
Abstract
Background & Objective
Benign paroxysmal positional vertigo (BPPV) is a leading cause of vertigo and has been loosely associated with osteoporosis, vitamin D deficiency, and broader metabolic dysfunction. Emerging evidence suggests that BPPV may relate to systemic conditions beyond the vestibular system. However, limited research has explored whether individuals with BPPV have increased rates of hypothyroidism, diabetes mellitus (DM), hypertension (HTN), or osteoporosis. The objective of this study was to examine the association between BPPV and hypothyroidism, diabetes mellitus (DM), hypertension (HTN), and osteoporosis.
Study Design & Setting
This study was a retrospective case-control study using patient records from a vestibular outpatient rehabilitation clinic in Florida, USA.
Patients & Outcomes
Adults diagnosed with BPPV over a six-month period were included in the study. Control data was derived from the National Center for Health Statistics (NCHS). Binomial logistic regression was performed to calculate odds ratios (ORs).
Results
A total of 140 individuals diagnosed with BPPV (98 female, 42 male) were analyzed. Patients with BPPV demonstrated statistically significant higher odds of hypothyroidism (OR 2.635, 95% CI 1.260–5.51) and diabetes mellitus (OR 2.28, 95% CI 1.09–4.76) compared to national estimates. No significant associations were found for hypertension or osteoporosis.
Conclusion
An association exists between BPPV and both hypothyroidism and diabetes mellitus. These findings support the role of systemic metabolic and endocrine dysfunction in the pathophysiology of BPPV and highlight the potential clinical value of screening for relevant comorbidities. Further research is warranted.
Introduction
Vertigo is a neurological condition that causes a false perception of motion, leading to sensations of dizziness. Benign paroxysmal positional vertigo (BPPV) is the most common cause of peripheral vertigo, occurring when gravity-sensitive calcium carbonate and protein-derived otoconia become dislodged from the utricle’s macula. 1 These free-floating otoconia travel through the endolymph of the semicircular canals, causing sensations of non-physiological angular acceleration with positional head changes. 1 While calcium and vitamin D are essential for healthy otolith function, the exact cause of idiopathic otoconia detachment remains largely unknown.2–5 However, underlying pathologies that disrupt nutrient homeostasis may increase a patient’s risk for this benign but often debilitating condition.
BPPV is most common in older adults and has an estimated lifetime prevalence of 2.4%, though some studies report even higher rates among females. 6 Its episodic nature coupled with the potential for recurrence contributes to substantial healthcare burden, particularly in outpatient and emergency settings. In addition to the transient vertigo, BPPV can also lead to persistent unsteadiness, increased fall risk, and functional limitations that impact quality of life, especially in older populations.7–9 Furthermore, deficits in spinal mobility and tolerance to transitional mobility limit a patient’s tolerance to positional maneuvers necessary to identify and treat BPPV. These complications may be further compounded by systemic medical conditions that alter vestibular compensation or increase otoconial instability.
Several studies have identified positive associations between BPPV and medical conditions, including post-menopause, osteoporosis, decreased bone mineral density (BMD), vitamin D deficiency, calcium deficiency, genetics, increased uric acid levels, hypertension, hypercholesterolemia, Ménière’s disease, and hyperparathyroidism.10–13 Additionally, recurrent BPPV episodes have been linked to conditions such as head trauma, migraine, advanced age, female sex, hypertension, diabetes mellitus (DM), hyperlipidemia, osteoporosis, vascular diseases, and vitamin D deficiency.12,14–17 Similarly, vascular comorbidities such as hypertension (HTN) may significantly contribute to BPPV recurrence, disease duration, and severity.18,19
Research continues to explore the association between BPPV and medical comorbidities, however, limited data exist regarding its relationship with thyroid dysfunction. A few studies have reported positive associations between BPPV and thyroid dysfunctions such as goiter, hypothyroidism, thyroiditis, hyperthyroidism, and hyperparathyroidism.20,21 A recent systematic review did not find a general association between BPPV and hypothyroidism but did identify a significant relationship between BPPV and Hashimoto’s thyroiditis. 22 Similar studies have not found a link and propose that other common comorbidities better explain the observed associations. 23 Regarding BPPV recurrence, multiple studies have reported that anti-thyroid autoantibodies are associated with increased recurrence, indicating that autoimmune mechanisms may play a role.15,24,25 Collectively, current literature indicates that the association between BPPV and thyroid dysfunction is not well understood but likely exists.
