
Abstract
The paper offers an exploration of triadic attachment dynamics in families with a child with a diagnosis of autism. The Meaning of the Child (MotC) framework was employed as part of a multiple case study design with 18 parents (9 couples) in order to examine their representation of parenting and relationship with their child. The MotC analysis employed concepts of parental sensitivity, mentalisation and reflective functioning, and a triadic, analysis was added to consider the family relational processes. The findings indicate that the parents were significantly influenced by the use of a dominant ‘autism discourse’. ‘Autism’ in their child presented a severe challenge for them and could foster a sense of disempowerment and emotional withdrawal. Locating the difficulties as reflecting ‘autism’ could also serve to detour conflicts between the parents, and in the parents themselves, trapping the family in unresolved anger or fear that could neither be named nor its impact addressed. Autism discourse tended to rob the actions of family members of interpersonal meaning, rendering conflict fixed and unalterable and requiring them to mask the deep feelings inherent in these relational ruptures. The analysis included an exploration of the parents’ own childhood attachment histories which revealed that the parents were also driven by corrective scripts in wishing to form better relationships with their child than had been their own childhood experiences of parenting. A sense of failure to achieve these added to their sense of disappointment and frustration, but also indicated potential avenues for positive changes and growth.
Introduction
Bowlby (1988) suggested that there are two inter-related attachment systems: the child’s proximity and comfort-seeking system and a reciprocal parental care-giving system, both of which have an evolutionary survival function to enable the process of care-seeking and giving to occur. Ainsworth (1969) observed that a key feature of how the child’s attachment security developed was how sensitive, controlling, available and accepting of the child’s needs parents were able to be. Her pioneering work on parenting employed detailed and careful observations of laboratory and home-based interactions, but she also offered insightful formulations about the parent’s mental states: ‘the mother’s ability to perceive and to interpret accurately the signals and communications implicit in her infant’s behaviour’ (Ainsworth, 1969, p.1). The focus on exploring not just what parents do, but on their construing of the child, themselves and their relationship with the child has led to a number of approaches to assess parenting in terms of parent–child attachment connections (Benoit et al., 1997; George and Solomon, 2008; Grey and Farnfield, 2017a). These approaches have sought to develop our theoretical understanding of the connections between parenting and child development, and to build models of aetiology of children’s problems. These in turn serve to offer guidance for clinical and therapeutic practice and assessment of risk to children.
However, a more negative and contentious consequence of such research is the risk of potential blaming of parents for causing problems in their children. This is particularly sensitive topic in relation to autism since it is widely perceived that some clinicians and researchers had suggested that there may be some parental involvement in causation or even the severity of the presentation of the ‘symptom’ (Bettelheim, 1972). Such suggestions have regularly been criticised as being ‘parent blaming’ in suggesting that autism is anything other than a neuro-developmental condition (Dallos, 2019; McKenzie and Dallos, 2017). This has fuelled a great deal of discussion regarding parenting in relation to autism and also some heated debates about the nature of its overlap with attachment processes (Coughlan et al., 2019; McKenzie and Dallos, 2017). Currently, there is a debate between seeing autism as a ‘difference’ versus a ‘disability’: in effect regarding autism as more like a personality trait rather than a clinical difficulty. This is embedded in the widely prevalent view of autism as a neuro-development condition and people with the diagnosis as ‘neuro-atypical’. Also, autism has been re-classified in DSM 5 as an axis condition, whereby it is seen as embracing an extremely wide range and severity of difficulties. An unfortunate consequence of these debates and changes may be that parents of children with a diagnosis have to contend with a confusing and contested picture of their child’s condition.
An important line of research has developed linking parents’ understanding and perceptions of their children employing the concepts of mentalisation and reflective functioning (Grey and Farnfield, 2017b; Slade et al., 2005). Several studies indicate that parents’ abilities to be curious about and to try to understand their child’s mental states including their feelings, emotions and intentions is related to the child’s mental health and development. It has been argued that this is a more complex and challenging issue in the context of autism, with parents facing the dilemma of ‘mentalizing the unmentalizable’ (Slade, 2009), in that these children have a deficit in theory of mind and do not give communication cues to their parents that allows the parents to be able to develop their understanding of them. This argument can be seen to run through much of the autism literature in that the child is seen as fundamentally a ‘problem’ that the parents face, despite the alternative discourse that these children are just ‘different’. More broadly these children are regarded as presenting their parents with increased levels of stress which also promotes the argument that this in turn causes the widely observed findings of poorer levels of mental health in the parents (McKenzie and Dallos, 2017; Roberts et al., 2014).
However, there are a number of possibilities that arise from this perspective of the child with autism as presenting a special challenge to understand for the parents. One possibility is that the challenge makes it harder for parents to understand their child and consequently they develop a reduced level of mentalising and awareness of their child. Ansari et al. (2020) found that parents indicated use of fewer mental state concepts regarding their child with autism as compared to a non-autistic sibling. They also used fewer positive descriptors of their child with the autism diagnosis. A second possibility is that parents faced with the puzzle posed by their child’s restricted communication try harder to understand them. Consistent with this idea a study by Enav et al. (2020) suggests that parents compensate by developing higher levels of mentalisation (reflective functioning) in relation to their child with autism as opposed to their neuro-typical child. In contrast, Kirk and Sharma (2017) suggest that parents have similar levels of mentalisation towards their children but hold more negative emotionally toned descriptions of their child with autism. In short, these recent studies suggest a somewhat contradictory picture and use different ways of measuring mentalisation with only Enav et al. (2020) using the more sophisticated measure of reflecting functioning offered by the Parent Development Interview (PDI: Aber et al., 1985).
One problem with this line of explanation is that it appears to ignore the fact that at least some parents of children with a diagnosis are likely to employ insecure attachment strategies. In addition, there is considerable research to indicate that insecurity is in fact much higher in the population of parents with a child with a diagnosis of autism (McKenzie and Dallos, 2017; Teague et al., 2017). Studies indicate that many parents have a history of trauma and difficulties in their own childhoods (Roberts et al., 2014) and that the experience of parenting a child with a challenging condition may in itself trigger insecurity and traumatic states. Hence, we would therefore expect attachment insecurity to be a significant factor in the challenges for parents with a child with a diagnosis of autism. One conclusion from this may be that ‘mentalizing the unmentalizable’ may be even more difficult for parents who already, as a consequence of their own childhoods, have difficulty in mentalisation about their own and other’s actions and emotional states. Further, Siller and Sigman (2008) found that children with autism developed higher levels of joint attention and language if their parents showed higher levels of synchronisation during their play with them. This suggests a link between parental sensitivity and the subsequent development of communication skills in children with autism.
