagostomy and esophageal discontinuity procedures, focusing on indications, reversal strategies (including novel gastrointestinal allotransplantation), and patient outcomes in the modern era. We introduce the term foregut failure to describe this complex clinical condition, with the goal of promoting standardized nomenclature and research collaboration.
Methods
The objectives, study characteristics, and methods of this scoping review were detailed in a previously published protocol. 18 Reporting followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Extension for Scoping Reviews (PRISMA-Sc) and Arksey and O’Malley scoping review framework.19,20 This review was registered with Open Science Framework (osf.io/s3b4g). 18
Objectives
This scoping review addressed the following questions:
What are the clinical indications for esophageal discontinuity procedures?
What are the short- and long-term outcomes for esophageal discontinuity procedures including healthcare utilization and disease-specific metrics?
What are the indications and outcomes of reversal procedures?
Data Sources, Search Strategy
The search strategy was developed in consultation with a health sciences librarian at the University of Toronto. The strategy was initially developed for use within MEDLINE (Supplemental Table 1) and subsequently adopted for EMBASE and CENTRAL.
Eligibility Criteria
The population for this study includes pediatric (<18 years old) and adult (≥18 years old) patients, who have received a cervical esophagostomy in the context of a gastrointestinal discontinuity procedure or those who have had reversal of a cervical esophagostomy. Randomized and non-randomized interventional trials, prospective and retrospective observational studies, reviews and meta-analysis, case series, and qualitative study designs written in English were included. Editorials, opinion pieces, dissertations, conference abstracts, protocols, and grey literature studies, and animal studies were excluded. Moreover, studies examining resection of the esophagus with no diversion, studies examining creation of esophagostomy with no underlying resection, or studies where a non-surgical esophagostomy was created (ie, image-guided or endoscopic-guided esophagostomy) were excluded (Supplemental Table 2). MEDLINE, EMBSAE and CENTRAL were searched for eligible papers from 1990 to 2023 were included to represent literature within the “modern era.”
Evidence Screening and Selection
Studies were input into Covidence Systematic Review Tool (Veritas Health Innovation, Melbourne, Australia). Prior to beginning the full abstract screening, a random sample of 25 titles were screened by two reviewers to assess the clarity of the selection and inclusion/exclusion criteria. Once an inter-observer reliability of ≥75% between the two independent reviewers was achieved, title and abstract screening commenced followed by full text selection by the two independent reviewers. Conflicts were resolved by consensus and/or consultation with the research team.
Exposures: Cervical Esophagostomy and Esophageal Discontinuity
The primary concept of this study is identifying patients who have been left in esophageal discontinuity with a cervical esophagostomy. As described above, the conditions by which cervical esophagostomies are created, in the context of esophageal discontinuity procedures, is usually a complex, high-acuity, highly morbid clinical scenario. Under these conditions patients are usually either critically ill or had a catastrophic intra operative event.6 -8 Similarly, reversing esophageal discontinuity remains a technical challenge. Reversing cervical esophagostomies in patients that have been left in esophageal discontinuity requires a suitable conduit or graft, and given the conditions and physiological insult at the time of the first operation, options may be limited.21 -23 Therefore, reversing esophagostomies often requires a multidisciplinary approach to reconstruction and may include multi-stage operations in collaboration with otolaryngology – head and neck surgery, and plastic and reconstructive surgery.2,24
Outcomes: Post-Operative Outcomes, Healthcare Utilization, and Disease-Specific Outcomes
We examined the literature for relevant post-operative outcomes in the short and long term for patients left in esophageal discontinuity with a cervical esophagostomy. These included measures of mortality, morbidity, and procedure specific outcomes (ie, anastomotic leaks), fistula formation, and rates of reversal. Similarly, we examined healthcare utilization outcomes in this population including measures of re-operation, hospital length of stay, return to emergency department, hospital readmission, and quality of life measures such as functional status and patient reported outcomes. We also examined disease-specific outcomes in the context of their underlying pathology (such as functional outcomes or oncologic outcomes) as well as explored if there were any components of the index procedure that were performed in a minimally invasive surgical (MIS) fashion. Finally, we stratified results based on adult versus pediatric patient population, benign versus oncologic indications and by geographical region.
Data Extraction and Analysis
Data extraction followed an iterative process as outlined by Arksey and O’Malley. 19 Data extraction tables were designed a priori based on content expertise and scoping review guidance and were previously published. 18 Data extraction was completed by two independent researchers and subsequently reviewed with the research team. Thematic analysis was performed, and data extraction tables were iteratively updated guided by the research objectives and study findings (Table 1).
Data Extraction Table for Included Multi-Institutional Observational Studies, Controlled Trials, and Large Volume Single Institutional Observational Studies.
