
Abstract
Esophageal cancer is amongst the most common types of cancer in Asia. It is a deadly disease where incidence almost parallels mortality. It is of 2 major subtypes, adenocarcinoma being more common in the global north and squamous cell carcinoma being more common in the global south. China, Japan, India, Iran, and other Asian countries contribute to roughly 80% of the global disease burden. Fortunately, esophageal squamous cell cancers (ESCC) are also amenable for screening. Natural history studies have shown that severe dysplasia carries the highest risk of progression to ESCC. Early detection has shown to be extremely beneficial, with cure rates above 90% for precursor lesions and early-stage esophageal cancer. There are various modalities available for screening—Chinese balloon cytology is a low cost technique that can be applied for mass screening but has only moderate sensitivity (39%-62%). Recent studies have demonstrated that using methylated DNA markers and applying artificial intelligence technology can significantly improve the yield of cytology. Lugol’s chromo-endoscopy has been demonstrated to have good sensitivity and specificity (>85%), but is an invasive technique and requires operator expertise. Other image enhancing techniques such as narrow-band imaging, autofluorescence, endocytoscopy and micro-endoscopy are promising, but currently not cost effective for mass screening. There are 3 large randomized trials underway in China, initial published results have demonstrated a detection rate between 0.7% to 1.2% for ESCC and 4% to 6% for pre cursor lesions. These trials, with some of them involving >100 000 patients have demonstrated the feasibility of endoscopic screening, but long term results are awaited.
Introduction
Esophageal cancer is a dreaded malignancy, where the mortality parallels its’ incidence, with esophageal cancer being the eighth most common cancer worldwide and the sixth most common cause of cancer related mortality. 1 It accounted for 3.1% of all solid tumors and 5.5% of cancer related deaths internationally. 2 There has been a consistent increase in the incidence of esophageal cancer worldwide. As per GLOBOCAN predictions based on current trends, there is a likely to be around 60% increase in esophageal cancer incidence by 2040 as shown in Figure 1.2-4
