
Abstract
Introduction
Challenges associated with COVID-19 are not only associated with its acute phase but also with its sequelae. Multiple studies have been conducted on long-term follow ups of patients suffering from COVID-19. In a detailed search of the literature, we did not find any long-term follow up study in the Indian population.
Methodology
The present study is an ambi-directional observational follow up study. A total of 83 patients were included in the study and a follow up was conducted at 2, 6 and 12 weeks after recovery from acute phase of moderate to severe COVID-19. The primary objective was to identify symptoms pertaining to respiratory, cardiac, neurological and mental health in post-COVID period. Secondary objectives were to identify patients consistent with a diagnosis of post-COVID syndrome and to assess the difference in the recovery profile between moderate and severe cases.
Results
Significant improvement was observed in fatigue, cough, SpO2, breath-holding time and EuroQL-5D with maximum improvement by 12 weeks of recovery. Patients having longer ICU stays and requiring non-invasive ventilation had a longer persistence of symptoms. Forty-five patients had symptoms persistent even after 12 weeks consistent with a diagnosis of post-COVID syndrome.
Conclusion
We observed 50% of the patients in the cohort had complete resolution of symptoms by six weeks follow up. Therefore, a follow up period of at least six weeks is warranted for all patients suffering from moderate to severe COVID-19, along with continuous screening of patients who tend to develop post-COVID-19 syndrome.
Introduction
The COVID-19 pandemic brought emergent challenges to the world. During this long course of the pandemic, we witnessed multiple presenting features of the disease. Apart from dealing with the acute disease process, medical centers throughout the world are reporting an increasing number of hospital visits by patients experiencing post-COVID complications. Therefore, the challenges associated with COVID-19 extended to the management of the squeal of COVID-19 as well.
The first study published by Indian authors recommending long-term follow up of COVID-19 was by Balachander et al. 1 The first long-term follow up of six months was carried out in Wuhan, China from January to May 2020. 2 Further a number of studies conducted in different nations reported similar results.3–5 Apart from these comprehensive studies, there are a number of individual studies assessing pulmonary, cardiac, neurological and psychiatric symptoms.6–8
After a detailed search of the literature, we did not find any comprehensive long-term follow up study on the Indian population during the second wave of COVID-19. Therefore, with the present knowledge of the available literature, we planned to conduct a follow up study on COVID-19 survivors of moderate to severe disease for a duration of up to 12 weeks.
Methodology
The present study was an ambi-directional observational follow up study. The study was carried out in two centrally located hospitals in north, India. The study was conducted between April 2021 to January 2022.
All patients with diagnosis of moderate to severe COVID-19, where moderate and severe COVID-19 were defined as per MOHFW India. Moderate COVID-19-adults with presence of clinical features of dyspnea and or hypoxia, fever, cough, including SpO2 90 to ≤93% on room air, Respiratory Rate more or equal to 24 per minute. Severe COVID-19- adults with clinical signs of pneumonia plus one of the following; respiratory rate >30 breaths/min, severe respiratory distress, SpO2 <90% on room air.
During the second wave of COVID-19 in India, patients aged between 18 to 80 years and discharged from the hospital based on the following criteria: Maintaining oxygen saturation >90% on room air, no fever for three days, no breathlessness on rest and respiratory rate of <30 breaths per minute were included in the study. Patients not meeting inclusion criteria, discharge criteria and not giving consent were excluded from the study.
The record of patients was retrieved from the records of the two hospitals. For retrospective data, a record of all patients discharged two weeks prior to the study approval was retrieved. Prospective data was collected up to two months after study approval. The follow up was conducted at 2 weeks, 6 weeks and 12 weeks after discharge from hospital. The digital informed consent in the form of a Google form was sent to all the participant through WhatsApp or Email. At first follow up this digital informed consent was obtained from all participants. The telephonic follow up was conducted by a trained physician through a video conferencing with the patients the approximate duration of each follow up interview was 45 minutes; as with the ongoing COVID-19 pandemic calling for hospital visit was not possible.
The primary objective of the study was to identify symptoms pertaining to respiratory, cardiac, neurological and mental health in post-COVID period at various time points of follow up.9–11 Secondary objectives were to Identify patients consistent with diagnosis of post-COVID syndrome (Includes symptoms and abnormalities persisting or present at or beyond 12 weeks of acute COVID) 12 and to assess difference in the recovery profile between moderate and severe cases.