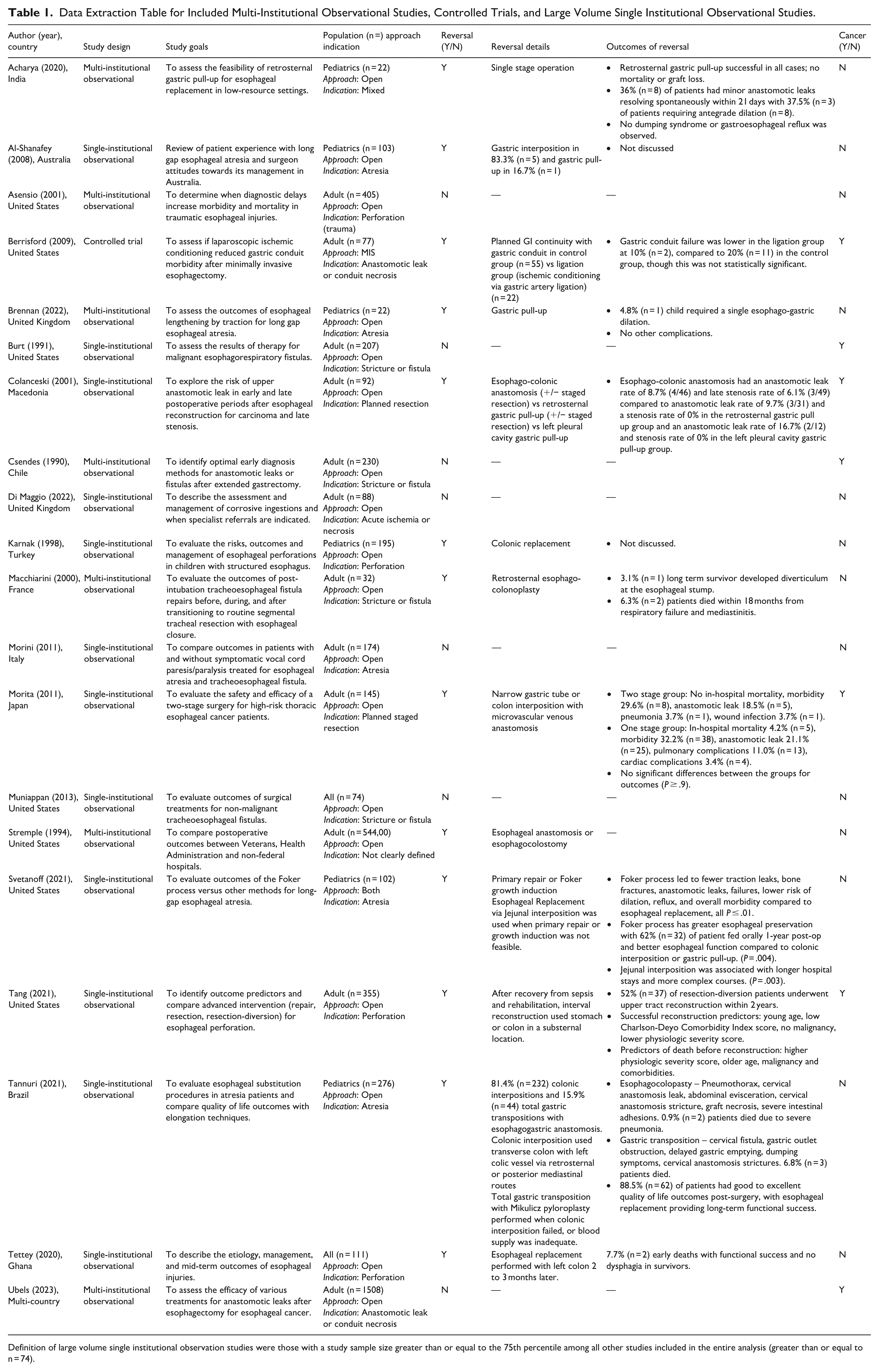
Definition of large volume single institutional observation studies were those with a study sample size greater than or equal to the 75th percentile among all other studies included in the entire analysis (greater than or equal to n = 74).
Ethics
Ethics approval was not required given that this study only utilized published data.
Results
Included Studies Characteristics
After removal of duplicates, 3659 abstracts from MEDLINE, EMBASE and CENTRAL were screened for eligibility. Of those abstracts screened, 231 studies from 217 authors in 43 countries were included in the final analysis (Supplemental Figure 1). By country, most studies came from United States of America (USA, 23.8%), followed by Japan (15.6%), India (10%), and the United Kingdom (UK, 7.4%) with several other countries with less than 10 studies. When exploring studies by geographical region, studies from East Asia were most frequent (32%), followed by North America (24.2%), and Western Europe (24.2%), North Africa and the Middle East (6.1%), Eastern Europe and Central Asia (5.6%), Latin America and the Caribbean (5.6%), and Sub-Sahara Africa (1.3%). Figure 1 outlines included studies by geographical region.
