
Abstract
Introduction
Managing multiple health conditions can create a demanding workload, especially when capacity is limited. This can lead to disengagement and poor health outcomes. Our pilot trial explored the feasibility of care coordination using a minimally-disruptive medicine approach.
Methods
The setting was a community health service in rural Victoria, Australia. People with multimorbidity and complex life demands were linked to care coordinators who evaluated and addressed burden and capacity imbalance, informed by client priorities. Clinicians underwent training in capacity-burden assessment and participated in ongoing case conferencing. A mixed-methods evaluation was undertaken guided by Bowen’s feasibility framework with treatment burden and quality of life as quantitative outcomes.
Results
26 clients (mean age 66.5 years) engaged with 3 care coordinators. Clients reported high treatment burden with a mean of 11 chronic conditions each, dominated by mental health and chronic pain conditions. The program was highly acceptable to clients, who reported increased control over their health and life demands. Six-month outcomes showed a significant reduction in treatment burden level (MMTBQ) p=0.019, Phi=0.524 and improvement in quality-of-life scores (EQ-VAS) p=0.019. Clinicians valued the program and highlighted the importance of putting aside one’s discipline lens and focusing on the client priorities, aided by the assessment tools and training.
Discussion
A burden-capacity model of care coordination is feasible in the community health setting and may lead to reduced treatment burden. Barriers identified were related to community health funding and structures favouring single diseases and disciplinary boundaries, which may not reflect the lived experience of clients.
Introduction
Effective management of chronic health conditions (CHCs) requires long-term commitment to self-management, but adherence to such approaches is known to be poor.1–3 Traditional self-management focuses on building individual capacity and self-efficacy to manage ones’ health,4,5 and this can be overwhelming, especially for those with few resources.6,7 People need sufficient capacity, including social support, socioeconomic resources, and adequate mental/physical functioning, to cope with the workload, or burden, associated with living with a CHC, such as self-management tasks, health system interactions and other life demands. Treatment burden 8 has been explored using Normalization Process Theory to describe the complex and interlinked mechanisms required to embed chronic condition management into one’s everyday life. Shippee et al.’s Cumulative Complexity Model 9 builds on Burden of Treatment theory by describing how illness burden (symptomatology) impacts on treatment burden. If individual capacity (e.g. social or financial resources) is insufficient, or life demands are too great, negative feedback loops can result, reducing treatment adherence and leading to disease escalation. Healthcare systems typically respond by intensifying treatment, increasing burden further and resulting in ‘cumulative complexity’. 9
A traditional self-management approach which focuses on the individual patient, rather than considering the fit between patient and healthcare system, 8 can be challenging for those with high healthcare demands and/or low resources, whether physical, social or material. 10 Minimally Disruptive Medicine (MDM)11–14 is a practical model of care that builds on the concepts described in the Cumulative Complexity Model and Burden of Treatment theory,13,14 and advocates for health systems to fit patients instead of the other way round.
The key elements of MDM are: 1. To assess burden and capacity levels 2. To undertake practical actions designed to reduce burden and/or increase capacity.
Examples of actions are medication deprescribing, shared decision-making, care navigation and teaming with social welfare agencies. Although many of these strategies are recommended when managing multimorbidity,15,16 incorporating them into a systematic approach which targets burden-capacity deficits is less common.
While integration of MDM into primary care settings is still in its early days,17–19 interventions that focus on burden and/or capacity in disadvantaged or multimorbid patients have reported improvements in patient engagement with healthcare, quality of life, lower emergency healthcare utilisation and reduced treatment burden.20,21 An MDM approach can also benefit healthcare providers (HCPs), since managing complex multimorbid clients in socially deprived circumstances is a well-known stressor and can contribute to burnout.22,23 Provision of training and resources to address complex multimorbidity has been recommended to improve HCP well-being, 23 and HCPs who have skills and organisational capacity in these areas have reported lower rates of burnout. 24 Therefore, interventions designed specifically for these contexts, rather than current single disease models which ignore burden and capacity25,26 may improve patient outcomes, reduce HCP burden and promote truly client-centred care.22–24
Objectives
This paper describes a pilot trial of an MDM-based intervention for multimorbid community health clients living in rural Victoria, Australia. The aim was to assess the feasibility and acceptability of an MDM care coordination intervention, from the perspective of clients and health providers who participated in the program.
