
Abstract
Background:
People living with human immunodeficiency virus (HIV) are facing an increased burden of noncommunicable diseases (NCDs) comorbidity. There is, however, paucity of information on the magnitude of HIV-NCDs comorbidity, its associated factors, and how the health system is responding to the double burden in Ethiopia.
Objective:
To determine the magnitude of comorbidity between HIV and hypertension or diabetes and associated factors among HIV-positive adults receiving antiretroviral therapy (ART) in Bahir Dar city, Ethiopia.
Methods:
A facility-based cross-sectional study was conducted among 560 randomly selected HIV-positive adults taking ART. Data were collected using a structured questionnaire and analyzed using SPSS version 23. Descriptive statistics were used to describe the data. A logistic regression model was fit to identify associated factors with comorbidity of HIV and NCDs.
Results:
The magnitude of comorbidity was 19.6% (95% confidence interval (CI): 16.0–23.0). Being older (55 and above years) adjusted odds ratio (AOR: 8.5; 95% CI: 3.2–15.1), taking second-line ART regimen containing tenofovir (AOR: 2.7; 95% CI: 1.3–5.6), and increased body mass index (BMI) ≥25 (AOR: 2.7; 95% CI: 1.2–6.5) were the factors associated with comorbidity. Participants reported that they were not managed in an integrated and coordinated manner.
Conclusions:
The magnitude of comorbidity among adults was high in the study area. Being older, second-line ART regimen and high BMI ≥25 increased the odds of having NCDs among HIV-positive adults. Targeted screening for the incidences of NCDs, addressing modifiable risk factors, and providing integrated care would help to improve the quality of life comorbid patients.
Background
Noncommunicable diseases (NCDs) refer to a complex and heterogeneous group of diseases mainly cardiovascular disease (hypertension and stroke), diabetes mellitus (DM), renal diseases, mental illness, chronic respiratory diseases, and cancer. 1 These diseases are rapidly emerging and increasing in developing countries, where communicable diseases also remain the major public health challenges. 2
World Health Organization’s (WHO’s) projections show that NCDs will be responsible for a significantly increased total number of deaths in the next decade. Deaths due to NCDs are projected to increase by 15% globally. The greatest increases will be in the Africa region, as the rapidly urbanizing poorer population became more susceptible to comorbidity and its adverse outcomes. NCDs are predicted to overtake the burden of mortality and morbidity from communicable diseases by the year 2030. 3
Access to antiretroviral therapy (ART) has resulted in increasing survival for people living with human immunodeficiency virus (HIV). 4,5 With the longer life spans that ART has made possible, a larger number of people living with HIV are facing the increased burden of NCDs. 6
The epidemiologic overlap between NCDs and HIV and the impact of NCDs-HIV comorbidity in sub-Saharan Africa, including Ethiopia, are likely to be very large. 4,7
Patients living with HIV share many common risk factors of NCDs. These mainly include unhealthy diets (high intake of fat, salt, and refined sugars), physical inactivity, tobacco use, and harmful use of alcohol. 8 Moreover, evidence on the causal underlying mechanisms revealed that there is a complex interaction among HIV infection, ART, and NCDs risk factors. NCDs in HIV-positive people are occurring due to a mix of chronic immune activation, medication side effects, coinfections, and the aging process itself and they may get worsened by HIV and some antiretroviral drugs. 9
Comorbidity results in a very complex disease pattern that could have additive or multiplicative consequences on health outcomes. 10 NCDs are the major cause of death in people living with HIV/aquired immunodeficiency syndrome and cardiovascular diseases account for 46% of the total deaths. 5 There is a huge concern that the survival and aging possibility of patient on ART could have severely hampered by the rapidly evolving and emerging NCDs among this group of population. Both HIV and NCDs need chronic care for long follow-up, revisits, referrals, counseling, social support systems, and collaborative actions. 11
Studies on the prevalence of isolated cases of chronic NCDs are flourishing in Ethiopia. However, there is sparse evidence on the magnitude of HIV-NCD comorbidity, associated factors, and how the health system is responding to this high need patient group.
