
Abstract
Background
In sub-Saharan Africa, the rising burden of noncommunicable diseases (NCDs), such as diabetes mellitus (DM) and hypertension (HT), coexists with the ongoing challenge of HIV, a leading cause of death. People living with HIV (PLHIV) also have NCDs, which may affect their healthcare experiences. This study explored patient perceptions of the quality of care received by PLHIV, with and without NCDs, at an antiretroviral treatment (ART) clinic in an urban district hospital in KwaZulu-Natal, South Africa.
Methods
A sequential mixed-methods design was employed, comprising quantitative and qualitative phases. A structured questionnaire was systematically administered to 301 patients, followed by semi-structured interviews with ten purposively selected persons living with HIV (PLHIV), either without comorbidities or diagnosed with HT, DM, or both. Quantitative data were analysed using factor analysis and Principal Component Analysis (PCA) to identify key themes, while qualitative data were analysed using thematic content analysis based on the Donabedian Framework.
Results
Quantitative findings indicated that 86% of patients expressed overall satisfaction with their care. However, qualitative insights highlighted structural, procedural, and outcome-related challenges, including long waiting times, staff shortages, and varying perceptions of healthcare provider competence. Patients prioritised HIV treatment. While some instances of integrated care were reported, fragmented service delivery remained prevalent.
Conclusion
Although most patients reported positive care experiences, long waiting times and inadequate staffing negatively impacted service delivery. Strengthening health education is essential to improve patient adherence. Expanding integrated care and addressing staffing shortages could enhance the overall quality of care for PLHIV, particularly those with comorbid NCDs.
Introduction
Globally, an estimated 70 million individuals are living with HIV, with South Africa (SA) bearing a syndemic burden of disease, prominently featuring chronic communicable and noncommunicable diseases (NCDs). 1 With the advent of antiretroviral therapy (ART), HIV has transitioned into a chronic, manageable condition, significantly extending patients’ lifespans 1 and consequently predisposing them to the development of NCDs, which remain the leading cause of death worldwide.2–5 Noncommunicable conditions such as diabetes mellitus (DM) and hypertension (HT) constitute significant contributors to the NCD burden in sub-Saharan Africa, where over 36 million people succumb to NCDs annually, primarily affecting populations in low- and middle-income countries (LMICs). 6 Data on this subject is sparse, but a small study done on five facilities in Eswatini in Southern Africa showed that 23% (n = 59) of deaths in PLHIV were due to NCDs and this was broken down as follows: (HT related =18%, DM=5%, Cardiovascular disease = 15%, Anaemia =6%. Seventy-three percent (73%) of these participants had HIV Stage 1 or 2 disease. 2
Advancements in ART have led to increased longevity, consequently elevating the risk of developing DM and HT among persons living with HIV (PLHIV). Numerous studies have underscored DM and HT as the most prevalent comorbidities in PLHIV.7–9 Projections suggest a concerning trajectory, with an anticipated doubling in NCD-related deaths in the region by 2030, highlighting the urgent need for effective management strategies. 10
South Africa boasts the most extensive public sector antiretroviral therapy (ART) rollout programme globally, encompassing over 80% of PLHIV. 11 To address the evolving healthcare landscape, South Africa has embraced the Integrated Chronic Disease Model (ICDM), which encompasses facility reorganisation, clinical management support, assisted self-management at the community level, and health promotion and population screening initiatives. These efforts aim to integrate HIV and NCD services across various care settings and are already underway, recognising the prevalence of NCDs among PLHIV.(12) Integrated care models in this study are defined as care for HIV and NCDs in one clinic. Fragmented care is care for HIV and NCDs that happen in different clinics.
