
Abstract
Background:
Outcomes of laparoscopic revisional surgery involving Magnetic Sphincter Augmentation (MSA) have not been clearly delineated, whether MSA was the presenting or the revisional surgery. We compared safety and clinical outcomes of 4 main categories: fundoplication revised to fundoplication (F-F); fundoplication to MSA (F-M), MSA to fundoplication (M-F) and MSA to MSA (M-M).
Methods:
Analysis of prospective data from 10 U.S. sites participating in the Registry of Outcomes of Anti-Reflux Surgery (ROARS). Patients had undergone at least one prior procedure on the esophagogastric junction with subsequent need for revisional surgery.
Results:
Between 2/1/2005 and 1/19/23, 742 patients underwent 819 revisional surgeries, of which 645 patients had 722 surgeries in the 4 main categories. Seventy-six percent had their prior operation elsewhere. Indications for reoperation (GERD, hiatal hernia, dysphagia, gas-bloat) were similar across categories. Preoperative and intraoperative findings disclosed disruption of prior hernia repair in 80% and 97% of patients respectively. Hernia size was larger with an antecedent fundoplication (13% >5 cm, 37% 3-5 cm) compared to patients with prior MSA (1.5% >5 cm, 18% 3-5 cm (P < .0001). Revision of fundoplication resulted in 11% intraoperative complication rate, versus 2% for MSA. Six hundred patients (73.2%) were followed a mean of 2.7 years. Subsequent operation was performed on 77 (12.7%) a mean of 2.5 years; no difference between categories. Kaplan-Meier analysis showed equivalent subsequent reoperation rates at 5 years (20% ± 5%). Similar improvements in GERD-HRQL, bloating, dysphagia scores, ability to belch or vomit were seen.
Conclusions:
Over 95% of patients had disruption of the hiatus requiring repair, though prior MSA was associated with far fewer >3 cm hernias than prior fundoplication. Patients with an antecedent MSA can be revised with similar safety and outcomes as those having an antecedent fundoplication. MSA has equivalent results to fundoplication when used as a revisional procedure post antecedent fundoplication.
Keywords
Abbreviations
GERD: Gastroesophageal Reflux Disease
MSA: Magnetic Sphincter Augmentation
(F-F): Revision of prior fundoplication to fundoplication
(F-M), Revision of prior fundoplication to MSA
(M-F), Revision of prior MSA to fundoplication
(M-M), Revision of prior MSA to MSA
BMI: Body Mass Index
ANOVA: Analysis of Variance
PPI: Proton Pump Inhibitor
PRN: As needed
LA Grade: Los Angeles Grade
CLE: Columnar Lined Esophagus
EGD: EsophagoGastroDuodenoscopy
HH: Hiatal Hernia
ASM: Acid Suppressive Medication
GERD-HRQL: gastroesophageal reflux disease-health related quality of life
Key Learning Points
Patients with an antecedent MSA can be revised with similar safety and outcomes as those having an antecedent fundoplication.
Magnetic Sphincter Augmentation has equivalent results to fundoplication when used as a revisional procedure post antecedent fundoplication.
Disruption of the hiatus requiring surgical revision was found in 90% of patients with antecedent MSA.
Introduction
Hiatal hernias and associated gastroesophageal reflux disease (GERD) have a substantial impact on patients’ quality of life, prompting the need for surgical interventions aimed at symptom relief and anatomical correction. However, due to the reconstructive nature of these procedures, revisional surgery may be required over time. Surgical revision of prior antireflux or hiatal hernia procedures is performed when de novo symptoms, recurrent GERD, or recurrent hiatal hernia cannot be managed medically or observed. A logical question is whether revisional surgery should utilize the same methods as the prior surgery, or use a different approach. Among the various surgical options available for hiatal hernia repair and GERD management, fundoplication has been the historical standard, with gastrectomy and Roux-Y reconstruction reserved as a salvage operation. 1 The introduction of Magnetic Sphincter Augmentation as a novel method to treat GERD, 2 demonstration of long-term success 3 and research supporting its utility when accompanied by hiatal hernia repair regardless of size,4-6 raises the question of the use of MSA in revisional surgery in such instances.
The comparative effectiveness of MSA as a revisional surgery, both when transitioning from fundoplication to MSA or when using MSA as the revisional procedure itself, has not been reported. This study reports the outcomes of MSA and Fundoplication in revisional surgery after prior Fundoplication or MSA.
Materials and Methods
Study Design
A multi-center prospective Registry (Registry of Outcomes of AntiReflux Surgery, ROARS) (ClinicalTrials.gov Identifier: NCT02923362) was begun in 2016 to evaluate the safety and results of laparoscopic MSA and fundoplication. Ten U.S. sites with surgeons experienced in MSA implantation participated in the Registry.
Patient Population and Grouping
The Registry allowed inclusion of patients undergoing revisional surgery on the esophagogastric junction regardless of whether the prior surgery was performed for GERD or for a paraesophageal hernia. Patients included in this study of revisional surgery were required to have undergone at least one prior procedure on the esophagogastric junction which had failed and met appropriate clinical standards for having revisional surgery.