This emerging double burden of disease challenges sub-Saharan’s African health infrastructure and demands an effective response while recognizing the context of scarce resources within the region. 12 The attention given to this wave of fatal epidemic looks suboptimal, perhaps not available in poor resource countries like Ethiopia. 13,14
The impact of HIV-NCDs comorbidity at the health system level is recognized globally. 13,14 The management of HIV-NCDs comorbidity is much more complicated and demanding for the health system, patients, and their families compared to those without. 15 However, the current model of care and guidelines, developed at a time when single disease frameworks were predominant, tend to focus on diseases in isolation rather than the needs and circumstances of the person with complexity care needs. 16
The absence of a strong generalist and integrated care may lead to poor quality of care and patient outcome. 17 Understanding the burden of HIV and the commonest NCDs comorbidity, identifying modifiable factors, and exploring how well the health system is responding to this colliding epidemic have a paramount importance 9 to design and strengthen the existing prevention and management strategies. Therefore, the objective of the study was to determine the magnitude of HIV-hypertension and diabetes comorbidity and identify associated factors and figure out how the current health-care system is responding to the problem among HIV-positive adults attending ART follow-up at public health facilities of Bahir Dar city, Amhara region, Ethiopia.
Methods
Study design, area, and period
A facility-based cross-sectional study was employed to determine the magnitude of HIV-hypertension and diabetes comorbidity and identify associated factors among adults attending follow-up in ART clinic at public health facilities of Bahir Dar city. The data were collected from March 1 to 31, 2018, during clinic visits.
The study was conducted in Bahir Dar city, the capital of the Amhara region. The city has a total population of 314,007. 18 It has 2 public hospitals, 10 health centers, 10 health posts, 1 private hospital, and 45 private clinics. These facilities are serving about five million populations living in the city and surrounding districts. Among all the health facilities in the city, 2 public hospitals and 5 health centers had ART clinic and about 11,259 patients were on ART at the time of the study.
Source population and inclusion criteria
All HIV-positive adults attending follow-up in the ART clinic at public health facilities of Bahir Dar city administration were the source population. Adults with HIV positive whose age is 18 years and above and on ART for at least 6 months were included in the study.
Study variables
Presence or absence of comorbidity of hypertension and diabetes in HIV patients was the outcome variable. Sociodemographic variables (age, sex, residency, education level, occupation, marital status, monthly income (Birr), and family history of NCDs), lifestyle variables (tobacco use, alcohol consumption, and physical exercise), clinical feature variables (parameters WHO HIV disease clinical stage, ART drug class exposure, and duration of exposure), and biomedical measurements (cluster differentiation 4+ (CD4+) cell count, viral load, body mass index (BMI), blood pressure (BP), and blood glucose level) were the independent variables.
Operational definitions
HIV-NCD comorbidity refers to the occurrence of at least one chronic NCD (hypertension and/or DM) in HIV-positive patients. As ascertaining the accuracy of the diagnosis of other chronic diseases was difficult during the study period, we limited the number and kinds of NCDs to be considered for the definition of comorbidity in this study. Hence, we decided to only include hypertension and diabetes.
Hypertension
For the purpose of this study, hypertension was defined as systolic BP ≥140 mmHg and/or diastolic BP ≥90 mmHg or currently taking medication for hypertension. 19
DM was defined as random blood sugar >11.1 mmol/L (200 mg/dL) or fasting blood sugar ≥7 mmol/L (126 mg/dL) or being on diabetes medication. 20
Physical exercise
It was defined as having high = vigorous activity for at least 3 days per week each lasting 30 min or more. Moderate = vigorous activity for 3 days per week each lasting 20 min or 5 days of walking for at least 30 min per day. Low = any activity less than those categories mentioned above. 21
Anthropometric measurements
Weighing carried out without shoes and light indoor clothing using the calibrated digital weighing scale recorded to the nearest 0.1 kg (100 g). A body meter (measured up to 2 m) used to measure the height of respondents. The respondents were barefooted and stood on a flat surface with their back on the tape attached to the wall recorded to the nearest 0.1 cm. All anthropometric measurements of weight and height performed twice separately and then the average of the two readings recorded. 19
BMI was obtained by dividing weight in kilograms by height in meters squared (weight (kg)/height (m2)). Cutoff levels by WHO as underweight <18.5 kg/m2, normal 18.5–24.9 kg/m2, overweight 25–29.9 kg/m2, and obese
Employed: a person who had a permanent job with a monthly salary whereas daily laborer: a person who does not have a permanent job, but earns money by doing labor works daily.
