
Abstract
Literature is lacking on the spectrum of symptoms of long COVID-19 (defined as symptoms persisting beyond 28 days of diagnosis) and its impact on quality of life. This single-center, cross-sectional study included mild COVID-19 cases as determined by a positive real-time reverse transcription polymerase chain reaction test. Patients were contacted at least 28 days after diagnosis and were interviewed telephonically using semi-structured questionnaires for duration of symptoms, fatigue using Fatigue Severity Scale (FSS) and quality of life using the World Health Organization Quality of Life: Brief Version (WHOQOL-BREF). A total of 251 COVID-19 patients were included; of which 169 (67.3%) were males. The mean age of the patients was 35.8 years (SD = 12.5). The prevalence of long COVID-19 was 28.2% (n = 71, 95% CI: 23.0–34.2). The most common symptoms involved the musculoskeletal system (12.7%), upper respiratory tract (7.6%), and fatigue among 17 (6.8%) patients. Patients with long COVID-19 had significantly higher FSS score and lower WHOQOL-BREF score compared to the patients without long COVID-19 (<28 days).
Introduction
COVID-19, caused by SARS-CoV-2 was declared a pandemic on March, 11 2020, by the World Health Organization (1). Clinical course of the disease varies from asymptomatic carriage to severe respiratory distress, multiple organ dysfunction, and death (2). Most available literature has focused on patients that required hospitalization (3). The median time for clinical recovery is approximately 2 weeks for mild cases (4). Such cases remain infectious for less than 10 days after symptom onset and guidelines from different countries recommend isolation ranging from 10 to 17 days following which usual duties can be resumed (5,6). This period of isolation does not necessarily correlate with full clinical recovery as recent studies have shown that a significant number of patients have symptoms lasting beyond the acute illness (7–9). Most of the literature, in India and worldwide also, has been reported in hospitalized patients. With a case fatality rate of around 1.3%, the severity of COVID-19 has been mild in majority of the patients who did not require hospitalization and were managed at home (10). Hence, there may be under reporting of post-COVID-19 sequelae in these group of patients.. Long COVID-19 is a recognized entity now and has been described as symptoms that linger on after 4 weeks of acute disease (11). While these symptoms may not be severe enough to warrant hospitalization, the associated morbidity can cause fatigue, affect the quality of life, and requires redressal. As we have battled various waves of the pandemic, patients with ongoing symptoms after recovery from COVID-19 are increasingly recognized as a growing population in need of attention. Globally, survivors of COVID-19 are reported to have sequelae related to various systems including respiratory, neurological, neuropsychiatric, cardiovascular systems, etc (10). Post-COVID-19 condition has also been given a separate International Classification of Diseases (ICD) section and that itself highlights the need to address and increase our awareness regarding the same (12). Recent studies have highlighted the impact of the pandemic not only on physical health, but also on the mental well-being and health-related quality of the population (13,14). We thereby conducted this study to estimate the prevalence of long COVID-19 and its effect on the quality of life among mild COVID-19 patients.
Methods
Study Design and Patients
This single-center, cross-sectional study was conducted at the All India Institute of Medical Sciences (AIIMS), New Delhi, a tertiary care hospital in northern India. We included patients who were ≥ 18 years of age, presented to our dedicated COVID-19 clinic with mild disease, and tested positive for COVID-19 with a real-time reverse transcriptase polymerase chain reaction test between May, 1 2020 and July, 31 2020. Patients who were advised home isolation were contacted telephonically after minimum 28 days of diagnosis. We excluded patients who were asymptomatic, required hospitalization or oxygen during illness, or patients who could not be contacted via telephone after 2 attempts a day on 2 separate days. Patients were enrolled consecutively in the study and were interviewed telephonically using a semi-structured questionnaire.
Ethics Statement
Ethical clearance was obtained prior to the commencement of the study from the Institutional Ethics Committee. Due to the ongoing pandemic, telephonic consent was taken from the patients (mentioned in the protocol). Permission to use the WHOQOL-BREF and FSS questionnaire was obtained from the World Health Organization and Dr Lauren Krupp (creator), respectively.