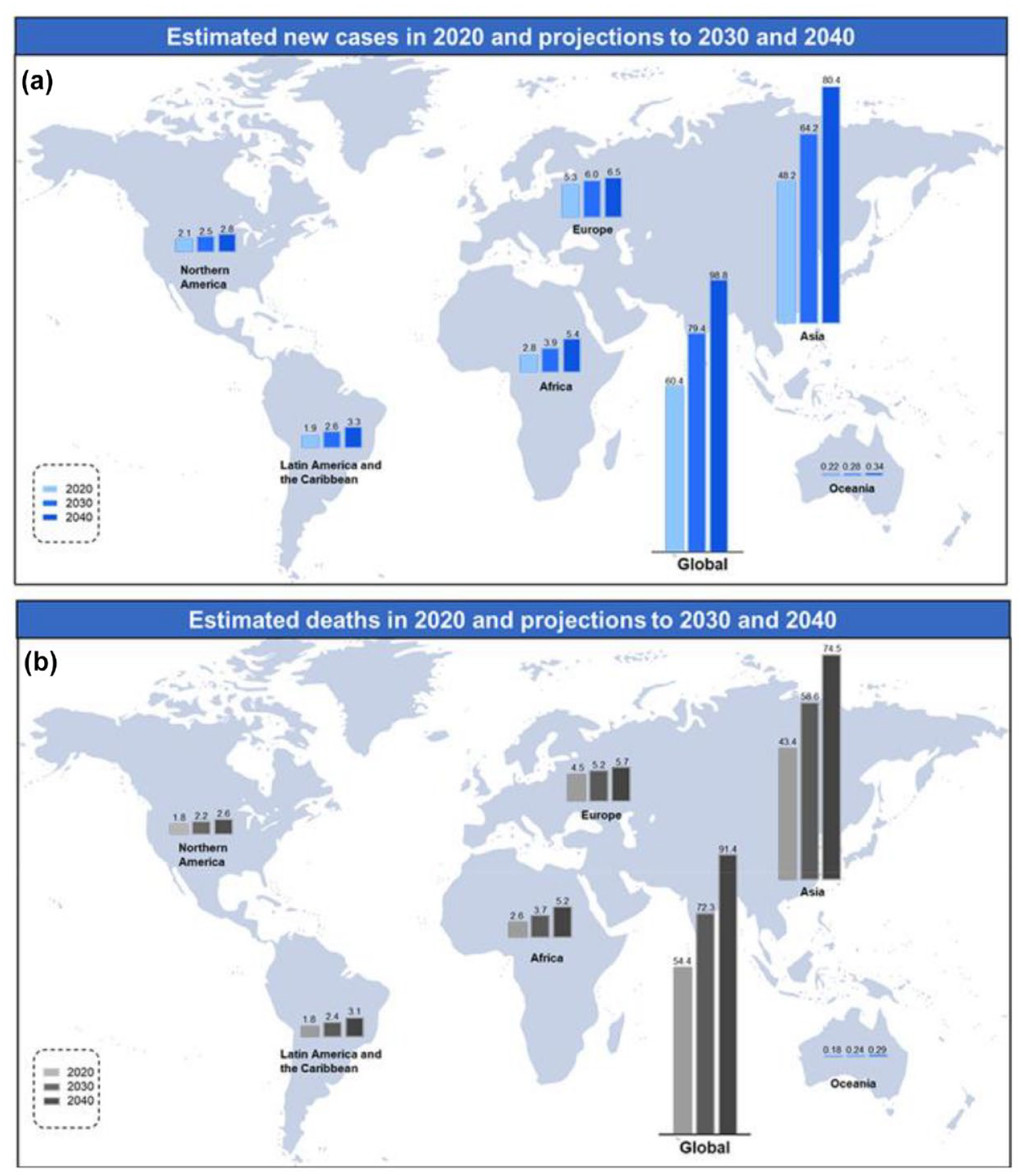
Global projections for 2040 continent wise: (a) estimated new cases in 2020 and projections to 2030 and 2014 and (b) estimated deaths in 2020 and projections to 2030 and 2040. (Borrowed with permission from Prof. Pengfei Xu). 4
Esophageal cancer is predominantly of 2 histological types—squamous and adeno carcinoma. Other histological types are relatively rare. World over 604 100 cases of esophageal cancer were diagnosed in 2020, with approximately 80% of cases being contributed by Asian countries as shown in Figure 2. 1
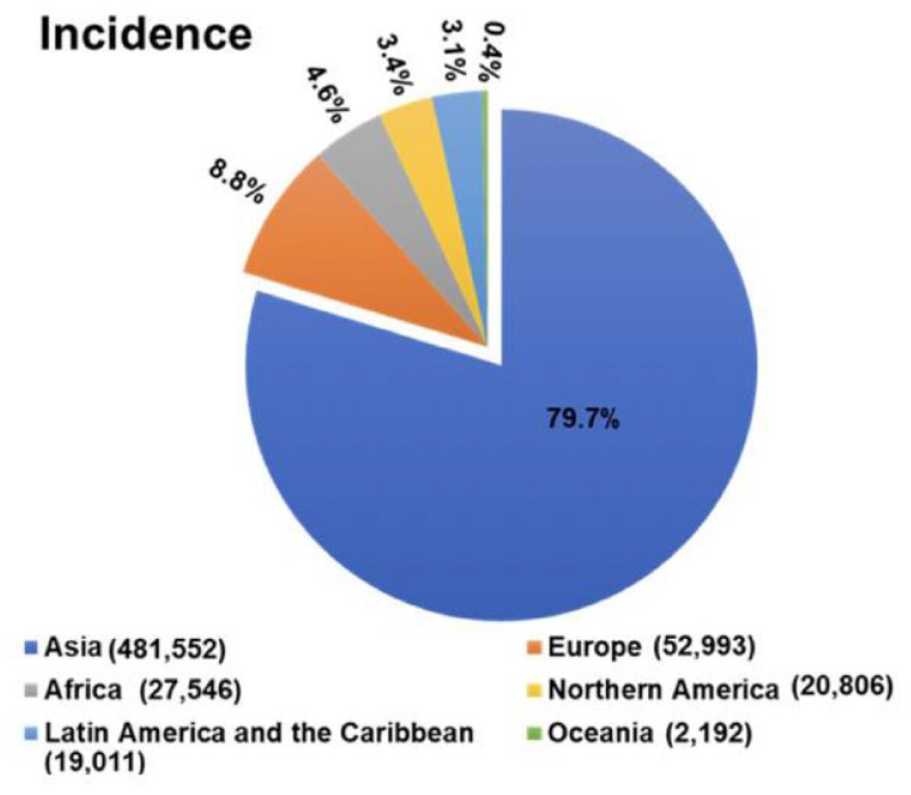
Pie-chart showing proportion of disease distribution continent wise. Borrowed with permission from Prof. Pengfei Xu. 4
There is a dramatic regional variation in the incidence of these 2 types of esophageal cancers. In Western nations with predominant Caucasian populations, adenocarcinoma is the most common type, accounting for >90% of esophageal cancers, whereas in the East, in countries such as China, Japan, parts of Africa and India squamous cell cancers predominate.1-4 The exact reasons for this are still unknown, but as per latest evidence it is likely to be a combination of environmental factors, dietary habits and genetics.1,5,6
Need for Screening
Esophageal cancers carry a high mortality with estimated survival of 20% at 5 years, mainly due to delay in diagnosis. 7 Majority of the cancers, even in developed countries are diagnosed in stage III and only 15% to 30% are eligible for curative intent therapy.7,8 The large difference in stage-wise survival of esophageal cancer indicates that disease detected earlier has better prognosis. International data used for staging has shown that T1 lesions have a 5-year OS of >90%.8,9
Squamous cancers of the esophagus may be considered amenable to screening as they meet the criteria for screening to be effective such as
(1) High incidence of disease—disease of public health importance.
(2) Validated test that can detect the disease at an early stage.
(3) Detectable preclinical phase.