Understanding patients’ perspectives on care experiences is paramount for tailoring person-centred care models effectively. Integrated care models have shown promise in reducing stigma, minimising travel costs, and improving overall patient outcomes. 1 However, experiences from other settings, such as Cambodia, underscore challenges like prolonged waiting times due to budget constraints and staff shortages, necessitating a nuanced approach to implementation.1
This study was motivated by the concerns of overburdened healthcare workers (HCWs) seeking insights into patients’ perceptions of received and expected care. While literature identifies gaps in the holistic management of multimorbidity, limited attention has been given to patient perspectives on integrated healthcare for HIV and NCDs, particularly in the district hospital setting. Our research question for this study was to explore patient perceptions regarding the quality of care that was rendered to PLHIV with and without NCDs. We gauged insight into the lived experiences of the participants, the model of care they received, and the treatment they prioritised.
Methods
Research design
This study utilised a cross-sectional mixed-methods design. The focus of this study was to gain insight into the quality of care of NCDs among PLHIV patients as well as those without NCDs.
Setting
This cross-sectional study employed a sequential mixed-methods approach, integrating both quantitative and qualitative data to gain insight into the quality of care for NCDs among PLHIV, with or without comorbidities. Conducted at the ART clinic of a district hospital in KwaZulu-Natal, South Africa, the study’s setting catered to a catchment population of 410,000 and received referrals from seven nurse-run primary healthcare clinics. Approximately 1,379 PLHIV receive care monthly at the ART clinic, with about 25% having DM and/or HT. The clinic offers integrated care for some PLHIV with comorbidities, while others receive only HIV care and access NCD treatment at outpatient departments or primary healthcare clinics, depending on patient and provider preference.
Target population/Study population
The study was conducted amongst PLHIV and accessing care at the antiretroviral therapy (ART) Clinic in Wentworth Hospital (WWH), KwaZulu-Natal, South Africa. All participants were PLHIV with or without an NCD. All male and female adult patients (18 years and older) who were HIV positive and presented to the WWH antiretroviral therapy (ART) Clinic and were willing to participate were included. Patients who were cognitively impaired were not included.
Sampling strategy
The sample size of 301 was estimated using a confidence level of 95% with a precision of 5% based on a study population of 1379 patients who collected antiretroviral therapy (ART) at the hospital during July 2017 and 10 PLHIV with or without a comorbidity were included in the qualitative part of the study. Research aims such as the difference in the model of care used for patients with HIV only and with HIV and NCDs were included. These research aims were considered during interpretation but were not explicitly included in the sample size calculation.’ Prioritisation of treatment for HIV and NCDs was also included.
Patient questionnaire
Sampling was conducted as participants were waiting to see the doctor. Every second patient was approached, and if they refused to participate or were not eligible, the next patient in the line was approached.
Patient semi-structured interviews
Patients were purposively sampled as they awaited their consultations.
Data collection and study tools
Our study consisted of two phases of data collection that generated both quantitative and qualitative data. Recruitment was from April 2017 until November 2017. All interviews were conducted in English. Quantitative data was collected using a satisfaction survey (Supplemental file 1). Qualitative data was collected through semi-structured qualitative interviews (Supplemental file 2) by the Principal Investigator (PI). Participants were given an overview of the study and invited to participate. After agreeing to participate, they signed written informed consent.
Patient questionnaire
Participants were recruited as they waited for consultations. For the quantitative arm, a survey assessing satisfaction with care was administered to 301 PLHIV. The survey, adapted from a validated tool by the Rand Corporation 2 (Supplemental File 3), was available in English and isiZulu. It consisted of structured questions designed to evaluate perceptions of care quality, and responses were measured on a four-point ordinal scale.
Patients’ perceptions of the quality of care was evaluated using satisfaction scores. This satisfaction survey is widely used to determine the quality of healthcare. We used their questions and modified a few to align them with our study. A copy of their questionnaire and our study questionnaire is in the supplementary files.