The studies also mention wider differences in how the parents perceive and feel towards their children. For example, Ansari et al. (2020) and Kirk et al. (2017) suggest that they may come to hold more negative views towards their children with the diagnosis of autism, possibly related to the increased demands and stress of parenting. What we know less about is how the complex and contested explanations that parents are presented with, and their own attachment experiences combine to form a ‘working mode’ of their child and their relationship with them. In an earlier study (Dallos et al., 2020), we found that parents could experience distress and disappointment at their child with the diagnosis of autism in not allowing them to achieve their ‘corrective scripts’ (Byng-Hall, 1988) of forming a better a relationship than they had had with their own parents. Also, as with much attachment research in general, the focus is almost exclusively on dyadic relationships, predominantly between the mother and the child. Systemic therapy emphasises the importance of considering triadic relationships (Dallos et al., 2015). This is particularly pertinent when a child is seen as demanding and challenging since the parents need to support each other and work together to manage the child with the diagnosis and also ensure that the other children are adequately attended to.
In a previous study (Grey et al., 2021), we employed the Meaning of the Child (MotC: Grey and Farnfield, 2017b; 2017a) analysis on the PDI interview with 16 parents of children with a diagnosis of autism. The aim of the study was to explore their understandings and feelings about their child, themselves and their relationship with the child. Our findings revealed a high level of trauma in the parents’ early childhoods that shaped the way they interpreted their child and the parent–child relationship. They all expressed clear positive intentions either to repeat positive aspects or to correct for negative aspects of their own childhood experiences of how they were parented. The parents’ own experiences, especially traumas shaped the outcomes of these positive intentions in many cases leading them to apply these in rigid ways that interfered with their abilities to be empathetic towards their children. The patterns of parenting were found in this sample to all fall within non-sensitive categories of the MotC, reflecting the levels of conflict and frustration in the parent–child relationship, and parental perceptions of caregiving in part shaped by the parents’ own trauma as much as the particular characteristics of the child. A significant finding was also that the diagnosis of autism came to have a significant role in shaping the parents’ understandings of their child and their relationships. We termed this their ‘autism discourse’, (which embodies the wider societal and professional explanations of autism) and we observed that it appeared to promote a short-circuiting of the ability and willingness to engage in mentalisation towards their child. Rather than staying curious about what their child might be feeling or thinking, they saw their child’s experience and ‘meltdowns’, as outside their parental influence, or alternatively, a controlling stance indicated by expression of hostility, for example, referring to their child special interests as ‘obsessions’.
Aims of the study
Attachment theory has arguably developed as and remains a largely dyadic approach. This present study is an attempt to extend our previous study beyond a dyadic focus to explore triadic interactional processes of how the two parents/carers working models of the child with autism combine and to understand how this might be experienced by the child. In turn we wanted to employ a systemic analysis to consider how the process in these triads may function and how the child’s ‘symptoms’ are shaped by, and in turn shape, the parent’s narratives and behaviours towards the child.
Methodology
Rationale and study design
In keeping with the study’s aim of developing systemic and relational understanding of the ‘problems of living’ encountered by families who have a child with a diagnosis of autism the study employed a qualitative, explanation building, multiple case-study methodology to study the attachment and caregiving narratives of 9 couples (18 participants). It also attempted to develop systemic formulations for each family of how both shaped and in turn were shaped by interactional processes in the family.
This methodology preserves the full rich context of the relationships within a family, allowing systemic processes to remain ‘intact’ and open to analysis. It is idiographic, avoiding the fragmentation of data into impersonal categories, factors or themes required by group-based quantitative methods, and some qualitative methods, which can hinder the observation and analysis of systemic and other localised and context-bound relationship and influences, as they are not preserved in generalised data (Maxwell, 2012; Miles and Huberman, 1994). Using multiple cases allows for comparison and the analysis of differences, and to refine theory by examining its ability to make sense of new contexts. The data is drawn from a larger study of an intervention for families with children who have a diagnosis of autism (McKenzie et al., 2020). Parents were interviewed using the Parent Development Interview (PDI: Aber et al., 1985), a semi-structured interview asking parents about their child, their relationship with their child and their experience of being parented. This latter section was expanded to include questions from the Adult Attachment Interview (AAI: George et al., 1985) to allow for analysis of any connections between childhood experiences and current relationships. Further questions were added around the diagnosis of the child’s autism and the parents’ experience of it.
As with the previous study, the researchers used the Meaning of the Child Interview system of analysis (MotC: Grey and Farnfield, 2017b; 2017a) to make sense of parental discourse in the PDI, because of the ability of the MotC to shed light on systemic and interpersonal aspects of parental thinking and feeling apparent in their speech. The MotC builds on the attachment-based discourse analysis of the Adult Attachment Interview (Crittenden and Landini, 2011) which examines the role of self-protection in transforming the meaning of experience, to look specifically at the meanings that shape parent–child relationships. In particular, the MotC looks at the parents’ management of arousal around the child in the context of the network of relationships the parent is situated in; not just at the level of the parent–child dyad, but also within the family system, wider social relationships and cultural setting in which the family is embedded (Grey et al., 2021). In addition, the section of the interview relating to the parents’ history was separately analysed for the childhood dangers experienced by the parent, and the self-protective representations of early relationships derived from it (Crittenden and Landini, 2011).
Once each of interviews was coded for both attachment and caregiving related discourse, the researchers used Miles and Huberman’s (1994) method of data reduction, display and conclusion drawing/verification (data collection having already taken place), to build a family formulation of the principal issues identified, based on triangulating the information from both parents with the inferred experience of the child (insofar as attachment theory would suggest the impact of the parental patterns might be). The study lacked an independent assessment of the child beyond the diagnosis, but the relational impact on the child of parental patterns of thinking and behaviour is central to the MotC analysis (Grey and Farnfield, 2017a).
Peer evaluation
The coding and analysis of the interviews was carried out separately by the first two authors and then integrated into a common analysis at an individual level. In order to integrate multiple perspectives, 10 transcripts were then coded separately by other coders and their analysis incorporated into the case formulations (in keeping with the study’s qualitative methodology). Then family formulations were separately developed and again discussed and revised to integrate the insights of the different authors.
Participants
18 participants (7 birth-fathers, 2 step-fathers and 9 mothers) were chosen randomly from the larger sample from a single UK region. This analysis needed a large enough sample to look at differences between participants, but be small enough that the particular social, family and cultural contexts of each parent were not lost in too much data reduction. Two stepfathers and 1 separated family were included so that the different dynamics of these family situations could be considered. The families were part of a research study developing a family-based intervention (SAFE – McKenzie et al., 2021) for family with a child with a diagnosis of autism. All of the families had received this systemic family-based intervention alongside sign-posting for continuing community based support. The families were all located in the southwest of the UK and White British. They were predominantly of middle class, five of them married and the child living with both parents, one family divorced and parents living separately and one divorced and re-constituted family.
