
Abstract
Esophageal squamous cell carcinoma (ESCC) is a leading cause of death worldwide, particularly prevalent in Southern and Eastern Africa, and central Asia. Initial studies identified various factors associated with an increased risk of ESCC, leading to subsequent research investigating the underlying biological mechanisms. This narrative review aims to summarize the role of risk factors in ESCC development and propose future research directions. A systematic literature search was conducted using EMBASE, MEDLINE/PubMed, and CENTRAL databases to identify relevant publications. Included studies updated the epidemiology of ESCC, including the incidence, prevalence and mortality and its variations globally. We reported on socio-demographic impact on these geographic variations. We, then, focused on identifying risk factors associated with ESCC. The identified risk factors were categorized into 5 subcategories: smoking, alcohol, dietary factors, environmental factors and infection. Each subcategory’s risk factors were summarized and explored, providing geographical links for these associations. The review emphasizes the current understanding of several risk factors for ESCC, and specifically makes geographical links, and potential explanations for their associations were explored. However, further research is essential to validate these findings and gain insights into their impact on tumor biology.
Introduction
Esophageal squamous cell carcinoma (ESCC) is an aggressive condition that ranks eighth in incidence and sixth in mortality amongst all malignancies worldwide. Its burden varies greatly across countries and populations. 1 Despite numerous advances in diagnosis and treatment, mortality from esophageal cancer remains high, with 5 years survival after diagnosis at only 10%–30%. Previous studies have captured a clear geographic variation in the distribution of ESCC globally, and have linked this trend to pre-disposing risk factors such as diet, environmental factors, infections and smoking. 2 Subsequent work then proposed mechanisms to explain these relationships at a molecular level and characterized interactions between various risk factors. Previous work has covered the updated epidemiology of esophageal cancer of both squamous cell and adenocarcinoma histological subtypes. 3 Our group has previously summarized the risk factors and their underlying mechanisms in ESCC. 4 In this review, we aim to provide an update on the epidemiology of ESCC and map these to risk factors where there is a strong geographical link to the histological subtype.
Methods
Search
We performed a search of the literature using following electronic databases: MEDLINE/PubMed (1966 to May 2023), EMBASE (1980 to May 2023), and the Cochrane Central Register of Controlled Trials (CENTRAL) from The Cochrane Library (2023) on the 18th of May 2023. The search strategy for this review was constructed for each database by using a combination of medical subject headings (MeSH) and free-text terms. Reference lists of selected articles were also examined to identify relevant studies that were not identified in the database searches. In addition, the World Health Organization International Clinical Trials Registry, ClinicalTrials.gov, ISRCTN Register and PROSPERO were searched to identify ongoing and unpublished studies.
Study Selection
The inclusion criteria were studies describing and evaluating the strength of association of risk factors within ESCC. We included all studies that evaluate the role of epidemiological characteristics such as age, sex and socio-economic status. All randomized controlled trials (RCTs) and observational studies, adult only studies, human studies, English studies, and studies where the patients had ESCC were included. The exclusion criteria were pediatric studies, non-human studies, non-English studies, non-ESCC studies, case series, case reports, editorials, conference abstracts and opinions. One author (SC) independently reviewed all studies identified by the search strategy. After removing duplicates, the titles and abstracts of the studies were screened for inclusion using Covidence software (1). Where there was uncertainty from the study abstract, the full paper was assessed for relevance.
Data Extraction
Data was extracted from the included studies using an electronic data extraction spreadsheet. This included study design, sample size, epidemiological details (age, sex, socio-economic status), risk factor being studied and effects of risk factors, where available. The primary outcome was identifying risk factors associated with ESCC. Risk factors were divided into 5 subcategories: smoking, alcohol, diet, infection, and environmental risk factors.