(4) Effective treatment option at an early stage that can prolong survival. (Adapted from Wilson and Jungner’s criteria for screening). 10
Applying these principles to squamous cell cancers of the esophagus (ESCC), age-standardized incidence rate of esophageal cancers in Eastern Asia is 18.2 per100 000 population, with a predominance of squamous cell cancers, 3 making it a disease of high incidence and of public health importance. Certain rural regions in China such as Cixian and Yanting have an incidence of >150 per100 000 population.3,11
Natural History and Pre-Cursor Lesions
Presence of detectable pre-cursor lesions are essential for screening to be successful.8,10 Studies from China have shown that squamous dysplasia is a definite precursor lesion for ESCC.5,8,12
Wang et al performed a sub-set analysis of the Linxian Nutritional Intervention Study. 13 They followed up 682 patients who had undergone endoscopy and biopsy from the esophagus for a median of 13.5 years. Patients who became symptomatic were biopsied again. Biopsy results were then compared and the risk of developing malignancy was analyzed. In patients with a biopsy report of carcinoma-in-situ and severe dysplasia, there was a 74% risk of developing malignancy. For patients who had mild and moderate dysplasia, the risk was 24% and 50% respectively. In contrast, it 15% in those with basal cell hyperplasia and 8% for those with esophagitis
In a prospective endoscopic study conducted in rural China from 2006 to 2015 where 1753 cases were followed up for 2.9 years(median), the authors found increased risk of progression to esophageal squamous cell carcinoma with higher grades of dysplasia and also demonstrated a 2.6 times increased risk of developing ESCC in males and 1.2 times increased risk in elderly participants(>50 years). 12
Lu et al followed up patients with “atypia” and demonstrated that patients with atypia had a 2.9 times higher risk of developing ESCC compared to normal controls. 14 Wang et al published large studies involving >3000 patients demonstrating the feasibility of using Lugol chromo-endoscopy for screening of pre cursor lesions, described their treatment and reported optimal survival outcomes.13,15-17 A few studies from Iran have also demonstrated the high incidence of esophageal pre cursor lesions in high-risk areas and the feasibility of using balloon cytology to detect them.18,19
Who Needs to be Screened?
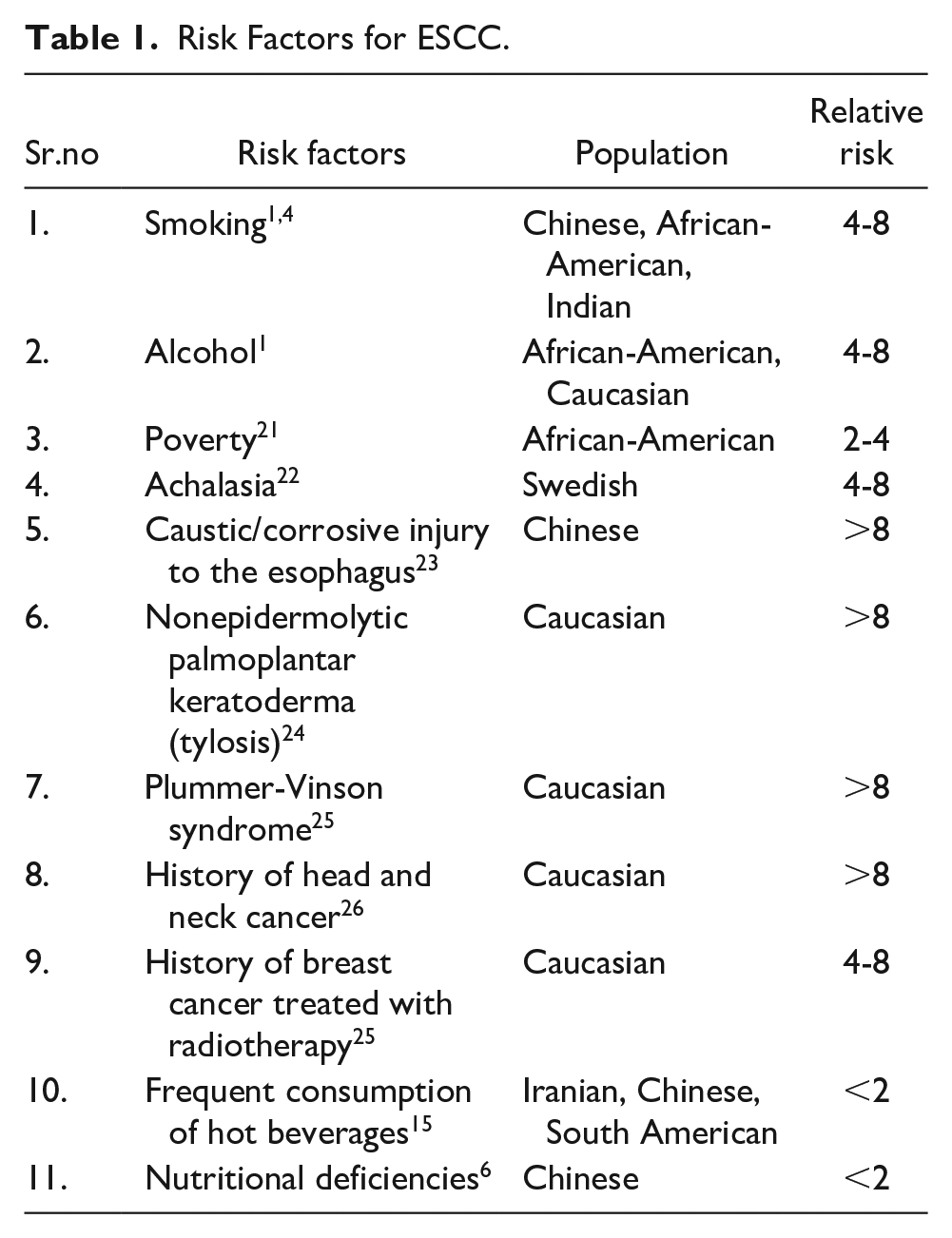
Smoking and alcohol consumption are established risk factors world over for ESCC. 1 Apart from these, there is evidence from high incidence areas regarding consumption of hot liquids, salted/pickled or fermented food, diet lacking in fresh fruits and vegetables, presence of achalasia cardia, family history of ESCC, ingestion of caustic substances and previous history of head and neck cancers conferring a higher risk of developing ESCC as shown in Table 1.5,6,20 These factors play a major role in participant selection for screening.