Failure was defined as the need for a subsequent reoperation and was the primary study endpoint. Patients having a subsequent operation at the same site are captured in the database. Additional information on subsequent operation was accrued from patient-reported outcomes collected annually for up to 5 years, which includes a question about need for subsequent reoperation.
Patients were grouped according the type of prior surgery performed and the type of revisional surgery performed: fundoplication to fundoplication (F-F), fundoplication to MSA (F-M), MSA to fundoplication (M-F), and MSA to MSA (M-M), and Other. As there was significant variation in the “Other” including 50 unknown procedures, characteristics of the “Other” category were included in baseline characteristics and are not included in outcome results
The GERD-HRQL has 10 questions scored 0 to 5 with a higher score indicating a worse quality of life. As not all patients were operated on for GERD, we restricted analysis to patients with a worst GERD-HRQL score (whether on or off Acid-Suppressive Medication- ASM) at baseline of ≥15 as this cutoff has been used in prior antireflux surgery studies. 2
Statistical Methods
Categorical parameters are displayed by number and frequency; normal or nonparametric continuous parameters are expressed as mean (SD) or median [interquartile range [IQR]]. Kaplan-Meier analysis was used to compare durability and to account for patients lost to follow-up. Comparative analyses (chi-square), and ANOVA were used to compare groups as appropriate using XLStat software.
Results
Patient Disposition, Demographic and Clinical Characteristics
Between 2/1/2005 and 1/19/2023 742 patients underwent 819 revisional surgeries at 10 sites. Patients were categorized based on presenting surgical procedure and revisional surgical procedure. The majority of patients (76.4%, 567/742) had a prior operation elsewhere. When reported, paraesophageal hernia was the reason for the prior surgery in 26% of operations (83/317).
Baseline characteristics are shown in Table 1.
Baseline Characteristics by Category of Revision. Most Baseline Characteristics Reflect Characteristics at a Given Reoperation.
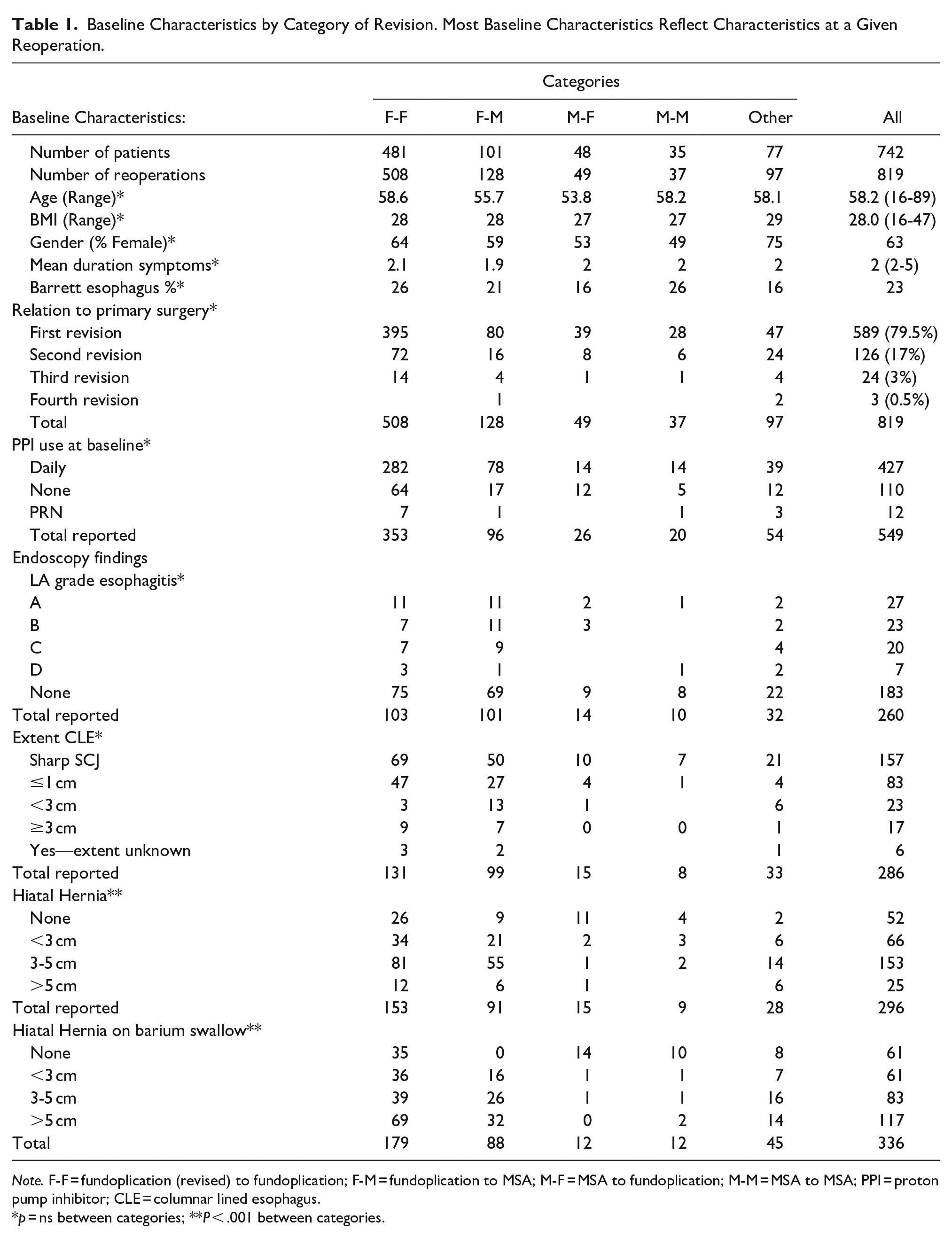
Note. F-F = fundoplication (revised) to fundoplication; F-M = fundoplication to MSA; M-F = MSA to fundoplication; M-M = MSA to MSA; PPI = proton pump inhibitor; CLE = columnar lined esophagus.
p = ns between categories; **P < .001 between categories.