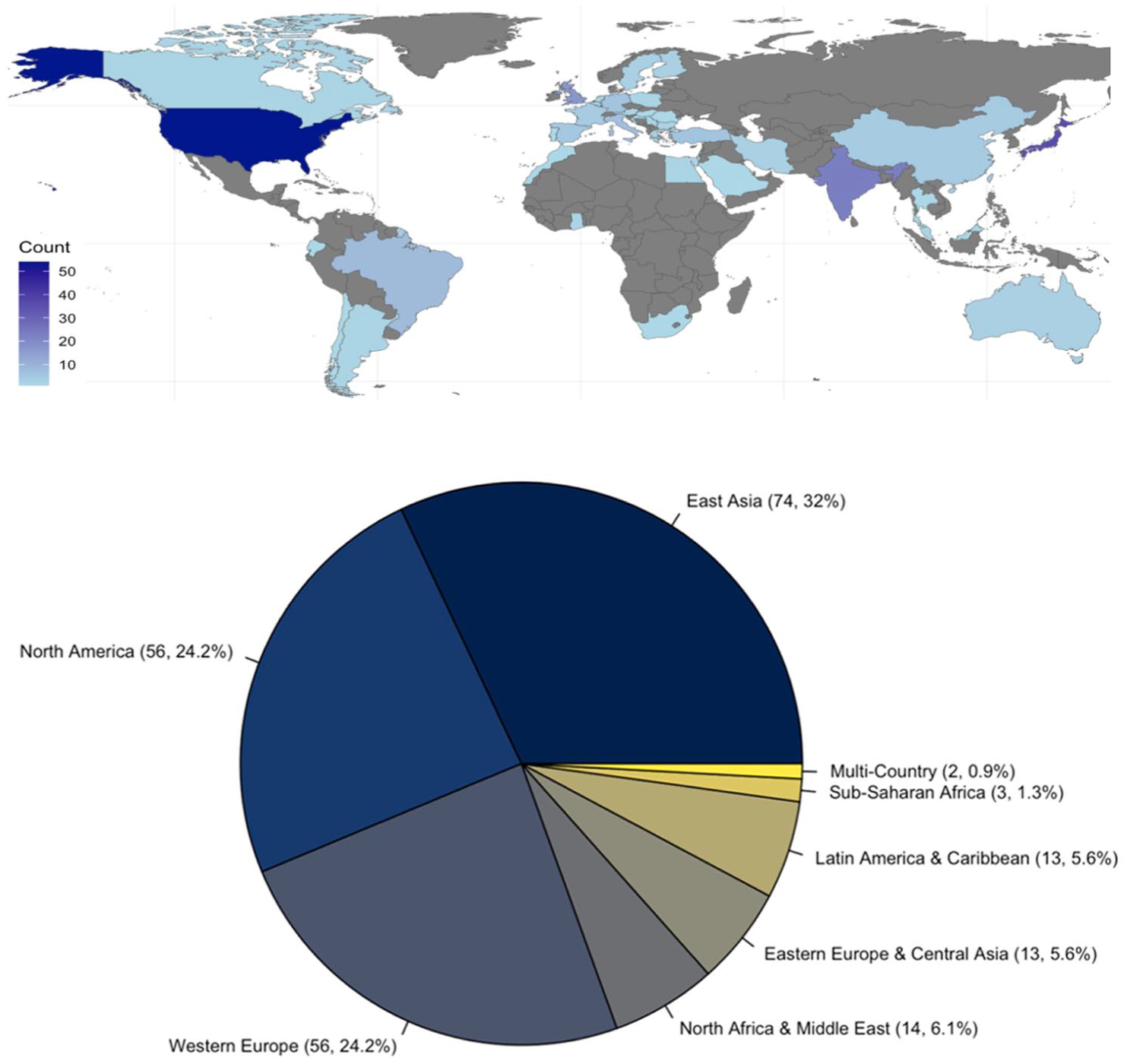
Studies by geographical region.
Studies were published from 1990 to 2023 with varying degree of frequency. Of the included studies, 150 (65%) were case reports, 62 (26.5%) were single-institutional observational studies, and 10 (4.3%) were reviews with few studies being multi-institutional observational or mixed methods studies. There was one clinical trial.
The median sample size of included studies was 1 with an interquartile range (IQR) of 1 to 19.5. When excluding case reports (restricting to n = 81 studies), the median sample size of included studies was 34 (IQR 17-74). Figure 2 outlines included studies by year and study design type. Supplemental File 1 outlines the data extraction file for all the included studies (n = 231).
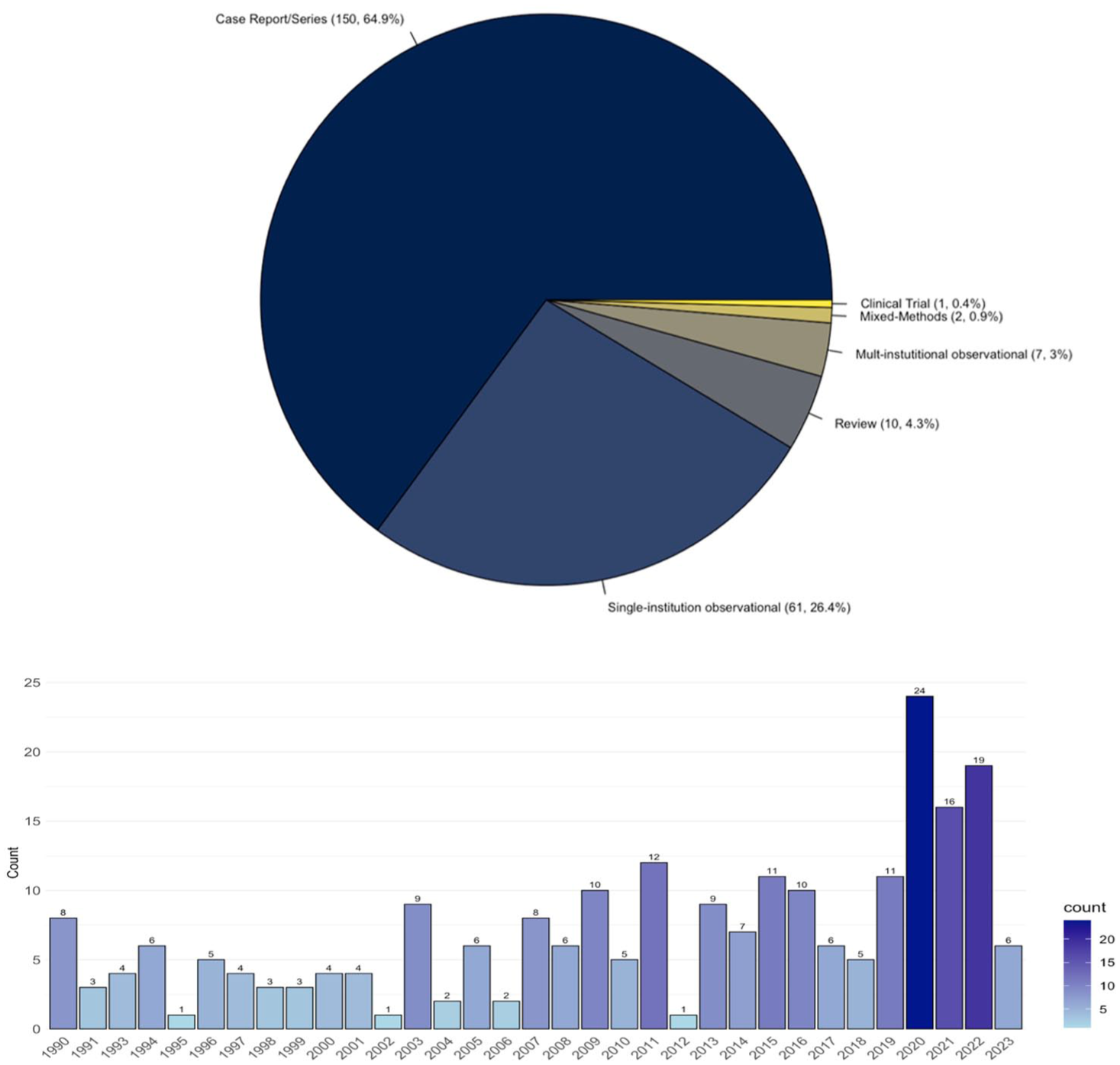
Studies by year and type.
Baseline Characteristics of Patients
Of the included studies, 67.1% of the patient population were adults, 29.4% were pediatric and the remaining studies (3.5%) had a mixed population. Most studies described an open procedure (87.9%) at the index procedure, with 9.5% describing a minimally invasive surgical (MIS) procedure at the index procedure (for example as minimally invasive esophagectomy or hiatal hernia repair) and the remaining 2.6% describing both. The indication for diversion and defunctioning was benign (example perforation) in most studies (75.8%), while fewer studies occurred in the oncologic setting.
Indications for Esophagostomy
Indications for esophageal discontinuity fell into nine broad categories across acute and elective settings in both the pediatric and adult population. In order of prevalence, indications were as follows: perforation (29%), stricture or fistula (21.6%), atresia (18.6%), anastomotic leak or conduit necrosis (7.8%), planned staged resection (7.8%), acute ischemia or necrosis (4.3%), mixed pathologies (3.5%), and other congenital malformation (2.2%). Moreover, 4.3% of papers were categorized as “other” which included indications such as end stage neuromuscular disorders, palliative esophagostomy among other miscellaneous indications.