Risk Factors for ESCC.
Human papilloma viruses have been shown to play an important role in pathogenesis of other squamous cell cancers, however in esophagus, the evidence is inconclusive. 27
Most of the studies done on screening are from high incidence areas, where the entire adult population between the age group of 40 and 69 years have been screened.28-36 In an ongoing RCT in China, 33 considering the risk factors for ESCC, in non-endemic areas- heavy smokers (>10 pack years), those with a family history of ESCC in first degree relatives, heavy alcohol consumers (>28 g/day for 10 years), history of esophagitis and reflux disease, eating salted food/pickled food at least once a week were used as inclusion criteria to select patients for screening. Using the above criteria, the detection rate in non-high-risk areas was about 0.9% and in high-risk areas where all adults between 40 and 69 years were included, it was 0.8%. 33 This can be considered an average pick-up rate, when compared to screening trials conducted for other common cancers, such as the National Lung Screening Trial(NLST), which had a pick-up rate of 2.6%. 37
As most of the data is from China as shown in Table 3, it would be difficult to extrapolate this data to other regions. Hence, patient selection needs to be specific to the population that we need to screen and criteria will have to be based on data available regarding risk factors in that region. However, based on available data—old age (>60 years), smoking and alcohol consumption seem to be common risk factors across regions. 1
Modalities for Screening
Standard Endoscopy
Fiber-optic endoscopy as of today, is widely available and is the first choice of investigation in patients with symptoms suggestive of ESCC. Gruber et al 38 from Brazil, published their results for detection of esophageal dysplasia by conventional white-light endoscopy(standard), the sensitivity was 40.6% and specificity was 76.8%. They concluded that standard endoscopy is not accurate enough for detection of pre-cancerous lesions.
Chromo-Endoscopy With Lugol’s Iodine
The basic principle of using Lugol’s iodine is that abnormal squamous cells do not take up iodine staining, where as normal squamous epithelium of the esophagus does as shown in Figure 3.39,40 Abnormal squamous epithelium could be either frank malignancy, carcinoma in-situ, dysplasia or esophagitis.39-42 The stain helps to choose the site of biopsy. In this procedure, 10 to 40 mL of 0.3% to 0.5% of Lugol’s iodine is sprayed on the esophageal mucosa and in 5 to 8 minutes differential staining occurs. Areas which do not take up the stain are biopsied adequately.39,40
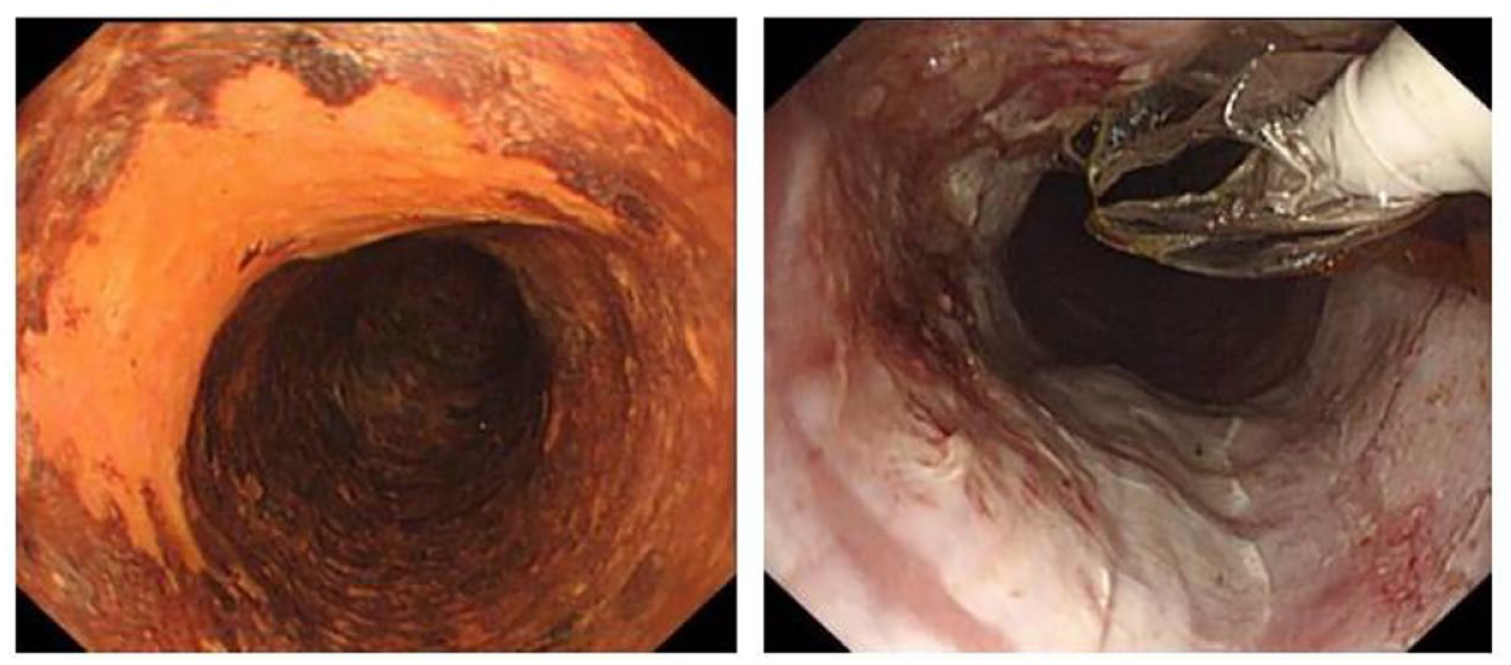
Lugol’s chromo-endoscopy—left image—iodine staining demonstrated over normal mucosa. Right image—planning for biopsy from unstained area. (Borrowed with permission from Prof. Jacques Bergman, Amsterdam Medical Center).