Sample size and sampling method
The sample size was determined using single population proportion formula by considering the following assumptions: prevalence of hypertension in the previous study (p = 33%) m, 22 marginal error (w = 5%), and 95% confidence interval (CI) (Zα /2 = 1.96), design effect of 1.5, and 10% nonrespondent rate. The final sample size required was 560. Since using the hypertension prevalence yielded the maximum sample size, we decided to use that.
There were two hospitals and five health centers that provide ART services in the study area at the time of the study. First, stratification was done by type of health facilities (hospitals and health centers). One hospital and two health centers were selected using simple random sampling. Proportion to size allocation was made to determine the required sample size from the hospital and health centers. Finally, a simple random sampling technique was used to select study participants using registration records of patients as a sampling frame.
Data collection tools
A structured questionnaire was developed and used to conduct face to face interviews and capture relevant data from the patients and their records. The questionnaire was initially prepared in English and translated to Amharic for collecting the required information, such as sociodemographic characteristics, associated factors, and clinical parameters (Online Supplement 1).
Pretest of the instrument was conducted to check its appropriateness and ensure consistency of understanding for administration. Data were collected by five trained ART nurses and two public health supervisors. Data quality was assured by providing a 1-day training on the objectives of study, how to obtain consent, and on the data collection process and confidentiality. Completed questionnaires were cross-checked daily for consistencies and completeness.
Data management and analysis
Data were entered using Epi Info version 7 software and exported to SPSS version 23 for analysis. Descriptive statistics were run to describe data. Binary logistic regression models were fit to identify predictors of comorbidity of NCD and HIV. The variables whose p value <0.05 in the binary analysis were considered for multivariable logistic regression. Adjusted odds ratio (AOR) with 95% CI was calculated to show the strength of association and to control for the effects of confounding. A p value <0.05 was considered statistically significant to identify predictors of comorbidity.
Ethical considerations
Ethical clearance was obtained from the College of Medicine and Health Sciences, Bahir Dar University. Formal letter was given to Amhara Regional Health Bureau and health facilities. Informed verbal consent was obtained from each study participant after briefing the objective of the study. Data were recorded anonymously to assure the confidentiality of the data. Individuals diagnosed to have a new incidence of hypertension or diabetes or both were referred to seek further care.
Results
Sociodemographic characteristics of study participants
In this study, 547 participants were enrolled with a response rate of 97.7%. Due to a shortage of time, 13 (2.3%) patients refused to participate in the study. Study participants were predominantly females 341 (62.3%). The mean (±standard deviation) age of the study participants was 39.3 (±9.6) years; 41.8 (±8.9) years for males and 37.8 (±9.6) years for females. Over one-third of the study participants (35%) had completed primary education. More than one-fourth of the study participants (28.3%) were daily laborers. More than half of the study participants (56.7%) were married and 40.8% of them had a monthly income per household less than 1000 Ethiopian Birr (Table 1).
Sociodemographic characteristics of study participants among adults attending ART follow-up in public health facilities of Bahir Dar city, 2018.

ART: antiretroviral therapy; SD: standard deviation.
