
Abstract
Manometric assessment of the gastroesophageal junction (GEJ) and esophageal body is the key to a better understanding of the mechanics of antireflux surgery (ARS) and maximizing its benefits while minimizing adverse outcomes. However, there is an attitude of uncertainty regarding the necessity of esophageal motility prior to ARS among some surgeons. This evidence-based review highlights the critical role of manometry in the preoperative workup for patients undergoing ARS. It also discusses how manometry can detect findings associated with favorable outcomes or the risk of postoperative dysphagia. Manometric data can be used for risk stratification and the prediction of outcomes, aiding the surgeon in matching an operation to the specific physiology of each individual patient.
Keywords
Introduction
The development of esophageal physiology testing in the second half of the 20th century provided insight into the physiologic consequences of anatomic abnormalities in the gastroesophageal junction (GEJ). This resulted in a conceptual change in antireflux surgery (ARS) from basic restoration of anatomy to operations designed to improve physiology. The discovery of the lower esophageal sphincter (LES) and improvement in the technique of manometry laid the foundations of the golden era of ARS. Nissen introduced his famous surgery in 1956, 1 which was followed by the Belsey partial fundoplication and the Hill posterior esophago-gastro-pexy, both introduced in 1967.2,3 Studies using conventional manometry showed that of these 3 procedures, the Nissen fundoplication was the most effective in improving the competency of the LES 4 and was therefore rapidly adopted by surgeons in Northern America and Europe, becoming the “modus operandi” for most surgeons treating gastroesophageal reflux disease (GERD) in the 20th century. Fundoplication was shown to augment the resting pressure of the LES. The degree of this increased pressure and the resistance imposed at the GEJ is correlated to the degree of constructed fundoplication. Based on this principle, Dor and Toupet proposed construction of a partial anterior and posterior fundoplication, to impose less resistance at the GEJ to minimize the rate of dysphagia observed after a 360° fundoplication and as an option in those with poor esophageal contraction.5,6 With multiple surgical options available, foregut surgeons gained the ability to individualize the ARS based on patients’ factor. The most notable component in this selection process was the status of esophageal contractile force assessed through esophageal manometry test. Therefore, this test became a critical element of the preoperative workup for patients undergoing ARS and the concept of tailoring fundoplication was born. The esophageal manometry test was not only useful as part of the diagnostic work-up, but also gradually showed its utility as a prognostic tool, in which the surgeon can use captured data for patient selection and predict outcomes. The latter has not well established in the literature, despite wide-spread clinical practice. At the beginning of the 21st century, high resolution manometry (HRM) became available. This technology allowed characterization of the esophageal body and GEJ motor function with details not previously available using conventional manometry. One would expect that these technical advances would have resulted in an abundance of research that leads to more clinical insight and improvement in the outcomes of anti-reflux surgery. However, with exception of a few institutions, studying the role of esophageal physiology has not been the focus of most surgical foregut centers. In fact, there is a growing attitude of uncertainty regarding the necessity of esophageal motility prior to ARS among some surgeons. The crux of their argument is that manometry does not impact the choice or the outcome of surgery and is therefore not a necessary test prior to surgery. They support their case with the following assumptions:
Videoesophagram without manometry is adequate for the evaluation of esophageal dysmotility prior to ARS.
Fundoplication results in improvement in esophageal motility and can therefore be tolerated even in patients with poor motility.
Tailoring ARS does not impact the outcome.
There are publications that support these speculations; however most do not adequately capture the breadth of physiologic ramifications. This manuscript will first review these studies and provide evidence that questions their global utility while highlighting the importance of manometry prior to ARS. It will then elaborate on the fact that the utility of esophageal manometry is not limited to a simple diagnostic tool but can also be used as a prognostic instrument utilized for risk stratification and predicting outcomes. In this capacity HRM can be used to form a more personalized approach in anti-reflux surgery through patient selection and preoperative counseling.
The Adequacy of Videoesophagram in Evaluation of Esophageal Dysmotility
Videoesophagram (VE) is a dynamic radiographic study that provides anatomical information such as esophageal length, presence of diverticulum, stricture, and types of hiatal hernia. It also provides limited quantitative information regarding esophageal motility. Some surgeons advocate use of VE alone to evaluate esophageal motility prior to ARS. This approach is encouraged by some clinicians in social media and physician discussion virtual forums, a position supported by a recent publication that found a high sensitivity of 96.4% and a negative predictive value of 99.6% for VE in detecting significant esophageal dysmotility. 7 This group of authors then concluded that a routine manometry is not warranted in patients with normal VE. There are few points to consider when interpreting the results of this study. This high degree of sensitivity has not been reproduced in other studies. In fact, an earlier publication from the same institution reported a low sensitivity of 55%. In this study, Fuller et al 8 from DeMeester’s lab concluded that VE is a relatively insensitive test in detecting motility disorders. O’Rourke et al 9 from Castell’s lab had also shown a sensitivity of 69% and stated that VE is a poor screening examination for the detection of esophageal dysmotility. Another limitation in this study is that the radiologists at University of Southern California use a very detailed and extensive protocol during the radiologic evaluation and use a reporting system with strict definitions of esophageal stasis and dysmotility, which are not widely utilized elsewhere. Although this “USC Protocol,” as it is commonly known, has a degree of details that enables a semi-quantitative assessment of esophageal dysmotility, it is proven to have low specificity in detecting esophageal dysmotility of 59% and low positive predictive value of 14.4%. 7
Improvement in Esophageal Motility After ARS
There is a school of thought that because peristaltic force improves after fundoplication, patients with poor peristaltic contractility at baseline are still able to tolerate a full fundoplication. However, the impact of fundoplication on modulating esophageal motility is complex with studies reporting conflicting results. Scheffer and colleagues 10 reported that nadir EGJ relaxation, intrabolus pressure (iBP), and distal esophageal contractile force, all increase following Nissen fundoplication. However, Fibbe et al 11 found that esophageal motor function remains unchanged following laparoscopic Nissen and Toupet fundoplication, reporting improvement in primary peristalsis only in patients with preoperative dysmotility and only after Toupet fundoplication. Furthermore, some authors have reported more vigorous contractions after Nissen compared to partial fundoplication.12,13 In contrast, studies on the impact of magnetic sphincter augmentation (MSA) on esophageal contractility report more consistent results, in part due to the standardized and reproducible nature of this procedure, resulting in minimal variation in technique (Figure 1). One such study showed a direct correlation between esophageal outflow resistance and postoperative distal contractile integral (DCI). 14 This suggests that the increase in contractility is an esophageal compensatory mechanism to overcome increased resistance at the GEJ.