A hiatal hernia was found in 82% of patients at baseline EsophagoGastroDuodenoscopy (EGD) and on baseline imaging in 80% of patients. The incidence in patients with a prior fundoplication rate was 86% (EGD and imaging) compared to 36%−37.5% (Imaging-EGD) for prior MSA (Chi-Sq < 0.0001). Additionally, 63% of hernias reported at baseline imaging in prior fundoplication patients were over 3 cm, compared to 12.5% of patients with a prior MSA (Chi-Sq < 0.0001).
Indications for Reoperation
The most common indications for reoperation in patients with a prior fundoplication were GERD (42.7%), symptomatic hiatal hernia (39.1%), dysphagia (12.4%) and gas-bloat (5.4%). For patients with prior MSA the indications were GERD (57%), dysphagia (24.3%), symptomatic hiatal hernia (17.1%) and gas-bloat (1.4%) (p = ns Less frequent indications for reoperation on antecedent fundoplication patients included fistula (1), abscess (2) and for prior MSA included erosion (3, all 12 bead devices), discontinuity (2), and need for MRI (1). In 234 cases the reason for reoperation was not reported.
Operative Findings
Operative indications and category of revision are shown in Figure 1.
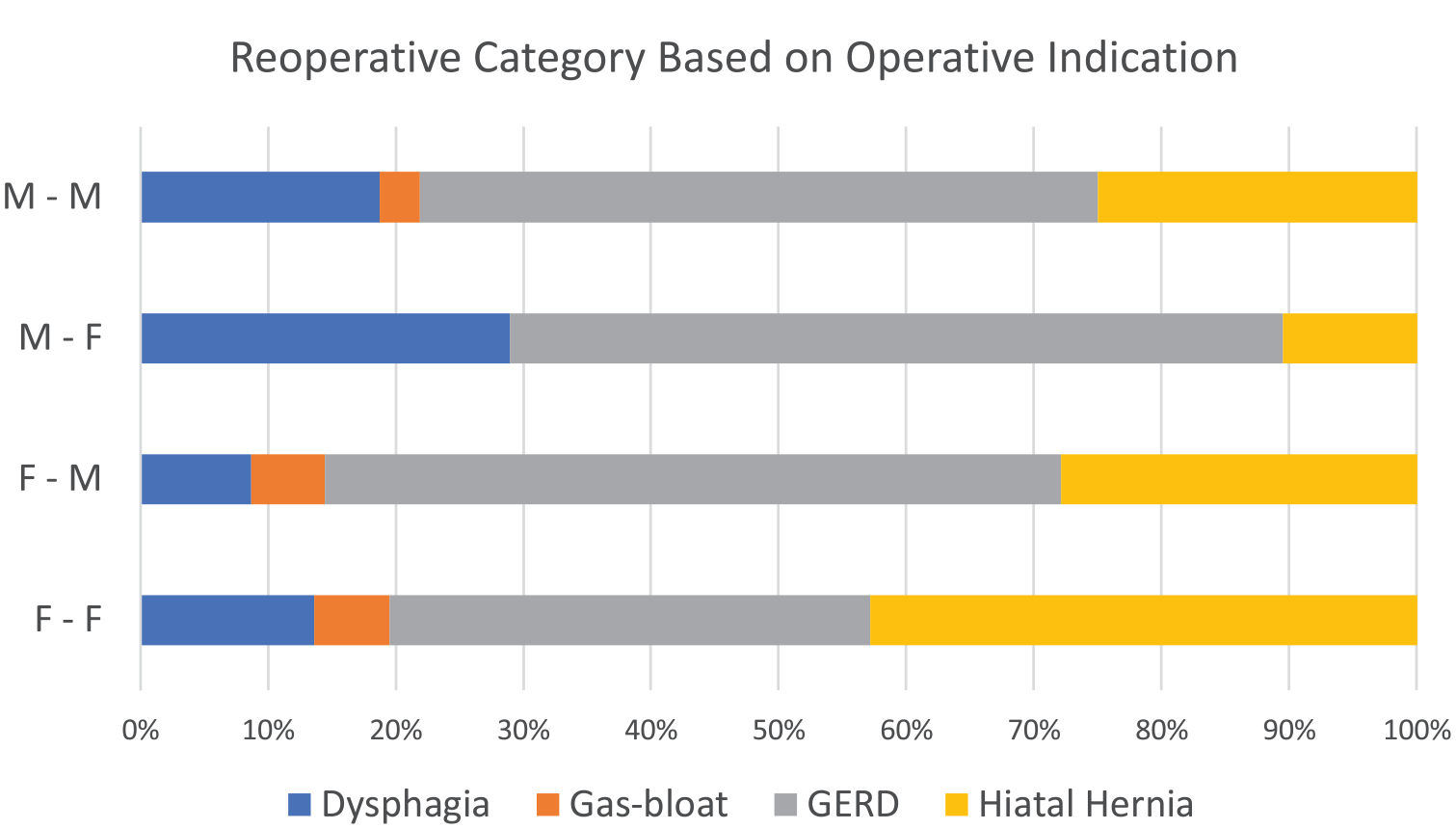
Revisional Surgery: Operative indications by category of revision performed.