The demographic data, chief complaints at presentation, presence of comorbidities, previous COVID infection, treatment received in hospital, duration of stay in hospital and ICU stay, history of non-invasive ventilation (NIV)/high-frequency nasal oxygen (HFNO)/Invasive mechanical ventilation were recorded at first follow up. At first and subsequent follow ups other parameters which were recorded include any escalation of comorbid illness, symptoms like fatigue/tiredness, joint pain/back pain, persisting fever, anorexia, loss of taste and loss of smell. Pulmonary symptoms including dyspnea and cough were recorded. Dyspnea was assessed by mMRC scale defined as: 0 - “I only get breathless with strenuous exercise”; 1 - “I get short of breath when hurrying on the level or walking up a slight hill”; 2 - “I walk slower than people of the same age on the level because of breathlessness or have to stop for breath when walking at my own pace on the level”; 3 - “I stop for breath after walking about 100 yards or after a few minutes on the level”; 4 - “I am too breathless to leave the house” or “I am breathless when dressing.” 13 Cough was assessed based on the cough severity index. Rating from 0 to 4: 0 - never, 1 - almost never, 2 - sometimes, 3 - almost always, 4 - always. Breath-holding time 14 and pulse oximetry readings were also recorded. For breath holding time, patients were asked to hold their breath after a normal breath and then time was noted in seconds, the test was done three times and the average value was noted. Oxygen saturation was noted with the standard portable pulse oximetry device. Cardiac symptoms were recorded as chest pain which was defined as severe discomfort in chest including a dull crushing or a sharp stabbing or burning feeling or pain that radiates to the neck or shoulder. Palpitations and any aggravation of hypertension were also recorded. In neurological symptoms of limb weakness, seizures, vertigo or headache were recorded. Vertigo was graded as mild vertigo: Occasionally for a brief time and goes away on its own. Nausea, but no vomiting, may be present. Moderate vertigo-requires patient to lie down and lie still and severe vertigo—occurs when a feeling of movement is continuous even when lying. Headache was recoded as number of episodes and their severity. Severity was assessed as mild: able to carry out daily activities, moderate: difficulty in carrying out daily activities and severe: cannot carry out daily activities. Assessment of quality of life was done based on EQL-5D-5LScale 15 . Each of the parameters is graded from one to five and total score out of 25 was recorded. Quality of life score was recorded as patients were asked about how much good they feel about their health today and the grading was done from one to 100.
Results
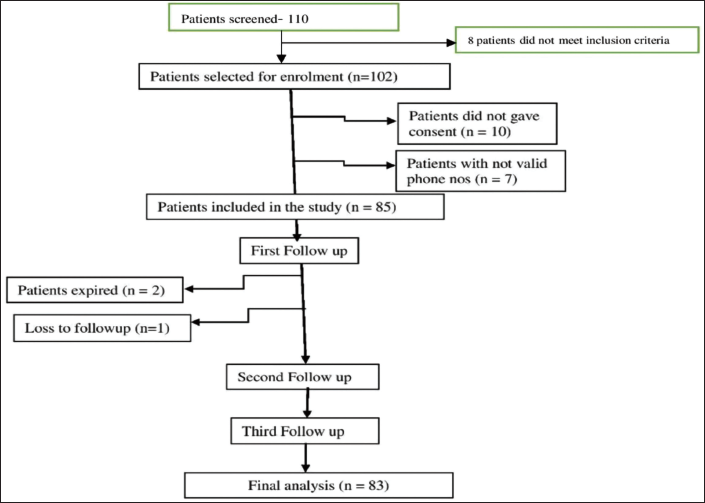
A total of 110 patients were screened consecutively; 102 patients were enrolled as they satisfied the inclusion criteria. Ten patients did not give consent, seven patients did not have a valid contact number, therefore a total of 85 patients were finally included in the study. Twenty-one patients were from one centre and 64 patients were from the other were included, one patient was lost to follow up at first follow up, and two patients had expired at the first contact. Eighty-three patients were included in final analysis. Consort Diagram showing the patient enrollment and follow up is shown in Figure 1.