Methods
Study design
This was a pilot trial using a mixed-methods study design. Since the focus was on feasibility, we applied Bowen et al’s 27 framework to guide our evaluation.
Study setting/context
The trial was undertaken in a large rural town in northwest Victoria, Australia (population 57,000), located 400km from the next town of equal or greater size. The area has an older population with high rates of chronic health conditions, and with health workforce shortages especially of general practitioners (GPs). 28 The setting was a community health centre with approximately 200 employees. Community health centres provide state-funded primary healthcare under a social model of health, focusing on those with greater social and economic need. They employ a diverse range of health and social care disciplines in services ranging from antenatal to palliative care and drug and alcohol programs to chronic disease management. 29
The chief investigator (CI) was funded for 2 days/week to undertake the research and evaluation. All care coordinators were able to undertake the intervention as part of their usual role, with the addition of one hour per fortnight case conferencing.
Study sample/participant recruitment
Client inclusion/exclusion criteria.

Intervention
Prior to commencing the intervention, training in MDM was offered to nursing and allied health clinicians who worked in chronic disease management. Content included theory (the Cumulative Complexity model) 9 ; use of the shared decision-making tool (ICAN)18,19; building skills in generic/synergistic treatments30,31 that apply across multiple conditions, such as sleep hygiene, stress management, establishing daily routines and behavioural activation; and the use of clinical vignettes to practice application of MDM. Thirteen clinicians attended the workshops during April-July 2022, and three subsequently expressed interest in a care coordinator role. The first client was referred for care coordination in August 2022 and the program concluded in September 2023.
Key intervention elements were: • Use of the ICAN and care plan tool at the first client encounter, to assess and document burden and capacity. The ICAN18,19 is a self-report tool, specifically developed to support an MDM approach.
19
It rates individual capacity and burden and is designed to initiate a client-clinician conversation on this topic. A care plan document (see Appendix 1) was developed in-house to complement the ICAN. • Treatment choice and priority to be based on burden/capacity assessment. Treatments could include health coaching; education; care navigation; the use of generic interventions as outlined earlier; or referrals to other health or social services, supported by the online ‘health literacy document’ which contained resources, linkages and local referral pathways. • Participation in fortnightly case discussions. This was an opportunity for care coordinators to both reflect on clients with each other and to seek condition-specific advice from a ‘secondary consult’ team, consisting of a diabetes nurse practitioner; a senior mental health nurse, and a titled pain physiotherapist (who was also the chief investigator). • At least 2 ICANs and care plans to be completed over the course of engagement, timing based on clinician assessment of need. • Discharge based on clients’ needs and preferences.