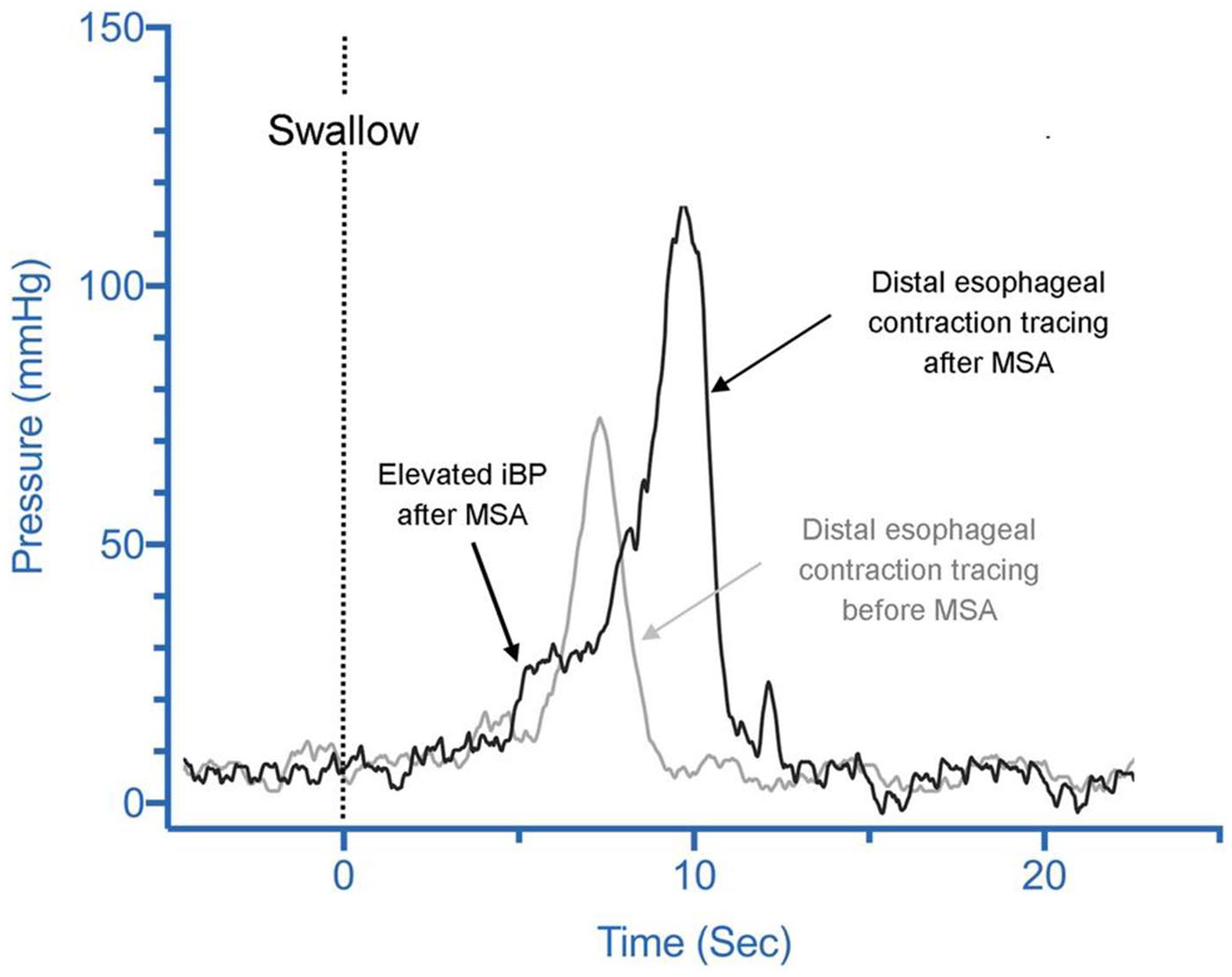
Distal esophageal contraction line tracing in a patient before (gray tracing) and after (black tracing) magnetic sphincter augmentation (MSA). The intrabolus pressure (iBP) as a marker for outflow resistance is significantly higher after MSA. Distal esophageal contraction amplitude is increased after MSA as a compensatory mechanism of the esophagus to overcome the outflow resistance of the augmented LES, from Ayazi et al. 14
The following consideration question the universal validity of advocating Nissen in patients with suboptimal motor function. Even if we accept that esophageal motility improves following ARS, this increased contractile force needs to overcome a much higher resistance at the GEJ. This compensatory response may not be sufficient in all cases to facilitate bolus transit across the surgically augmented GEJ. In addition, previous studies have shown that long-standing GERD can result in progressive mucosal injury and lead to fibrosis of the esophageal body, loss of esophageal contractility, and eventual shortening of the esophagus, requiring Collis gastroplasty in some patients15,16 (Figure 2). It is unlikely that esophageal contractility improves following surgery in this group of patients with organ failure caused by severe GERD.