Results
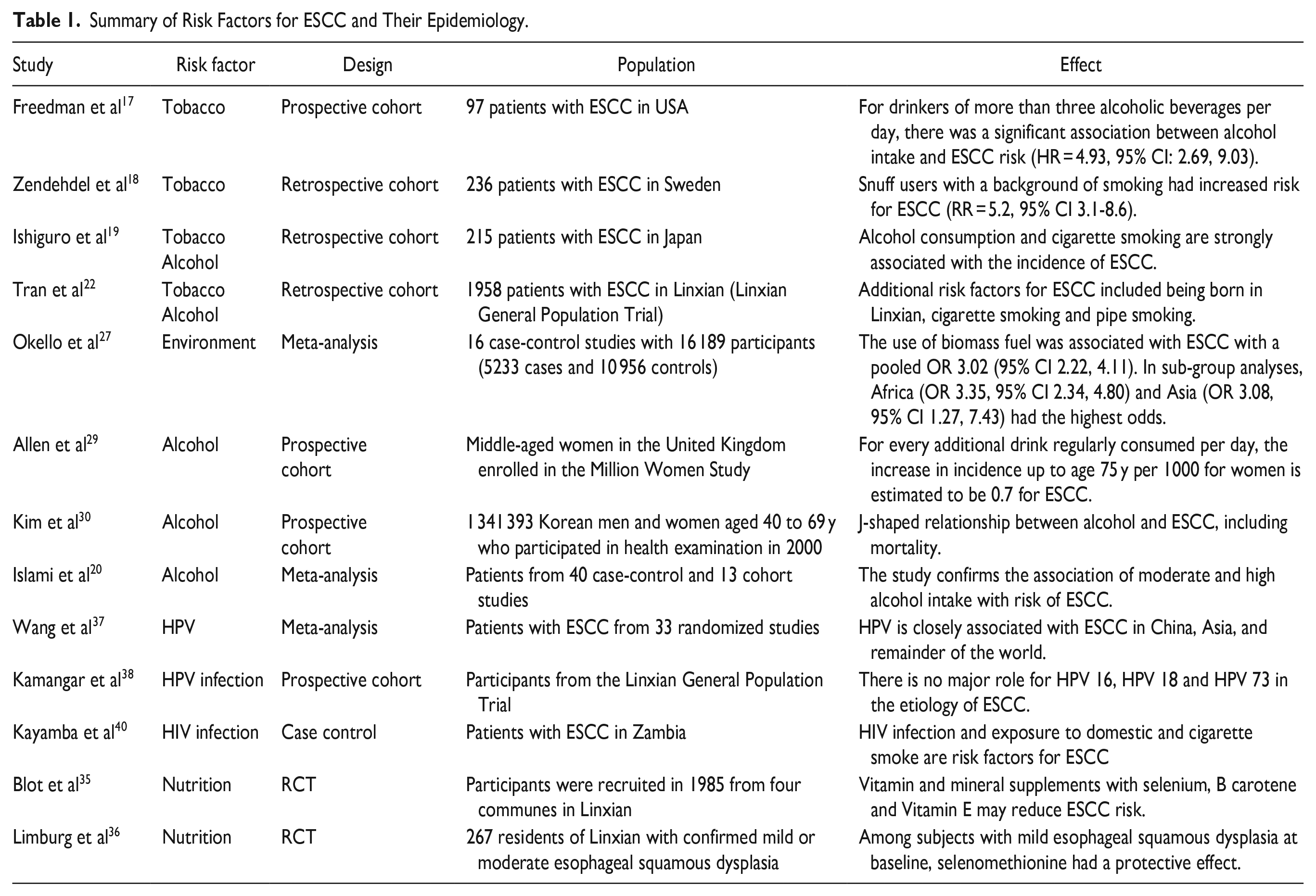
The literature search identified 971 studies. After removing duplicates, 654 abstracts were assessed for eligibility. Following abstract screening, 432 studies were excluded based on title and abstract relevance. Of the remaining articles, we used 38 studies in our review. PRISMA flowchart summarizing the search strategy is demonstrated in Figure 1. All included studies were observational studies, RCTs or meta-analyses. Of these studies, 8 were on tobacco and smoking; 4 on environmental factors; 4 on alcohol; 6 on dietary factors and 5 on infections. The remainder of the included studies provided other general epidemiological details. A summary of the identified risk factors associated with the development of ESCC is presented in Table 1.