Numbers of reoperations by category (excluding “Other” as types of operation in this category were extremely varied) with associated operative time, incidence of mesh use, and presence of hiatal hernia at surgery are detailed in Table 2 (p = ns across categories).
Operative Findings.
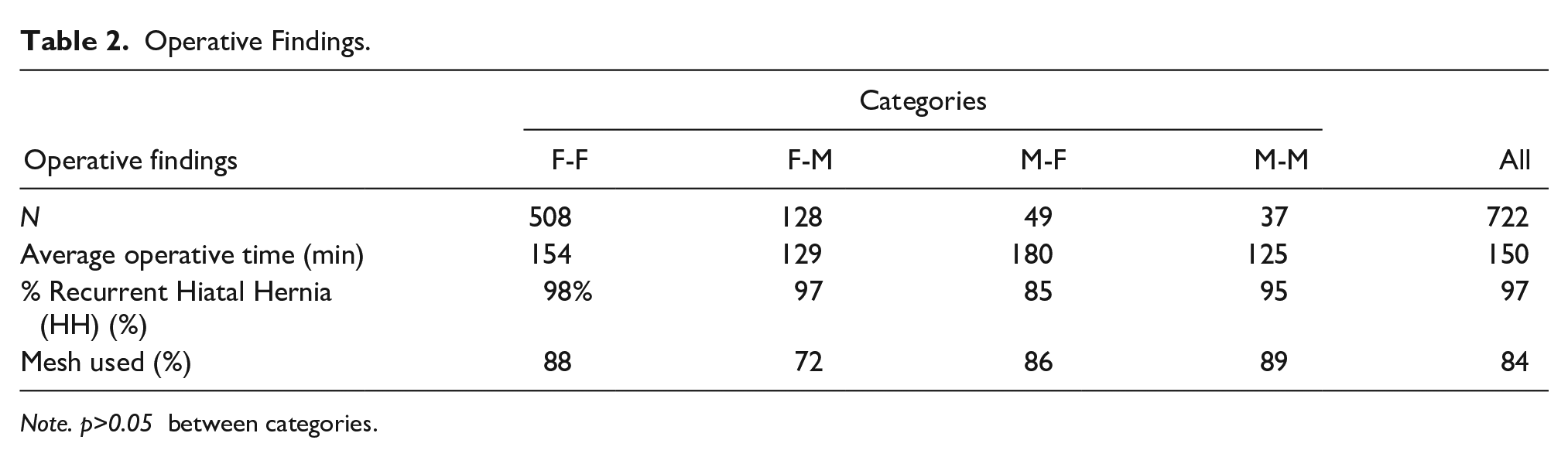
Note. p>0.05 between categories.
Prior MSA was associated with fewer >5 cm hernias (1.5% vs 13%) and 3 to 5 cm hernias (18% vs 37%) than prior fundoplication (ChiSq P < .0001).
For patients revised to fundoplication, a complete (360°) fundoplication was performed in 41% of patients, a posterior fundoplication in 34% of patients, and an anterior fundoplication in 25% of patients. For patients revised to MSA, 52 patients were implanted with a size 16 bead, 48 with a 17, 35 with a 15, 14 with a 13 bead, and 1 each with a 12 and 13 bead device. When a known sized MSA was replaced with an MSA, 2 were downsized by 1 bead, 5 remained the same, 4 upsized 1 bead, 5 upsized 2 beads.