Intervention timeline.

Outcome measures
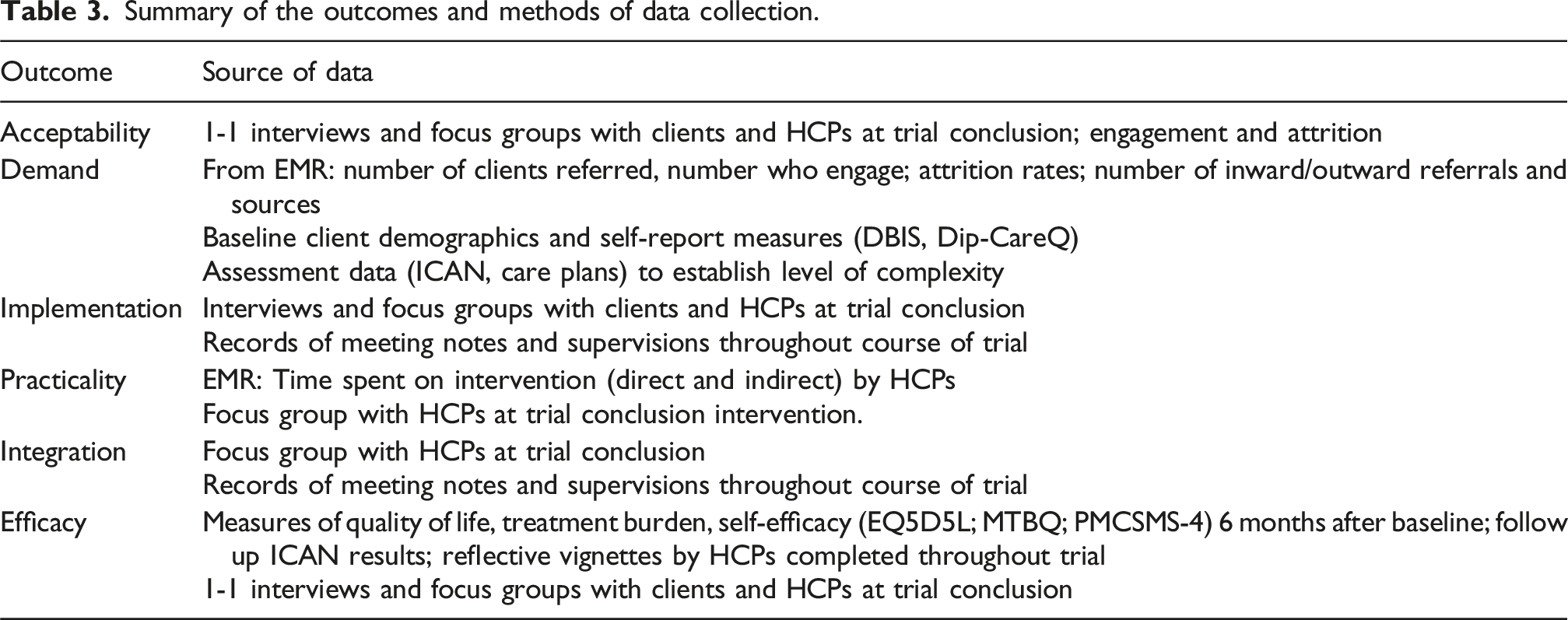
For a feasibility study, using a mixture of quantitative and qualitative methods enabled us to understand barriers to participation and implementation. Feasibility outcomes were explored using the framework developed by Bowen et al, 27 covering acceptability, demand, implementation, practicality, integration, and efficacy. Table 3 describes data sources for each implementation outcome.
Qualitative data included interviews, focus groups, meeting notes, care planning documents and reflective vignettes, to explore the views and experiences of all stakeholders. Clients were interviewed by phone following the intervention and this was recorded and transcribed verbatim. Clinicians participated in a 60-minute focus group which was recorded and transcribed verbatim. Completed ICANs, care plans, case conference notes and reflective case-studies (template in Appendix 1) completed by clinicians were also included in the qualitative analysis.
Quantitative data included client demographics, attendance records, and referral patterns all of which were obtained from the electronic medical record (EMR). Social, health and financial disadvantage was recorded at baseline using the DiPCare-Q (Deprivation in Primary Care Questionnaire) 32 and number and type of health conditions measured using the DBIS, Disease Burden Impact Scale. 33 Measures of health-related quality of life (EQ-5D5L); treatment burden (Multimorbidity Treatment Burden Questionnaire, MMTBQ) 34 ; and Self-efficacy (PMCSMS-4) 35 were completed at baseline and six months after initial engagement with the service.
Data analysis
Qualitative data was analysed descriptively and coded according to the Bowen feasibility framework. 27 Interviews were transcribed verbatim by the authors and a research assistant. Coding of interviews was undertaken by ES and RH independently but simultaneously, utilising the steps of framework analysis: transcription, familiarisation, coding, developing, applying, charting and interpreting. 36 Findings were reviewed with a series of consistent themes agreed on. Disagreements were resolved in discussion with all authors.
In view of the small sample size and lack of control group, quantitative analysis was largely descriptive with limited exploration of data trends. We undertook bivariate analysis (chi-square and matched-samples t-tests) for pre-post quantitative data, using Jamovi 37 statistical software. We used the STROBE 38 checklist (Appendix 3) to assess our report.
Ethics
Ethics approval was obtained from La Trobe University (HEC 22026) and research conducted in accordance with the Declaration of Helsinki. Informed written consent for quantitative and qualitative data was completed for all participants.
Results
Participant characteristics
Of thirty clients referred into the program, two were ineligible and two declined to participate. Twenty-six clients were enrolled in the program and completed baseline measures.
Summary of the outcomes and methods of data collection.