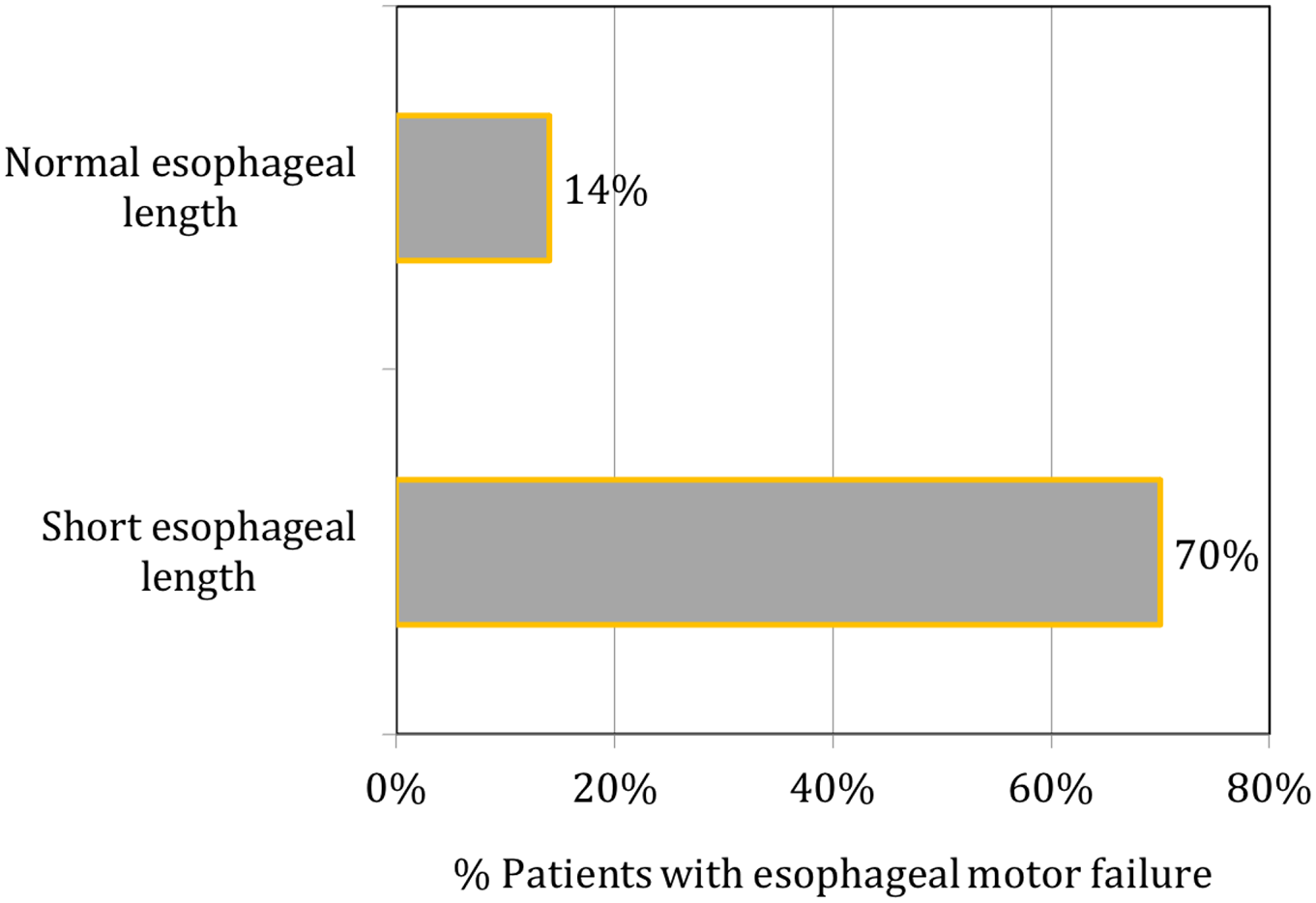
Prevalence of esophageal motor disorders in patients with and without short esophagus length requiring Collis gastroplasty (P < .05). Failure of esophageal function was identified by the presence of one or both of the following parameters: mean distal esophageal contraction amplitude <20 mmHg or more than 20% simultaneous waves in the distal esophagus, from Kauer et al. 17
The Inconsistency in Literature Regarding Tailoring Approach
Patients with reflux disease are often referred for consideration of ARS only after the disease has progressed to substantial functional and anatomical derangements of the foregut, making ARS particularly challenging. Early studies had emphasized the importance of adjusting for these abnormalities to maximize the reflux control and minimize the side effects of ARS. Surgery is designed to restore the competency of the LES, thereby increasing resistance at the GEJ (Figure 3). In order to avoid persistent dysphagia after ARS, the contraction amplitude of the peristaltic waves in the distal esophageal body must overcome the outflow resistance imposed by the surgically augmented GEJ. The concept of tailoring is based on the logic that patients with dysmotility have reduced esophageal contractile force and therefore the degree of outflow resistance needs to be tailored to allow transit of bolus through the surgically augmented GEJ. Results of several early studies support that failure to tailor the operation in patients with poor esophageal motor function results in a high percentage of unsatisfactory results.18-20 Yet, there is a growing tendency to disregard the need for tailoring surgery based on foregut abnormalities, stemming from several studies that have shown no benefits in the tailoring approach.21-24 The authors of these studies promote the concept of “one size fits all” in ARS, recommending that Nissen fundoplication can be used in all patients, regardless of the preoperative manometry findings. This conclusion disregards the development of dysphagia imposed by overly augmented outflow resistance and questions the routine use of manometry prior to ARS. These studies have limitations that are important to fully recognize prior to applying their findings to clinical practice. Almost all of these studies have utilized conventional manometry and there is inconsistency in criteria used to define esophageal dysfunction, which also deviates from currently accepted classifications. Various cutoffs for esophageal body contraction, amplitude, and percent of intact swallows used in these studies, confound the evaluation of the impact of tailoring. Another potential explanation is that many of these studies were conducted in Europe, where eating habits are significantly different from the US. The European eating style typically consists of small meals eaten slowly, which is better tolerated after a full fundoplication and may not cause significant dysphagia. The results of these studies may not be reproducible in an American population with an eating style of large meals consumed rapidly.