The children had a diagnosis of autism with severity of autism levels 1 or 2, as described by DSM 5. These are more able children who can communicate verbally and do not have accompanying learning difficulties. All had been diagnosed within 12 months, as the researchers wished to focus on families who had not already received significant treatment or support around the child’s autism. The PDIs were carried out early in the process, prior to any intervention.
Ethics
The study relates to the analysis of an existing data set. The analysis is covered by the SAFE project’s ethics permission (South-West Exeter Research Ethics Committee, Reference: 17/SW/0192). Data protection procedures were followed, with some personal details changed or omitted to prevent identification.
Analysis
In order to preserve the essential features of the case-by-case analysis in this report we will focus on three families, selected to show both differences and similarities in the families we studied.
Tracy, Tony and Emma
Background
Emma (15) lives with her mother Tracy and two sisters, Natalie and Sonia. Tony is father to Emma and Natalie and the parents separated a year ago. Emma and Natalie live with mum through the week, with Tony at weekends. Tony is in the Navy and contact with the girls was disjointed until recently.
Parental attachment and caregiving
In relation to her childhood attachment figures, Tracy used on the surface an emotionally independent and self-reliant stance, minimising and dismissing the significance of a range of dangers in her childhood (her mother’s alcoholism, her own physical abuse and being drawn into her parents’ conflict). At times, behind this, her discussion revealed a simmering anger towards her parents, especially in being triangulated into their conflicts. She conveys a strong narrative of feelings that she did not ‘fit in’ and felt invisible in trying to please her parents.
This same combination of attempted self-reliance with underlying resentment and fear of being judged, had strong echoes in her parenting of Emma, the child with an autism diagnosis. Tracy finds parenting to be exhausting and a struggle, often feeling alone with the burden of the two children, angry with Tony for leaving the responsibility to her and experiencing herself as judged and blamed by her parents looking on. Perhaps to ensure her struggles are taken seriously, her overriding tone towards the children is very blaming, for example, stating that the children can be deceptive and manipulative, such that she ends up looking like a bad mother.
Tracy feels the children do not acknowledge her efforts and see how she has tried to be a better mother for them than her own mother. Her theme of ‘not fitting in’ seems central to her corrective scripts which feature being more responsive to her children than her parents were, engaging with things her children are interested in. History is seen to be repeating itself in her parenting with Tony, who she sees as not sharing the responsibility with the children.
However, her anger and disappointment in Emma was more covertly expressed than in regard to Natalie, where her hostility was much more open and direct. Tracy felt her relationship changed dramatically with Emma when she was given the diagnosis:
‘She was very tantrummy, very screamy… As a toddler she wouldn’t listen… (sighs) I found it very difficult to bond with her… I blamed myself then a lot for the fact.’
Now they have an ‘amazing relationship’:
‘[Autism] changed everything! But changed everything for the good! Because there was, there was… suddenly a reason, or an, an… explanation. I’ve always told her she can’t use things like this as an excuse, ‘cause she has to get through life. Um, but just to be able to understand… what’s going on… helps me empathise with her. Which I couldn’t… I had no empathy for her at all before.’
Tracy feels that the autism diagnosis gave her an explanation, presumably lightening the sense of blame she felt, making it possible for her to empathise with her. Notice though the tension between autism as an ‘explanation’ and an ‘excuse’; to rely on the former would appear to remove agency and personal responsibility for her daughter’s actions. This potentially removes the sting of Tracy’s anger at feeling invisible to and rejected by her children. Possibly feeling angry helped her to feel less of a failure and to blame as a mother, for this reason, it remained, albeit ‘below the surface’ in negatively orientated, undermining comments. There was frequently a ‘but’ (or sense of it) that subverted her attempts to be positive about Emma: ‘It’s always, it’s nice when she, when you hear she’s enthusiastic about something. So, that, that’s quite nice. It just goes on and on and on… for a long time.’
Overall, Tony’s interview is mildly pre-occupied with difficulties in his childhood and experiences ongoing frustration. He spoke of being bullied at school, and then learnt to fight; with images of fighting emerging occasionally in his interview. He was frustrated with his mother, whom he experienced as over emotional and absent in terms of providing comfort.
Tony describes his parents as being incompatible in that his mother was emotionally over-reactive and his father under-reactive. A strong theme is that things were hidden away:
‘My Mum and Dad were very good at hiding anything. When they did get into massive fights… you would only really see it if it flared up while we were there. Everything was kept… pretty much away from us… so it was quite hard to understand for us why they were splitting up.’
Early in his interview he notes that this is a similar incompatibility to him and Tracy.
His overall parenting pattern indicates some sense of enjoyment of Emma, and key to this seems to be his perceptions that he and she are alike in sharing aspects of autism:
‘So I think me and Emma of all the family understand… each other… probably better than, than… than anybody else.’
Discussing more difficult moments with the Emma he digresses into a triangulated description of how he gets angry with their mother for the demands she puts on him. Overall, he avoids direct questions regarding feelings and emotions and instead offers descriptions or changes of topic with a similar air of mild complaint (usually about Tracy) we saw in his discussion of his childhood. There was sometimes a slightly self-referential quality, with Tony finding it difficult to talk about Emma in a way that clearly separated her from him. Interestingly, as with Tracy, his discourse about Natalie, his daughter without a diagnosis, came across as more negative and blaming, without the sense of identification that characterised his relationship with Emma.
Family relationships: Trapped by autism that keeps the conflict at bay
There is conflict between Tracy and Tony. She sees him as not taking enough responsibility and he sees her as excessively interfering and trying to make demands. Both share a history of mothers who were seen as over emotional, and for Tracy as dangerous. Likewise, both their parents split up, though Tracy’s got back together. It is interesting that in terms of corrective scripts, neither mentions the disturbing effects that seeing parents’ conflicts can have on children, and in Tracy’s case becoming triangulated – a ‘pawn’ in her mother’s battle with her father. The conflict has already resulted in the pair from separating as partners, but they remain active as co-parents – just.