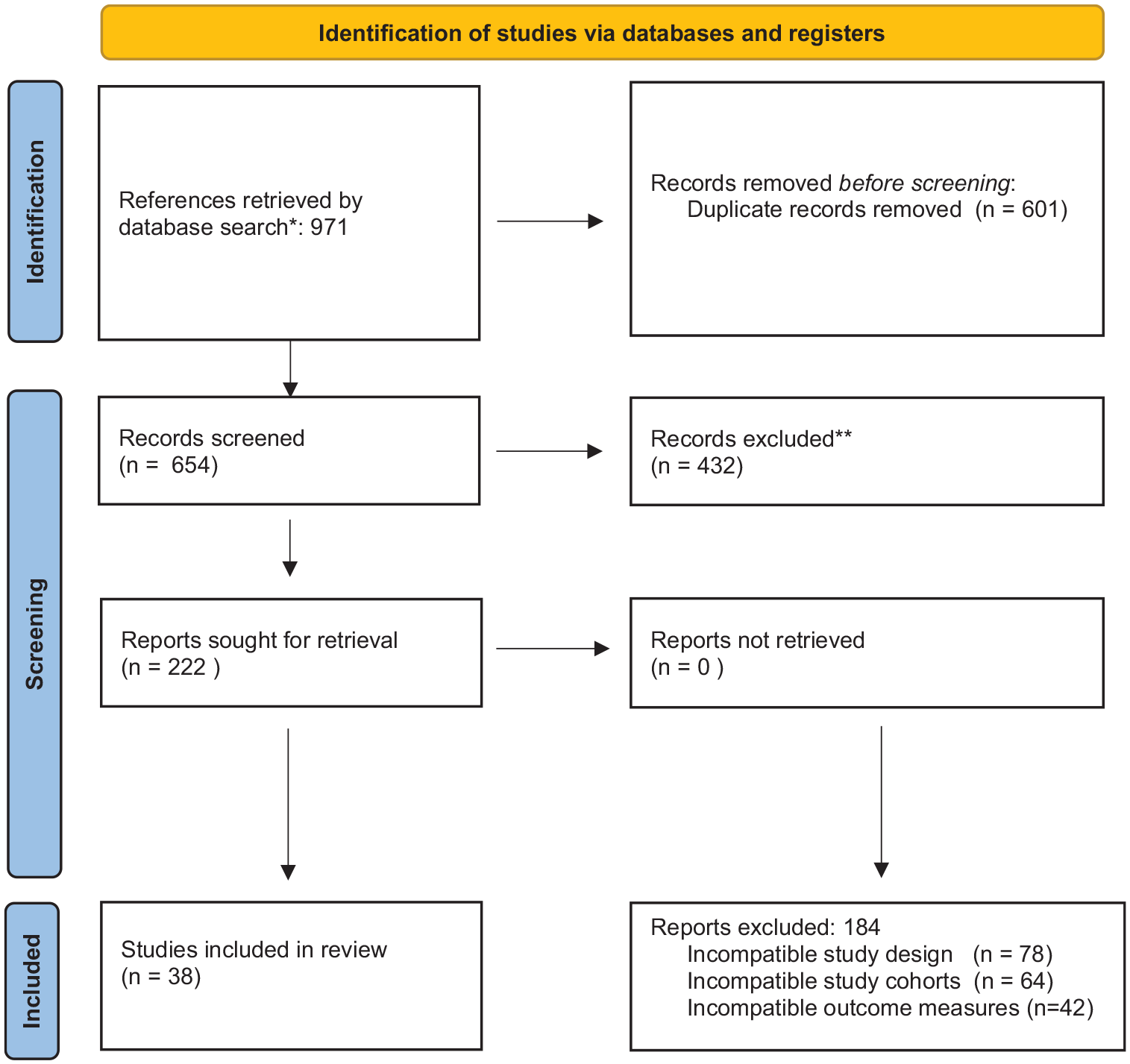
PRISMA flowchart summarizing study selection.
Summary of Risk Factors for ESCC and Their Epidemiology.