Misumi from Japan first reported this technique, 40 However, it was the landmark study by Dawsey et al 39 conducted in Linxian province in China, that demonstrated the effectiveness of this technique in a large population to pick up pre cursor lesions.
In a French study by Dubuc et al, 43 using Lugol’s iodine they were able to demonstrate superiority over conventional endoscopy. Patients were divided into 4 groups—(1) previous history of head and neck cancers, (2) alcohol and tobacco addicts, (3) alcoholic pancreatitis, and (4) alcoholic cirrhosis. Conventional endoscopy was able to pick up 35 abnormal lesions compared to chromo-endoscopy which picked up 67 lesions. The difference was more apparent for early pre cursor lesion such as dysplasia and carcinoma in-situ.
Zeng et al recently conducted a cluster RCT in China, where 345 villages in high incidence areas underwent randomization. All adults aged between 40 and 69 years old, who had no past history of cancer and had not received endoscopy in the past 3 years were invited to participate in the trial. In total,37 922 subjects underwent chromo-endoscopy with Lugol’s iodine and 528 (1.8%) positive cases were detected. Of the invited participants, only 45% consented for endoscopy and there were no significant serious adverse events associated with this procedure. This large study demonstrated the safety and efficacy of chromo-endoscopy with Lugol’s iodine in a community setting. 33
Chromo-endoscopy with Lugol’s iodine appears to be effective, but endoscopy it is still an invasive procedure and compliance of asymptomatic patients is still low. It requires a clinic or a hospital setting and an experienced operator, especially to pick up pre cursor lesions. 44
Chinese Cytology Technique
Innovative, low-cost technique developed in China in the 1950s. 45 It involves using a balloon catheter covered with a cotton web as shown in Figure 4. The catheter is inserted in a similar fashion to a conventional naso-gastric tube (blind procedure) (Figure 2). Once the balloon is in the gastric mucosa, it is inflated with a syringe and then withdrawn across the esophagus, till resistance is encountered at the upper esophageal sphincter. At this point the balloon is deflated and withdrawn through the oral cavity. The sample then obtained is put on a glass slide and stained by the Papincolou method.
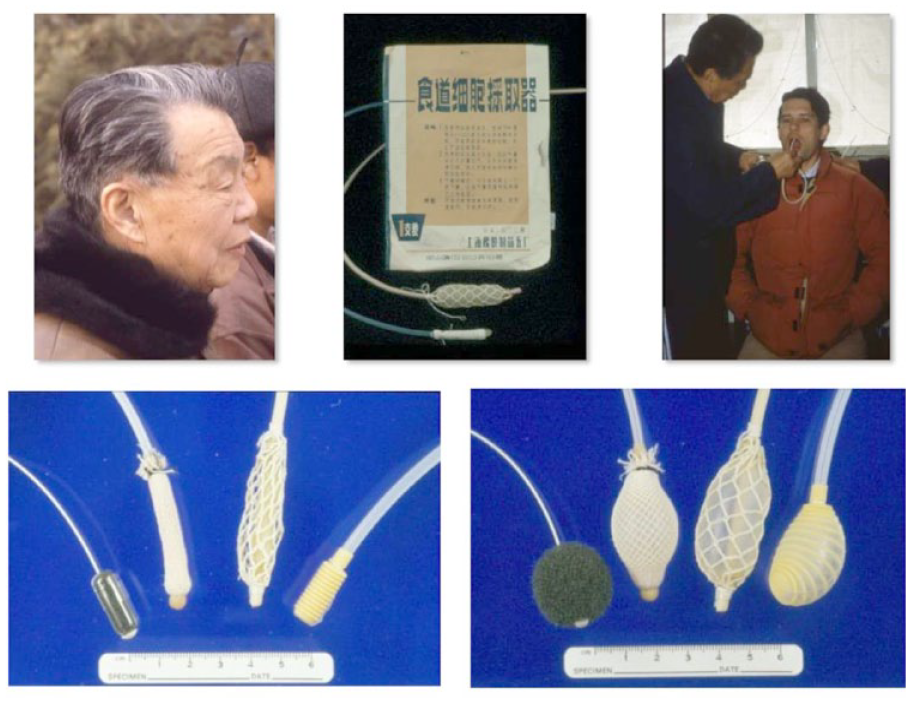
Picture demonstrating Chinese balloon cytology—Left upper corner—Prof. Shen Q taking a cytology exam, right upper corner—Prof Dawsey being administered a balloon test by Prof. Shen. Other images—various types of balloons and equipment used for the procedure. (Picture borrowed with permission from Prof. Sanford Dawsey, NCI).
The samples are then graded like other squamous lesions using the Bethesda system 46 —atypical squamous cells of undetermined significance (ASCUS), low grade squamous intraepithelial neoplasia (LSIL), high grade squamous intra epithelial neoplasia (HSIL).