Safety
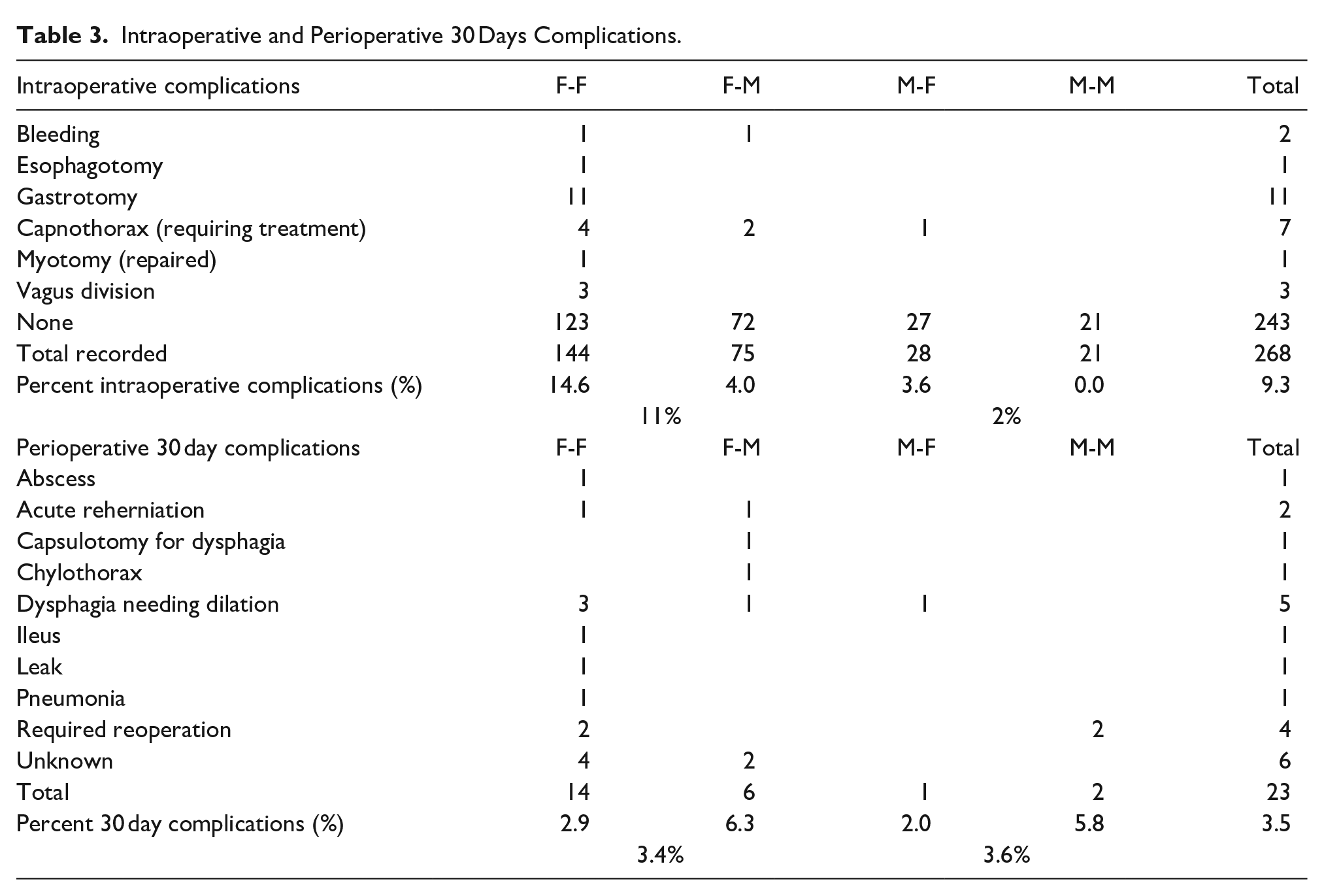
Intraoperative complications were reported in 25 (9.3%) of patients; 11% in patients with a prior fundoplication and 2% in patients with prior MSA. Injury to esophagus or stomach was not reported in patients having had a prior MSA. There were no perioperative (30 days) deaths. Complications requiring hospitalization or intervention were reported in 23 patients, though follow-up may be incomplete. Complications by specific category of revision are reported in Table 3.
Intraoperative and Perioperative 30 Days Complications.
Durability
Follow-up was obtained in 600 (73.2%) patients at a mean of 2.7 years. A subsequent operation was performed on 77 (12.7%) of patients a mean of 2.5 years postoperatively, and was not significantly different between categories.