The narrative of Emma as having autism could usefully be seen as having multiple beneficial aspects for the parents and the family as a whole. It potentially relieves the conflicts with her mother since Tracy now understands it as autism as opposed to the ‘tantrummy and screamy’ baby that Emma had been. For Tony, it also makes his relationship with Emma feel ‘close’ and he feels good at being able to help her. In effect she helps both parents to feel better about themselves (Figure 1). Autism masks the dangerous emotions that threaten family breakdown.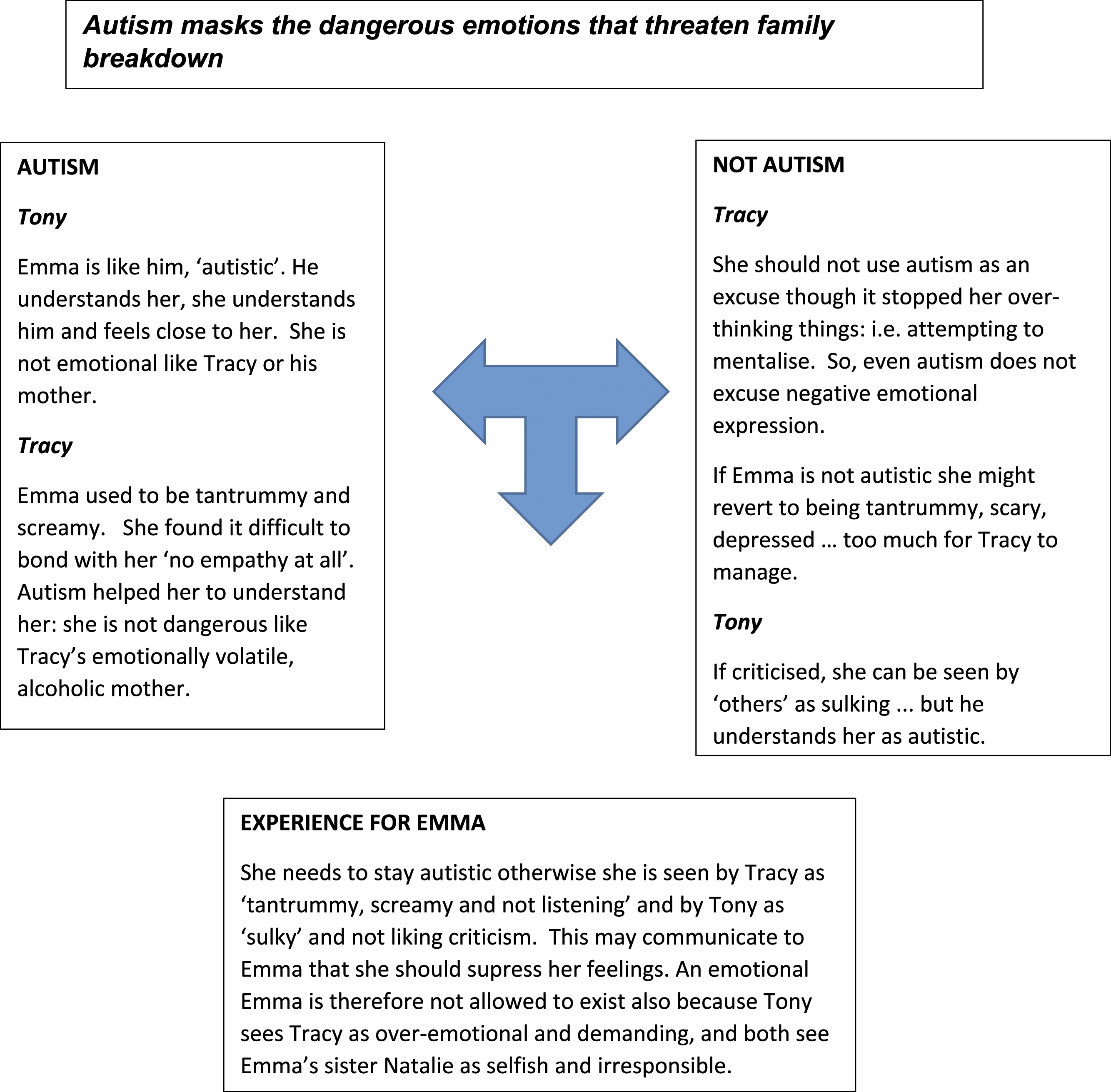
It is quite likely that Emma and the other children have picked up on the conflicts between the parents and Emma’s autism can usefully be seen as functioning to protect the parent’s relationship, allowing them to manage as parents if not partners. Rather than them feeling that they have failed as parents, or that their conflicts have caused problems, Emma’s autism as a neuro-development condition is seen to imply that they are not to blame in any way. Further, since Emma’s dad is also seen as possibly having autism and therefore not so responsible for some of his behaviour, this softens the anger Tracy feels towards him. But the underlying issue is direct emotional expression, and this is not allowed in this family system. For both Tracy and Tony, their relationship with Emma is emotionally distant but less problematic than with the other children. Interestingly both parents were seeking a diagnosis for Natalie, perhaps as a similar way of keeping the conflict in check.
Charles and Daisy
Background
Charles and Daisy parent 3 children, Vickie (aged 11, who has the diagnosis of autism), Walter (9) and Susan (7). They are in regular contact with both sets of parents, who remain together, although the relationship with Charles’ family is more distant.
Parental attachment and caregiving
Daisy: ‘Why can’t you just be normal?’
Daisy felt she had to (and still has to) work hard at her relationships as a child to gain any love or recognition from her parents:
‘I was desperate to please… always. I was desperate to please my family… I never really did… I never did please the family.’
Daisy sees her relationships as a constant struggle, effort that is resented; everything depends on her.
‘I don’t want to be a supporter and a carer I want to be… I would like to be more… sort of… (sighs) not a friend… but… where I don’t feel like I have to kind of prop her up the whole time.’
She is trying very hard to re-create the kind of mother-daughter connection that she never had with her mother (or father) but ends up resenting her child for not playing her role, as she resented her parents for her lack of visibility to them. This failure to recreate what she was hoping for leaves a crushing sense of failure and disappointment: ‘Why can’t you just be normal?!’ She experiences Vickie as difficult and relentless, and her daughter’s ability to hide her difficulties socially adds to the sense of not being seen or believed she carries from childhood:
‘It’s just like… and part of me just goes… ‘There! There it is!’ (laughs) … even now I still think that they think I’m… (pause) I’m making it up. (sighs) Um… my friends don’t believe me.’
Daisy feels she should be positive about her daughter and sympathetic to her disability but experiences frustration with Vickie, for not being the daughter she wanted and resents others for not seeing what she has to manage.
Charles: ‘I can’t fathom out why’
Charles wants to re-create the ‘rational’, conflict-less activity-based childhood that allowed him to manage emotional neglect and the trauma of his father’s stroke, wanting his family to be ‘independent confident individuals, who aren’t overwhelmed by difficult emotions’
Charles’ suppression of his own feelings in childhood means that in his parenting he is tripped up by feelings that he cannot understand or regulate, as they don’t fit his script of being ‘rational’. At such points he tends to opt out, feeling helpless to intervene or control his own feelings:
‘I’m not the right person to deal with it because I'm I just can't I can't fathom out why that's there and it's about knowing … because I just cannot understand her enough and I don't have enough tolerance to tolerate that.’
Because this map of relationships excludes his difficult feelings, he is struggling to own them or see any choice or agency in his responses to the children. The situation getting out of control feels inevitable, and Charles finds himself stuck in a vicious cycle he can’t get out of.
‘I don't have tolerance when I'm angry at something when that gets the better of me and I exhibit that by shouting sort of like forcing people out of the door.’