Discussion
Incidence and Geographical Variations
In 2012, the International Agency for Research on Cancer (IARC) estimated approximately 450 000 cases of esophageal cancer, of which 88% cases of were ESCC. 1 The report also highlighted the significant variation in the geographical distribution of ESCC, including 3 different belts of high incidence based on previous epidemiological studies. The first region recording the highest incidence extends from Eastern to Central Asia, while the second region stretches along the Indian Ocean coast of Africa along the Great Rift Valley. 5 The third area involves the entire Gaucho Region of the South America, specifically Uruguay.6,7 The incidence of ESCC had been decreasing in Australia, Europe, Europe and other Western nations. 8 In Eastern Europe, Japan, South America, Asia and Sub-saharan Africa, ESCC is still the predominant subtype. 9
Although the incidence of EAC has been increasing for decades, the updated GLOBOCAN study still records ESCC as the dominant histological subtype in 21 mostly highly developed countries, including Australia, Canada, and several countries in Northern and Western Europe (Figure 2).10,11 As a result, the distinct regional differences in incidence have remained static between the 2 subtypes, with EAC incidence rates highest in Northern Europe and North America and ESCC rates highest in Eastern and South Central Asia and South Africa. 11 Within countries, there can also be significant differences in the incidence of ESCC. China accounts for nearly half the cases of ESCC globally, but the majority of these can be accounted for in certain hotspots. The rates of esophageal cancer can vary 10-fold, with stark differences over short geographic distances. 12 For example, in the North Central Taihang Mountain range, the incidence often exceeds 125/100 000, making it the leading cause of mortality in the region. 13 Such variations can be explained by evaluating the environmental and population-level factors such as lifestyle and habits of the population.
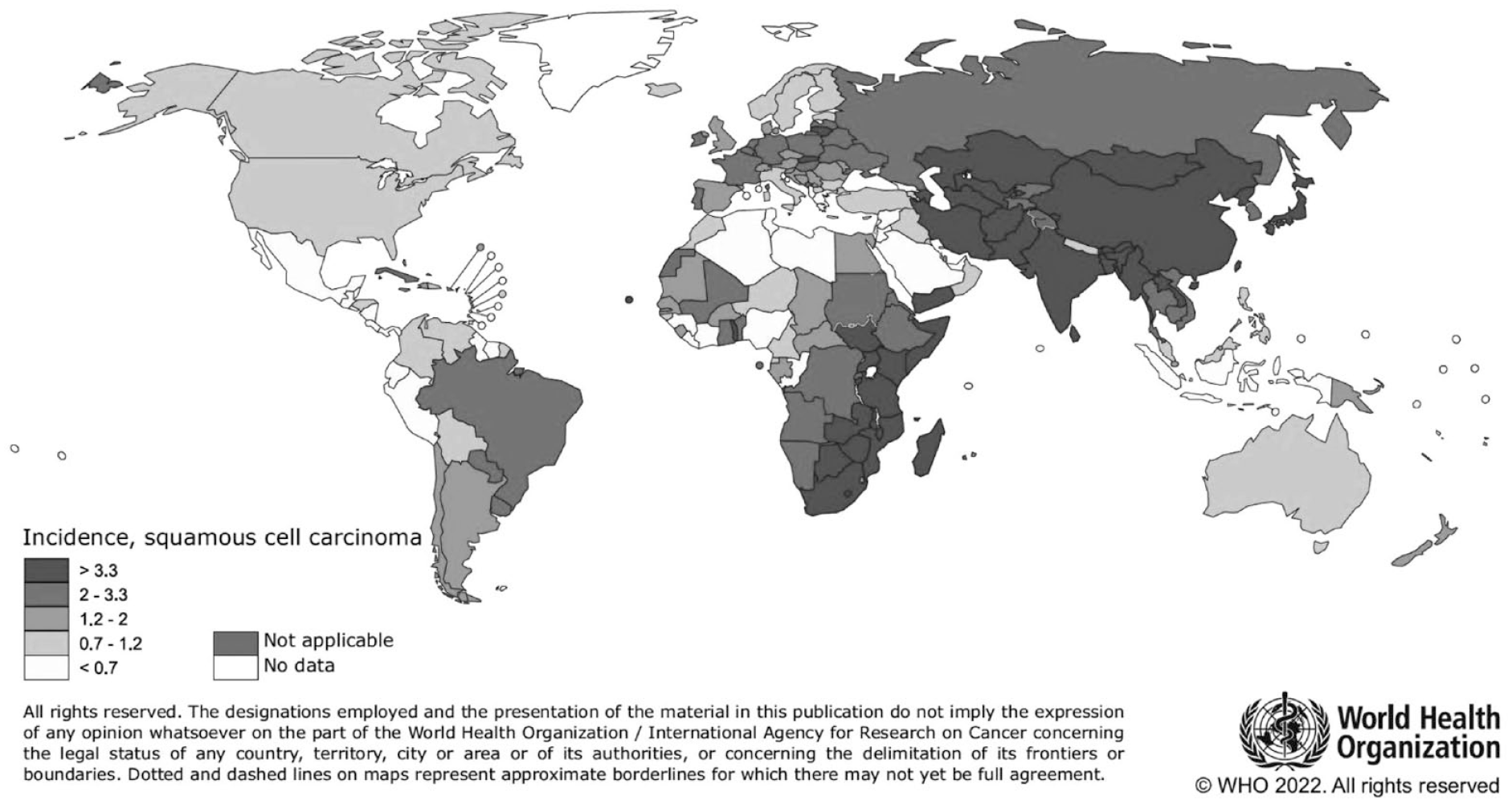
Worldwide esophageal AC and SCC incidence rates (age-adjusted according to the world standard population, per 100 000) in 2020. The image is taken from the publication of the GLOBOCAN study on ESCC. 11
Impact of Socio-Demographic Characteristics on Geographical Variations
ESCC is more generally common in men than women, with the ratio being 4:1 in low-risk areas like the United States and as low as 1:1 in high-risk areas like China and Iran. In a few places in the north east Africa and Middle East, the incidence is higher in women than men. This is likely due to higher prevalence of risk promoting behaviors such as smoking and heavy alcohol consumption in men than women, although further work is necessary to explain this relationship. In less homogenous ethnic populations, there are also variations between races and ethnicities. Histological type, cancer stage, tumor grade, and other clinical features have been found to differ significantly between ethnic/racial groups in United States. 14 For example, African-Americans are 7 times more likely to be diagnosed with ESCC, while White Caucasians are 4 times more likely to develop EAC. 9 In another analysis of49 766 patients from the SEER database, Chen et al reported that 85.5% of the black group and 75.4% of the Asian group had ESCC. 15 Overall, the incidence of ESCC in different ethnicities decreased since 1973, and although this drop was steepest for black males, it was still higher than all other groups.