Data Collection:
Patients were interviewed using a semi-structured questionnaire which comprised of demographics, anthropometry, comorbidities, clinical symptoms, and duration of symptoms. It also included the following questionnaires. Long COVID-19 was defined as symptoms lasting more than 28 days from the date of COVID-19 diagnosis (11). Data on height and weight was self-reported by the patients. The data were collected regarding the duration of symptoms, fatigue using Fatigue Severity Scale (FSS), and quality of life using the World Health Organization Quality of Life: Brief Version (WHOBREF-QOL).
FSS: FSS was used to detect the presence and quantify the severity of fatigue. The FSS consisted of 9 questions, each answered on a 7-point Likert scale. A mean FSS score was calculated for the patient and a mean score of ≥4 was defined as significant fatigue. It has been used widely in various conditions for quantifying and assessing the severity of fatigue (15,16).
WHOQOL-BREF: This questionnaire was used to assess the quality of life and consists of 26 questions. Of these, 24 questions were divided into 4 domains—physical, psychological, social relations, and environmental. The remaining 2 questions assessed self-perceived ratings for quality of life and satisfaction with overall health (Questions 1 and 2). Responses were rated on a 5-point Likert scale. The raw score was converted into a transformed score on a scale of 0 to 100; the higher score indicates better quality of life. The overall WHOQOL-BREF score was calculated using the mean score of all 4 domains. WHOQOL-BREF has been validated across various populations in evaluating the quality of life in patients suffering from a varied spectrum of diseases (17–19).
Statistical Analysis
Data were recorded and analyzed using Stata 13. Descriptive analysis was performed for the prevalence, duration of symptoms, and scores of WHOQOL-BREF and FSS. Quantitative data were expressed as median (interquartile range—IQR) and mean (standard deviation—SD). The BMI was calculated and categorized with reference to Asian population (20). Prevalence of symptoms was reported with a 95% confidence interval. For the patients with symptoms at the time of interview, the duration of symptom was calculated from the date of onset till the date of interview. For test of significance, chi-square test/Fisher's exact test, Student’s t-test, and ANOVA were used. Correlation between the overall WHOQOL-BREF score, mean FSS score, and duration of symptoms was assessed using the Spearman’s correlation coefficient. Linear regression was performed to quantify the relationship between WHOQOL-BREF score and duration of symptoms. We used bivariable and multivariable logistic regression to assess the factors associated with the duration of symptoms >28 days (long COVID-19). Factors with potential significance (P value <.2) on the bivariable analysis were included in the multivariable logistic regression model.
Results
General Characteristics
A total of 300 patients were screened, out of which 32 patients did not respond and 17 patients did not give consent so finally 251 patients were enrolled in this study. The mean age of the participants was 35.8 years (SD = 12.5), and 169 (67.3%) were males. At least 1 comorbidity was present in 45 (17.9%) patients. A total of 174 patients were able to provide data on their height and weight (Supplementary Table 1). The median time to interview after the test of diagnosis was 62 days (IQR: 53.5-81).
Symptoms
The most common symptom reported at the onset of illness was fever (n = 184, 73.3%), followed by myalgia (n = 102, 40.6%) and sore throat in (n = 102, 40.6%) (Table 1). Among the 251 patients, symptoms of 208 (82.8%) patients had resolved completely at the time of interview. The prevalence of symptoms at 14 days (2 weeks) was 42.28% (95% CI: 36.2−48.4). The prevalence of symptoms at 42 days (6 weeks) was 16.3% (95% CI: 12.2−21.4%). The percentage of patients having symptoms at disease onset and after 28 days (n = 251) is shown in Figure 1.

Percentage of patients with symptoms at the presentation and beyond 28 days (n = 251).
Symptomatology Among COVID-19-Positive Patients (n1 = 251) and Duration of Symptom Among Recovered Patients at the Time of Interview (n2 = 208).

Patients had more than 1 symptom.
Conjunctivitis and eye pain.
Only 208 patients had recovered at the time of interview so symptom resolution was calculated in them.
Abbreviations: IQR, interquartile range; NA, not applicable.