This spills over into overtly controlling and intrusive behaviour (e.g. ‘frog-march her out the door’) to try and get others to fall in with his sense of what ‘efficient’ relationships would be like, as well as angry outbursts (‘he’s being a shit’) when his children are ‘obstinate’ in thwarting this. Charles’ anger and distress is an elephant in the room throughout the transcript – a shadowy ‘something that gets the better of me’, ‘me, escalating the situation’, but cannot be truly reflected upon, because of the script to put aside unhelpful emotions and behaviour (Figure 2). Family Relationships: Trapped by anger that cannot be named.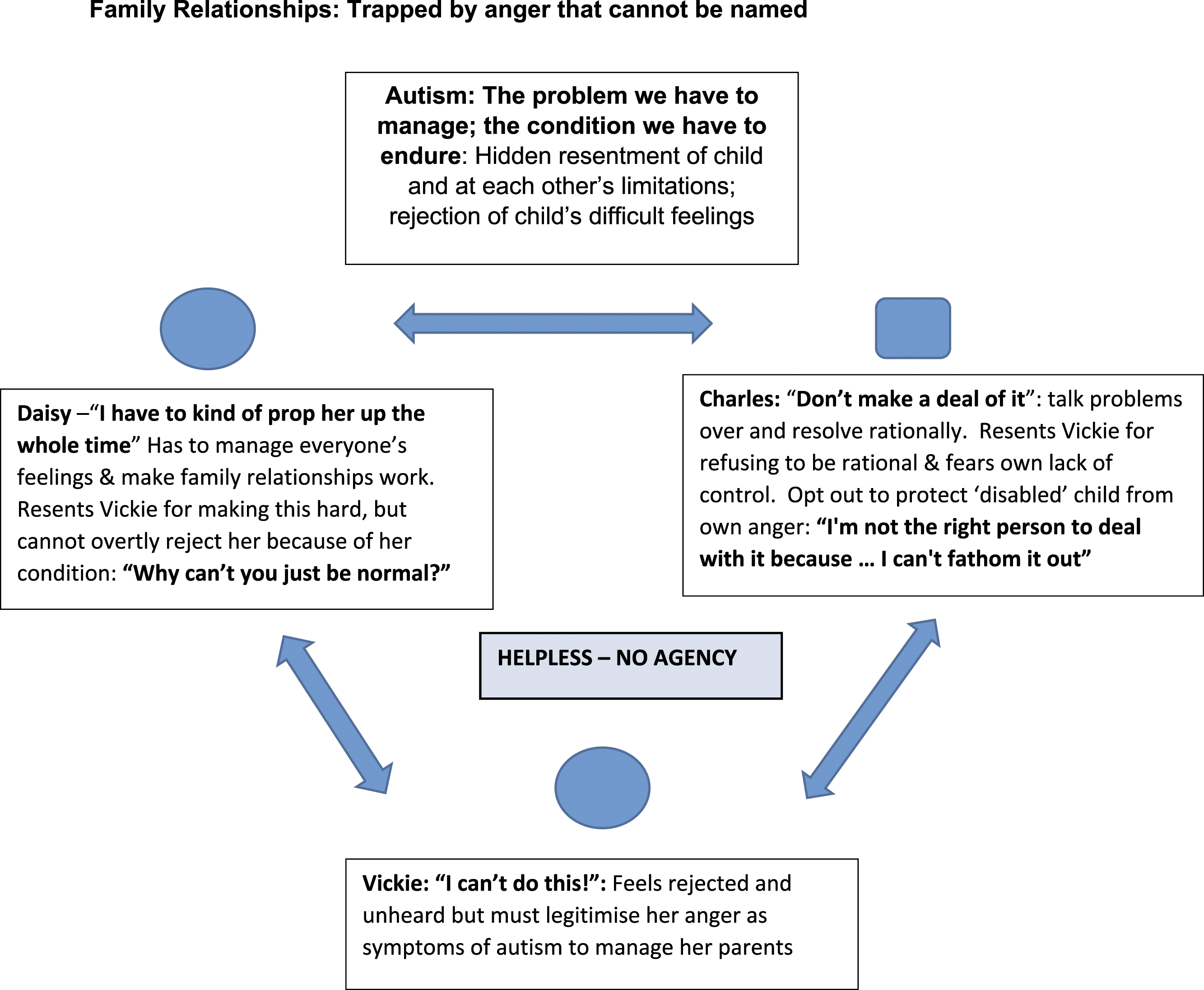
As we have seen, Daisy and Charles each developed an anger management style in their early relationships; one of passive frustration for Daisy and for Charles, repression. Both Charles and Daisy felt unsafe and uncomforted in childhood without a model for dealing with anger and difficult feelings. This seems to coalesce around a common construction about the children’s anger (especially Vickie’s) as the problem that they must manage. The construction that Daisy is the emotional one and Charles the rational one, that appears in both transcripts (especially Charles’), fits with Daisy’s perception that she is the one responsible for everyone, reinforcing her sense of being a mother, but also feeding her simmering frustration at being put upon. Charles feels both aggrieved that his ‘knowledge’ is rejected (by Vickie and Daisy) and guilty that he opts out when his strategy of resolving conflict ‘rationally’ doesn’t work.
Vickie’s diagnosis of autism seems to have an essentialising effect on all the relationships, fixing relational interactions as individual traits. She becomes the one who is deficient, upsetting both parents’ intentions for family life. Paradoxically this also brings Charles and Daisy together as fellow problem solvers, but as mutual sufferers rather than through connection. The discourse of the ‘problem child’ absolves them of blame (though Charles, who feels Daisy’s disappointment, is struggling with this) but contributes to their anger going underground – as you can’t be angry with a disabled child, you have to meet their needs. This renders both of them trapped, and feeling that they have failed, and resenting being a parent.
By the same token, the children are likely to feel their parents’ anger (Vickie who is ‘frog-marched’ and told ‘why can’t you be normal?’, Walter who is a called a ‘little shit’) without having any script available for them as to what it means and how to deal with it. In the case of Vickie, the autism discourse means that her anger cannot be seen for what it is either, as it becomes a symptom of her autism without any interpersonal meaning. She also has to hide her anger under the label of her autism, as a problem to be managed, lest her father opt out or lose control, or she adds to her mother’s resentment and frustration, risking rejection. All three of them are trapped in a cycle of unacknowledged anger and conflict which cannot be seen or addressed interpersonally. ‘Autism’ helps them manage their anger but imprisons them within it.
Bob and Sally
Family context
Bob and Sally are partners, living separately as two families with accommodation nearby. They have two sets of children from previous relationships, with Sally’s child Preston (aged 11), the child with autism, the subject of the interview. At the time of the research interview, Sally was about to give birth to their own child.