Kaplan-Meier analysis of freedom from subsequent operation (eg, second to third operation) is illustrated for all patients and for the 4 categories of revision, Figure 2. There was no significant difference in time to subsequent operation by category.
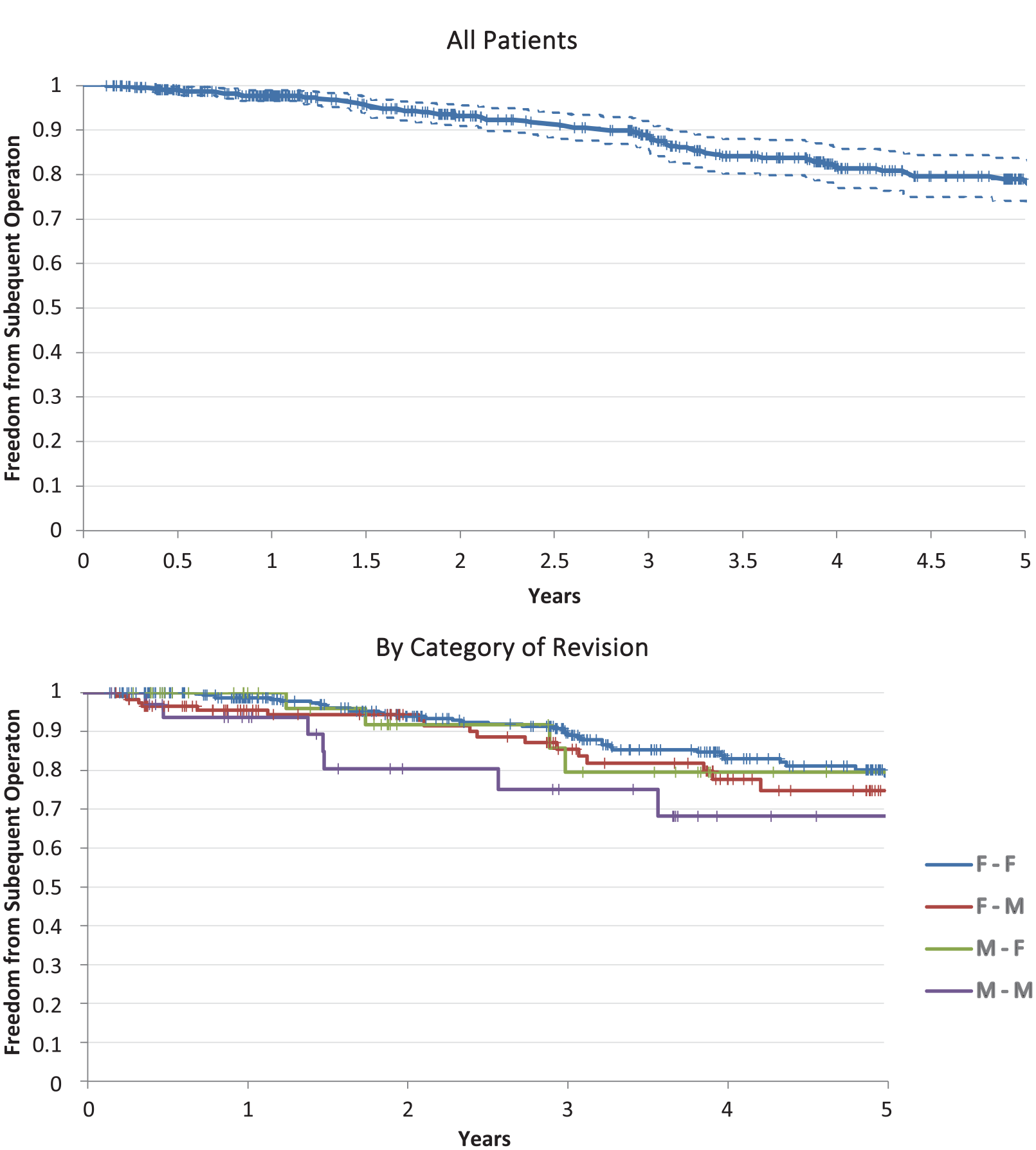
Freedom from subsequent operation by time. There is no significant difference by category.
Analysis showed no difference in outcomes when categorized by procedure number (P = .91 logrank), though did trend worse with larger hernia sizes (P = .141 logrank), Figure 3.
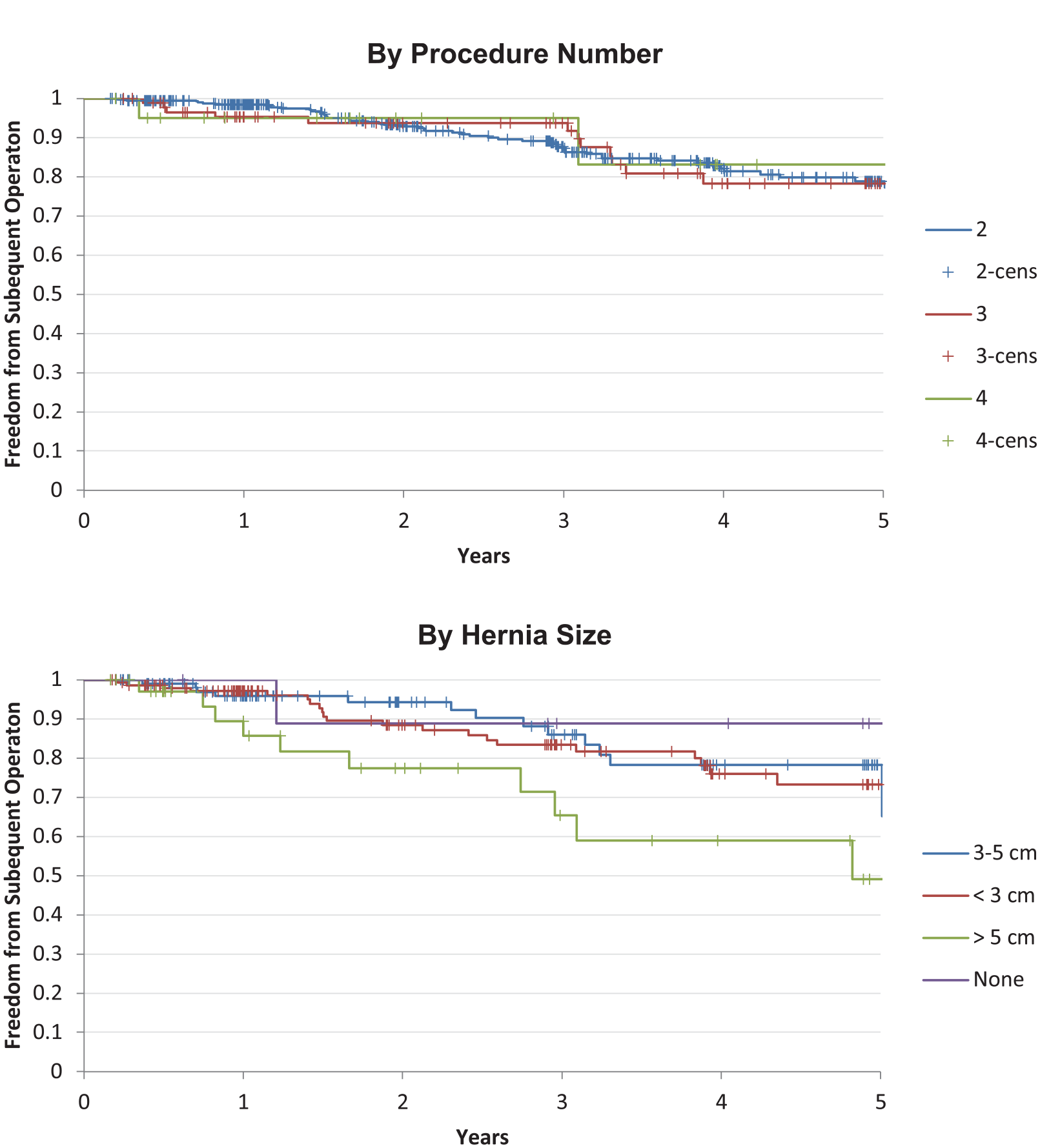
Freedom from subsequent operation by procedure number and hernia size. p = ns by procedure number or hernia size.