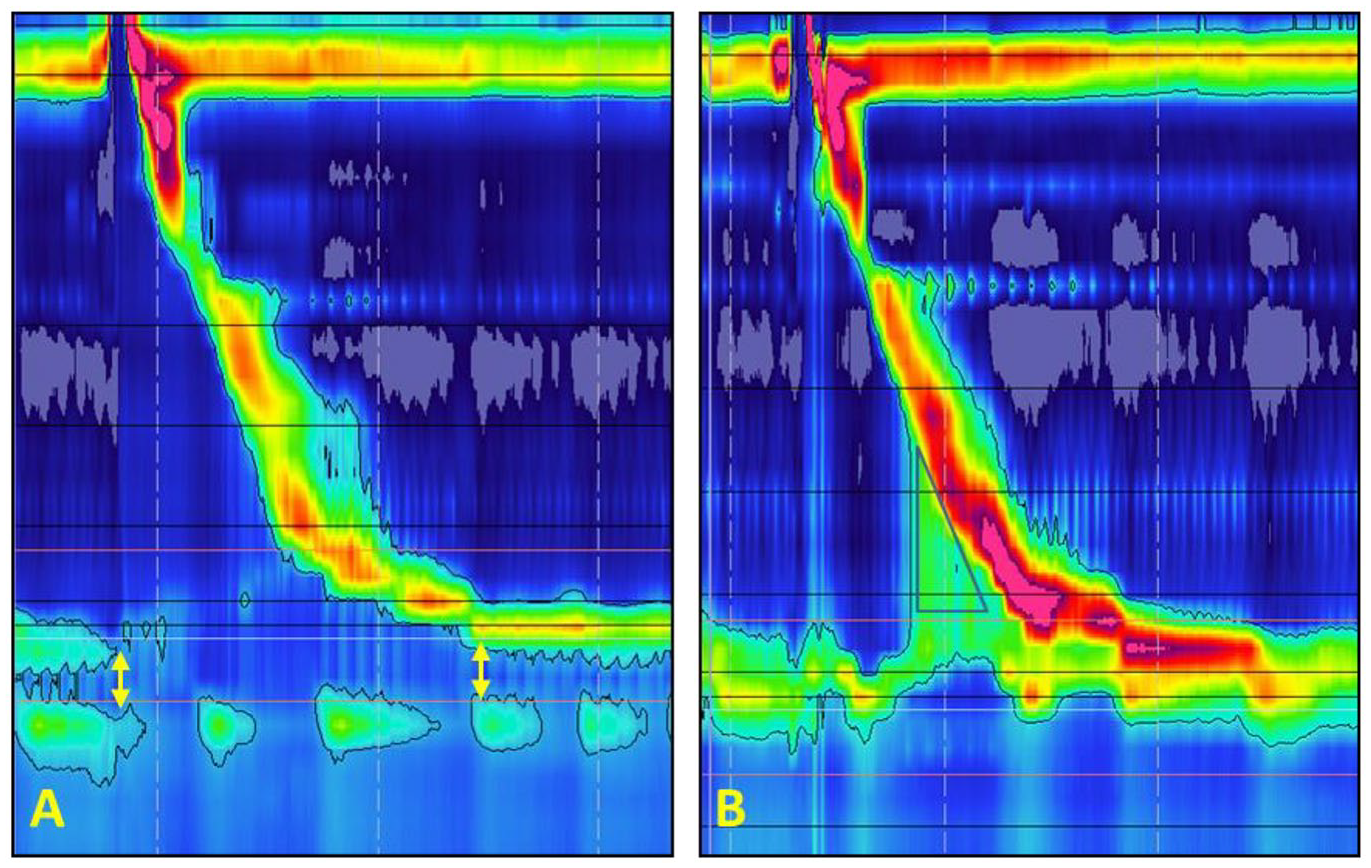
High resolution manometry topographic plot of a GERD patient before (A) and after (B) hiatal hernia repair and antireflux surgery: (A) topographic plot showing a defective LES with a low resting pressure, no intra-abdominal length, and short overall length. Note the separation between LES and crura diaphragm that indicates presence of a hiatal hernia (yellow arrows); (B) topographic plot of the same patient after surgery shows augmentation of the LES resting pressure and abdominal length. The elevated intra-bolus pressure (iBP) is marked with black triangle.
In addition, ARS is considered a reconstructive surgery aiming to improve the foregut function by correcting underlying anatomic and physiologic defects, rather than excising a diseased organ. Therefore, it is a very technique dependent procedure. Variations in technique between surgeons results in variation in outflow resistance, which translates to variation in the outcome of the procedure.
Two other notions that question the validity of a non-tailored approach are dysphagia secondary to outflow resistance imposed by a hypertensive LES and near-universal use of manometry prior to MSA. Patients with a hypertensive LES or true gastroesophageal junction outflow obstruction (GEJOO) have a high intrabolus pressure and require a myotomy of the sphincter to relieve dysphagia.25,26 The other observation is that even surgeons, who do not tailor fundoplication, obtain HRM prior to MSA. This suggests that even this group of surgeons believe that there is a level of outflow resistance at the GEJ that induces dysphagia in patients with inadequate peristaltic contraction.
The Necessity of Preoperative Physiologic Testing
Studies have shown that an inadequate preoperative workup is one of the main factors that leads to poor outcomes following ARS. 27 The value of esophageal function testing as an essential preoperative assessment before ARS is highlighted by Chan et al 28 from Gyawali’s lab in a study of large cohort of patients referred for manometric evaluation prior to ARS. In this study, undiagnosed achalasia was found in 1%, and significant impairment in LES relaxation in an additional 1.5% of the 1103 motility studies performed prior to ARS. These motor disorders are absolute contraindication to fundoplication and need to be managed by endoscopic or surgical myotomy. Another 3.2% had aperistalsis, and 1.3% had more than 80% failed contractions. Collectively, 7% of patients had findings that would be considered as absolute or relative contraindications to Nissen fundoplication (Figure 4). They also found that nearly one-quarter of the patients had no objective evidence of reflux disease on esophageal pH monitoring. These patients did not have any prior documentation of severe erosive esophagitis, alternate non-GERD hiatal hernia indications, or prior ambulatory pH monitoring.