Given the episodic nature of BPPV and the growing recognition that systemic factors may influence its onset or recurrence, there is increasing interest in identifying comorbidities that may contribute to its pathogenesis. However, the extent to which individuals with BPPV differ from the general population in terms of systemic disease burden remains underexplored. This question holds clinical relevance for otolaryngologists and vestibular specialists, as early identification of coexisting endocrine or metabolic disorders may influence prognosis, recurrence risk, or referral patterns.
Further investigation is warranted to clarify the relationship between BPPV and systemic medical conditions, particularly those involving metabolic and endocrine dysfunction. This study aims to address this gap by comparing the prevalence of hypothyroidism, diabetes mellitus, hypertension, and osteoporosis in patients with BPPV to national prevalence estimates. Furthermore, this study explores potential sex-based differences in these associations. This study hypothesized that there would be a significant relationship between BPPV and each of the specified comorbidities compared to controls, where patients with BPPV are more likely to suffer from additional comorbidities compared to those without BPPV.
Materials & methods
Study Design & Setting
This study employed a retrospective case-control design to investigate the prevalence of systemic comorbidities in individuals diagnosed with BPPV. Patient data were obtained from an outpatient sports medicine and rehabilitation clinic operating in association with a neuro-otolaryngologist in Florida, USA. The clinic specializes in vestibular rehabilitation and serves a large population of patients suffering from dizziness, imbalance, and vertigo-related symptoms.
Data collection occurred over a consecutive six-month period and included adult patients evaluated for suspected BPPV. Patients were referred to the clinic by otolaryngology, neurology, and primary care providers. BPPV diagnoses were made by a licensed physician and physical therapist using a standardized clinical assessment, including a detailed history of symptoms, head impulse test, test of skew, and spontaneous nystagmus (HINTS) examination, additional vestibular screening, and positional testing to identify canal involvement. Only patients who demonstrated clear, canal-specific nystagmus and positional vertigo consistent with BPPV were included in the study.
Inclusion and exclusion criteria
Inclusion criteria: • Age 18 years or older • Confirmed clinical diagnosis of BPPV based on physical exam findings • Availability of demographic and medical history data
Exclusion criteria: • History of other vestibular disorders (e.g., vestibular neuritis, Meniere’s disease, bilateral vestibulopathy) • Concurrent neurological or inner ear pathology at the time of diagnosis • Incomplete or ambiguous documentation of comorbidities
Patients
Patients were retrospectively recruited through a sample of convenience from electronic medical records of patients that presented to the clinic with complaints of vertigo. Comorbidities were considered present if there was a physician-documented diagnosis in the medical record or if the condition was listed among the patient’s active medical problems. Medication use and laboratory values were not available for verification in this dataset.
Instead of recruiting a control sample, this study used prevalence estimates from the National Center for Health Statistics (NCHS) to provide benchmark population data.25–29 This approach was selected due to the retrospective nature of the study and the lack of available matched controls within the clinic’s electronic records system. National data from 2017 to 2023 were extracted from publicly available CDC sources, stratified by sex where applicable. Prevalence estimates for hypothyroidism, DM, HTN, and osteoporosis were matched to the sex distribution of the study sample to approximate expected frequencies. National Health Statistics indicate that overall health trends in Florida align closely with national averages and therefore provide a reasonable approximation for national baseline risk. However, the authors acknowledge this method may introduce population-level variation.
Statistical analysis
A chi-square goodness of fit test was used to compare the observed sex distribution in the BPPV sample to the expected distribution based on national BPPV prevalence (assumed 2:1 female to male ratio). Logistic regression analysis was used to evaluate the odds of comorbid conditions in the BPPV sample relative to national prevalence estimates. Binomial logistic regression models were constructed with BPPV as the dependent variable and hypothyroidism, DM, HTN, and osteoporosis as independent variables. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated for each comorbidity. Statistical significance was defined as p < .05. To explore potential sex-specific effects, models were stratified by sex and repeated separately for male and female patients. All analyses were conducted using RStudio Team (2020, Boston, MA) and Jamovi (The Jamovi Project, 2025, Sydney, Australia).
Results
Subject characteristics by age and sex.

This table summarizes the age distribution of male and female patients diagnosed with benign paroxysmal positional vertigo (BPPV) in the study sample (N = 140). Age groups are represented in 10-year increments, with frequencies provided for each sex.
Observed vs. expected sex distribution of BPPV patients.