Lifestyle and behavioral characteristics of study participants
About 112 (20.5%) patients had a BMI less than 18.5 (underweight), 338 (61.8%) were in the normal range, and 97 (17.7%) were having BMI 25 and more (overweight or obese). With regard to lifestyle and behavioral characteristics, a relatively higher proportion of the participants had history of alcohol intake and the proportion of people who smoke cigarette was the lowest among the list (Figure 1).

Behavioral characteristics of study participants among adults attending ART follow-up in public health facilities of Bahir Dar city, 2018. ART: antiretroviral therapy.
Clinical parameters of the participants
Among study participants, 64% (350) had CD4+ cell count greater than 350 cells/mL and 95.4% (522) of participants were put on treatment stage I. Viral load was undetectable in 510 (93.2%) participants and only 2.9% of patients had a detectable viral load greater than 10,000 copes/mL. In terms of duration on ART, approximately 71.3% (400) of the study participants took ART for over 5 years and 19.4% had been on treatment for the last 10 years or more at the time of data collection. Tenofovir (TDF)-containing regimens were mostly prescribed (45.5%) followed by zidovudine (AZT)-based regimen (43.1%) and second-line drug regimen were the least (11.3%) prescribed.
Magnitude of HIV-NCDs comorbidity
The prevalence of NCDs (hypertension and/or DM) among adults attending ART follow-up was 19.6% (95% CI: 16–23). Of these, 14.1% (95% CI: 11–17) of them had hypertension and 8.6% (95% CI: 6–11) had DM (Table 2).
Prevalence of NCDs (hypertension and DM) among adults attending ART follow-up in public health facilities of Bahir Dar city, 2018.

NCD: noncommunicable disease; DM: diabetes mellitus; ART: antiretroviral therapy; CI: confidence interval; HIV: human immunodeficiency virus.
NCDs and HIV service delivery
When asked about the time of NCDs diagnosis, 74 (96.1%) of hypertensive and 43 (91.5%) of diabetic patients reported that the diagnosis of their chronic conditions was made after the initiation of ART either in other units or other health facilities, but not within the ART unit. The study found that patients do not receive health care for NCDs in the ART clinic. In terms of the place of follow-up for NCDs, 86 (81.1%) had follow-up in the same health facility but at a different unit and 20 (18.9%) had follow-up from other health facilities including private clinics.
Factors associated with HIV-NCD comorbidity
Being older, taking second-line ART regimens containing TDF, and a BMI value of 18.5 and above were the factors significantly associated with HIV-NCDs comorbidity (Table 3).
Factors associated with HIV-NCDs comorbidity among adults living with HIV in Bahir Dar city, 2018.

HIV: human immunodeficiency virus; NCD: noncommunicable disease; HTN: hypertension; DM: diabetes mellitus; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; ART: antiretroviral therapy; 3TC: lamivudine; Efv: Efavirenz; CD4+: cluster differentiation 4+; BMI: body mass index; TDF: tenofovir; AZT: zidovudine.
a p < 0.05.
b p < 0.01.
c Dropped in the final model.
Compared to the age group between 18 years and 34 years, the odds of having HIV-NCDs comorbidity was two times and eight times higher in the age group between 35 years and 54 years (AOR 2.37; 95% CI: 1.19–4.79) and 55+ years (AOR 8.45; 95% CI: 3.16–15.07), respectively. The odds of having HIV-NCDs comorbidity was 2.7 times higher among participants who took second-line ART drug regimens containing TDF (AOR 2.73; 95% CI: 1.33–5.63) compared with that of AZT-containing regimens. Compared to those having BMI less than 18.5, the odds of having NCDs comorbidity was 2.3 (AOR 2.32; 95% CI: 1.09–4.93) times and 2.7 (AOR 2.74; 95% CI: 1.16–6.49) times higher among those having BMI 18.5–24.9 and BMI greater than or equals 25, respectively (Table 3).
HIV-hypertension comorbidity
Old age and BMI of 25 or more were the factors significantly associated with HIV-hypertension comorbidity. However, unlike HIV-diabetes comorbidity, taking ART regimens containing TDF was negatively associated with HIV-hypertension comorbidity (Table 4).