Risk Factors
Smoking
Tobacco smoking and chewing are known risk factors for ESCC. 16 More importantly, with some studies reporting smokers at 3 to 9 times higher risk of developing ESCC compared to non-smokers, they are also likely to be the biggest modifiable risk factor of ESCC.17-19 Both high intensity and long duration are strong risk factors for ESCC. An increase in risk of SCC is associated with cigar and pipe smoking, although the magnitude of risk is less than with cigarettes. Interestingly, this magnitude of elevated risk has only been shown in economically developed countries, while a weaker risk ratio of 1.5 has been observed in economically developing countries.20,21 For example, Engel et al estimated a population-attributable risk of 89% in the US, while a larger cohort study by Tran et al in China found a weak association between tobacco smoking and ESCC.16,22 In the Shanghai Cohort Study, Chinese smokers were comparably exposed to less tobacco-specific nitrosamines than US smokers. 23 Given nitrosamines are the major carcinogens driving the tumorigenesis process, this may explain the discordance in the magnitude of smoking as a risk factor between economically different countries.
Environmental factors
Environmental factors contribute to the geographical variation in ESCC rates. Research on environmental risk factors has primarily hypothesized that an imbalance of trace elements in the soil could potentially contribute to the risk of ESCC. For example, in the high incidence areas of South African, the soil has lower concentrations of manganese, iron, magnesium, and sodium. 24 These regions are recognized for their eroded sedimentary soils known as “Beaufort Soils.” 25 Similar observations were made regarding the soil along the southern shores of the Caspian Sea in Iran, which also has high rates of ESCC. 26 In these areas, mineral levels such as boron, molybdenum, zinc, and copper were found to be low, while heavy metal levels, such as lead, tended to be excessive. Furthermore, a comparative analysis of soil composition in Africa and Iran revealed significant similarities. The results confirmed a correlation between ESCC risk and soils with high potential, elevated organic matter content, and low subsoil pH values. Solid biomass fuels from wood, charcoal, coal and crop residues are the primary source of fuel in poorer communities in Africa, Asia, and South America. These biomass fuels produce polycyclic aromatic hydrocarbons during their combustion and may be the mechanism underlying the higher risk for ESCC, as shown by a meta-analysis of 16 case-control studies. 27 Thus, populations may also be at risk of ESCC due to external environmental factors that directly lead onto affect other related risk factors such as diet and lifestyle.