Parental attachment and caregiving
When talking about her childhood relationships, Sally predominantly employs an emotionally inhibiting strategy, where she was adopted into a family where the parents fostered a large number of highly challenging, distressed and suicidal children. Despite her parents having little time for her, she describes them as ‘very good parents’. Her narrative veers into a preoccupying anger when she expresses an overwhelming sense of injustice and anger regarding the fostering, but these are disconnected from her parents who chose to foster. Sally told us quite firmly: ‘I’m never going to raise my children the same way I was raised’ but when queried could not articulate what that meant:
‘I don't know, my mother's quite, she's probably a better parent than me, if I'm being honest with you. They're probably better parents than I, fostered 400 kids in 35 years, you've got to be something crazy to do that haven't you? Um, I don't know probably not as perfectionistly clean and tidy, I heard my mom swear for the first time a few months ago in my entire life.’
Sally’s neglect and pain is only hinted at in the words ‘slightly crazy’, and her sense of shame at her different lifestyle from her parents in the suggestion that her mother was ‘perfectionistly clean’. Sally was only able to voice this indirectly through her sister: ‘we bring shame to the rest of them … my sister said you bring shame to us.’
Sally’s sense of resentment and shame about her childhood possibly resonates in her relationship with Preston. Preston is not ‘right’, and the pained, emotive quality of her language suggests that it feels as though he runs her life, and she is reluctantly enslaved. There is a pervading sense that a lot has been taken away from her and now she is having to cope with, and is judged for having, a difficult child:
‘Um Preston he's a very complex character um there's 2 sides to him. You either leave him alone and don't go near him, or he's just in your face talking a load of crap.’
Sally sees Preston as clever, but this almost seems to become mixed in with an irritation at his ‘obsessive’ abilities (which include teaching himself a foreign language) and further holding him responsible for being difficult. In contrast, when he is not irritating, he is distant and not capable of expressing feelings. This suggests a sense of history repeating itself – a childhood of distressed foster children spoiling her life, and now parenting a demanding child who offers her little emotional reward.
Bob’s narratives employed an emotionally inhibiting attachment pattern when talking of his childhood but spoke of his ex-wife in a highly aroused pre-occupied pattern which frames him as her victim. He described that his father drank heavily and was a distant figure. He describes his mother as more ‘cuddly’ but there is scant evidence for such warmth, and it is contradicted by his description of himself as a very anxious person and having been a heavy drinker. Bob’s caregiving narratives indicate a resigned hostility towards Preston; a sense that he is beyond parenting. He views Preston as difficult, as frequently going ‘mental’ and keeps his distance from him.
Bob realises that his own father was strict and frightening: ‘you don’t want to be as strict as him’. This desire to be different from his father may contribute to his rejection and distancing from Preston who elicits in him precisely the anger he experienced in his dad:
‘Sometimes I rant and rave, when I shouldn't rant and rave and sometimes, I need to listen more. Uh, I do struggle with the mixture. Without a doubt, uh, my dad was a strict he ranted and raved when he shouldn't have ranted and raved, and he should have been calm, when I can't, I struggle with the balance.’
To avoid failing to control himself, Bob opts out of engaging fully with Preston so that he does not replicate his own parenting.
Family relationships: Feeling trapped and victimised by their autistic child