The prevalence of long COVID-19 (>28days) was 28.2% (95% CI, 23.0-34.2). Only 1 patient with BMI <18.5 kg/m2 had persistent symptoms. Exercise intolerance was reported by 76 (30.2%) patients and 16 patients (6.37%) reported of anxiety or low mood. Out of the 203 people who were working before suffering from COVID-19, 181 (89.1%) patients resumed their work after a median duration of 13.5 (IQR: 14-22.5) days. The most common symptom to persist included musculoskeletal complaints (n = 32, 12.7%), upper respiratory tract symptoms (n = 19, 7.6%), and fatigue (n = 17, 6.8%) (Figure 1). The symptoms most likely to persist beyond 28 days were arthralgia (11 of 17 patients, 64.7%), followed by fatigue (17 of 54 patients, 31.48%) and myalgia (30 of 102 patients, 29.4%). Rates of resolution of individual symptom are provided in Supplementary Table 3. The duration of symptoms was significantly more in females compared to males (median 15 days vs 10 days, P <.01).
Post-COVID-19 Fatigue
A total of 54 patients (21.5%) complained of fatigue and this persisted beyond 28 days among 17 patients (31.48%) out of 54. When assessed using FSS, 32 patients (12.7%) had significant fatigue (FSS ≥4). This was significantly more common in females compared to males (25.6% vs 6.5%; P value <.01). Patients who had a mean FSS≥4 had symptoms lasting more than 2 weeks, 4 weeks, and 6 weeks, respectively, compared to those patients who had a mean FSS<4. (P value <.05) (Supplementary Table 4). The mean (SD) FSS score among patients with long COVID-19 (>28 days) was higher compared to patients without the same (<28 days) [3.5 (SD = 1.5) vs 1.3 (SD = 0.8); P value <.001].
Quality of Life
The overall WHOQOL BREF score for 251 patients was 68.5 ± 10.6. The mean (SD) overall WHOQOL-BREF score among patients with long COVID-19 (>28 days) was lower compared to patients without long COVID-19 (<28 days) [60.4 (SD = 13) vs 71.7 (SD = 7.4); P value <.001]. The mean (SD) overall WHOQOL-BREF score was higher in males when compared to females [70 (SD = 10.2) vs 65.5 (SD = 10.9)]; P value <.01) (Table 2). The mean WHOQOL-BREF score and symptom duration were negatively correlated (r = −0.53, P value <.01). In linear regression, 1 day increase in the duration of symptoms decreased the mean WHOQOL-BREF score by 0.3 (95% CI: −0.34 to −0.23, P value <.01) (Supplementary Figure 1A). The mean WHO-QOL BREF score and mean FSS score of individual patients reporting fatigue were negatively correlated (r = −0.62, P value <.01) (Supplementary Figure 1B).
WHOQOL-BREF of COVID-19 Patients (n = 251).

Abbreviations: IQR, interquartile range; WHOOL-BREF, World Health Organization Quality of Life: Brief Version.
Risk Factors
In the bivariable regression for determinants of symptoms >28 days (long COVID-19) factor which was potentially significant were sex, age, comorbidities, and BMI. In the multivariable regression, sex and BMI were significantly associated with the long COVID-19; females were 3.3 times (95% CI: 1.4–8.1) more likely to have long COVID-19 compared to males. Patients having BMI ≥23 kg/m2 were more likely to have a persistent symptom when adjusted for other variables (Table 3). As data on height and weight was self-reported by the patients, which could have affected the estimates so we made a multivariable logistic regression model after removal of BMI variable, and we didn’t find any significant difference between the 2 models.
Factors Associated With Symptoms Present at >28 Days (Long COVID-19) in COVID-19 Patients (n = 71).