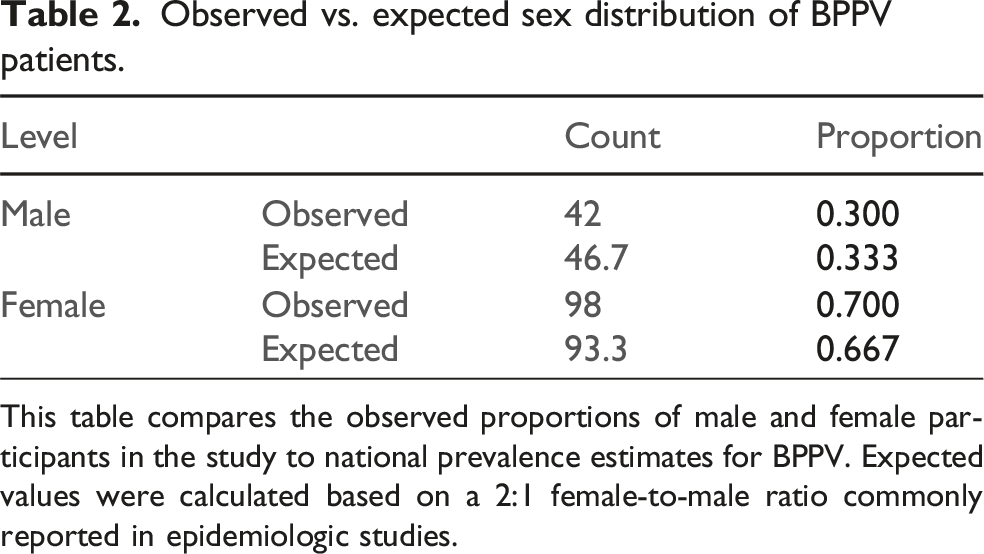
This table compares the observed proportions of male and female participants in the study to national prevalence estimates for BPPV. Expected values were calculated based on a 2:1 female-to-male ratio commonly reported in epidemiologic studies.
Chi-square goodness of fit test for sex distribution.

This table presents the results of a chi-square test used to determine whether the sex distribution of the study sample significantly differs from national expectations. No significant difference was found.

This table outlines sex-specific national prevalence rates for hypothyroidism, diabetes mellitus, hypertension, and osteoporosis in U.S. adults, based on publicly available data from the National Center for Health Statistics (NCHS).
Logistic regression results: Association between BPPV and comorbidities (All patients).

Note. Estimates represent the log odds of “BPPV = Y” vs. “BPPV = N”.
This table presents binomial logistic regression coefficients estimating the odds of having BPPV for patients with each comorbidity, compared to national prevalence rates. Significant associations were observed for hypothyroidism and diabetes mellitus.
Although the observed proportion of BPPV patients with HTN was elevated compared to national data, the association did not reach statistical significance (OR = 1.18, 95% CI [0.70–1.99], p = .527). Similarly, the prevalence of osteoporosis/osteopenia in the sample was slightly lower than expected, and the analysis indicated a non-significant trend toward reduced odds (OR = 0.46, 95% CI [0.20–1.06], p = .068). These non-significant findings may reflect either a true lack of association or limited statistical power, particularly in sex-stratified analyses.
Logistic regression results: Association between BPPV and comorbidities (Males only).