Patient semi-structured interviews
PLHIV with or without one or more comorbidities, specifically DM or HT, were approached to participate in this study to determine satisfaction with care based on the experience of care they received. An interview schedule was developed for the qualitative interviews. The qualitative participant interviews followed the quantitative satisfaction survey. Interviews were audio-recorded and conducted in a private setting, with strict confidence standards applied by the PI and the interviewee at a place convenient for both the interviewer and interviewee. Interviews lasted up to 40 minutes. Semi-structured interviews were conducted over a month. Both the quantitative and qualitative data covered similar items relating to quality of care.
Validity and reliability
Quantitative study
The quantitative questionnaires were pretested and piloted. Consent forms were available for patients in isiZulu (translated by an approved translator). Fieldworkers were trained on data collection and the importance of confidentiality, and they signed a contract that included a clause not to divulge information.
Qualitative study
Qualitative in-depth interviews were audio-recorded and transcribed verbatim to ensure that the data generated was a true reflection of the participant. The data from the qualitative interviews was validated by having an independent researcher conduct inductive content analysis after the PI and the supervisor’s interpretation was completed. The PI is a Master’s graduate and conducted qualitative interviews as part of the Master’s dissertation. The independent researcher is a lecturer in industrial psychology and has several years of experience in qualitative interviews.
Data management
Quantitative study
The completed questionnaires were checked to ensure that almost all were fully answered. The information received was entered into a Microsoft Office 2016 spreadsheet. Data was then imported into the statistical software package (Stata Version 14) for data analysis.
Qualitative study
The in-depth interviews and focus group discussion were typed using Microsoft Word 2016 and password protected.
Data analysis strategies
Quantitative study
The participants were asked 42 questions (Supplemental File 4) that related to the experience of care that they received. An ordinal scale was used. Responses were coded as follows; 1 = never; 2 = sometimes; 3 = most times; 4 = always. 0 = n/a and 99 = unsure. Even though all questions were answered by the participants, the “0” and “99” entries were excluded from the analysis to determine sensible groupings and latent variables. To analyse quality of care, these items, q28–38 and 42–70, that is attached as Supplemental File 4, needed to be reduced so that they could be grouped together into groups that have ‘like’ items together to find latent variables. Before this analysis could be done, reverse coding was done for all the items that were worded such that higher frequency indicated worse quality of care. A higher score (higher frequency) for an item suggested that the quality of care was ‘good’. Responses such as ‘unsure’ were excluded so that there was an ordinal scale for this analysis. Reverse coding applied to the following items: 29, 33, 35, 37, 42, 44, 46, 47, 50, 51, 52, 54, 56, 57, 59, 60, 62, 66, 69 and 70. Items that were excluded from the analysis are highlighted in Supplemental File 1. Structure consisted of 6 items, process consisted of 14 items and outcome consisted of 7 items.
Ideally, one needs to have at least five points on an ordinal scale to apply methods like factor analysis (Supplemental File 6), which was carried out on the 4-point scale. Factor analysis was done to find appropriate groups and identify factors. Results from factor analysis were confirmed by performing a categorical Principal Component Analysis (PCA) analysis. The same groupings were found. Quantitative data underwent rigorous preprocessing, including reverse coding of items where higher frequencies indicated a worse quality of care. Items were grouped into themes of structure, process, and outcomes, guided by Donabedian’s healthcare quality framework. PCA with promax rotation was applied to 40 items to reduce the dataset and identify latent variables, with results validated through a categorical principal components analysis. Reliability was confirmed using Cronbach’s alpha, achieving a minimum threshold of 0.7, while sampling adequacy was assessed using the Kaiser-Meyer-Olkin measure and Bartlett’s test of sphericity.
During the PCA, some items were dropped either because they did not load strongly enough onto any factor or because they cross-loaded onto multiple factors. Repeated questions were dropped. The reliability of combining the items into a single latent variable is tested using Cronbach’s alpha. An alpha value of at least 0.7 is considered adequate. The factor extraction is deemed to be successful if the Kaiser-Meyer-Olkin Measure of Sampling Adequacy (KMO) exceeds 0.6 and Bartlett’s test of sphericity is significant. (Supplemental file 5).