Quality of Life Assessments
Patient-reported quality of life assessments were available on 284 patients at a mean of 852 days (no differences in times between categories).
GERD-HRQL
Between Categories there no significant difference in Baseline and Post-Operative GERD-HRQL, or Regurgitation scores. Within each Category there was significant improvement from Baseline to Postoperative status, Table 4.
Baseline and Postoperative GERD-HRQL, Regurgitation, and Dysphagia Scores by Category.
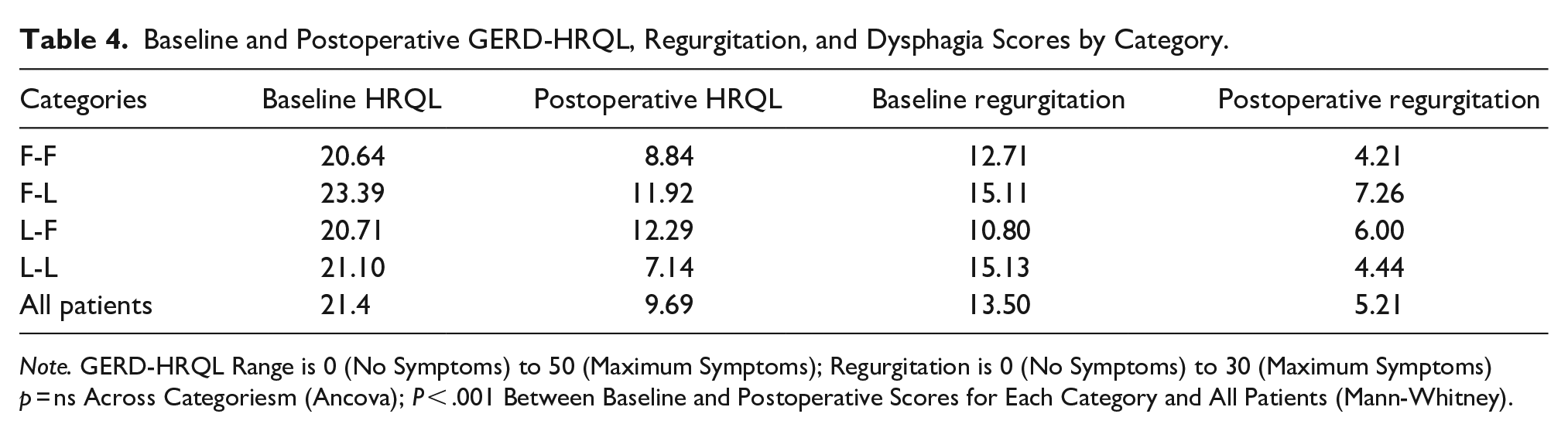
Note. GERD-HRQL Range is 0 (No Symptoms) to 50 (Maximum Symptoms); Regurgitation is 0 (No Symptoms) to 30 (Maximum Symptoms) p = ns Across Categoriesm (Ancova); P < .001 Between Baseline and Postoperative Scores for Each Category and All Patients (Mann-Whitney).
There was no significant difference in final GERD-HRQL scores between second (310 patients) third (60) and fourth (15) procedures (9.5., 10.5, 10.2, respectively).
Bloating, Belching, Vomiting
One question in the GERD-HRQL evaluates whether patients experience a gassy or bloating feeling (0-5). Patients reported an average of 25% improvement (from 2.4 to 1.8), with no significant differences between Categories.
Ninety-three percent of patients revised to MSA reported being able to belch, compared to 89% revised to fundoplication (p = ns). Ability to vomit was reported in 61% of patients revised to fundoplication, 78% of patients revised to MSA (P = .03).
Dysphagia
GERD-HRQL has 2 questions related to dysphagia—difficulty with swallowing and pain with swallowing (0-5 each). Combining these 2 scores (0-10), revisional surgery improved dysphagia across all categories (3.5-2.1), with no significant differences between categories.