Factors associated with HIV-hypertension comorbidity among adults living with HIV in Bahir Dar city, 2018.

HIV: human immunodeficiency virus; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; ART: antiretroviral therapy; CD4+: cluster differentiation 4+; BMI: body mass index; TDF: tenofovir; AZT: zidovudine.
a p < 0.05.
b p < 0.01.
The odds of having hypertension was 4.2 times and 6.8 times higher among in the age group between 35 years and 54 years (AOR 4.24; 95% CI: 1.72–10.45) and 55+ years (AOR 6.79; 95% CI: 1.94–15.12), respectively, compared to the age between 18 years and 34 years. The odds of having hypertension among patients having BMI 18.5–24.9 (AOR 2.49; 95% CI: 1.01–6.15) and greater than or equals 25 (AOR 4.27; 95% CI: 1.55–8.75) were 2.5 and 4.2 times higher, respectively, compared to those participants having a BMI less than 18.5. The odds of having hypertension was significantly lower among participants who took ART-drug-regimen-containing TDF (AOR 0.53; 95% CI: 0.29–0.95) and second-line ART drug regimens containing TDF (AOR 0.20; 95% CI: 0.06–0.65) compared to that of AZT-containing regimens (Table 4).
HIV-DM comorbidity
Similarly, old age, higher BMI index, and long duration on ART were the factors significantly associated with HIV-DM comorbidity. However, unlike HIV-hypertension comorbidity ART regimens containing TDF increased the risk of HIV-diabetes comorbidity (Table 5).
Factors associated with HIV-DM comorbidity among adults living with HIV in Bahir Dar city, 2018.
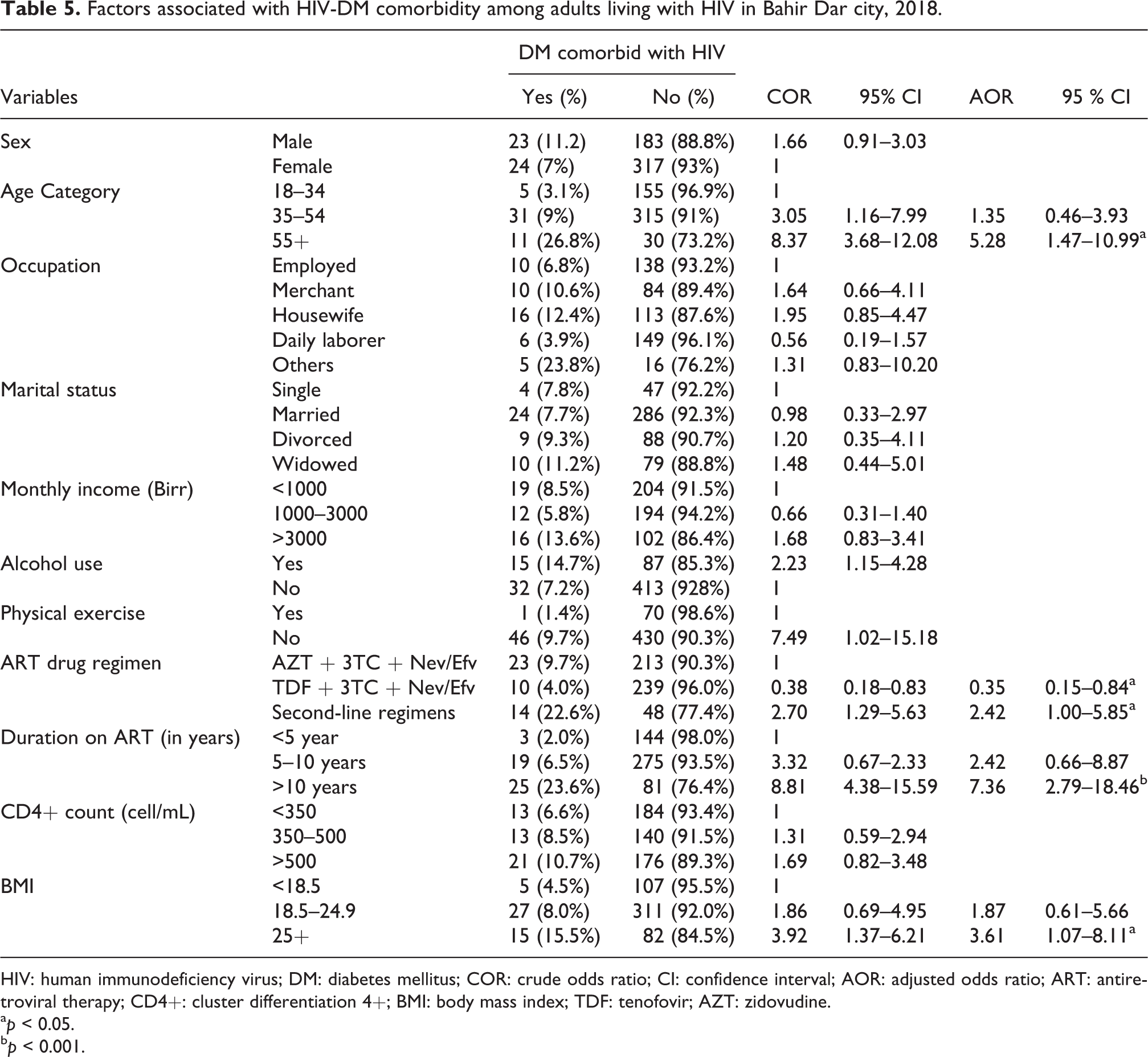
HIV: human immunodeficiency virus; DM: diabetes mellitus; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; ART: antiretroviral therapy; CD4+: cluster differentiation 4+; BMI: body mass index; TDF: tenofovir; AZT: zidovudine.
a p < 0.05.
b p < 0.001.
The odds of having DM among older patients aged 55+ (AOR 5.28; 95% CI: 1.47–10.99) was 5.3 times higher compared to the age between 18 years and 34 years. Moreover, the odds of having DM among those having BMI greater than or equals 25 (AOR 3.61; 95% CI: 1.07–8.11) were 3.6 times higher compared to those having BMI less than 18.5. The odds of having DM was significantly lower among participants who took TDF-containing first-line ART (AOR 0.35; 95% CI: 0.15–0.84), but it was higher among those who took second-line ART (AOR 2.42; 95% CI: 1.00–5.85). The odds of having DM among those who have taken ART for more than 10 years was 7 times (AOR 7.36; 95% CI: 2.79–8.46) higher compared to those who have been on ART for less than 5 years (Table 5).