Intervention characteristics
Demographic and health characteristics.

aDepression n=21; Bipolar disorder n=1; PTSD n=1; BPD/complex PTSD n=1.
bLow/medium/high scored as per Duncan et al. 34
cScore calculated as per Vaucher et al. 32
Burden/capacity assessments (ICAN and care plan) and reflective case-studies were completed for 23 clients and post-trial quantitative data obtained for nineteen clients. At the trial conclusion (Aug-Sept 2023), telephone interviews (4-19 minutes in length, median 15 minutes) were undertaken with twelve clients, after which data saturation was deemed to have been achieved. Care coordinators participated in a 60-minute face-to-face focus group.
Results have been reported under the Bowen et al feasibility headings 27 and include reflections from clients followed by those from clinicians, where relevant.
Acceptability
Acceptability explores the perceived benefits or otherwise of the intervention from the perspective of clients and HCPs, including suggested improvements. ‘CC’ (care coordinator) refers to the clinician participant.
I just think it [the care coordination program] worked really well. For me, and hopefully for others too, and I think they should try and keep it going for as long as possible. (client 3, F, 70y) I think it [the program] would be good for others maybe the elderly and people living alone especially people who haven’t got family around (client 12, F, 68y).
The time allowed by clinicians to develop a relationship, compared to the brief time-pressured GP consults most people were used to, was important. Clients expressed relief that there was finally sufficient time and willingness to explore their complex issues. Several clients referred to the clinician as a friend, who they enjoyed spending time with and with whom they could have ‘a laugh’. They hear you. They listen to you about what you are concerned about…(CC) knows how to say the right things at the right times. And that's because (CC) listens to me. (client 1, M, 69y)
A secondary element, also identified by most clients, was the ongoing encouragement and support provided by their clinician, especially in terms of self-management and health education. (the CC) gets along with me and encourages me and gets me going and back up again. Mentally, physically, you know.(client 1, M, 69y) (the CC) does give you an incentive to keep going.(client 2, F, 72y)
Clients also appreciated the focus on their individual priorities and concerns, and this encouraged them to see themselves as partners in their healthcare rather than patients. [It was good] That (the CC) did work together, we worked together. It was an individual thing… (CC) didn't try and tell me what to do, and they didn't expect me to do it all on my own either, so that was very good. (client 3, F, 70y)
Several clients noted that this was in stark contrast to their usual experiences of health service delivery, which were often impersonal and invalidating. (CC) has been able to listen for my concerns rather than just telling me what to do. (client 9, F, 55y) (CC) seemed to be more interested in my problems. A lot of professionals - they are what I said. They are professionals. They don't have much feeling. They just do the job and that's about it. But (CC) had feeling. (client 6, M, 72y)
The focus on client priorities meant that clinicians were often addressing needs beyond health conditions, for example financial concerns. Many clients valued the provision of a range of options and ideas, especially the fact that clinicians would follow up and resolve concerns properly rather than simply handing them on to someone else. The difference is that (CC) has never promised me anything they have gone ahead with things - like other workers have promised me things and done nothing. (CC) has gone ahead and done what they said they would do.(client 10, M, 64 y) I've just found that I have been able to make comments to (CC) and they have been able to offer that ear and have said, Oh well, maybe you can try this or maybe you can try that… So I just found with (CC) it opened doors.(client 4, F, 82y) (CC) just said anything… Any problem I have got they can work out something or they can send you off to somewhere else to get help….and they follow up too.(client 5, F, 75y)
For good to have that one contact for them, so they know just if they need help, they can contact that one person…otherwise it's… they're trying to ring 15 different people… that's when they get overwhelmed…(CC2)
All clinicians felt that the focus on burden and capacity had been beneficial for their clinical practice. They reported that this focus changed their perspective on their clients’ needs, enabling them to look beyond their specific disciplines and be more open to client priorities. I think it eliminated our clinician bias and… Obviously, each clinician is in their own realm and then this sort of, a program or a tool like the ICAN or the care plan sort of eliminates that sort of area, right? (CC3)
Although the eligibility criteria specified multimorbidity, clinicians felt that psychosocial complexity was a more important factor for most clients, and a better indicator of those likely to benefit from care coordination. Additional psychosocial complexity is the biggest issue, not the health conditions… quite often they come in and you don't address the health issues you address the social issues…(CC3)
Demand
Demand is an exploration of the numbers of people engaged and whether those engaged were the intended target population for the intervention. The demographic characteristics (Table 4) indicate that participants fitted the expected population with high levels of treatment burden and multimorbidity.