Qualitative interviews
The audiotapes from the qualitative semi-structured interviews were transcribed verbatim onto Microsoft Word 2016 documents that were password protected. The transcripts were revisited to ensure nothing was missing, and the researchers listened to the interviews several times. The PI coded and categorised the data according to themes. Open coding was achieved by highlighting keywords and phrases from the transcripts, and common themes were found. 4 The last step was finding the themes and emergent concepts and re-coding the data to develop well-defined categories. Categories were combined for all transcripts. Triangulation with other data collection methods occurred (quantitative patient survey, direct observations, individual interviews, and consulting with staff to ensure clarity). Data were analysed to saturation until the same themes emerged, after which no further interviews were conducted. For qualitative data, deductive content analysis was performed. Transcripts were reviewed multiple times to ensure accuracy, and themes were derived through open coding, categorisation, and triangulation with survey data and direct observations. Themes were aligned with the structure, process, and outcomes domains of Donabedian’s model. Independent analysis by two researchers ensured credibility, while reflexive notes safeguarded against investigator bias.Data was collated after the transcripts were analysed independently by an external reviewer DS and the PI (AR), and supervisor (MN). We used the survey data and qualitative data to develop a comprehensive understanding of the phenomenon of interest under the Donabedian Framework.
Ethical considerations
The Biomedical Research Ethics Review Board at the University of KwaZulu-Natal (BREC 645/116) approved the study. The KwaZulu-Natal Department of Health and Wentworth Hospital also provided ethics and gatekeeper approval. All patients were assured of anonymity, and strict confidentiality was maintained throughout the study. Written informed consent was obtained from all participants. No incentives were used in this study. Participation was voluntary, and patients were informed they could withdraw during the study period.
Results
The quantitative and qualitative results from our study are reported below.
Socio-demographic characteristics of participants
Quantitative phase
Among the 301 patients from the satisfaction survey, 230 (76.41%) had HIV only (95% confidence interval [CI]: 71.25-80.89) and 71 (23.59%) had HIV and at least one comorbidity(95% CI: 19.11-28.75, namely DM and/or HT). Hypertension was the most prevalent comorbidity.
Qualitative phase
Six participants were female, while four were male. Four had HIV only, and two had HIV, DM, and HT; one had HIV and DM, while three had HIV and HT.
Quantitative data
Reliability of the latent variables to measure quality of care.

The above constructs depicted (Supplemental File 2) in the 22 items that were aligned to the Donabedian Framework are reported below under structure, process and outcome. The frequency analysis below was done for the survey responses. The process dimension had two constructs that fit into the Donabedian Framework.
Results show that medical care is available significantly often, while respondents indicate that personal interactions/satisfaction are significantly enjoyed. In contrast, general care conditions and the perceived competency of medical staff are both experienced significantly less often, as can be seen in Figure 1 below. Percentage of patients with HIV and HIV with comorbidities. AVAIL Better availability of medical care. GEN Better general care and conditions. DOC_NURS Better care/more perceived competence regarding doctors and nurses. PERS Better personal interactions and general satisfaction.
There was a moderate positive correlation between accessibility and personal care and satisfaction, rho =. 461, p<.001. Accessibility to care facilities (structure) is associated with good personal interactions (process) and general satisfaction (outcome).
Frequency analysis of responses of patients.

aPearson’s chi-square
bFisher’s exact
Reliability of the constructs aligned to the Donebedian framework.

In order to compare the two groups, we did a descriptive analysis showing the percentage in each group that rated these four constructs as either most times or always. We grouped the never and sometimes, and the most times and always.
Figure 1 above shows evidence that in this study, care between PLHIV only and PLHIV and comorbidity was the same across the constructs. Table 3 depicts the reliability of the chosen construct.