Large studies from China involving more than 10 000 patients15,31,32,47 have shown that the yield of cells with this technique is adequate, but sensitivity only ranges from 39% to 62%. Even though this could pick up some early precursor lesions, accuracy was not optimal for this technique to be recommended as the standard.
Improving Sensitivity Using Molecular Markers
To improve sensitivity, various authors have analyzed immunohistochemical and molecular markers in cytology specimens. Methylated DNA markers (MDM) have shown promise in recent studies. An international multi-nation study involving subjects from China, United States and Iran, where 430 samples were analyzed for MDM has shown promising results. In this study, balloon cytology samples from China were also included. Statistical modeling was done and area under the RoC curve was calculated. In all 3 models, the AUC was >0.90. Another interesting finding in the Chinese cytology specimens was that the degree of methylation corresponded to the grades of dysplasia. 48 A pilot study in China published in 2022 also showed promising results when p16 alone was used as a methylation marker. 49
The Chinese cytology technique has potential to be an ideal screening technique. However, compliance and acceptance rates may vary across regions and using molecular markers for screening might not be a cost-effective option.
Cytosponge Technique
There are various other devices designed based on similar principles
The Cytosponge technique developed by Professor Fitzgerald from UK, 50 has shown a lot of promise in screening for Barret’s Esophagus (BE) in a GERD population. The combination of Cytosponge and trefoil factor 3(TFF3) increases the detection of Barret’s esophagus by 10.6 times in a primary care setting. 51 It consists of a gelatin capsule attached to a string; the capsule contains a compressed foam sphere. The patient is expected to swallow the capsule whole, while holding the string. The capsule dissolves in the stomach and the sponge expands, then the sponge is pulled up through the esophagus and oral cavity. 50 In an Iranian study of 301 participants, cytosponge combined with p53 staining showed a sensitivity of 100% and a specificity of 97%. 52 Larger studies are required to assess its feasibility and cost effectiveness for screening.
Gao et al used artificial intelligence and machine learning techniques to select high risk patients and analyze the cytology specimens obtained by cytosponge and reported that more than 90% of screening endoscopies could be avoided. 53
Image Enhanced Endoscopy—Narrow Band Imaging (NBI) and Autofluorescence
These are newer endoscopic techniques that are expensive and may not be cost-effective for mass screening, however, they have shown promising results.
Narrow Band Imaging is generally combined in modern endoscopic units, a single twist of the knob or pressing of a button can introduce the NBI filter. 54 In this real-time imaging, abnormal esophageal mucosa is seen as brownish spots, sensitivity in expert hands has been demonstrated to be in the range of 85% to 90%. 55 Autofluorescence is based on the principle of differential absorption of fluorescent light between normal and abnormal mucosa, but sensitivity and specificity for esophageal lesions is lesser than NBI. 20 In a review article by Chung et al, 26 the pooled average risk of developing an esophageal second primary in a patient with head and neck cancer was 8.1% (28 studies, >4000 patients). With the addition of enhanced imaging (chromoendoscopy, NBI) detection rates were increased by 5% to 10%.26,56
Microendoscopy and endocytoscopy are other promising image enhancing technologies that are in development and may become important in the near future. 20
Less Invasive Endoscopic Modalities
Transnasal endoscopy (TNE) uses a thin scope, which is inserted through the nose, this avoids touching the base of tongue, hence reduces gag reflex. 20 Various randomized trials and meta-analysis have concluded that TNE is equivalent to conventional endoscopy for endoscopic diagnosis, but is inferior for histologic diagnosis, possibly due to inferior image quality. 57 However, patient acceptance is higher for TNE compared to conventional endoscopy. Wang et al and Arantes et al have shown that TNE is also safe and feasible for detecting ESCC.58,59
Capsule endoscopy has shown some promise in screening for adenocarcinoma. 51 A meta-analysis of 9 pooled studies showed a sensitivity of 77% and specificity of 86% for diagnosing Barrett’s Esophagus in GERD patients. 60 However, as per Western data, the cost of capsule endoscopy appears to be prohibitive for mass screening 51
However, capsule endoscopy has not been used or tested for screening in squamous cell cancers.
Non-Invasive Tests/Non-Endoscopic Methods
These tests are hypothesized to be effective for mass screening—as they don’t require a skilled operator, likely to be cost effective and have higher patient acceptability.