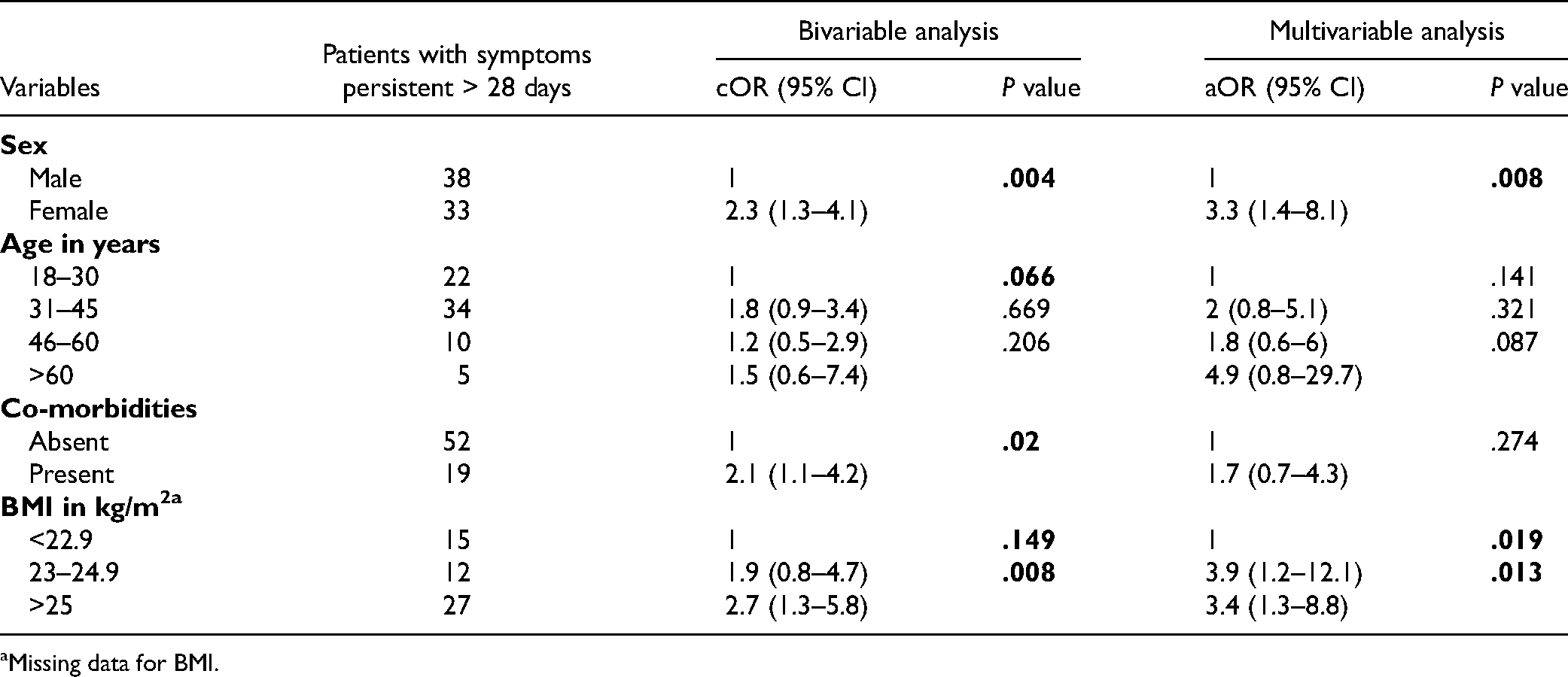
Missing data for BMI.
Discussion
The most common presenting symptoms reported by our patients were fever, respiratory tract symptoms, and myalgia. Published literature on the symptomatology in mild-to-moderate COVID-19 patients has reported a highly variable frequency of symptoms depending on the clinical setting and populations studied (8,21–23). Therefore, caution must be exercised while assessing the likelihood of COVID-19 infection in individual patients as no symptom seems to be universal and patients may seek medical attention for non-respiratory symptoms.
Our study showed that 28.2% of patients had long COVID-19 which commonly involved musculoskeletal complaints, upper respiratory tract symptoms, and fatigue. Viral illness is known to cause persistent symptoms including fatigue. Tansey et al. followed up on recovered patients of the 2003 SARS epidemic and reported fatigue as the most common symptom to persist (64% and 54% at 3 months and 6 months, respectively) (24). Lam et al. studied SARS patients from Hong Kong for 4 years and reported chronic fatigue in 40.3% of its patient pool (25). Chronic fatigue has also been reported in patients during the Ebola outbreak as well as many non-epidemic viral illnesses (25–28). Fatigue is a multifaceted issue that is often compounded with an associated physical disability, altered sleep patterns, psychological distress, and an overall reduced quality of life.