Consort Diagram Showing the Patient Enrollment and Follow-up.
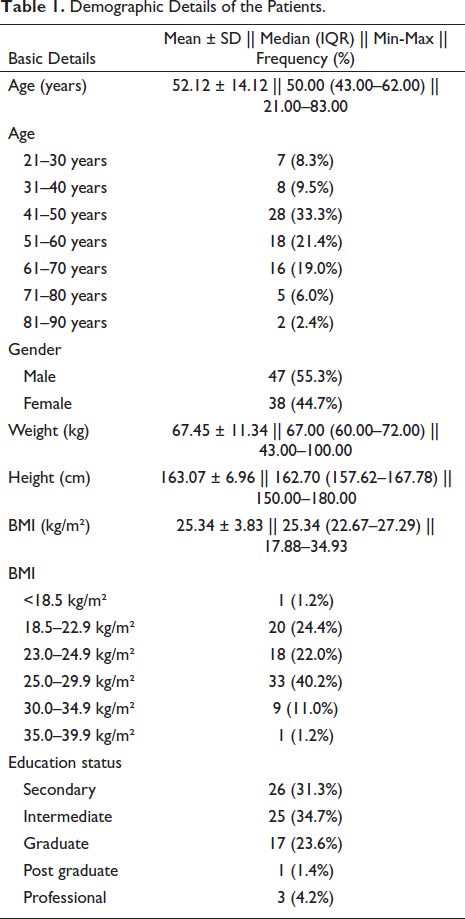
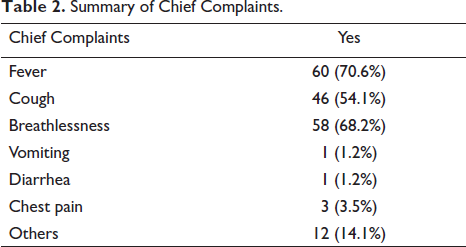
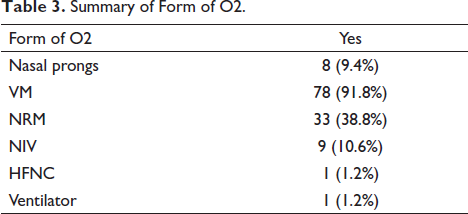
The demographic data of all the patients was recorded as shown in Table 1. The chief complaints presented by the patients are as detailed in Table 2. All of the patients included in our study were suffering from moderate to severe COVID-19 with requirement of the oxygen therapy. The form of oxygen required by the patients is shown in Table 3. A total of 76 patients received steroids in treatment and a total of 78 patients received antifibrinolytics.
Demographic Details of the Patients.
Summary of Chief Complaints.
Summary of Form of O2.
The average duration of hospital stay was 15.36 ± 10.65 days with an ICU stay of 1.5 ± 3.40 days. A total of 54 (63.5%) patients had known comorbidities with 44.7% having diabetes mellitus followed by hypertension in 21.2%, CAD in 7.1%, thyroid disease in 3.5% and bronchial asthma in 2.4%.
Out of the total patients, 33 (39.8%) patients had an escalation of comorbidities at the follow up, maximum escalation being observed in patients with pre-existing diabetes 26 (31.3%) followed by hypertension five (6%) and other comorbidities in five (6%) patients. During the second follow up nine (11%) patients still reported the escalation of their comorbid conditions out of which six (7.3%) patients were diabetic and one (1.2%) patient being hypertensive and two (2.4%) being other comorbidities. During the third follow up nine (11%) patients were still suffering from escalation of comorbidities with seven patients suffering from diabetes and two patients with other comorbid conditions.