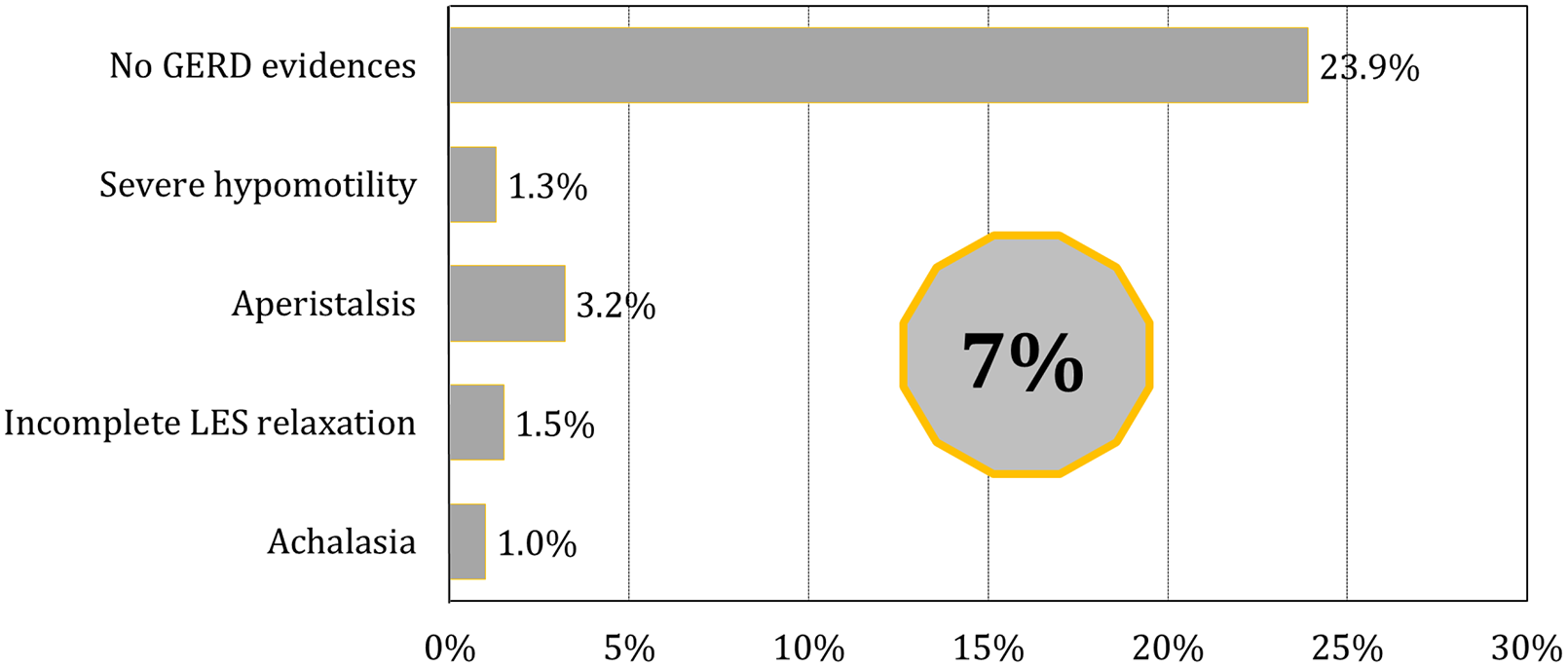
Proportion of patients with absolute or relative contraindications for a Nissen fundoplication, of note 24% of the patients were found to have no objective evidence of reflux disease on esophageal pH monitoring, from Chan et al. 28
The Impact of Esophageal Hypercontractility on Outcome
The focus of clinicians during the review of preoperative esophageal manometry testing is to identify patients with poor esophageal motility and there is a tendency to disregard hypercontractile features. However, studies have shown the importance of these features on the outcome of ARS. Non-specific spastic disorders (NSSDs) are a manometric designation used prior to introduction of the Chicago classification. Criteria used to define this manometric disorder are listed in Table 1.29-31 This classification of hypermotility does not include achalasia or diffuse esophageal spasm and its features are often subtle and not noted by some esophageal motility laboratories. This category of motility findings cannot be diagnosed with other modalities like videoesophagram. They are, however, common, with rates as high as 40% to 50% in some series of unselected patients referred for manometry testing. 30 The highest prevalence of this disorder is among patients referred for evaluation of non-cardiac chest pain, but its prevalence is even high in cohorts consisting of patients referred for preoperative evaluation for ARS, with publications reporting rate of 29%. 31 Studies have shown that presence of NSSDs is a predictor for suboptimal outcome after ARS. Winslow et al 31 reported that although patients with NSSDs and documented reflux disease experience improvement in their foregut symptoms after ARS, they were more likely to report heartburn (22% vs 7%), waterbrash (14% vs 4%), and reinitiate or continue antisecretory medications (17% vs 5%) when compared to non-spastic patients (P < .05 for all comparisons). In another study, Barreca et al 32 defined hypercontractility as a hypertensive LES or high amplitude esophageal body contractions and reported that heartburn resolved in only 57% of patients with hypercontractility and that chest pain was still present in 22% of patients after ARS. They concluded that hypercontractile esophagus is not a contraindication to fundoplication, but that both patient and surgeon should be aware of postoperative symptoms. There is evidence that patients with NSSDs have an intensified esophageal sensory perception and a lower threshold for reporting symptom, which may explain the suboptimal response to ARS.
Manometric Criteria to Define Nonspecific Spastic Disorder (NSSD) of the Esophageal Body.