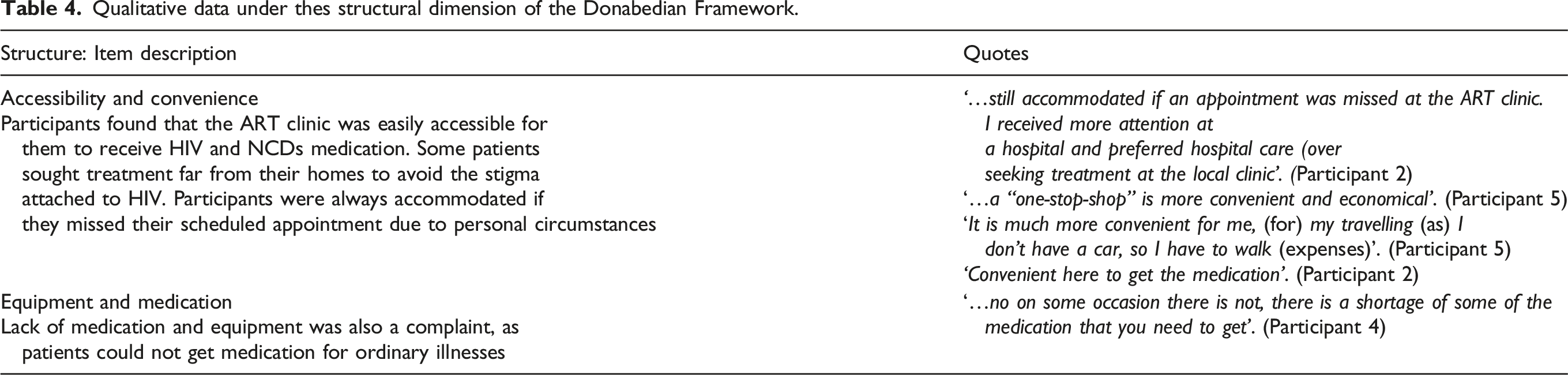
Qualitative data under thes structural dimension of the Donabedian Framework.
Qualitative data under the process dimension under the Donabedian Framework.

Qualitative data under the outcomes dimension under the Donabedian Framework.

Qualitative interviews
Structure
Process
Quality of care and alignment to structure, process and outcomes
The main themes that emerged were accessibility and convenience (fragmented vs integrated care), stigma, lack of medication and equipment, waiting times, staff attitudes, implementation of guidelines, self-efficacy, health literacy and adherence, and prioritisation of medication that influence patient satisfaction of care. The study findings are broadly depicted in Figure 2, which articulates the chosen conceptual framework and highlights how this impacts the quality of care. Summary of findings aligned to the Donabedian Framework.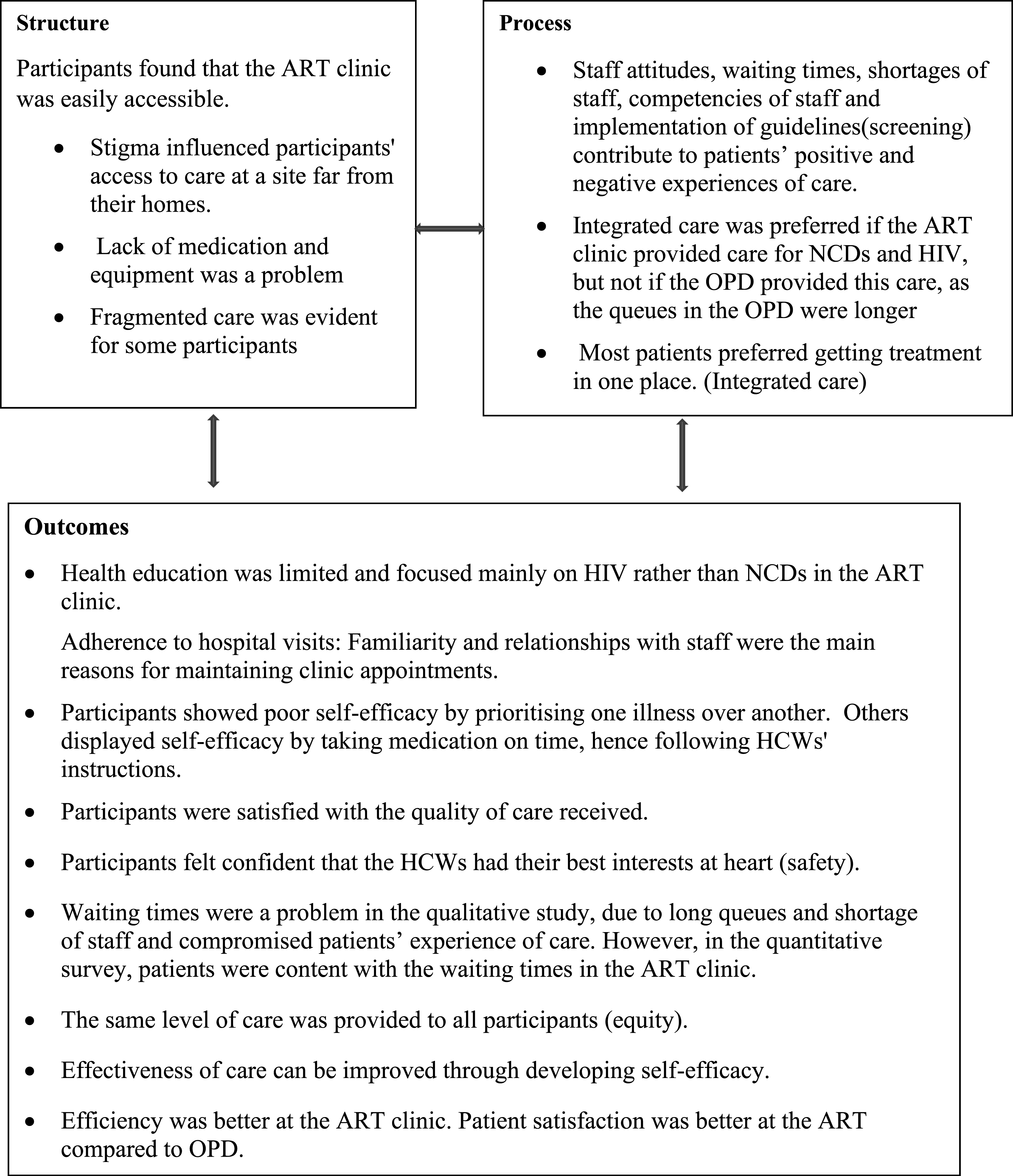
A summary of the results from the satisfaction score and qualitative surveys are presented in Figure 2 below.
Discussion
This mixed-method study, drawing insights from the experiences of individuals living with HIV and HT and/or DM, is a valuable contribution to the understanding of healthcare dynamics. The study employed the Donabedian Framework, a well-established tool for evaluating healthcare quality, which encompasses three crucial dimensions: structure, process, and outcome. The study discerned emergent themes within these dimensions, revealing a comprehensive understanding of the complex interplay of factors influencing patient experiences. A cross-sectional study was conducted as it was inexpensive and feasible in a busy ART clinic. Face-to-face interviews were conducted. Qualitative data were generated from the PLHIV-validated responses. The methodological approach was chosen for its cost-effectiveness and ability to provide a comprehensive understanding of care quality.