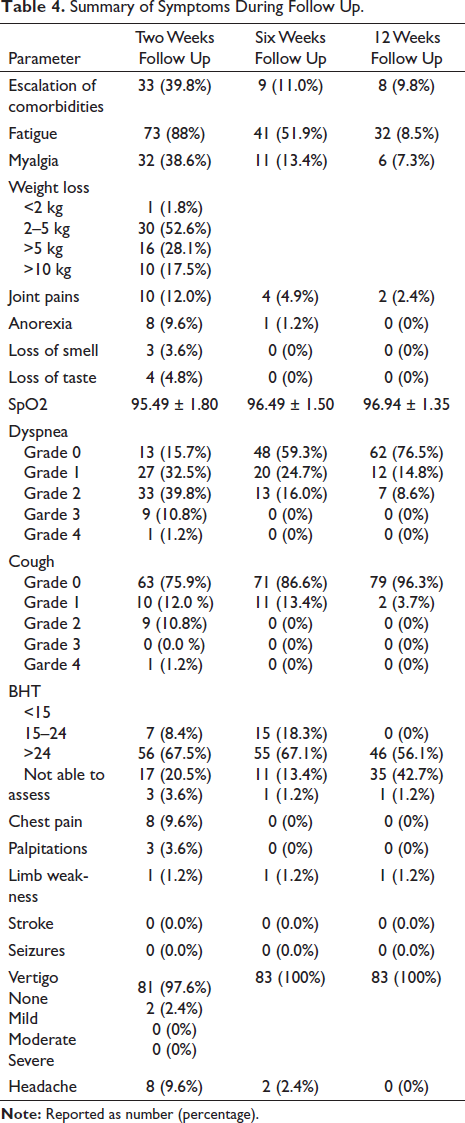
The patients were followed up for symptoms of fatigue, joint pains, myalgias, fever, anorexia, loss of taste, loss of smell, dyspnea, cough, breath-holding time, Spo2, chest pain, palpitations, headache, stroke, limb weakness, vertigo, seizure as described in Table 4.
Summary of Symptoms During Follow Up.
The change in fatigue over time was found to be significant when first follow up was compared to second and third follow up. McNemar’s test was used to assess the change in fatigue between the two timepoints. A significant number of patients moved from yes to no category (p < .001 for both comparisons). The change for myalgia over time was also found to be statistically significant (p < .001). Twenty-five patients moved to category no from yes at second follow up and 29 patients moved from category yes to no at third follow up. The change in anorexia over timepoints was also significant eight (9.8%) patients moved from the category yes to no. (p = .020) at second follow up. Eight (9.8%) patients moved from the category yes to no. (p = .005) at third follow up.
The severity of cough changed over time significantly. At first follow up 20 patients reported cough, with one patient reporting severe degree grade 4 cough. At second follow up two patients reported to have new onset of cough of grade 1 severity. Sixteen patients reported reduction in severity of cough to up to grade 0 (11 patients) and grade 1 (four patients). At third follow up only three out of the four patients reported grade 1 cough, rest of the patients were free of this symptom. This change was significant with p = .03 between first and second follow up and p = .006 between first and third follow up.
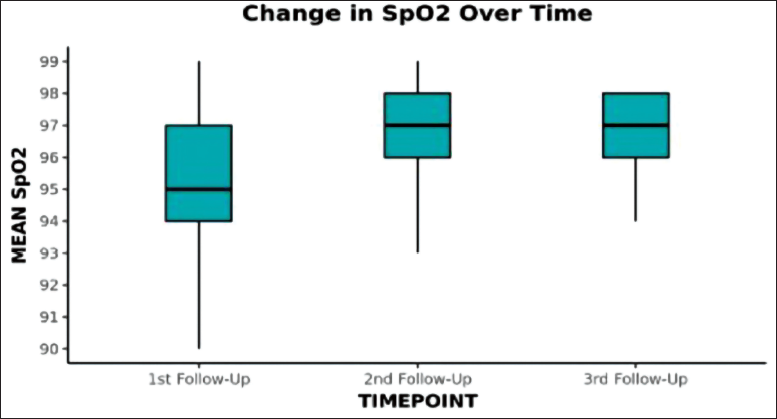
The mean Spo2 observed during the three follow ups were 95.49 ± 1.8, 96.49 ± 1.5, 96.4 ± 1.35, respectively. The change was significant over time (p < .001). On post-hoc pairwise analysis the maximum change in Spo2 was observed from first follow up to third follow up (p < .01). Change in SpO2 values over different time points during follow up is demonstrated in Figure 2. The change in BHT was statistically significant only for comparison between first and third follow up. Three (3.7%) patients moved from the category BHT: <15 seconds to the category 15–24 seconds. Four (4.9%) patients moved from the category BHT: <15 seconds to the category >25 seconds. Fourteen (17.1%) patients moved from the category BHT: 15–24 seconds to the category >25 seconds. Two (2.4%) patients moved from the category BHT: No Able to Assess to the category 15–24 seconds. The overall change in BHT was statistically significant (Stuart-Maxwell test: χ2 = 21.473, p = <.001) between first and third follow up.