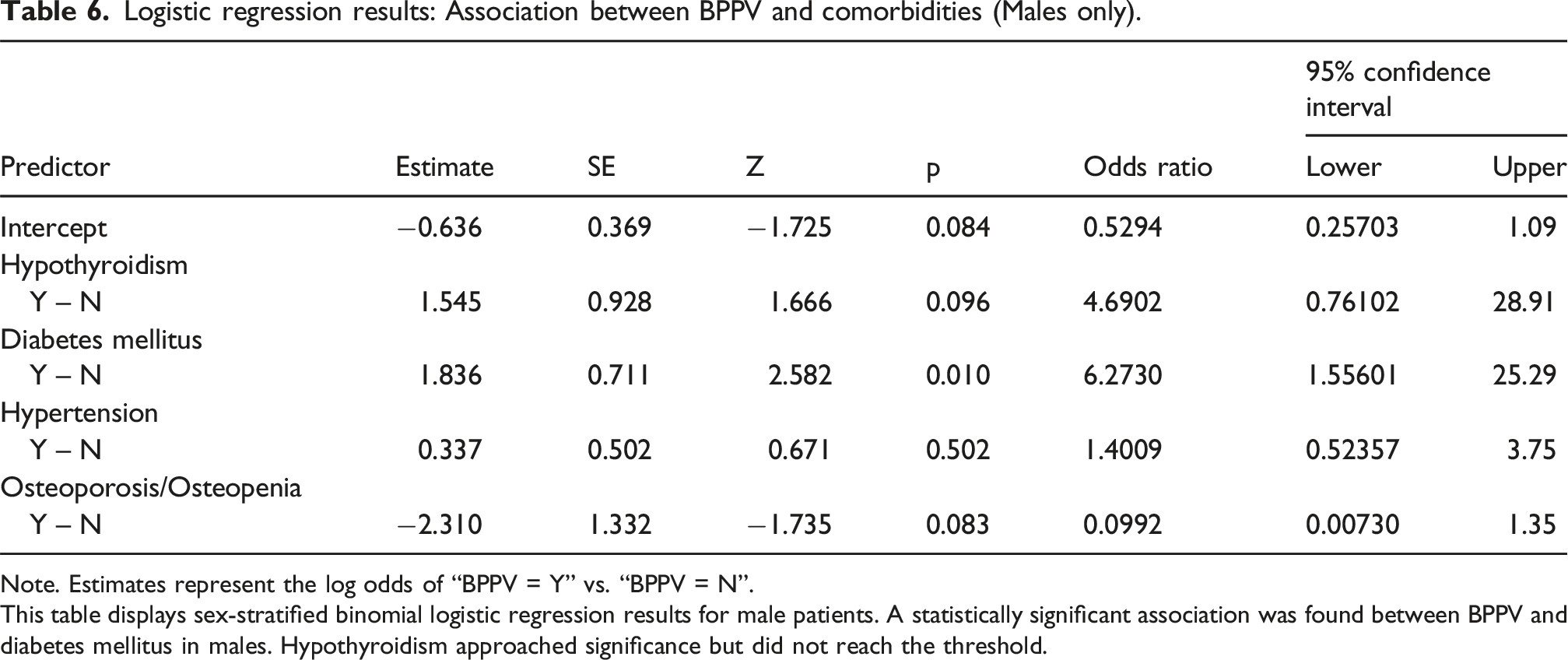
Note. Estimates represent the log odds of “BPPV = Y” vs. “BPPV = N”.
This table displays sex-stratified binomial logistic regression results for male patients. A statistically significant association was found between BPPV and diabetes mellitus in males. Hypothyroidism approached significance but did not reach the threshold.
Logistic regression results: Association between BPPV and comorbidities (Females only).

Note. Estimates represent the log odds of “BPPV = Y” vs. “BPPV = N”.
This table presents logistic regression results limited to female participants. A statistically significant association was identified between BPPV and hypothyroidism. No other comorbidities reached statistical significance in this subgroup.
In contrast, among females, hypothyroidism was significantly more common in those with BPPV compared to national estimates (OR = 2.66, 95% CI [1.16–6.08], p = .021). However, DM did not reach statistical significance in the female subgroup (OR = 1.40, 95% CI [0.54–3.63], p = .491), despite showing a trend toward increased prevalence. Neither HTN nor osteoporosis showed significant associations in the sex-stratified models.