Esophageal Reversal
Overall, 75.8% (n = 175) of studies described some version of a reversal procedure. Studies that reported reversal procedures consisted mostly of case reports (68.6%, n = 120) followed by single-institutional observation studies (22.9%, n = 40), and reviews (4.6%, n = 8). Among patients with esophageal discontinuity (n = 1184 patients), the rate of reversal was 79.8% (945/1184). Excluding patients who had esophageal discontinuity for atresia, the rate of reversal was 73.2% (517/706). Among patients with esophageal discontinuity for the indication of atresia alone, the rate of reversal was 89.5% (428/478).
Overall, 24.2% (n = 56) did not describe esophageal reversal. Among those studies, it was impossible to determine if reversal was planned for a later date or reversal simply never occurred. Studies that did not report reversal procedures consisted mostly of case report/case series (53.6%, n = 30) followed by single-institutional observational studies (37.5%, n = 21), multi-institutional observation studies (5.4%, n = 3), and reviews (3.6%, n = 2).
Reconstructive Strategies Discussed in the Literature
Reconstructive options varied significantly depending on the operation at index. In patients where there was no underlying resection and simple cervical esophagostomy was performed, many studies described either spontaneous closure or primary closure of esophagostomy over a nasogastric tube. In studies where underlying esophagectomy was performed, authors described reconstructive procedures involving either esophago-esophagostomy, gastric pull up, pedicled or free jejunal reconstruction (+/− microvascular anastomoses), or colonic interposition grafts. Several free flaps were described in the literature including myocutaneous free flaps, osteomyocutaneous free flaps, local skin flaps and pericardial / omental flaps. Supplemental Table 3 outlines reconstructive options in full detail.