The trustworthiness of qualitative data was triangulated against that of quantitative data. Credibility was ensured through a process of constantly revisiting the data through critical listening. Confirmability was ensured through participant verification of the data and the interpretation. Transferability was achieved by ensuring the study was conceptually designed and applicable to similar settings in KwaZulu-Natal. Two researchers, AR and MN, independently analysed the qualitative data, discussed convergence and divergence areas, and settled on final themes through consensus. Trustworthiness was maintained through triangulation, participant verification, and collaborative analysis, ensuring credibility, transferability, and confirmability. The findings are conceptually relevant and transferable to similar healthcare settings in KwaZulu-Natal.
The key findings of this study were that participants were overall satisfied with the care they received, irrespective of their NCD status. Quantitative data revealed that patients were satisfied with the care they received. Patients also alluded to that in qualitative interviews. Accessibility to medical services was associated with good personal interactions, staff attitudes, familiarity, and general satisfaction (shorter waiting times and accessibility). There was a weak negative correlation between the availability of care facilities and the perceived competence of doctors/nurses. A lower availability of medical care (shortage of staff) is associated with a poorer perception of the competence of doctors/nurses. Waiting times, shortage of staff and budget constraints were major barriers to fully implementing integrated care. In the quantitative survey, patients were happy with the waiting times; however, qualitative interviews revealed that they were dissatisfied with the waiting times.
Accessibility to the antiretroviral therapy (ART) clinic was good in both the quantitative and qualitative phases. Fragmented and integrated care were evident in our study. This structural fragmentation led to conflicting information and communication gaps among clinicians, underscoring the importance of a unified system to ensure consistent and comprehensive care. 5 Stigma was reduced when care for HIV and NCDs was integrated. A minority of NCD clients, either with HT or DM, were unhappy with the model mainly because of structural challenges at the health facilities, which were too open, and consultation rooms were few and small, undermining confidentiality and privacy, in contrast to our study. 6 Studies highlighted the lack of equipment and medication as a barrier to integrated care.7,8 Space and shortage of medications were common challenges encountered during the integration of services.9,10
Resource constraints emerged as a significant barrier, emphasising the delicate balance required for successful implementation. This resonates with broader literature, acknowledging the challenges healthcare systems face in achieving seamless integration, especially in resource-constrained environments. 3 The structural elements not only influence the accessibility of services but also impact patient convenience and adherence to hospital visits. The study’s findings align with existing research, emphasising the pivotal role of the healthcare infrastructure in shaping patient perceptions and experiences. 4 The care offered at this hospital for PLHIV and NCDs was both integrated and fragmented.
The inconsistency in HIV screening in the outpatient department (OPD) revealed gaps in the implementation of guidelines. The study emphasised the need for consistent adherence to screening protocols, underlining the importance of systematic processes in ensuring early detection and management of diseases. 5 OPD and the antiretroviral therapy (ART) clinic require upskilled staff trained to manage both conditions. Robust health education should ensure that patients realise the need to know their HIV and NCD status. Not all patients will present with DM and HT, but either of these conditions interacts with HIV management. As PLHIV live and age with HIV, they also gain weight, increasing their risk of getting NCDs.(13).
Waiting times and staff shortages emerged as significant influencers of patient satisfaction. Prolonged waiting times were identified as a common barrier, impacting the quality of care. 6 The staff shortage, compounded by trainee doctors’ presence, contributed to a perception of suboptimal healthcare delivery. This aligns with broader literature highlighting the relationship between staffing levels, waiting times, and patient satisfaction.7,8 Long waiting times were a common complaint 9 impacting the quality of care, and were reduced during the integration of care.
Adherence to treatment varied between HIV and NCDs, with patients initially prioritising HIV treatment. The study acknowledged the complexities of patient behaviours and highlighted the need for ongoing counselling and health education to promote adherence to NCD treatments over time. Patient education on both NCDs and HIV emerged as a crucial aspect of the care process. The study highlighted that patients tend to prioritise treatment based on their awareness, demonstrating the need for comprehensive health education strategies to bridge information gaps and promote holistic healthcare. 3 The limited focus on health education in the respective clinics resulted in patients prioritising treatment for one condition. Health education is imperative to ensure participants adhere to treatment, reduce stigma, and prevent treatment interruption and prioritisation. Due to donor funding and a more explicit operational plan, patients tend to prioritise antiretroviral therapy (ART) over NCD treatment. 10 This finding correlates with better antiretroviral therapy (ART) adherence, resulting in a reduction in the viral load in the short term and better clinical outcomes. However, the outcomes of NCD medication may not be immediately apparent.