Figure 1 presents a forest plot illustrating the odds ratios and confidence intervals for each comorbidity, visually highlighting the significant associations for hypothyroidism and DM, as well as the non-significant trends for HTN and osteoporosis. Forest plot of odds ratios for comorbidities in patients with BPPV. This figure illustrates the odds ratios (ORs) and corresponding 95% confidence intervals for hypothyroidism, diabetes mellitus, hypertension, and osteoporosis in individuals diagnosed with benign paroxysmal positional vertigo (BPPV), relative to national prevalence estimates. OR values to the right of the vertical line at 1.0 indicate increased odds among BPPV patients. Asterisks (*) denote statistically significant differences (p < .05).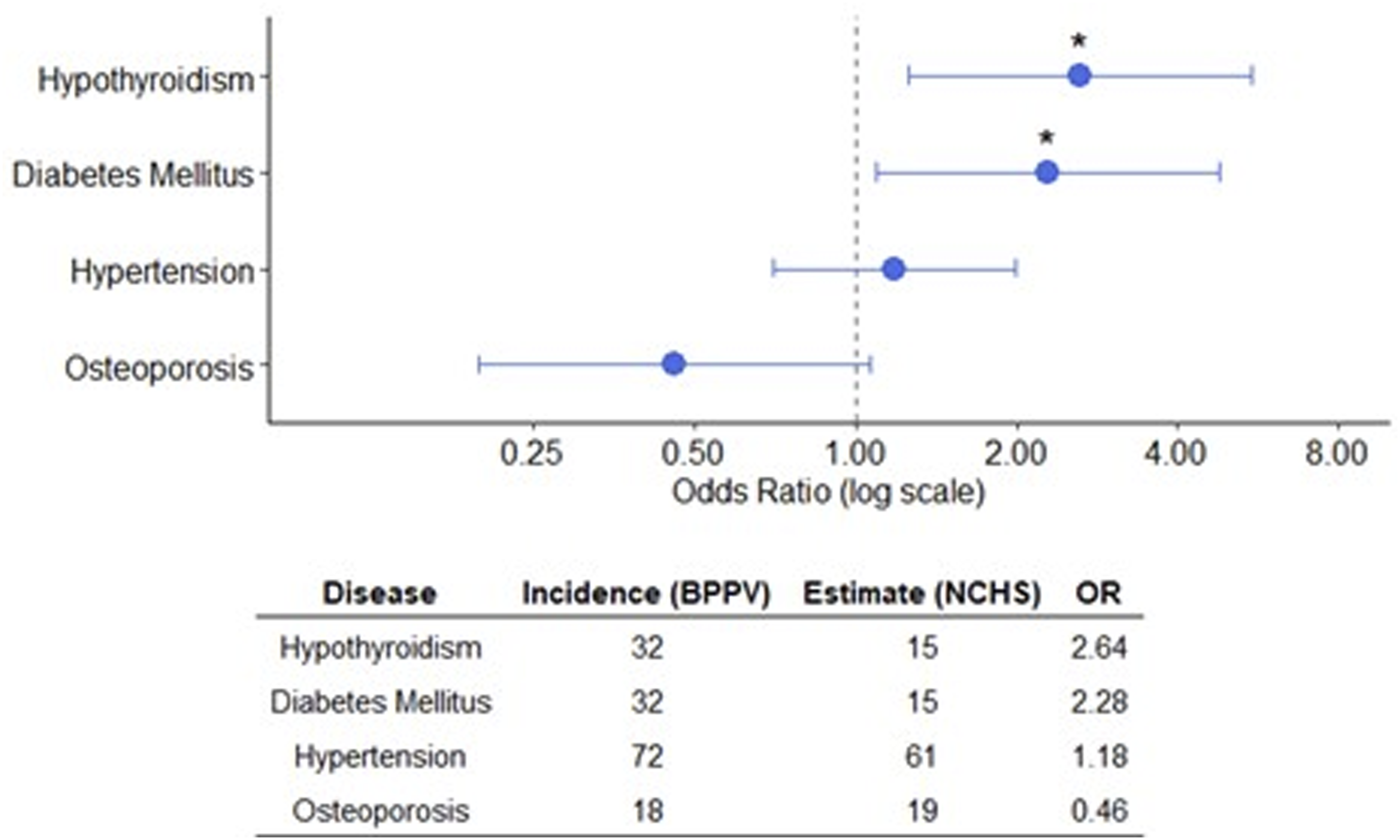
Discussion
This retrospective case-control study revealed statistically significant associations between BPPV development and both hypothyroidism and DM. The results obtained from this analysis support the growing body of evidence that BPPV may not occur in isolation. The development of BPPV may share common underlying pathophysiological mechanisms with certain endocrine and metabolic disorders. These findings contribute to a broader understanding of BPPV as a condition that may be influenced by systemic health factors, rather than being confined solely to abnormalities within the vestibular apparatus.
Notably, individuals with BPPV had nearly three times the odds of having hypothyroidism compared to national prevalence rates. Even greater odds were observed in the male subgroup; however, the association in males did not reach statistical significance. This lack of significance is most attributable to limitations in the sample size, which may have reduced the statistical power necessary to detect meaningful differences within this subgroup. These results align with prior literature indicating that autoimmune and metabolic dysfunctions may contribute to the onset or recurrence of BPPV. Specifically, the presence of anti-thyroid antibodies has been associated with increased BPPV recurrence, supporting the hypothesis that thyroid dysfunction may influence inner ear homeostasis and the stability of otoconia.15,24 Several studies have investigated a possible link between Hashimoto’s thyroiditis and BPPV, but the findings have been mixed.20,22–25 The significantly increased odds of hypothyroidism observed in this sample highlight the need for further research into sex-specific risk pathways, as well as the possibility of underdiagnosed thyroid disease, particularly among men.