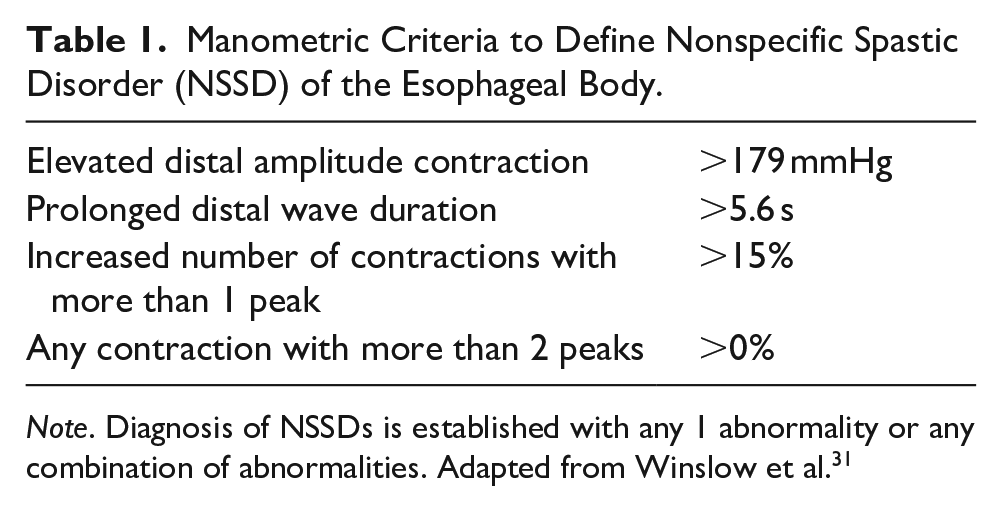
Note. Diagnosis of NSSDs is established with any 1 abnormality or any combination of abnormalities. Adapted from Winslow et al. 31
The available literature suggests that patients with NSSD on manometry (23.1%-43.9%), especially those with a negative pH study (23.9%), would be expected to have a higher likelihood of a poor surgical outcome and persistent symptoms after ARS. In these patients, an evaluation to rule out anatomic/physiologic failure should be first performed. If no specific cause can be identified, then medical therapy aimed to impact the underlying sensory motor dysfunction can be considered. 33
The Impact of Preoperative LES Status and Esophageal Contractility on Postoperative Dysphagia
In a study led by Blom et al, 34 authors investigated if preoperative manometric parameters predict new-onset dysphagia following ARS. They found that preoperative LES competence (P = .02) and mean LES resting pressure (P = .04) were the only preoperative variables associated with the development of postoperative dysphagia. The severity of the new-onset dysphagia also showed a correlation with mean preoperative LES pressure (P = .07). This study also reported a significant correlation between preoperative LES resting pressure and postoperative LES resting pressure (r = .48, P = .01). Several other studies have observed that the magnitude of postoperative resting pressure and residual pressure are associated with the development of postoperative dysphagia.35,36
In a study evaluating factors predicting dysphagia following MSA, elevated preoperative DCI was not found to be a predictor of postoperative dysphagia. However, authors reported that among patients with hypercontractile esophagus (defined by DCI > 40 000 mmHg cm sec), there was a stepwise increase in the rate of persistent dysphagia with an increase in the preoperative DCI. 37
The Impact of Esophageal Hypomotility on the Outcome
Presence of a hypotensive LES is the most common manometric findings in patients referred for preoperative manometry. Several studies report that this rate is greater than 50%. This is consistent with reports in the literature that refractory response to medical therapy is frequently associated with mechanically defective LES. 38 In contrast to patients with NSSDs, those with hypotensive LES and a positive pH study would have the highest likelihood of a favorable result after ARS. 28
Esophageal body hypomotility is a very common finding in GERD patients, affecting 21% to 49% of patients referred for consideration of ARS. 39 Although some studies of primary Nissen fundoplication have shown that the presence of ineffective esophageal motility (IEM) or low-amplitude contraction in the distal esophagus, is not associated with higher rates of postoperative dysphagia following Nissen fundoplication,24,40 studies on revisional ARS have reported different conclusion. Furnée et al found that adequate preoperative distal esophageal contraction amplitude is an independent predictor for resolution of dysphagia in patients who underwent revisional ARS. Their explanation for this observation was that there is a subgroup of patients with borderline esophageal motility reserve that are at risk for dysphagia after construction of a suboptimal wrap (not short or “floppy” enough) or a tight crural closure. Therefore, surgeons should be aware that reoperation may not resolve the dysphagia in those with low distal esophageal amplitude established prior to reoperation. 41
Using iBP, the GEJ resistance measured following MSA was found to be higher than values reported for Nissen fundoplication. 14 Therefore, in order to avoid persistent postoperative dysphagia, the force of esophageal peristalsis must be incorporated into patient selection, such that it is sufficient to overcome the elevated resistance imposed by the LINX device. In a recent study, DCI < 750 mmHg cm sec, distal wave amplitude <43 mmHg, and less than 80% peristaltic contractions on preoperative manometry were found to be risk factors for postoperative dysphagia. 42 Using these parameters, a nomogram has been constructed to allow prediction of postoperative dysphagia that can be used in patient selection and preoperative counseling when offering MSA to a patient.