Discussion
The magnitude of HIV-hypertension and HIV-diabetes comorbidity was high. Advanced age, type of ART regimen, and high BMI increased the odds of having NCDs among HIV-positive adults. The study also revealed that HIV patients with coexisting chronic NCDs were being managed in isolated and fragmented fashion.
NCDs comorbidity is emerging problems in developing populations, including those living with HIV due to improving life expectance and other factors. 23 Management of HIV-NCDs comorbidity is much more complicated and demanding for the already resource-constrained health systems. 24 Not only living with HIV, but also taking ART drugs is related to the incidences of HIV-NCDs comorbidity. 25
In this study, the magnitude of NCDs (hypertension and/or DM, 19.6% (95% CI: 16–23)) among adult patients on ART follow-up was high. The magnitude of this study is consistent with other studies done in Zimbabwe (19.6% with 95% CI: 17.3–22.2) 26 and South Africa (22.6% with 95% CI: 22.1–23.1). 8 Hypertension and DM are a growing problem in HIV-infected adults and are the leading risk factors for mortality. 25 There is evidence that the prevalence of hypertension and elevated blood glucose levels in the African population was high, 27,28 showing an increasing trend. The increasing trend of these diseases and other NCDs is due to adverse environmental conditions, increasing urbanization, and lifestyle changes in the urban setting of developing countries. 24 The prevalence of hypertension in our study was 14.1%. Prevalence rates in the general population in Ethiopia have been reported as between 16% 29 and 19.6%. 30 The prevalence of hypertension in patients on ART has been reported as 17.1% 13 in other studies. In light of this, our findings show a lower prevalence of hypertension as compared to the rate in the general population and among patients taking ART in the region. It was, however, consistent with other similar studies conducted in Ethiopia, 31 Kenya, 32 and other African countries. 7,22 The result is also consistent with global studies in general. 33 The possible explanation of having an increased prevalence of hypertension in HIV-infected adults could be due to chronic inflammatory and immune reconstitution syndromes caused by ART drugs 34,35 and the relation between HIV-specific factors and ART 25 rather than a direct effect of HIV drugs on BP.