Serum based bio-markers—require only venous blood sampling from the patient. Auto-antibodies to tumor associated antigens (TAA) have been tested for diagnosing ESCC—A 6-panel autoantibody test in 237 patients demonstrated a poor sensitivity of 45%. 61 Circulating microRNA (miRNAs) have been extensively studied for diagnosing ESCC. A recent meta-analysis showed a pooled sensitivity of 79.9% and specificity of 81.3% for diagnosis of ESCC. 62 Further studies are required to validate it in a screening population. Salivary biomarkers also have shown some promise in recent studies, but are yet to be tested for screening. 63
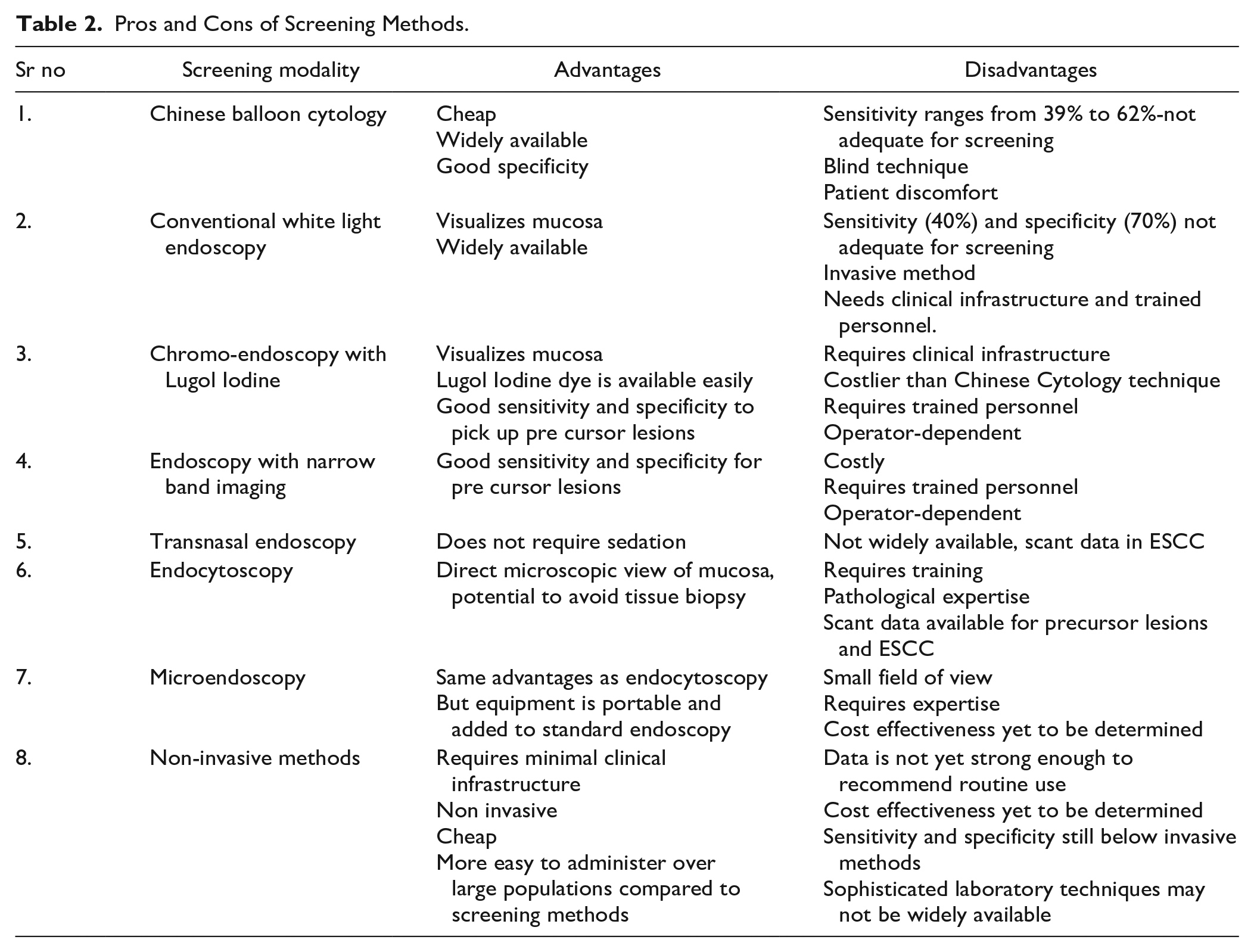
The relative merits and demerits of these modalities have been summarized in Table 2.
Pros and Cons of Screening Methods.
Is There Evidence at Present to Support Screening?
The evidence to support screening for squamous cell cancer of the esophagus is insufficient at present. However, as of today, 3 large randomized controlled trials are underway in high-risk areas of China as shown in Table 3. One of them is a cluster randomized controlled trial (RCT) of 345 eligible clusters, 33 they have recruited 145 956 participants from high risk and non-high-risk areas to screen for esophageal and gastric cancers. Chromo-endoscopy with Lugol’s iodine for esophageal and indigo-carmine dye for gastric cancers was used for detection of early lesions.
Summary of Major Screening Studies on ESCC.