Mapping of Studies by Geographic Region
Mapping of geographic region of origin onto esophagostomy indications and surgical approach revealed distinct patterns of variation globally. There was high frequency of stricture or fistulas in East Asia and high frequency of atresia in Western Europe. Perforation remained relatively consistent across various geographical regions. Figure 3 depicts a heat map of the etiology for cervical esophagostomy by world geographical regions. Moreover, it appeared that MIS was most predominant in East Asia, followed by North America and Western Europe. Supplemental Figure 2 depicts a heat map of surgical approach by world geographical regions.
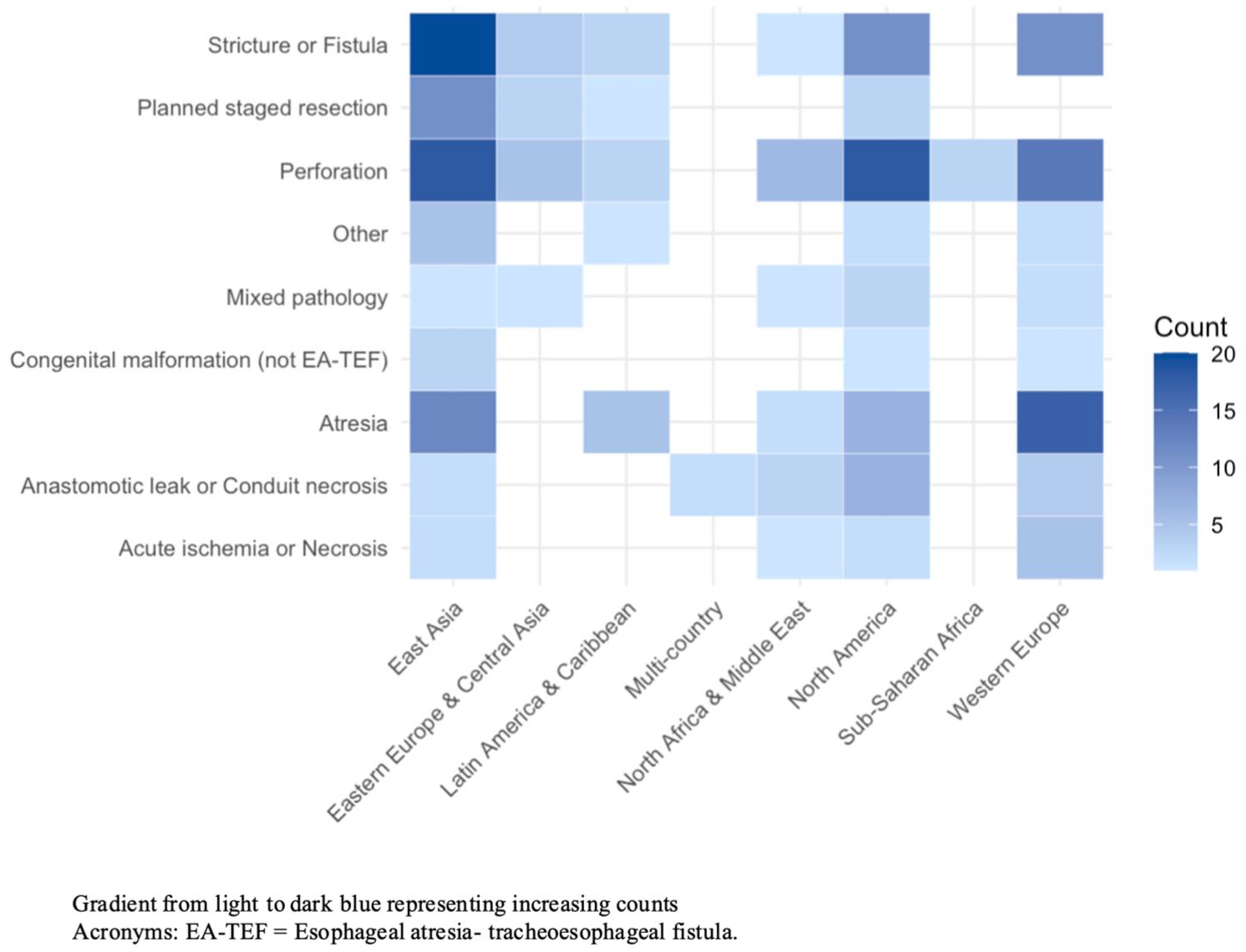
Heat map visually mapping etiology for cervical esophagostomy creation mapped on to regions in the world.
Subgroup Analysis: Adult Versus Pediatric Population
Recognizing the distinct difference between adult versus pediatric population, we explored outcomes stratified by adults (n = 155 studies) versus pediatric (n = 68 studies). In the adult population the indications for discontinuity (in order of prevalence) were as follows: perforation (35%), stricture or fistula (27%), anastomotic leak or conduit necrosis (11%), planned staged resection (11%), acute ischemia or necrosis (6.5%), and mixed pathologies (3%). Moreover, 6.5% of papers were categorized as “other” which included indications such as end stage neuromuscular disorders, palliative esophagostomy among other miscellaneous indications. Among adult patients with esophageal discontinuity (n = 631 patients), the rate of reversal was 72.1% (455/631).
In the pediatric the indications for discontinuity (in order of prevalence) were as follows: atresia (63%), perforation (13%), stricture or fistula (9%), congenital malformation (7%), mixed pathology (5%), anastomotic leak or conduit necrosis (2%), and planned staged resection (2%). Among pediatric patients with esophageal discontinuity (n = 524 patients), the rate of reversal was 89.9% (471/524).