The ICAN tool, care plan and reflective case studies were used to explore the impact of capacity and burden on individual participants. Lower levels of capacity were experienced in the domains of emotional well-being, physical functioning, and financial capacity, with fewer than 20% of clients reporting satisfaction in these areas. Support from family and friends was a relative strength, with 50% of clients reporting increased capacity from this source. Perceived burden was largely related to psychosocial factors, specifically poor mental health, social isolation and limited practical resources (finances, transport, housing).
Care coordination services provided to participants.

Implementation
Implementation explores fidelity to the key elements of the intervention; adaptations made; and barriers and enablers to implementing the programme as planned.
Fidelity to the burden-capacity model was explored in trial process data and interviews. Table 5 describes the tasks completed by clinicians (as documented in the EMR and reflective case-studies), which illustrate the focus on reducing burden and increasing capacity.
(the CC) sat there and said, is there anything I can do for you in any way or any form? Be that financial or medical, healthwise, whatever. And what I loved about it is that (CC) said, if I don't know the answer, I will find out for you or refer you to someone who does..(client 5, F, 75y) I arrived in front of (the CC), …they started to talk about the trial. And [the community health organisation] just opened up to me like an oyster…And (the CC) was the sheep dog at the back…they were following up everybody and everyone.(client 11, M, 60y) [the focus was](to) work out what I needed and what my goals were. That was really good (client 3, F, 70y)
it sort of forces you to ‘OK, maybe, … that's clearly not, your priorities don’t align with the clients…(CC1) …it's sort of seeing it from more their point of view and working out what their main things are, whether it's to fix their broken toe or fix their broken window in the house.(CC3)
Clinicians reported that the online health literacy resource, fortnightly case conferencing, and the assessment tools all helped maintain the focus on burden and capacity, although they felt the assessment tools could be combined and modified to more closely suit the client population. the case conferencing with like the three of us and [the CI] was very beneficial. Just touching base and seeing what [the other participants] are doing differently to what I am, what ways we can help the clients, was really good (CC2)
Barriers to implementation were related to role familiarity and to bureaucratic systems. At times, clients and other health providers (especially GPs) were unclear about the clinician coordinator role. Most clients and providers expected chronic disease clinicians to provide disease-specific and discipline-specific services. This was a change for clients, other HCPs, and the clinicians themselves, and required education and explanation. However, in general the clinicians found that they were able to strengthen their connections with other providers across and outside the organisation. System and organisational bureaucracy, especially the aged care referral and linkage processes, remained challenging to navigate, but the assistance of a clinician was in some cases crucial to obtain appropriate support. It's made a big difference at a minimal cost, but it took too much arguing [to initiate the program], for an organisation that’s meant to be about improving people’s health…so management was the biggest barrier that I’ve come across.(CC2)
Practicality
Practicality includes time costs and additional administrative support. Data was obtained from the EMR.
Initial training consisted of 6 hours. Case conferencing occurred for one hour per fortnight and was deemed essential for performance of the role.
There was a median of 4 face to face appointments (each lasting 45 minutes) and 8 phone calls per client (mean 28 minutes per call). Clinicians reported that an initial or early face-to-face appointment was important to make a connection and build rapport and empathy but after that much of the contact and follow up happened over the phone and for most clients this was ideal and helped to reduce burden. The use of email and especially texts to and from clients was highlighted as a simple way to remain in touch with minimal client burden.
All clients required indirect time for follow up of specific issues, but this varied from 15% to 70% of total client contact time, mean 3 hours per client, range from 1 to 15 hours. Some clients received more direct contact for health coaching purposes, whilst those who required multiple onward referrals and liaison had more indirect time recorded.
Integration
Integration explores the extent to which the intervention could become part of the routine organizational practices and policies and is thus focused on the perspective of health service employees rather than clients.
Personal traits of clinicians as well as organisational pathways were considered critical for long-term sustainability.