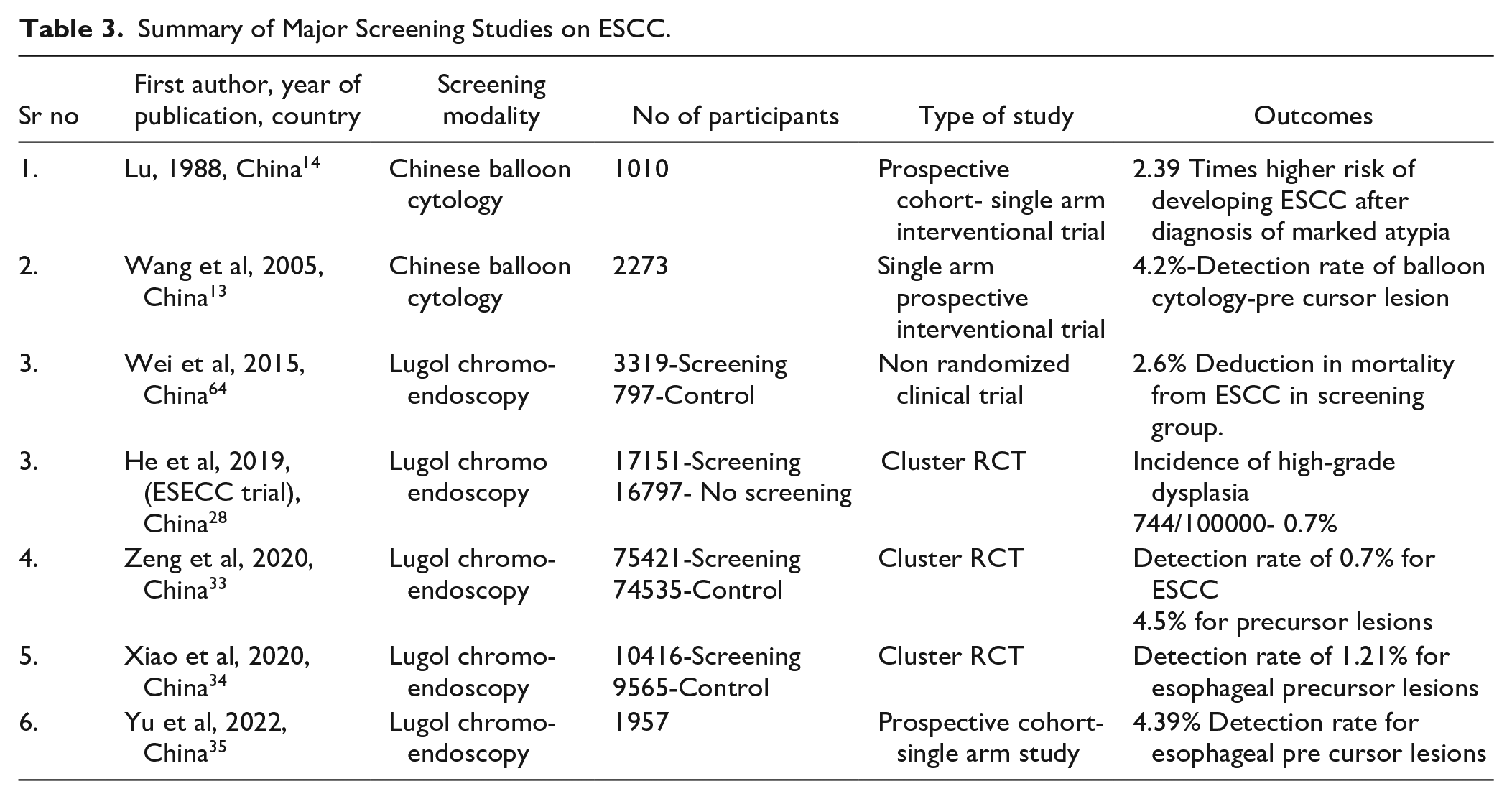
As per the initial results, the detection rate was 0.7% in non-high-risk areas and 0.8% in high-risk areas. Majority of the cases detected (92.9%) were early stage (0/I). Long term results are awaited.
The other large cluster RCT underway in China (Hua County, Henan Province) is the ESECC trial—Efficacy of endoscopic screening for esophageal cancer in China. 28 Seventeen thousand one hundred fifty-one participants have been recruited in the screening arm and 16 797 in the control arm. Participants in the screening arm underwent one-time Lugol chromo-endoscopy. Initial results showed a detection rate of 0.74%. In this study 113 lesions were detected which were classified as high grade and 69.9% were early-stage cancers (stage 0/I). Long term and detailed results are awaited.
A large non randomized interventional study by Wei et al 64 conducted in China demonstrated 1.7% reduction in mortality. In this study 3319 participants underwent one-time Lugol chromo-endoscopy and the control arm consisted of 797 participants from 10 different villages from another geographical region who were under observation only. At 10 years of follow up the screened arm had a 3.35% mortality rate from ESCC compared to 5.05% in the control arm (P < .001).
Cost Effectiveness
Li et al 65 using data from the ESECC trial estimated the cost of screening with chromoendoscopy with a valid pathological diagnosis as 196$ and the cost of detecting one early-stage esophageal cancer was37 687$. Considering the per capita income in rural China to be around 5000$, the cost of screening endoscopy was estimated to be around 3.5% to 4% of the per capita income, which was considered to be quite a significant burden on the exchequer. By using precision screening methodology and selecting only high-risk cases to be screened the costs could be reduced by around 25% to 30%.
Xia et al 66 also estimated the cost effectiveness of endoscopic screening for esophageal and gastric cancers in high-risk areas in China. They used a Markov model and estimated that endoscopic screening improved effectiveness by 1087 to 10362 quality adjusted life years (QALYs) leading to incremental cost effectiveness ratio (ICERs) between 1343 and 3035 $ per QALY. They concluded that the most cost-effective strategy would be to screen the high-risk population between the age group of 40 and 69 years every 2 years
Conclusions
To summarize, screening for esophageal squamous cancers appears to be feasible in high incidence areas. Patient selection is still controversial, older age, smoking and alcohol consumption seem to be established risk factors, but other environmental and dietary factors need to be quantified and considered. Amongst the various modalities available for screening, Lugol chromoendoscopy appears to be the method of choice, especially with regards to accuracy and cost-effectiveness. Evidence from prospective studies and initial results from Chinese trials do not provide robust evidence for screening, but they demonstrate its safety and feasibility. Further long-term data on the effect on mortality is still awaited. Screening high-risk individuals has been adopted across many cancers and is a continuously evolving field for esophageal squamous carcinoma. Lack of a cost-effective and non-invasive suitable modality seems to be the major hurdle in generating evidence for screening this disease.
Footnotes
Acknowledgements
Prof. Sanford Dawsey, NCI(USA), Prof. Jacques Bergman and Prof. Pengfei Xu for allowing to use their materials.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.