Gaps in Literature
There are significant gaps within the literature that can be organized into geographical, clinical, and methodological/research gaps.
From a geographical perspective, there was severe lack of multi-institutional studies within the literature (n = 7 studies, 3%). Additionally, only two studies (0.9%) occurred across different countries. Lastly, there appeared to be a severe lack of studies from Eastern Europe and Central Asia and Sub-Saharan Africa.
From a clinical perspective, there were significant gaps in describing reversal strategies for patients left in discontinuity. This includes both describing intentions for reversal and follow through at a later date. Additionally, planned stage resection appeared to be a relatively underutilized strategy where only 7.8% (n = 18) described this approach. Furthermore, there appears to be a lack of uniform terminology to describe this patient population with significant variation in the terms used (Supplemental Table 1). Furthermore, there was a lack of studies outlining specific strategies for optimizations of reversal and description of reversal. Additionally, no studies systemically described and assessed nutritional and functional outcomes in this patient population. Lastly, despite 24.2% (n = 56) of studies occurring in the oncologic setting only 32.1% (n = 18) explored typical short or long-term oncologic outcomes such as surgical margin status, lymph node harvest, overall survival, disease-free survival or tumor recurrence.
From a methodological and research perspective, given that most studies were case reports, there was a significant lack of comparison groups in the literature. In a single arm study without comparison groups, authors were typically limited to inferences about one treatment modality and therefore, the literature was mostly descriptive. Furthermore, there is significant lack of clinical trials and prospective studies in the field. We noted only one clinical trial in the study whose aim was to evaluate the role of laparoscopic ischemic conditioning of the stomach prior to minimally invasive esophagectomy. In this study gastric-conduit-related complication requiring defunctioning cervical esophagostomy occurred in three patients and subsequent reversal rates were not discussed.
Discussion
In this scoping review, we examined the global landscape of esophageal discontinuity and reconstructive practices. We identified several key gaps within the literature including the lack of robust study designs to examine this patient population, lack of description of reversal procedures (including intent for reversal and subsequent follow through), significant heterogeneity in terminology used to describe this patient population, lack of prospectively collected high-quality data, and lack of description of long-term functional or disease-specific outcomes. Among studies reporting reversal of esophageal discontinuity, the overall rate of reversal was 79.8%. Excluding patients who had esophageal discontinuity for atresia, the overall rate of reversal was 73.2%. This finding indicates that in many cases reversal is feasible and achievable. Subgroup analysis highlight important clinical distinctions: pediatric cases were overwhelmingly driven by congenital malformations such as atresia, with high reversal rates, whereas adult cases more commonly arose from acute acquired pathologies (eg, perforation, stricture) and had lower reversal rates. These differences have direct implications for reconstructive planning, expected outcomes, and timing of reversal. Despite this, there is considerable heterogeneity in surgical approaches with limited data justifying one modality over another and no data comparing long-term outcomes of different strategies head-to-head. At present, there is no consensus recommendations on the management of patients with esophageal discontinuity. The findings from this scoping review are important as it is the first systematic survey of the literature to identify key gaps and priorities for future investigation.
We noted several key gaps with this scoping review from a geographical, clinical, and research perspective. To that end we have several suggestions. First, as a community, we should aim for cross-country collaboration to study this rare disease entity. This includes the creation and use of shared, longitudinal, cross-country data registry. Second, it is important to describe the technical aspects of reversal procedures in this population including the specifics of the conduit, surgical teams involved, and decision-making around timing of reversal for every case. Additionally, documenting timing of initial diversion is similarly important, 6 as studies seldom made explicit reference to the 24-hours rule for diversion from disease presentation, and no consistent temporal trends were observed over the study period.25 -27 This reinforces the need for future studies to systemically document timing from injury to intervention. Third, researchers should aim to develop a core set of quality outcomes for this patient population. This would involve developing both short and long-term functional and disease-specific outcomes. For example, it is critical to explore how to adequately assess nutritional and functional outcomes in this patient population. This approach would allow for more thorough comparison of long-term outcomes allowing for head-to-head comparisons of different treatment modalities. Finally, it is imperative to name this rare-disease clinical entity. We suggest the terminology foregut failure to represent the complex patient population who has been left in esophageal discontinuity with limited reconstructive options. After initiating these steps, in the future we may develop clinical trials that may more-specifically appraise reconstructive options to determine best-practices in management of this complex surgical patient population. Figure 4 outlines recommendations for surgeons, researchers, and health systems to consider for patients with foregut failure.