Assessment of esophageal body function is particularly important in patients with laryngopharyngeal reflux (LPR), as esophageal body function has been shown to correlate with the severity of LPR measured by the number of symptoms (Figure 5). In addition, LPR patients with a normal esophageal motility are more likely to have relief of their symptoms compared to those with impaired esophageal motility (78% vs 25%, P < .05). 43
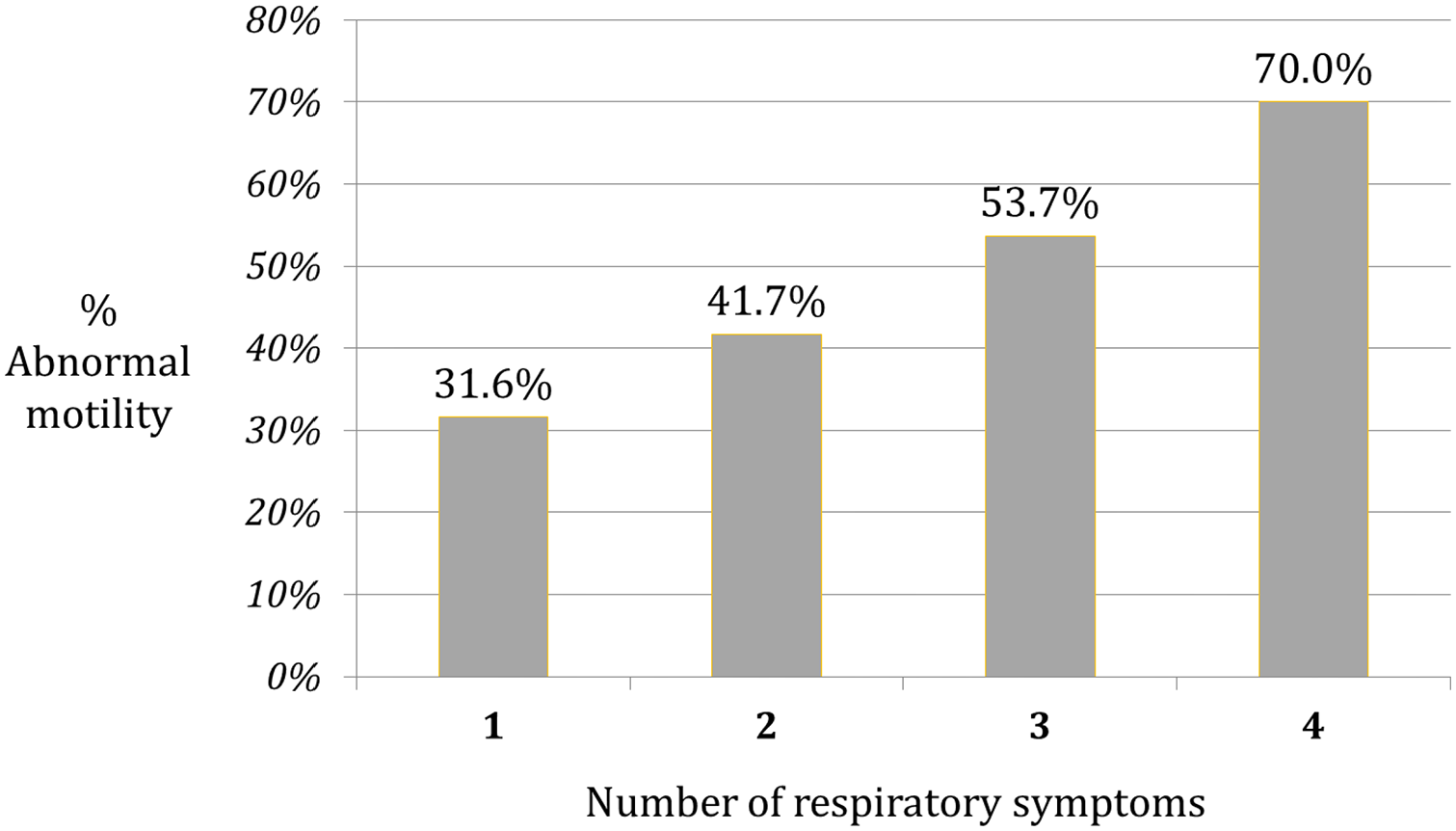
Prevalence of abnormal esophageal motility in 54 patients with respiratory symptoms and increased esophageal acid exposure, stratified according to the number of reported respiratory complains (P < .05), from DeMeester et al. 43
IEM is a very common manometric abnormality (20%-30%) in patients referred for ARS, yet a standard clinical approach for this diagnosis does not exist. Studies on the impact of IEM on the surgical outcomes report inconclusive results. Esophageal clinical physiology experts have identified a need to define distinct IEM phenotypes. Mello et al from Gyawali’s lab has demonstrated the presence of distinct cohorts of IEM manifesting different motor characteristics following fundoplication. This group of authors have demonstrated that these patterns could be predicted on provocative testing with multiple rapid swallows (MRS) prior to fundoplication, in that the degree of augmentation of post-MRS smooth muscle contraction varied significantly within these sub-types. 44
Results of the above studies show that foregut function testing allows collection of preoperative parameters that may help predict a favorable surgical outcome or occurrence of dysphagia following ARS. This information can be then used for risk stratification and shared with patients during preoperative counseling. This approach allows both the patient and surgeon to form realistic expectations about the degree of symptom relief and risk of complications after the surgery. Factors other than esophageal motor function also need to be included in the preoperative counseling. Previous studies have shown an abnormal DeMeester score, a typical primary symptom and clinical response to acid suppression therapy are predictors of a successful outcome after Nissen fundoplication. 45 A similar study on patients who underwent MSA showed that age younger than 45 years, male sex, GERD-HRQL total score >15, and an abnormal DeMeester score are indicative of a favorable outcome. 46
Need for Provocative Maneuvers and Novel Manometric Parameters
Due to the limitations of standard techniques during straightforward manometry there are many questions about the complex interplay between the impact of ARS, manometric changes, and patient symptoms that are left unanswered. Novel techniques must be explored in order to sufficiently evaluate esophageal function. The current literature suggests that physiological challenges increase the sensitivity and specificity of HRM studies obtained during preoperative assessment.47,48 Other studies have shown the importance of adding multiple rapid swallows (MRS) during a manometric protocol, which is a marker of contractile reserve of the esophagus. 49 Incorporating impedance into pressure flow parameters has been suggested to be of value. In 1 study, using impedance data, a newly defined dysphagia risk index appeared to be helpful in identifying patients at risk for post-fundoplication dysphagia. 50
The focus of the recent studies has been on the LES resting pressure and integrated relaxation pressure (IRP) as the markers of resistance at the EGJ, and IRP is a major component of the Chicago Classification in the characterization of several disorders. These parameters do not take into account all factors, particularly as related to surgical therapies. Intrabolus pressure (iBP) is a manometric measurement of the force exerted on a bolus during esophageal transit. It is a complex measurement which takes into account not only contractile force but also resistance to flow. 14 Quader et al 51 reported that iBP may be significantly elevated in patients with obstructive processes compared to those without obstructive processes as evidenced on upper endoscopy. With this in mind, iBP may provide a more complete reflection of outflow resistance especially during the evaluation of dysphagia following surgery.
In addition, novel 3D high-resolution manometry is a promising technology that can provide further insight into pressure morphology of complex area such as EGJ and the impact of surgical intervention on it. In this technology, the pressure sensors are spaced more closely together and the radial characteristics at each axial position are preserved (Figure 6).