Change in SpO2 Values Over Different Time Points During Follow-up.
Psychiatric illness was reported only in one patient (1.2%) at first follow up. Daily work restriction was reported by five (6%) patients at first follow up, two (2.5%) patients at second follow up and two (2.4%) patients at third follow up. The ED 95 score and quality of life index were recorded at different follow ups and are demonstrated in Table 5.
The Quality of Life and ED 95 Score at Follow Up.

Parameters like stroke, limb weakness, seizure, vertigo, headache were not significant over time. Respiratory support (BIPAP) was required by one patient in first follow up, while in second follow up one patient had recurrent pneumonia and one patient continued to require respiratory support during till third follow up. One patient reported to have undergone Percutaneous Coronary Intervention (PCI). One patient had limb weakness during the first follow up which persisted till the third follow up. There were other complaints which were reported by patients like mucor mycosis reported in five (6%) patients at first follow up, four (4.9%) in second follow up, four (4.9%) at third follow up. Skin-related complaints in three (3.6%) patients at first follow up, three (3.6%) patients at second follow up and eight (9.8%) patients at third follow up. Mobility, usual activity, anxiety/depression and quality of life improved significantly from first to the third follow up.
Forty-five patients had symptoms present even at follow up of 12 weeks consistent with diagnosis of post-COVID syndrome. Thirty-two patients still reported fatigue, 19 patients reported dyspnea, three patients had persistent cough, 12 patients reported depression and anxiety. Despite these complaints patient had other complaints explained by COVID-19 disease pathology or aggravated by COVID-19 which were recurrent pneumonia in one patient, eight patients had skin related complaints, one patient had myocardial infarction requiring PCI, one had left-sided weakness, one patient required respiratory support and three patients had mucor mycosis with complications requiring multiple surgeries.
Correlation of severity of illness with other parameters was also done. The patients having severe form of COVID requiring ICU stay and O2 in form of NRM, NIV, HFNC or Invasive Ventilation had more symptoms up to third follow up. The correlation between severity of illness and four variables, that is, dyspnea, anxiety/depression, quality of life index, cough, myalgia and ED 95 score was statistically significant. Therefore, a patient who suffered from severe COVID had complained of dyspnea and reduced quality of life even at 12 weeks. Therefore, the severe category patients warranted a more rigorous follow up.
Discussion
The present study inherits its novelty from being the first time-based long-duration follow up study of moderate to severe cases of COVID-19; based on an Indian population. The study mainly focuses on recovery profile following acute phase of moderate to severe COVID-19 diseases, and indicates that a majority of patients recover between two and six weeks. Although, a significant proportion also suffer from post-COVID-19 syndromes.
The most common symptoms were fatigue, dyspnea, cough and weight loss, while a few also reported anxiety, depression and headache. Fatigue has been reported to be one of the commonest symptoms during recovery from COVID-19. In the present study, fatigue was reported by 88% patients at two weeks follow up with reduction of up to 8.5% at 12 week follow up. The maximum reduction in reporting of fatigue was found between second and third follow up. A similar prevalence is reported in a systemic review and meta-analysis on long-term effects of COVID-19 with fatigue being present in 58%. 16 Myalgias was the next commonly reported symptom in 38% patients with reduction of up to 7.3% at 12-week follow up. A study by Huang et al. also reported fatigue and myalgias to be the most common symptom at follow up of six months reported in 63% patients. 2 A similar study reported a point prevalence of fatigue in 73% patients. 17 The present study reports a greater incidence of fatigue this can be explained by the fact that only patients with moderate to severe disease were enrolled and the time point of follow up was different in other studies.