Preston’s overall experience may be a consistent sense of rejection by both his mother and Bob. Both Sally and Bob can recognise that Preston has some positive qualities, such as being intelligent, but neither seem to like him very much. Both are united in feeling a victim of Preston, and possibly project some of their resentment onto him. He is given the message that he should like Bob and told to give him kisses. This may represent an emotional bind, fuelling his anger, which in turn confirms their views of him as regularly going ‘mental’.
Since Sally does not recognise and cannot voice the connection between her childhood sense of feeling trapped and being trapped with Preston, there is little possibility at present for providing a relationship for him that helps him to feel emotionally attended to. Preston appears to have some awareness that his mother is not interested in him and therefore tries all the harder:
‘He gets right up in your face, and you want him, you know, you tell him about personal space, especially with people and do, you know, yeah he’s just unique.’
This suggests a pattern which appears to be common in the context of a diagnosis of autism where the child’s attempts at contact are disqualified, regarded as an example of their autistic state (Figure 3). Process of disqualification between parent and child.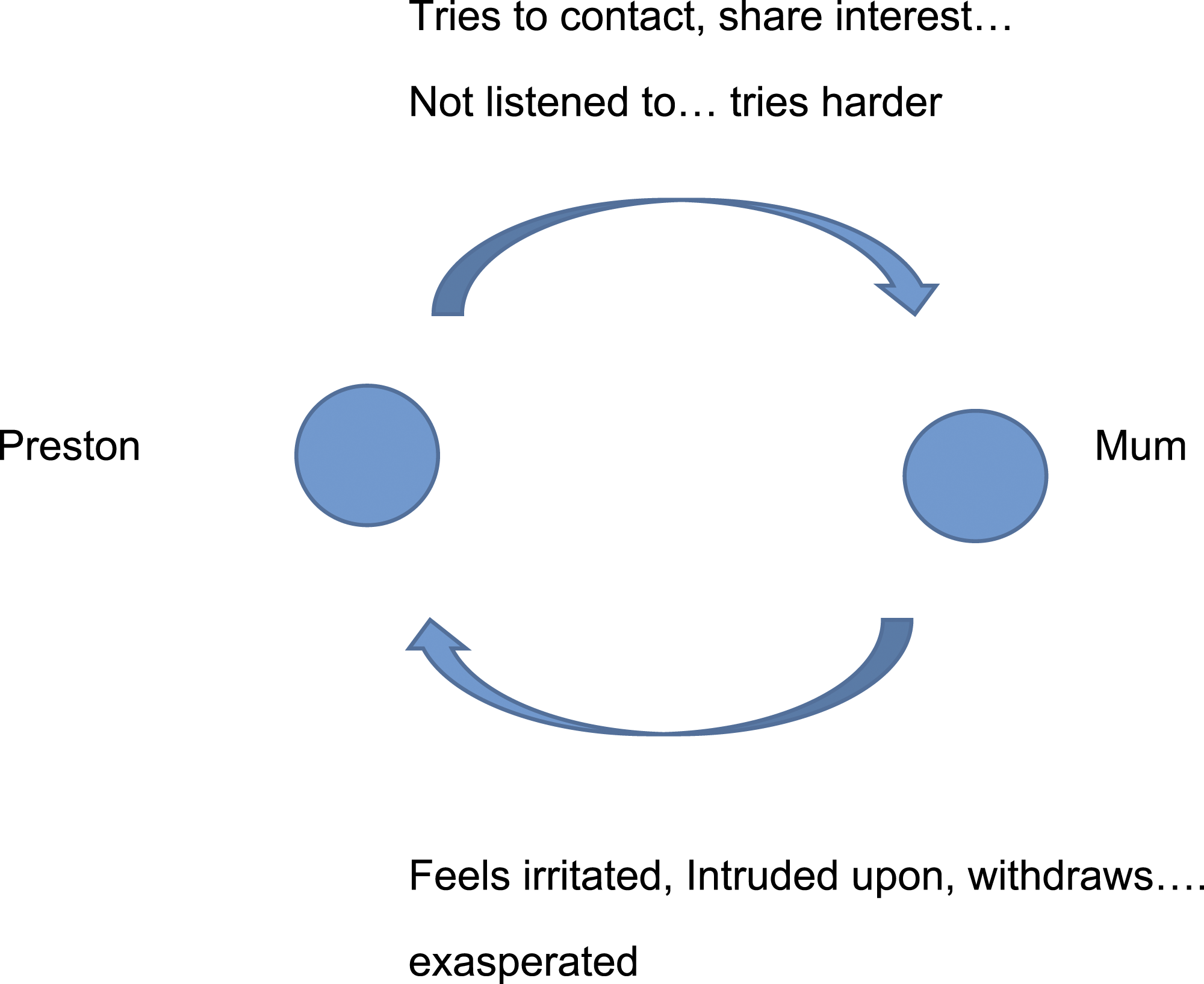
To some extent, both his mother and Bob have some recognition that they could do things a bit better with Preston but cannot see how. Unlike the previous two families, their anger is open and directly expressed, albeit with a sense of resigned futility, especially in Bob’s case. The solution appears to be to regard his anger not as anything to do with their relationship with him, but as a symptom of his autism. Hence there appears to be little alternative for Preston to be seen, and to see himself, as autistic. However, this may, in turn, reduce his capacity for mentalisation and taking responsibility for his actions: ‘Since I am autistic, I go mental’. It also confuses for him what he feels about his mum and Bob. Both Sally and Bob hold a biological/genetic view of autism, but interestingly not to the point that they don’t see him as also responsible for some of his actions. In one sense this is positive, since he does not disappear as a person totally within the autism discourse, but on the other, there is a double discrimination of seeing him as somehow flawed by the autism, which also results in them disengaging from him without helping him manage his feelings (Figure 4). Triadic process involving the child and parents.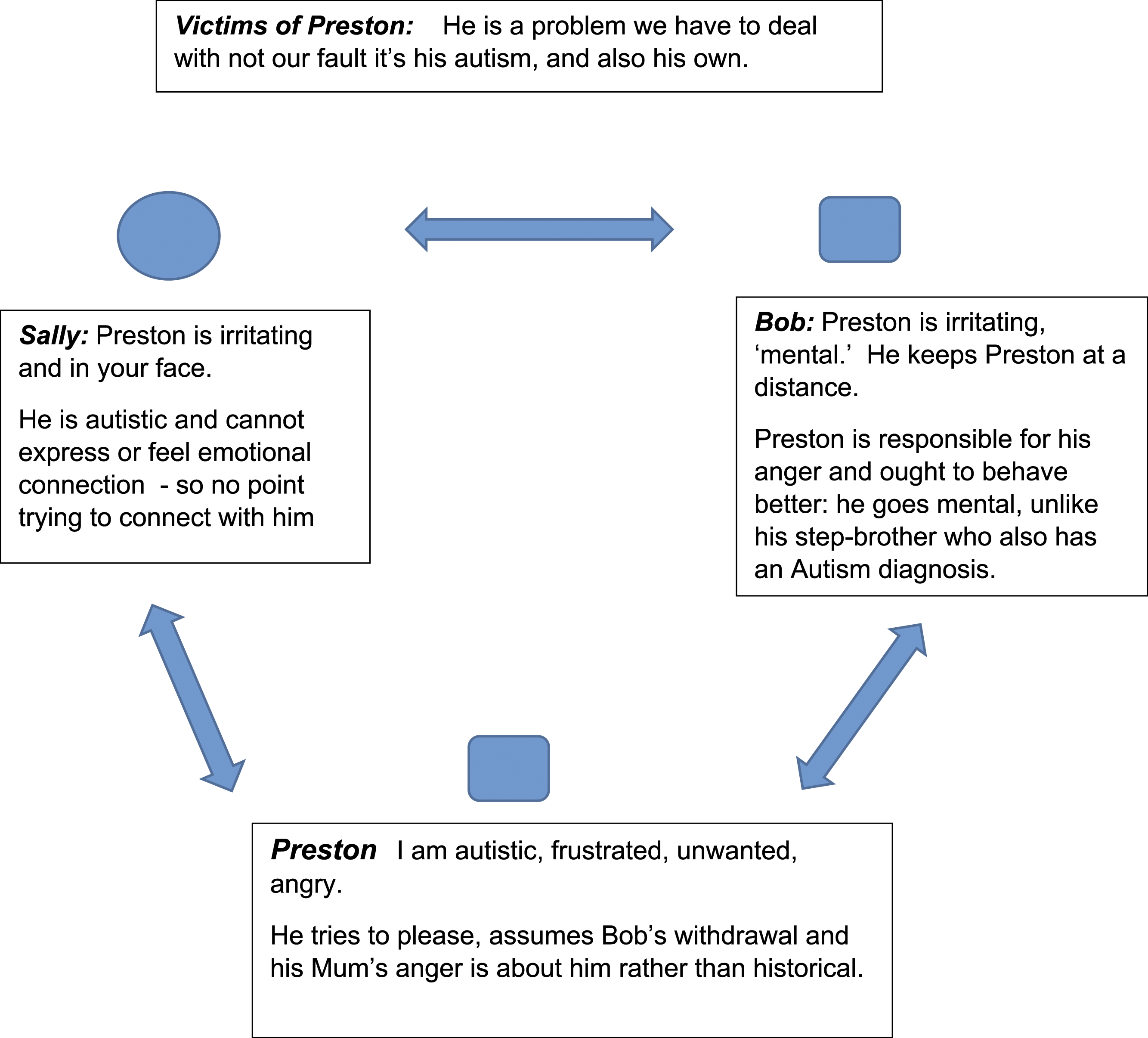
Despite these doubly negative views of Preston, the couple’s openness allows the possibility of seeing him as capable of change, as opposed to an all-embracing autism discourse which frames him exclusively within the diagnosis, as the previous two examples do, driving the conflict underground.
Summary and discussion
All the children in this sample had received an autism diagnosis and this predominantly entails a neuro-developmental explanation that their child has a form of genetically based condition. There is considerable debate whether this is seen as a ‘disability’ as opposed to a ‘difference’ and this can shape parents’ attitudes and orientation towards their child. In this sample the parents predominantly saw their child as presenting considerable challenges and problems for them. This was captured in a sense of the parents feeling ‘trapped’ in trying to manage a child that was not what they had expected. Tony was an exception to this, in seeing his daughter as not so much of a problem because she was like him, in that he felt they shared the experience of autism. Hence, he understood her. However, as we saw in the family system even this had a ‘fixing’ effect, as Emma needed to continue to frame her emotional needs in practical ways to preserve her father’s positive identification with her. Her identified autism reduced the conflict between Emma and her parents and between the parents themselves but rendered her emotional self-invisible. This contrasted with the very hostile way in which both parents viewed her sibling without a diagnosis.