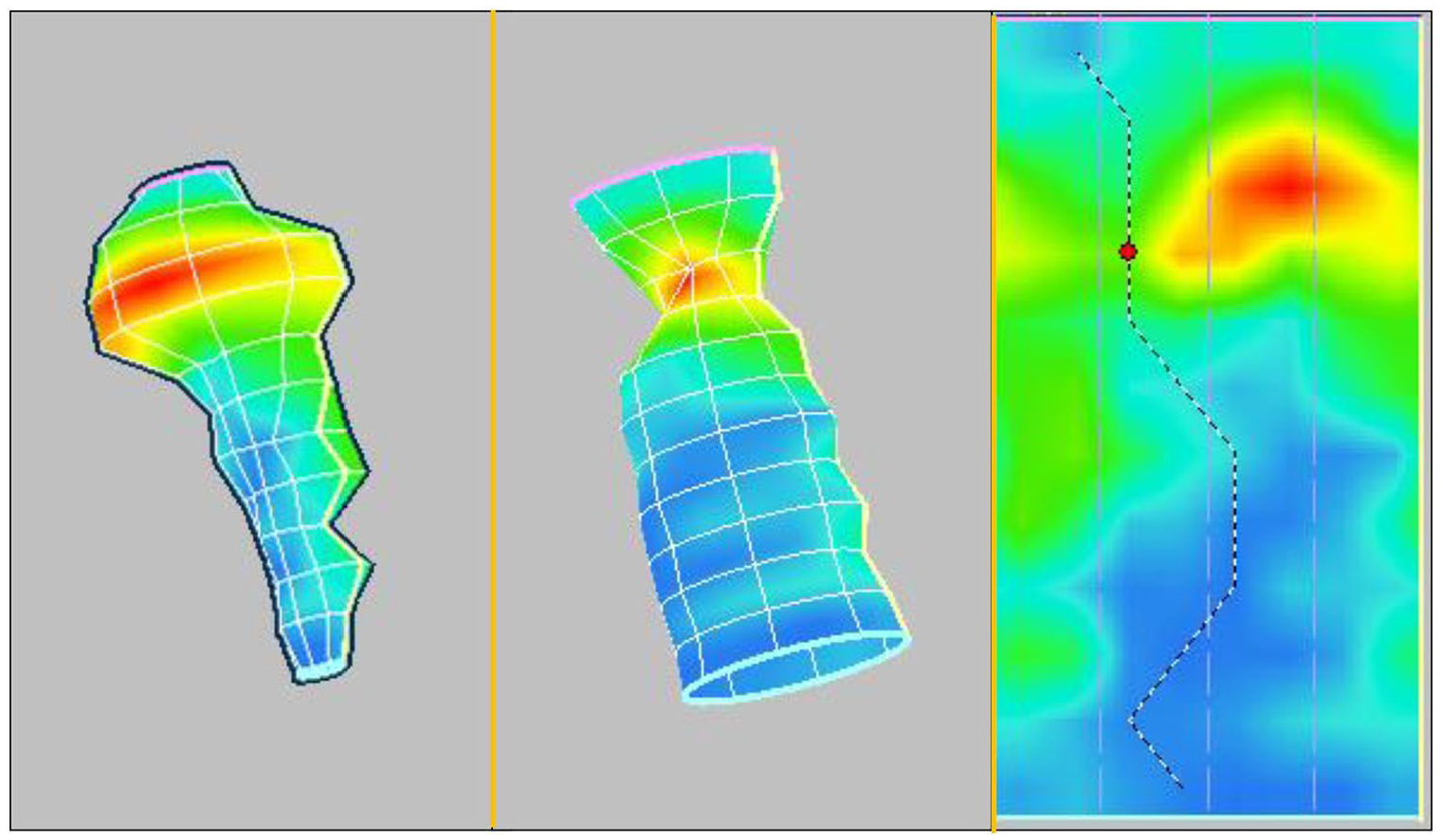
3D high-resolution manometry recordings of the EGJ. This technology allows preservation of the radial characteristics at each axial position.
Role of Manometry in Surgical Discoveries and Personalizing Antireflux Therapy
Our insight into a process and our capability to modulate it, is only as good as our ability to measure it. Therefore, objective measurements of GEJ function hold the key to better understanding of the mechanics of antireflux procedures and thereby maximize its benefits while minimizing adverse outcomes. Decades of research have led to a far better understanding of the pathophysiology of GERD. The scientific revolution that occurred in the 1950s and 1960s, brought science and research into the mainstream of clinical medicine. The federal government has begun to invest heavily in biomedical research. Esophageal manometry developed as a result of this movement and has since been utilized in clinical practice and investigational research. The technique of esophageal manometry and other physiology tests that became available in mid 1970s were used by founders of modern esophageal surgery (Figure 7) to combine investigative research studies with their routine clinical care, and in doing so became esophageal surgeons and so much more. They fostered the maturation of esophageal surgery into a scientific discipline.
Drs. Tom DeMeester (left) and, David Skinner (right), whose work established the field of foregut surgery as a scientific discipline.
Development of testing for HER2 overexpression in the 1990s followed by invention of Trastuzumab, a recombinant monoclonal antibody targeting HER2, demonstrated the advantages of a targeted approach to treat cancer. 52 Molecular profiling to targeted agents is now recommended practice in the field of oncology. In 2010, Eric Schmidt, Google CEO at that time said, “The technology will be so good it will be very hard for people to watch or consume something that has not in some sense been tailored for them.” Recent technologic advancement in medicine has also provided the opportunity for an individualized tailored therapeutic approach in all medicine disciplines. Foregut surgery is not an exception to this rule. The foregut surgeon in the 20th century had to decide between partial or full fundoplication as the only interventions available to treat reflux disease. Several other interventions are now added to the Foregut surgeon’s armamentarium in the 21st century. These include construction of fundoplication with various degrees, MSA, as well as several endoscopic interventions such as transoral incisionless fundoplication (TIF) created with the EsophyX device, endoscopic radiofrequency anti-reflux therapy (Stretta), anti-reflux mucosectomy (ARMS), and other still investigational techniques. This provides a unique opportunity for the foregut surgeon to individualize the antireflux intervention based on reflux disease state, physiologic parameters, and expectation of the patient. The foundation for any personalized medicine platform is the acquisition of relevant data. Esophageal manometry detects findings associated with favorable outcome or incidence of dysphagia after ARS and can be used as a tool to aid surgeon balancing all the patient factors in crafting an operation for the individual patient.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.