The importance of rapport building, as well as a willingness to step away from ones’ comfort zone or discipline and to explore whatever was needed to support the client, regardless of whether this was currently in their skillset, was consistently stressed by all participants. [what care coordinators need]…another attribute they need to have… someone that can say, I actually don't know, but I will find out, rather than try and fumble their way through it.(CC2) …you have to be happy to step out of your comfort zone… I think you have to want to make a meaningful difference to that person based on what their meaningful difference is.(CC1)
In relation to organisational integration, clinicians identified several important elements. These were. 1. Formal development of the care coordination role, providing vulnerable individuals with a single key contact, rather than encouraging everyone in the organization to ‘dabble’ in care coordination. Discipline or disease-specific care coordination was not considered necessary or even desirable, since for most clients the psychosocial rather than medical issues were paramount. 2. Systematic and early identification of clients at risk of burden-capacity imbalance, with a clear pathway from intake screening to linking with a clinician providing care coordination. 3. Ensuring care coordination remained a free or minimal-cost service, given the high level of financial burden identified amongst participants. 4. Regular and scheduled case conferencing 5. Having an open-door policy toward client reengagement. Despite the level of complexity, most participants were discharged from the service within nine months. However, an opportunity to reconnect as needed would recognize their long-term and fluctuating medical and social challenges. 6. Build connections and familiarity with GP practices and practice nurses around complex clients, to provide clear pathways enabling them to engage with the service. I think you might connect with… the GP management plans. Because they are very medically focussed, but then when it comes down to finance, social and all those other kind of things, it could be a referral into a care coordinator program.(CC3)
At the same time, clinicians identified that there were significant health system challenges with this model of care, which requires people to work across teams and doesn’t fit into standard discipline- or disease-specific models of care or funding.
Efficacy
Engagement pathways.

During interviews, clients were asked whether they thought there had been a change in their healthcare and, consistent with the focus on reducing treatment burden, one area of change reported was having more supports in place to manage their health. At the moment everything is in place. And I said that to (CC), everything is in place because (CC) has organised it. It's all just flowing along beautifully.(client 5, F, 75y) (getting the supports in place)… that release of pressure was fantastic. It was just like ‘oh thank goodness’... All this clutter has dropped away… It’s just a different outlook on life. (client 11, M, 60y) Six month outcomes, n=19.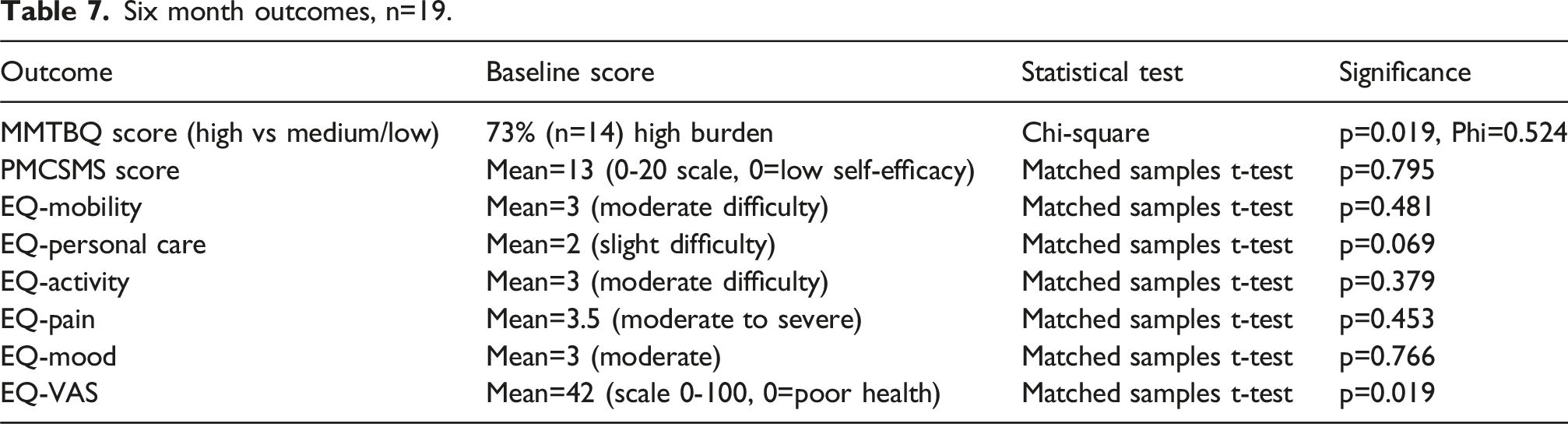
The second key change identified by clients was an increase in control and confidence in managing their lives, and feeling more hopeful about the future, which they related to the consistent support provided by their clinician. I’m feeling a lot more in control. I feel a lot more confident in handling myself and knowing that there is health help out there if you need it.(client 3, F, 70y). There’s a word for it. (CC) has helped me live on. And things have been bad for me, really bad with health problems and that. And (CC) has given me a little bit of hope.(client 10, M, 64y)
Clinicians echoed the above themes. They observed that whilst reduction of treatment burden associated with identifying priorities and providing appropriate linkages was important, a side benefit was that clients then felt empowered and more in control. This in turn built their capacity to communicate and engage with the services they needed. …it allows them to be able to take control a little bit more of their burdens… said, you're sort of acting as almost like a bit of a voice for that client when obtaining other services(CC2) … it improves their ability to communicate with the health professional that can then educate them(CC3)