Travelling costs will be significantly reduced with integrated care, which may ensure positive outcomes such as adherence to treatment regimens 11 and lessening the burden on health systems. 5 Integrated care improves patient satisfaction with care and results in better patient outcomes.1,11 In Soweto, numerous separatist clinics led to patients receiving only pieces of information from clinicians because of poor inter-provider communication. 3
Strengths of the study
This study assessed the real-world performance of HIV clinical care and patient satisfaction in terms of the prevention and management of NCDs. This was the first study conducted in an urban district hospital in eThekwini, SA, highlighting the participants’ perception of quality of care among PLHIV and NCDs. The patients without NCDs were included in the quantitative and qualitative interviews to identify if there was a difference in the quality of care offered to them.
Limitations of the study
A limitation of the study was that we focused on HT and DM, and no other NCDs. Patients were hesitant to participate in the qualitative interviews but were more amenable to the quantitative questionnaire. The study was done on a small population and needs to be replicated on a larger scale. We did not have the same number of patients with HIV and comorbidities; however, the number was sufficient to make inferences. ‘Measurement invariance across groups (individuals with and without NCDs) could not be formally tested due to insufficient sampling adequacy in one group (KMO = .378), which rendered the data unsuitable for factor analysis. As a result, we were unable to confirm whether the same factor structure applied across groups. This limits the interpretability of any direct comparisons between the groups.'
Conclusions
The findings contribute valuable insights to the broader discourse on healthcare quality, emphasising the need for a holistic understanding of the interplay between structure, process, and outcomes. The recommendations, which include staff upskilling, comprehensive health education, and further research on patient outcomes, provide a roadmap for policymakers and healthcare providers to enhance the quality of care in resource-constrained environments. The call for future studies to explore diverse settings and populations aligns with the ongoing efforts to achieve patient-centred, integrated care on a global scale for PLHIV and NCDs.
Supplemental Material
Supplemental Material - Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal
Supplemental Material for Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal by Althea Rajagopaul, Mergan Naidoo in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal
Supplemental Material for Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal by Althea Rajagopaul, Mergan Naidoo in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal
Supplemental Material for Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal by Althea Rajagopaul, Mergan Naidoo in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal
Supplemental Material for Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal by Althea Rajagopaul, Mergan Naidoo in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal
Supplemental Material for Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal by Althea Rajagopaul, Mergan Naidoo in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal
Supplemental Material for Patient perceptions of quality of care rendered for HIV and non-communicable diseases at an urban district hospital in KwaZulu-Natal by Althea Rajagopaul, Mergan Naidoo in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
The authors would like to thank Mrs. D. Ackerman, who reviewed the qualitative data independently and concurrently with the authors. Thank you to all the study participants.
Ethics approval
The Biomedical Research Ethics Review Board at the University of KwaZulu-Natal (BREC 645/116) approved the study. The KZN Department of Health and Wentworth Hospital also provided ethics and gatekeeper approval.
Consent to participate
Patients signed a form of informed consent to participate.
Author contributions
AR conducted this study for the Doctor of Philosophy in Family Medicine degree under the supervision of MN. AR was responsible for conceptualising the study, collecting, and analysing data and writing the final report. MN assisted with the approval of the final version.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors AR and MN declare that they have no competing interests.
Data Availability Statement
The data sets generated and/or analysed during the current study are not publicly available due to the confidentiality of patient responses but are available from the corresponding author on reasonable request or via the university’s Biomedical Ethics and Research Committee.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.