Discussion
The most significant new findings of this study are (1), that patients with an antecedent MSA can be revised with similar safety and outcomes as those having an antecedent fundoplication and (2), that MSA has equivalent results to fundoplication when used as a revisional procedure post antecedent fundoplication.
Reoperation following a failed fundoplication has traditionally involved repairing a (recurrent) hiatal hernia in the majority of patients followed by a choice of either redoing the fundoplication or converting to a Roux-Y gastric bypass. As our experience with using MSA successfully as a primary operation for GERD grew, we began using MSA as an option for revision of a failed fundoplication. Though the initial impetus was a few patients seeking relief of severe gas-bloat after a fundoplication, we began seeing potential benefit in settings where the prior fundus had been deformed as it herniated that recreating the fundoplication was problematic During reoperative surgery it is frequently challenging to obtain the 3 cm of visible intra-abdominal esophagus (measured as the distance from the angle of His to inferior edge of crural diaphragm) that is required for a fundoplication to be placed around the esophagus and not proximal stomach. An MSA, with a bead diameter of 6.8 mm, should only require 7 mm of esophagus between the angle of His and inferior edge of the crual diaphragm to circumscribe the esophagus without involving the proximal stomach. We therefore considered MSA an alternative to performing a Collis gastroplasty when visible abdominal esophageal length was <3 cm. Additionally, MSA failures can been revised to removal of the MSA with creation of a fundoplication, or to keeping or replacing the MSA. Results of these categories of revisional procedures (F-M, M-F, M-M) have not been reported nor have they been compared to revision of failed fundoplication by redo fundoplication (F-F).
Revisional surgery from prior fundoplication to fundoplication has reported subsequent reoperation rates between 5% and 22%.1,7,8 These reports have limited patient selection to those undergoing their primary surgery for GERD and have excluded patients presenting with a paraesophageal hernia. Since 2015 the authors have placed MSA during primary repair of paraesophageal hernias with results comparable to those obtained utilizing fundoplication.4,6,9 Included in this study were the 26% of patients who presented initially with a paraesophageal hernia, regardless of whether the revisional surgery was a fundoplication or MSA.
The data used for this study was collected prospectively in the Registry of Outcomes of Antireflux Surgery (ROARS), and as such has expected limitations of a registry, including selection bias and lack of a priori standardization of technique and incomplete follow-up in 27% of patients. However the large number of patients collected in such a multi-center database contributes significantly to a real-world understanding of patient outcomes and Kaplan-Meier analysis of large numbers addresses incomplete follow-up. There is lack of data on whether the primary operation was indicated for GERD or for PEH in many patients, and potential incomplete recording of complications. The survival analysis of revision of MSA to MSA, though not meeting statistical significance potentially due to small numbers of patients, suggests this may not be as effective as the other revisional procedures. Further research may help further refine these limitations.
Recognizing the above limitations, baseline characteristics were not significantly different between categories. There was a trend toward a higher proportion of patients with MSA having GERD and dysphagia as a primary reason for reoperation, whereas prior Fundoplication patients were reoperated on more often for hiatal hernia or “unknown.”
The rate of recurrent hernia during reoperation for MSA has not previously been reported. Disruption of the hiatus requiring repair was observed in 90% of patients with an antecedent MSA, similar to that for fundoplication.10-12 Size of hernia at reoperation was significantly smaller in patients with a prior MSA compared to fundoplication, with hernias ≥3 cm in 21% of MSA versus 60% of fundo, and for hernias >5 cm 1.6% versus 13% respectively (chisq < 0.0001). This difference may be due to the early use of MSA being limited to hernias <3 cm.
MSA was associated with fewer intraoperative and 30-day complications, especially esophageal or gastric injury, than was revision of fundoplication to fundoplication. In this carefully selected group of patients, operated on by surgeons with significant experience in using MSA as a primary surgery, no erosions were reported. Meticulous operating technique was employed and suspicion of injury that could lead to erosion was agreed upon as contraindication to implantation of MSA by all surgeons.
Durability was 80% at 5 years and was similar for all categories of repair. Quality of life assessments improved significantly and were also comparable across all categories. Our results are comparable to results limited to patients whose primary operation was for GERD, even though this study included patients with paraesophageal hernias at their initial operation.7,8,13-19 Roux-Y conversion was used in a very small number of patients, and number of prior operations was not associated with changes in outcomes.
Conclusion
All categories of revision found disruption of the hiatus requiring repair, though prior MSA was associated with far fewer >3 cm hernias than prior fundoplication. Patients with an antecedent MSA can be revised with similar safety and outcomes as those having an antecedent fundoplication. MSA has equivalent results to fundoplication when used as a revisional procedure post antecedent fundoplication.
Footnotes
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Reginald Bell M.D. is a consultant for Ethicon. F.P. “Tripp” Buckley is a consultant for Ethicon. John Lipham is a consultant for Ethicon. Subigya Parajuli has no conflicts. Rachel Heidrick has no conflicts.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No funding was received for this research. ROARS supported by a grant from Ethicon.
Ethical Approval
The design and execution of this study was obtained from the local reviewing committee (IRBNet [457630-22 approved 8/18/2022]).