Discussion
This pilot study aimed to explore the feasibility of an MDM model of care to support rural community health clients with multimorbidity and social complexity. The trial was evaluated using qualitative and quantitative data according to Bowen’s feasibility framework.
Acceptability was high amongst both clients and clinicians. Both groups stressed the importance of relationship building and for many clients this provided an increased sense of control over difficult circumstances. Clinicians valued the emphasis on burden and capacity which gave them a deeper understanding of their clients’ needs and priorities. In terms of demand, whilst fewer clients engaged than expected, those who engaged were a good fit for the intervention, with high levels of treatment burden, social isolation and financial stress. Implementation of the MDM model was feasible and trial documentation demonstrated fidelity to the burden-capacity focus. Important enablers included case conferencing, clear referral pathways and health literacy resources. The trial appeared to be practical, especially since much of the care coordination happened by phone, text and email rather than face-to-face. Allowance for ongoing indirect time (which was highly variable between clients) was an important component. Integration of the trial model into the organization longer term was enthusiastically advocated for, but the focus on burden and capacity, rather than care coordination per se, was considered the key element. The key sustainability challenge was funding models based on health conditions and disciplines that do not reflect multimorbidity and psychosocial complexity. There was limited exploration of efficacy given the small sample size and lack of a comparison group, but initial qualitative and quantitative observations were encouraging and support further investigation.
Key themes that emerged from this study were
Capacity-burden management is foundational for effective care coordination
Care coordination, where a clinician works with a client to manage their care, is commonly recommended for multimorbid clients in primary care20,26,39 and is expected to reduce treatment burden. Once a key part of the GP role, changes in both the health system (e.g. reduced GP consult times) and in patient complexity mean that it is now more often undertaken by nurses or allied health professionals. In rural settings, where GP shortages are acute, these roles can be crucial for continuity of care. This study underlined the importance of embedding capacity, burden and priority. Without this, care coordination can become an additional burden – for example by providing a client with everything they ‘need’, often to ensure ‘guideline based care’, rather than what is most important to, and manageable for them. This can easily become overwhelming for a client with multiple chronic conditions and limited resources. 40 Therefore, care coordination without attention to burden, capacity and priority is of limited benefit.
Multimorbidity is a biopsychosocial experience
Multimorbidity typically refers to diagnosed medical conditions such as diabetes and cardiovascular disease, 41 but in common with other studies,42,43 chronic pain and mental health conditions were the most reported and prioritized conditions for this group. Whilst these conditions often do not have a high component of treatment burden, they have significant impacts on capacity.44,45 In particular, poor mental health and limited resources (e.g. finances or social support) were associated with higher experience of treatment burden even without a high number of actual treatment tasks and this is consistent with other studies.44,46 This emphasises the importance of applying a biopsychosocial lens to multimorbidity and learning from relevant models such as those developed for persistent pain47. For the care coordination role, psychosocial skills were considered to be at least as important as medical knowledge. Bearing this in mind, although our focus was on multimorbid participants, this suggests that a capacity-burden approach may also be useful for those with fewer medical conditions but greater psychosocial complexity.