Alcohol
Both the IARC and World Cancer Research Fund have established alcohol as a causative risk factor for ESCC. 28 Alcohol is metabolized into acetaldehyde, which is a class I carcinogen and may mediate tumorigenesis. Even though alcohol intake is strongly associated with ESCC in most studies, most studies, including the Million Women Study, have corroborated a J-shaped relationship, where the risk is decreased at low alcohol intake (<70 g/wk) but raised at high alcohol intake (>150 g/wk). 29 Similar to smoking, large scale epidemiologic studies have confirmed that alcohol consumption is risk factor in both economically developing and developed areas, although their carcinogenic effects vary with degree of consumption. The risk is higher at 1.6 to 5.3-fold in Asian countries such as China, India, Iran and Japan, and threefold in Africa and South American. 30 However, the risk is actually even higher in areas with lower rates of ESCC. For example, the highest risk is seen at sixfold in Europe and ninefold in North America. 31 Hence, specific drinking patterns including type of alcohol and exposure need further examination.
Diet
Many studies conducted in various locations and utilizing different research designs have investigated the potential associations between diet, specific foods, beverages, or nutrients and the risk of ESCC. For example, pickled vegetables were a staple of the diet in numerous households residing in high-risk regions of China, and they were consumed for 9 to 12 months annually.3,32 The process of pickling vegetables has the potential to produce mycotoxins and N-nitroso compounds. 33 Based on the assessment conducted by an IARC Working Group, there is some evidence from human studies to substantiate the claim that pickled vegetables have carcinogenic properties. Furthermore, a meta-analysis indicated that the consumption of pickled vegetables was associated with a twofold increase in the risk of ESCC, as reported by several studies included in the analysis. 34 Micronutrients such as vitamin A, retinol, thiamine, riboflavin, calcium, iron, zinc, pro-vitamin A carotenoids, or β-cryptoxanthin may also contribute to development of ESCC. For example, the Nutrition Intervention Trial recorded high rates of nutritional deficiencies in the region of Linxian, China. 35 At 10 years follow-up, supplementation with selenium, β-carotene, and α-tocopherol had reduced ESCC-related deaths by 17%, especially in those aged above 55. In another trial, Limburg et al showed that selenium supplementation also increased regression in subjects with mild esophageal squamous dysplasia. 36 In Uruguay and the Gaucho Region of South America, ESCC is especially prevalent amongst individuals who consume large quantities of a beverage called mate, which is traditionally served at high temperatures. More recently, studies in Iran and Tanzanian cohorts with high ESCC rates showed that beverages were consumed at temperatures as high as 700C.
Infections
There is a degree of overlap between the epidemiology of ESCC and prevalence of certain infections, specifically Human Immunodeficiency Virus (HIV) and Human Papillomavirus (HPV). Unlike adenocarcinoma of the esophagus, where Helicobacter pylori is a well-established causative agent, the relationship between infectious agents and the risk of ESCC is not well-understood. In their meta-analysis, Wang et al showed a close relationship between HPV infection (types 16 and 18) and ESCC in Africa and Asia. 37 By integrating into the host genome in ESCC cases, the virus leads to the expression of onco-proteins, namely E6 and E7. The E6 protein facilitates cell proliferation by promoting the degradation of the p53 protein, while the E7 protein disrupts the interaction between Rb and E2F, causing the release of E2F factors in their transcriptionally active forms. The combined actions of these proteins result in enhanced cellular proliferation, contributing to the development of ESCC. However, subsequent work has failed to confirm this association.38,39 In sub-Saharan Africa, there is a significant burden of HIV, which frequently coexists with HPV infection. A case-control study revealed that HIV infection independently increased the risk of ESCC, and this effect was observed irrespective of HPV status. 40
Conclusion
ESCC incidence has been decreasing in many Western countries, primarily attributed to reduced tobacco consumption and a decrease in heavy alcohol consumption. Despite this decline, ESCC continues to be a significant cause of cancer-related mortality on a global scale. This review emphasizes the current understanding of epidemiology and risk factors associated with ESCC. However, further research is necessary to validate these findings and examine their effects on tumor biology.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.