For all the parents, the diagnosis had provided some sense of relief from feeling that they might be responsible and possibly to be blamed for the autism. Sally and Bob found Preston hard work and the diagnosis meant they felt less to blame; nevertheless, Preston was experienced as irritating and more difficult that his stepbrother who also had a diagnosis. Vickie likewise produced a sense of frustration for Charles, in that, despite the autism diagnosis, he could not fathom her out. Daisy wanted her daughter to be ‘normal’. She was also frustrated that Vickie could ‘mask’ her difficult behaviours in front of others, so she felt she made her look bad as a mother. Whilst the diagnosis provided some relief from blame, paradoxically it also created guilt for these parents – they felt required to empathise with their children’s ‘disability’ as it was ‘not their fault’, but still remained angry with them. Viewing their child as ‘different’ as opposed to having a ‘disability’ appeared to present an additional challenge for parents to empathise in that it required even further demands on them to be empathetic. Given that they felt they had not been given adequate advice and skills in how to manage their child and their own feelings this meant they still experienced the relationship with their child as ‘disabling’. It appeared therefore in our sample that the autism as ‘different’ not a ‘disability’ discourse was something that parents were outwardly and verbally attempting to employ, which masked their underlying experience of frustration, anger and helplessness.
This placed the family in a bind which was frequently expressed by a debate as to whether the children were responsible for their actions or whether instead the problems were caused by their ‘disability’. To see their children as people with agency threatened to undermine the relief from blame and conflict that the diagnosis gave them, however the mechanical explanations of behaviour that they associated with their children’s autism diagnosis seemed to rob them of any ability to effect any change as parents; essentially all they could do was manage their child rather than relate to them as a parent would. This kind of double bind has been found in systemic explanations of other diagnoses (e.g. eating disorders, Dallos, 2004; Ringer and Crittenden, 2007). Echoing this research, for all our participants, ‘autism’ represented the anger and conflict within the family that could not be voiced. Importantly, this was not just conflict with the child or between the parents, but also the anger that the parents had but could not express from their own childhood history. None of the parents appeared to have experienced secure attachment relationships with their own parents and their more negative emotional experiences may be related to a sense of loss and disappointment that they had not been able to create a different and more positive relationship with their child than had been their own experience of parenting. Strikingly, when it came to specifying what those differences were, they tended to be very muted and tended to cut off, change the subject or identify safer subjects rather than articulate what was actually negative about their experience of growing up. Voicing anger that they carried from childhood risked re-activating feelings of rejection for expressing anger in their own childhoods and similarly a felt risk of cutting themselves off from support. Overall, a risk of potentially being overwhelmed by feelings that they had learned to suppress to manage in the world.
Focussing on their child’s neurodevelopmental differences gave their sense of frustration a safe, impersonal explanation which sidestepped this, but also added to their sense of helplessness by fixing the problem in something that cannot be altered. Unlike with many other diagnoses, parents of autistic children are frequently not given much they can actually do to make things any better, which contributed to the near universal sense of being trapped with a child they did not experience as rewarding (Grey at al. 2021; Slade 2009). As one study participant put it, “You just feel hemmed in, like you’re in a, sometimes you feel like you’re on a ship, a prison ship or something, trapped with them and you can’t get away”. (Bowlby, 1988, p.3) talks of the intensity of feeling that accompanies attachment relationships: “If [the relationship] goes well, there is joy and a sense of security. If it is threatened, there is jealousy, anxiety, and anger. If broken, there is grief and depression.” Our participants were showing all the extreme feelings of threatened or broken relationships both with their child and childhood relationships but lacked a discourse with which this could be articulated. More broadly it is possible that the childhood traumas and losses prevalent for the parents made it harder for them to mentalise about their child. Hence the appeal of a diagnostic discourse is broader than just autism. At the same time, it is possible that the appeal of the ‘autism’ discourse’ is all the more pervasive for these families since the possibility of change is more proscribed within the framework of autism as predominantly a neuro-biologically based condition.
Our findings need to be taken in the wider context of the lives of the families we have described. There is a risk that as researchers we can reinforce a sense of failure and helplessness in our descriptions of these families that they feel about themselves. We have suggested (McKenzie et al., 2021) that there are major shortcomings in services for these families. Often, they wait several years for a diagnosis in the expectation that this will provide assistance for them, help their child to develop and improve their relationships as a family. Family therapy is rarely available for the families, not least since the diagnosis of autism as a neuro-developmental condition obscures the attachment needs of the family members.
However, in family therapy oriented clinical work with the families a more hopeful picture emerges. The first author worked clinically with Tony and Tracy and their daughters. As we have described, Tracy showed anger towards Emma’s younger sister and saw her as difficult and wilful. In contrast, Emma was less of a problem in that she did not display anger so much and appeared eager to try and placate and please her mother. However, over the course of sessions with the family, it was also possible to see softer and warmer emotions regarding their relationships. Tracy had described that as a child, she had been witness at age 14 to her mother finding out that her father was having an affair. She described that subsequently after their separation she felt used as ‘pawn’ in the battle between her mother and her father. In one session we explored using a button-sculpt how of her daughters regarded their relationships before, during and after her own separation from Tony. Tracy become overwhelmed when her daughters indicated that they actually felt closer to her after the separation, whereas she had always thought that she had emotionally damaged the girls, as her own mother had her. Tracy also described how her own parents’ affection has been conditional on her doing what they wanted whereas she was able to explain that, for example she shared a non-conditional mutual love of music and art with her daughters.
All of the parents expressed ‘corrective scripts’ concerning what they wanted to do better for their children, but many also felt sad, frustrated and angry that they could not achieve their hopes. These frustrations in turn seemed to exacerbate the negative interactions with their children. Giving an opportunity for parents to express their hopes appeared to be helpful in validating them and frequently triggered a softening of their more negative feelings towards their child with autism and also the other siblings. The frustrations were generally evident towards the other children as well, but the autism diagnosis could serve to help the parents feel less blamed. Moving to a focus on their benevolent intentions frequently led to less of a focus on the child as having a diagnosis of autism, and more on their unique qualities and actual thoughts and feelings. Similarly bringing the parent’s painful experience into the room, including present echoes of past trauma, as part of the reality experienced by the whole family, can help its influence on family relationships be owned and considered by all, rather than submerged in autism and disability discourses. Our case studies suggest that the mechanising discourse of autism especially, can rob the parents of the experience of being a parent and influencing their child, and deprive the child’s behaviour of any interpersonal meaning. Restoring both can feel dangerous and risky for all but has healing potential.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.