The need to transcend disciplinary limitations
The clinician focus group reported that skills in rapport building and listening were foundational for the role. Specifically, a willingness to step away from one’s disciplinary boundaries and be open to the clients’ needs and priorities, rather than maintaining preexisting ideas about what constitutes chronic disease self-management, was crucial. This is also consistent with the need for psychosocial rather than medical or disease specific expertise. Both clients and clinicians reflected on the need to be willing to ‘not know’ things but be prepared to find things out, in response to client need. This relational and exploratory approach is at odds with many health systems which are expertise-based, discipline- and disease-specific.48,49 Whilst clinician-participants found benefit, they also observed that at times they had to step out of their comfort zone to take on the role. It requires people to be facilitators rather than medical experts and may therefore sit better with health coaches or even peer workers with sufficient training and support. However, if as posited the barriers in managing chronic disease relate to burden and capacity, the expertise must be in ‘soft’ skills. Building trusting relationships might be more important for optimal management of multimorbidity than strict adherence to guideline-based care.
Health system challenges
Current recommendations for chronic disease care recognise that multimorbidity is the norm and an integrated approach to management is required. 26 However, the reality is that both funding systems and health disciplines still largely operate in single-disease silos.48,49 Additionally, for many people their medical conditions intersect with socioeconomic, psychological and environmental factors that traditional primary care has limited capacity to address. 22 For our population, although supports via disability and aged care organisations were funded, they were often not accessible. Care coordinators were key to enabling connection and opening the gates between disparate health and social services. The challenge remains that this bridging role of care coordination (which can be time-consuming) is rarely recognised or reimbursed, since it falls between the gaps of health system funding silos. This means that such interventions may struggle to progress beyond pilot programs unless there is integration into the wider healthcare system.
Strengths and limitations
This was a small pilot trial undertaken in a specific location: an Australian rural community with significant GP shortages, where it was difficult to achieve care continuity in a traditional primary care setting. The sample was small, with no control group, therefore outcomes must be interpreted with caution. However, the setting is not dissimilar from many rural communities with health workforce shortages and older, low-resourced populations. Additionally, the finding that treatment burden was significantly reduced with evidence of a moderate effect size supports further investigation. Larger experimental studies (e.g. cluster RCT) using capacity-burden approaches to reduce treatment burden are warranted. In addition, exploring the use of peer workers (who are not widely used in Australia outside of the mental health context) may provide a more affordable and available option. Due to resource limitations and the feasibility focus, our study focused only on answering specific questions related to the feasibility domain. Future qualitative and quantitative investigation in a larger sample could include a more comprehensive qualitative analysis of participants’ experience; use of acceptability metrics; exploration of the impact on social disadvantage measures; and formal cost-effectiveness measurement.
Conclusion
The success of this trial supports an approach to chronic disease self-management that is focused on burden and capacity. Chronic disease self-management has been criticised in the past for its focus on building individual client skills without addressing the barriers faced by those who are overburdened or under resourced.50,7,51 This can reduce engagement for those experiencing medical and psychosocial complexity. 50 In our trial we focused on providing self-management support, via care coordination which was informed by client burden and capacity. Our results suggest that addressing burdens and priorities first (which may initially mean more work for the clinician) might provide the foundation that is needed for people to effectively build their self-management capacity.
Supplemental material
Supplemental material - Focusing on burden and capacity to support self-management of chronic health conditions: A pilot trial of care coordination in rural Australia
Supplemental material for Focusing on burden and capacity to support self-management of chronic health conditions: A pilot trial of care coordination in rural Australia by Ruth Hardman, Stephen Begg, Evelien Spelten in Journal of Multimorbidity and Comorbidity.
Footnotes
Acknowledgements
The authors would like to thank all clinicians and clients who participated in this trial.
Ethical considerations
Ethics approval was obtained from La Trobe University (HEC 22026) and research conducted in accordance with the Declaration of Helsinki.
Consent to participate
Informed written consent for quantitative and qualitative data was completed for all participants.
Consent for publication
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially funded by a partnership grant from the Violet Vines Marshman Centre for Rural Health Research and Sunraysia Community Health Services.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.