This study revealed that the magnitude of DM was 8.6% (95% CI: 6–11) which is consistent with the study done conducted in HIV-infected adults in eastern Ethiopia, 31 Cambodia, 36 and Canada. 37 However, this result is higher than the national prevalence of DM (3.8%) in the general population reported by WHO in 2016 28 and the total prevalence of DM in Ethiopian adult population (20–79 years; 5–6%) as reported by International Diabetes Federation in 2017. 38 Therefore, the study has a high prevalence of DM in HIV-positive patients compared to the general population of Ethiopia. This could be due to HIV- and ART-related factors. It is known that people with HIV have an increased risk of developing a number of serious health problems due to a compromised immune system and the changes in metabolic derangements. Moreover, some ART drugs such as protease inhibitors have diabetogenic effects. Evidences documented that being HIV positive and exposure to ART were found to be the factors associated with diabetes. 31,39 –41
Studies revealed that the risk of NCD has considerably increased as age increases. 42,43 Being older, obesity, long duration of ART, and type of ART regimen were found to be predictors of HIV-NCD comorbidity in the present study. Different studies reported that the prevalence of NCD increased when age increases. For instance, studies reported that alterations in glucose tolerance were more prevalent among patients who were older age. 44,45 Obesity was also one of the modifiable predictors of HIV-NCD comorbidity in this study which is supported by other studies. 46,47 The fact that obese individuals have altered metabolic processes, follow sedentary lifestyle, or affected by some ART drugs, there is a tendency that they would develop hypertension or diabetes or both.
ART drug exposure and duration of exposure were associated with comorbidity in the present study. Duration of exposure to ART drug for more than 10 years was associated with increased DM comorbidity which is consistent with other studies. 48,49 Overall, the study participants had considerable ART experience with more than two-third of the participants having been on treatment for at least 5 years and near one-fourth for 10 years or more. As patients stay longer, the probability of having NCD increases as their age increases. In this study, even though second-line ART drug regimens were least the prescribed drug, it was one of the associated factors with all NCDs and DM comorbidity. However, it was 80% less likely to develop hypertension comorbidity. The relationship between ART and the development of hypertension remains controversial. Studies conducted in Norway and Spain showed that the longer patients took highly active antiretroviral therapy, the more likely that they will develop hypertension. 32,50 This may be due to numerous underlying physiological changes that occur due to aging or the effect of antiretroviral drugs on the development of risk of chronic diseases, including hypertension and diabetes. 13
The United Nations’ Sustainable Development Goal 3 requires countries to move toward ensuring that all people and communities have access to health services that are of high quality, integrated, and people-centered. 51,52 Both HIV and noncommunicable require regular appointments, medication adherence support, side-effect management, laboratory monitoring, defaulter tracing as well as screening and education. In Ethiopia, health services are organized around single conditions and hospital doctors who specialize in one condition or area of the body often manage patients with one condition in mind, although many people, especially as they get older, will end up with more than one diagnosed condition. Patients with several conditions will have to visit different specialists at different times and may be in different settings. General practitioners and other clinicians are oriented with a system of employing the conventional one-size-for-all chronic care guidelines in fragmented and siloed fashion. 53,54 Also this study revealed that the health system is poorly configured to diagnose NCDs among HIV-positive people and service delivery was not integrated to respond to the needs of HIV-positive individuals comorbid with NCDs. This may result in the provision of fragmented care that does not take account of the impact of comorbidity on a person’s quality of life and their priorities, ultimately leading to negative health outcomes, including mortality. 55
The study measured the prevalence of common NCDs (hypertension and DM) and associated factors in HIV patients. This study advances the state of knowledge of comorbidity prevalence and strength of the health system in responding to the evolving needs of comorbid individuals. To the best of our knowledge, this study is the first ever attempt pursued to explore the existing health service landscape for HIV-NCDs comorbid population groups.