Dyspnea was another common symptom reported by patients. At two weeks follow up 84.7% patients had complaints of dyspnea, while it reduced to be present in 23% of patients at 12 week follow up. Improvement in respiratory functions was assessed by breath-holding time and SpO2 values. Both the parameters improved significantly over time and maximum change being observed between first and third follow up which coincides with the clinical improvement in respiratory symptoms. An observational study conducted on cardiopulmonary recovery after COVID-19 indicated that dyspnea was the most frequent pulmonary symptom (36%) at 60 days of follow up. 18 Huang et al. reported that at six months post-COVID the prevalence of dyspnea was 36%–26% in patients suffering from severe to moderate COVID. 2 We report a similar incidence in the present study. These studies have employed the use of mMRC score for grading dyspnea as in the present study. Cough was reported in 24% patients at two weeks follow up and 3.7% at 12 weeks follow up. Literature reported incidence of cough to be 1.8% at three months in patients suffering from moderate to severe COVID. 6
Multiple studies have assessed impact of COVID-19 on mental health and have reported depression and anxiety as the most common symptom. In the present study 36% at two weeks follow up and 14.5% of the patients at 12 weeks follow up reported a score of less than five for depression and anxiety in ED 95 scale. A review article reports incidence of anxiety (6.3%–51%) and depression from 14.6% to 48.3%. The present study also reported depression and anxiety to be most common symptom. 19 Quality of life index was observed in the present study and was found out to be 75.41 at two weeks follow up and increased to 94.2 at 12 weeks follow up. Although the reported quality of life by Huang et al. is 80 (75–90) at six months of follow up. As quality of life is a subjective parameter and the difference can be attributed to the difference in demographic profile of the enrolled cohort. 2
Of the study cohort, 63.5% patients had known comorbid conditions. At two weeks following acute COVID, 61% patients with the known comorbid conditions had aggravation of the comorbidities with maximum aggravation being observed in patients with diabetes. Most of the study population was suffering from moderate to severe COVID-19 and hence required steroid treatment which further led to more deranged blood sugar levels. A significant finding in our study was that even after acute phase of illness and tapering of steroids patients had deranged blood sugar levels. Therefore, the aggravation in diabetes cannot be only iatrogenic but is also pathophysiological.20, 21
Skin-related complaints were observed in 9.6% patients, the most commonly reported symptom was hair fall, followed by itching and skin rashes. This incidence is similar to that reported at six months follow up, with 20% having hair loss and 3% reporting skin rash. 12
We report 54.2% of the study population as having post-COVID syndrome. The incidence of post-COVID syndrome has been reported from 10% to 35% with incidence reaching up to 85% in hospitalized patients. 20 The most common symptoms in patients with post-COVID syndrome were fatigue (38.5%) and dyspnea (23%) and depression/anxiety (14.4%). Similar incidence has been reported in multiple studies with fatigue being the commonest symptom.11, 17 Other reported symptoms were cough and skin-related complaints. A significant number of patients who were both diabetic and non-diabetic, were further affected with mucormycosis. Mucormycosis in these patients was multifactorial and largely attributed to diabetes, immunosuppression, unwarranted steroids usage and perhaps COVID-19 disease pathology. 22 Mucormycosis can be considered as a post-COVID sequelae which increased the healthcare burden manifolds especially in the Indian population.
Limitations
Our study results should be read in light of certain limitations of our study these include, the present study is an observational cohort study, the present study is limited by its small sample size, we were unable to do an objective assessment of cardiac and respiratory function as the data collection was a telephonic interview based due to limitation of the communicability of the COVID-19 itself.
Conclusion
We observed 50% of the patients of the cohort had complete resolution of symptoms by six weeks follow up. Therefore, a follow up period of at least six weeks is warranted for all patients suffering from moderate to severe COVID-19, along with continuous screening of patients who tend to develop post-COVID syndrome. Although mass vaccination has reduced the severity of disease, a number of new strains, are still causing severe disease. An effective follow up will help in early detection and treatment of COVID-19 complications.
Author contribution
D.G: Formulation of study plan, protocol writing, enrollment of participants, conduction of follow-up and manuscript writing. D.D: Formulation of study plan, protocol writing, enrollment of participants, conduction of follow-up and manuscript writing. J.G: Enrollment of participants and conduction of follow-up and manuscript writing. S.P: Formulation of plan and manuscript editing and writing. S.V: Enrollment and follow-up of participants.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the institutional ethics committee-wide letter no: GMCH/IEC650R/2022/19.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
Informed consent was obtained from all patients before enrollment into the study.