Post-COVID-19 fatigue has been reported by a few studies (7,8). Patients with symptoms persisting beyond 4 weeks were significantly associated with the objective presence of fatigue as assessed by FSS. This is consistent with findings of the study done at a European hospital where patients were assessed (100 patients, 68 wards, and 32 ICUs) post-COVID-19 discharge (9). They reported persistent fatigue in 35.3% and 53.1% of the ward and ICU admitted patients. The next common symptoms to persist were dyspnea and psychological distress. A study in Italy evaluated 143 patients post-COVID=19 discharge and reported 87.4% of the patients to have at least 1 persistent symptom, with fatigue (53.1%) as the most persistent symptom (7). The reason for a higher percentage of patients with persistent symptoms could be because their study population was relatively old (mean age = 56.5 years) and had a severe form of COVID-19. However, Wang et al. prospectively studied a cohort of 131 COVID-19 patients in Wuhan, China post-discharge and reported 86% of the patients to be free of symptoms by the end of 3 to 4 weeks and 1.5% prevalence of dyspnea (29). A Mediterranean study showed an incidence of post-COVID-19 syndrome (PCS) to be as high as 50.9% at median days of 77 days after disease onset. 30 However, they did not find any clinical features as risk factors for PCS. We found that patients with obesity, females, and those who presented with musculoskeletal symptoms and fatigue to be at higher risk for having persistent symptoms. The overall WHOQOL-BREF scores of our study participants were significantly better than those of participants in other studies done on healthy Indian individuals (18,19). However, the conspicuously low scores in the social domain highlights an additional dimension of difficulties faced during disease recovery from COVID-19 infection. The social disruption possibly stems from a multitude of factors including the need for isolation, movement restriction, and overall stigma associated with the disease in the society. When compared to patients having symptoms >4 and >6 weeks, patients with symptoms lasting less than 2 weeks had a significantly better quality of life scores indicating the major impact persistent symptoms had on the affected individuals. The FSS scores correlated negatively with the QOL scores indicating that higher levels of fatigue worsened perceived quality of life. The reported prevalence of exercise intolerance, psychological distress, and difficulty in performing daily activities point to the impact it has on the patient's QoL. Recent studies on COVID-19 also support this data. Halpin et al. reported neuropsychological distress in 31% of their cohort (9). Carfi et al. assessed the quality of life and reported worsened quality of life in 44.1% of the patients post-COVID-19 (7). A systematic review conducted to study the impact of the pandemic and the mental health consequences reported higher levels of post-traumatic stress symptoms and depressive symptoms in patients affected (14). This is observed in other epidemics of viral origin. A meta-analysis on short and long-term clinical outcomes of SARS and MERS found respiratory compromise, exercise intolerance, post-traumatic stress disorder, and reduced quality of life in recovered patients lasting up to 12 months after discharge (31).
Our study is the first of its kind from India to estimate the prevalence of symptoms of long COVID-19 and its impact on quality of life.
Limitations
Our study has its limitations; the median duration to interview was 62 days after diagnosis. The limitation to recall among the patients cannot be denied. Since patients with only mild COVID-19 disease and tested in a tertiary hospital were recruited in the study, the estimate may not be reflective of the overall prevalence of symptoms in symptomatic individuals. Patients were interviewed telephonically due to the ongoing pandemic using a questionnaire and this could have affected the findings of our study. We censored the analysis of duration of symptoms till the time of interview, as substantial proportion of patients (n = 43) had symptoms present at the time of interview. This study was not powered to determine the factors associated with long COVID-19. To generalize the findings further, community-based studies with a larger sample size are required with physical parameters and laboratory findings.
Interpretation and Conclusion
In conclusion, our study shows that more than one-fifth of the mild COVID-19 patients have long COVID-19. These consist most commonly of musculoskeletal complaints, respiratory symptoms, and fatigue. Patients with long COVID-19 had significantly higher FSS score and lower WHOQOL-BREF score compared to the patients without the same (<28 days). Increase in symptom duration significantly affects the quality of life. A special post-COVID-19 clinic may help in addressing these issues impacting the quality of life.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735221117358 - Supplemental material for Prevalence of Long COVID-19 and its Impact on Quality of Life Among Outpatients With Mild COVID-19 Disease at Tertiary Care Center in North India
Supplemental material, sj-docx-1-jpx-10.1177_23743735221117358 for Prevalence of Long COVID-19 and its Impact on Quality of Life Among Outpatients With Mild COVID-19 Disease at Tertiary Care Center in North India by Radhika Sarda, Arvind Kumar, Ankit Chandra, Megha Bir, Sanchit Kumar, Manish Soneja, Sanjeev Sinha and Naveet Wig in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.