The findings provide valuable information that can be used to improve HIV care through medical evaluation to detect and manage these diseases. This study has some limitations. Due to the lack of feasible methods of assessing other NCDs, we only ascertained the two most commonly reported NCDs (hypertension and diabetes) in the country and this might have underestimated the burden of HIV-NCDs comorbidity in the study area. A cross-sectional design does not establish temporal relationships between explanatory variables and outcome variable, so the observed associations might not necessarily be causal and the results may not represent the statuses in the general population in Ethiopia
Conclusions
The magnitude of HIV-hypertension and/or HIV-diabetes comorbidity was high in the study area. Being older (age 55+), taking second-line ART drug regimens, taking ART for a long duration (10 years or more), and obesity (BMI ≥ 25) increased the odds of having NCDs in HIV-positive adults. This study also revealed that people living with HIV-NCDs comorbidity did not get integrated health care and treatment service of NCDs in ART clinics.
We, therefore, recommended that HIV patients should be screened for coexisting NCDs. Addressing modifiable factors such as obesity through counseling on dietary intake and weight management and providing an integrated person-centered care would help to improve the quality of life and longevity of patients on ART. Further studies are needed on the effect of TDF containing ART regiment, including second-line ART regimens on HIV-NCDs comorbidity.
Supplemental material
Supplemental Material, STROBE_checklist_cross-sectional - Comorbidity of HIV, hypertension, and diabetes and associated factors among people receiving antiretroviral therapy in Bahir Dar city, Ethiopia
Supplemental Material, STROBE_checklist_cross-sectional for Comorbidity of HIV, hypertension, and diabetes and associated factors among people receiving antiretroviral therapy in Bahir Dar city, Ethiopia by Zenebework Getahun, Muluken Azage, Taye Abuhay and Fantu Abebe in Journal of Comorbidity
Supplemental material
Supplemental Material, Suplement_file_1_Questionnaire - Comorbidity of HIV, hypertension, and diabetes and associated factors among people receiving antiretroviral therapy in Bahir Dar city, Ethiopia
Supplemental Material, Suplement_file_1_Questionnaire for Comorbidity of HIV, hypertension, and diabetes and associated factors among people receiving antiretroviral therapy in Bahir Dar city, Ethiopia by Zenebework Getahun, Muluken Azage, Taye Abuhay and Fantu Abebe in Journal of Comorbidity
Footnotes
Acknowledgments
The authors want to thank Bahir Dar University for funding to cover the cost of data collection. We also extend our acknowledgment to Amhara Regional Health Bureau, Felege Hiwot referral hospital, Bahir Dar health center, Han health center, and staff working in ART clinic for their cooperation and support for data collection. We would like to thank supervisors and data collectors for their commitment and management of data collection and participants for their consent to participate and provision of information for the study.
Author contributions
ZG designed the study and oversaw its implementation, performed the analysis, was the primary author, and approved the final version of the manuscript. TA and MA contributed to the concept of the study, oversaw its implementation, helped guide the analysis, participated in the writing, and approved the final version of the manuscript. FA involved in designing the concept of the study and data analysis, participated in the development of the manuscript, and approved the final version of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: There was no fund secured for the study, but Bahir Dar University covered the expense related to data collection.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.