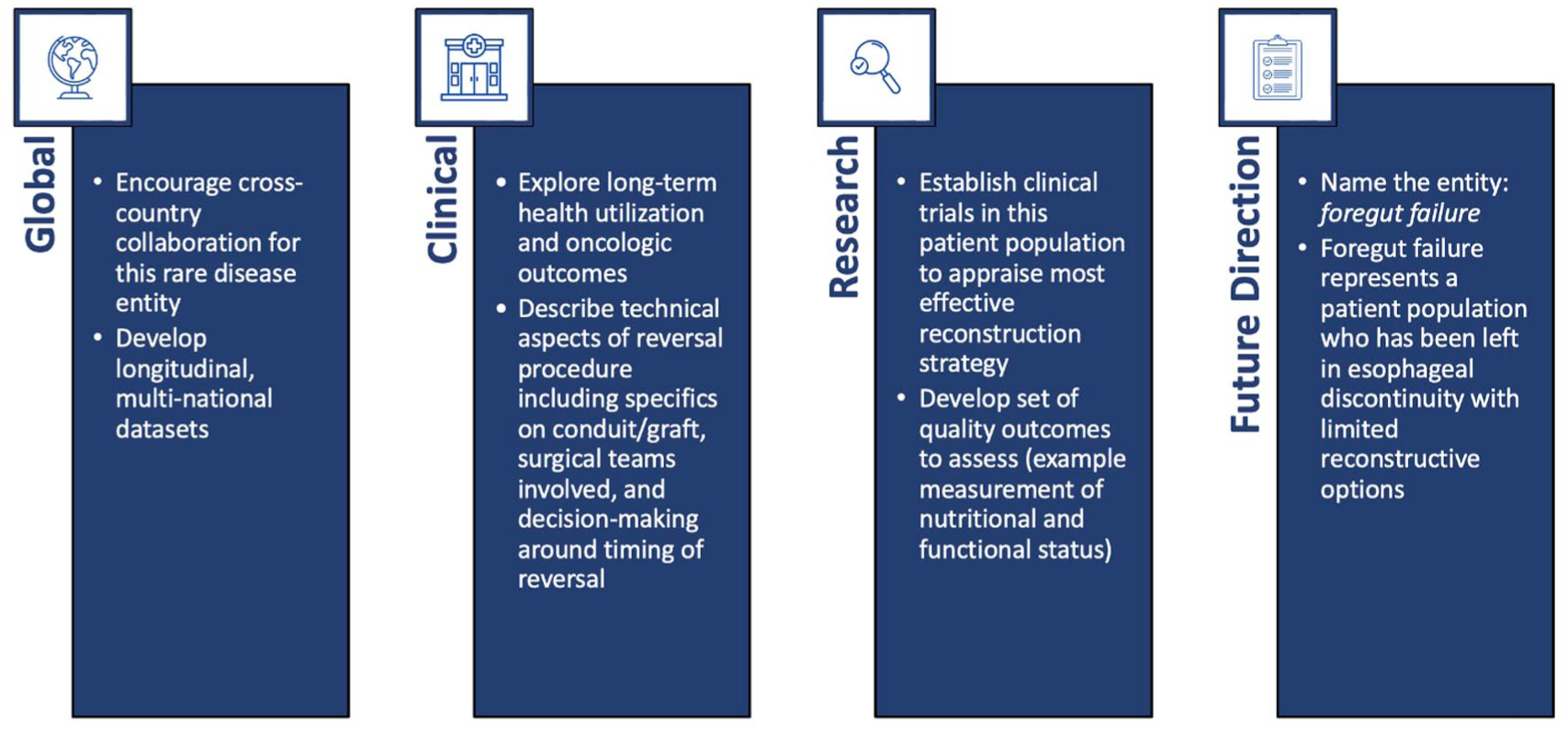
Recommendations for surgeons, researchers, and health systems to consider for esophageal discontinuity.
There are several challenges in this field that caused relative stagnation in surgical innovation relative to other areas in esophageal surgery.28 -30 First esophageal discontinuity is a low-volume, rare event. In this study we found the most common indication for cervical esophagostomy reported in the literature was from perforation. Esophageal perforation is rare disease itself with incidence estimates around 1 to 3 per 100 000 person-years.31 -33 Furthermore, those requiring surgical intervention from perforation are a small fraction of the entire population, and even smaller than that, are patients who would require esophageal discontinuity.3,32 Secondly, there are a number of surgical strategies to reconstruct including gastric, jejunal (+/− super-charged), and colonic interposition grafts.34 -37 These operations are usually multi-disciplinary, and given the rare incidence of this clinical entity, care providers almost always have a low-volume of cases and limited experience with the necessary procedure. Finally, these are complex patients with multiple considerations at the time of reconstruction including their underlying hemodynamics, short and long-term nutritional status, functional status, and oncologic considerations. 35 All of these factors make systematically studying this population uniquely challenging. For example, this review noted the number of case studies (n = 150 studies, 65%) far outweighed multi-institutional observational studies (n = 7 studies, 3%). Moreover, the median sample size of patients in included studies in this review was 1 (IQR 1-19.5). When excluding case reports, the median sample size increased to just 34 (IQR 17-74). This points towards systematic challenges in the generation of high-quality, robust, generalizable data that can make meaningful inferences about best practices for managing this challenging clinical entity.
Despite the challenges of studying and caring for this patient population, there are lessons to be learned from other rare-disease entities that can be applied in our patient population. For example, pediatric intestinal failure is a rare disease that represents an evolving field in pediatric surgery, gastroenterology and transplantation.38 -40 Once a uniformly fatal disease entity, pediatric intestinal failure is now a potentially survivable syndrome due to increase awareness, systematic attempts to improve the body of evidence, and multidisciplinary care teams.38,41,42 This disease entity has previously suffered from some of the challenges noted in patients with esophageal discontinuity such as the body of evidence confined to small sample size single-center reports, leading to challenges in data interpretation and significant knowledge gaps. 43 However, focused international collaboration has led to the creation of the International Intestinal Failure Registry, a large multicenter prospective data registry that started in 2018 which since as of May 2023, includes 362 children from 26 centers worldwide. 43
As a first step to counteract the challenge of studying this patient population, we suggest establishing the nomenclature of patients with foregut failure to represent patients who have been left in esophageal discontinuity with limited reconstructive options. Establishing this nomenclature is a first step to create a unified and systematic effort in managing patients who suffer from this disease by creating a shared language amongst providers who care for this patient population. The ultimate goal is to develop a comprehensive clinical and research program with shared resources and strengthened knowledge base. Furthermore, gaining a comprehensive understanding of the foregut failure patient population may give rise to novel interventions for patients with lack of reconstructive options such as gastrointestinal allografting which has been utilized in the pediatric intestinal failure population. 39
There are limitations to this study. First, to limit our overall search to a reasonable count (approximately 5000 abstracts to screen) we limited our search from 1990 onward. It is possible that papers published prior to 1990 may be of interest for this literature search, however this scoping review was focused on the body of evidence within the contemporary period for patients with esophageal discontinuity.
Secondly, there is significant variation in terminology to represent esophageal discontinuity with cervical esophagostomy at the time of the index operation (ie, esophageal diversion, exclusion, cervical esophagostomy, cervicostomy, spit-fistula, etc.). Although it is possible that not all studies of interest were identified, the inclusion criteria for this review, which was developed with the assistance of a health sciences librarian, was kept intentionally broad to capture a large breadth of papers in the thoracic, otolaryngology – head and neck surgery, plastic surgery, and general surgery disciplines.
Third, the reported overall rate of reversal of 79.8% and rate of reversal excluding atresia of 73.2% should be interpreted with some caution. This scoping review found that 24.2% (n = 56) did not include any details of reversal. Therefore, it is unknown if reversal never occurred or simply was not reported. Furthermore, these patients may have also had early mortality which would result in an over estimation of reversal rate in the remaining cohort of patients who survived (survival bias). For this reason, that is why we recommend investigators published all aspects of decision making for patients left in continuity with explicit mention of plan for reversal, specifics of the conduit, surgical teams involved and decision-making around timing of reversal.
Finally, given the search strategy, patients who have been left in discontinuity without cervical esophagostomy were not identified. Although this patient population may be of interest and represent an important patient population for evaluation of foregut failure in the future, this population would be challenging to identify from a search strategy perspective. Therefore, here we have coined the term foregut failure as an important nomenclature to represent the complex patient population who have been left in esophageal discontinuity with limited reconstructive options that may be used to develop robust and comprehensive clinical and research program to strengthen our knowledge base and improve outcomes for patients with this rare disease.
Conclusion
Significant gaps exist in the current literature surrounding esophageal discontinuity and cervical esophagostomy including a lack of multi-institutional studies, prospective datasets, and randomized clinical trials. Additionally, reporting of reversal procedures and long-term outcomes such as nutritional and functional outcomes remain inconsistent.
To advance the field, we advocate for international collaboration in developing shared data registries and defined short- and long-term quality outcome measures. Finally, we propose the term foregut failure to describe this complex patient population – those with disrupted foregut continuity and limited reconstructive options. Establishing unified terminology is a necessary step toward building a collaborative research framework and improving clinical care for these rare but high-risk patient population.
Supplemental Material
sj-docx-1-gut-10.1177_26345161251378419 – Supplemental material for Exploring the Landscape of Esophageal Discontinuity Procedures and Cervical Esophagostomy in the Modern Era: A Scoping Review
Supplemental material, sj-docx-1-gut-10.1177_26345161251378419 for Exploring the Landscape of Esophageal Discontinuity Procedures and Cervical Esophagostomy in the Modern Era: A Scoping Review by Adom Bondzi-Simpson, Hassan Momoh, Khadija Brouillette, Harsukh Benipal, Andreea C. Matei, Gursharan K. Sohi, Jonathan Yeung and Elliot Wakeam in Foregut
Supplemental Material
sj-xlsx-2-gut-10.1177_26345161251378419 – Supplemental material for Exploring the Landscape of Esophageal Discontinuity Procedures and Cervical Esophagostomy in the Modern Era: A Scoping Review
Supplemental material, sj-xlsx-2-gut-10.1177_26345161251378419 for Exploring the Landscape of Esophageal Discontinuity Procedures and Cervical Esophagostomy in the Modern Era: A Scoping Review by Adom Bondzi-Simpson, Hassan Momoh, Khadija Brouillette, Harsukh Benipal, Andreea C. Matei, Gursharan K. Sohi, Jonathan Yeung and Elliot Wakeam in Foregut
Footnotes
Author Contributions
AB-S, HM, HB, and EW conceived the idea, developed the research questions and study methods and drafted the initial protocol. AB-S, HM, HB, KB and ACM conceived and executed the search strategy. AB-S, HM, KB, HB, ACM, GKS, JY, and EW contributed meaningfully to the editing, revising, and critical review of this protocol and the final approval of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval is not required for this manuscript.
Use of Artificial Intelligence
No artificial intelligence (AI) was used in the preparation of this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.