Thyroid hormones play a multifaceted role in regulating a variety of physiological processes that are critical to maintaining systemic and cellular homeostasis. These hormones are known to influence calcium metabolism, mitochondrial energy production, and participate in the regulation and maintenance of neurosensory tissue. Each of these biological mechanisms has the potential to affect the delicate microenvironment of the vestibular system. Evidence from experimental models has demonstrated that inner ear structures exhibit a marked sensitivity to fluctuations in thyroid hormone levels, not only during critical periods of embryonic and postnatal development but also throughout adulthood. This hormonal sensitivity may help to explain how subtle dysfunction may predispose an individual to otoconial degeneration, increasing susceptibility of developing BPPV.30,31 Additionally, autoimmune thyroid disease may contribute to chronic inflammation or immune-mediated damage affecting the inner ear. These proposed mechanistic hypotheses are especially relevant when considering recurrent BPPV, which has been reported with greater frequency among individuals who demonstrate the presence of circulating thyroid-specific autoantibodies indicative of an underlying autoimmune thyroid disorder.30,31
Furthermore, individuals with BPPV exhibited more than twice the odds of DM compared to national prevalence estimates. This is consistent with existing literature suggesting that the microvascular changes associated with DM may impair vestibular function and contribute to BPPV development.32,33 Diabetes-related capillary dysfunction may reduce blood flow to the utricle and semicircular canals, impairing nutrient delivery and waste clearance in the vestibular system. Similarly, chronic hyperglycemia and insulin resistance can also promote systemic inflammation, oxidative stress, and altered calcium regulation, contributing to otoconia instability. 2
Within the male subgroup, the association between DM and BPPV remained statistically significant, whereas it did not reach significance within the female subgroup. This difference may be attributable to sex-specific factors, including differences in metabolic disease presentation, underdiagnosis, or the modifying influence of sex hormones on vestibular homeostasis. Male patients may also be more likely to present with DM-related microvascular complications that increase their susceptibility to vestibular dysfunction, though further study is needed. These findings support a growing body of literature suggesting that metabolic conditions may differentially affect vestibular health across sexes. 34
In contrast to previous studies, the current investigation did not reveal any statistically significant associations between BPPV development and the presence of either hypertension or osteoporosis. However, a higher, albeit non-significant rate of HTN was observed in patients with BPPV. Reduced bone mineral density and vitamin D deficiency are commonly cited risk factors for otoconial degeneration. Similarly, longstanding hypertension has been linked to impaired cerebral and inner ear perfusion.35,36 While previous research has consistently documented associations between BPPV and both vascular risk factors and compromised bone health, the results of this study did not reach the threshold for statistical significance to support such relationships.9,19 The lack of significance in the current study may reflect limitations in sample size, age distribution, or the methods used to identify comorbidities. Specifically, HTN and osteoporosis are often underreported in outpatient records unless directly managed within the same clinic, which may result in classification bias. The observed lack of association with HTN and osteoporosis may be influenced by confounding factors not controlled for in this study. Age, physical activity level, menopausal status, and medication use (e.g., bisphosphonates or antihypertensives) could all influence the presence or detection of these conditions. Given the complex interplay between aging, systemic health, and vestibular function, future studies should aim to account for these variables in a more comprehensive manner.
From a clinical perspective, these findings suggest that a more comprehensive evaluation of systemic health conditions in individuals who present with BPPV is warranted, particularly those exhibiting recurrent episodes or symptoms that are unyielding to standard canalith repositioning maneuvers. This comprehensive assessment should ideally include laboratory screening and clinical evaluation of thyroid functions such as measurement of thyroid hormone levels, thyroid-specific autoantibodies, and tests to assess glycemic control, including fasting blood glucose levels and hemoglobin A1c levels. Clinicians involved in the diagnosis and management of vestibular disorders including, but not limited to, otolaryngologists, audiologists, neurologists, and vestibular physical therapists should be aware of these potential associations and consider appropriate referrals when possible underlying metabolic and/or endocrine dysfunction may be present to ensure timely and targeted intervention. Moreover, the integration of interdisciplinary care models, involving collaboration among specialists from multiple fields, may offer substantial benefits in the management of patients who present with complex BPPV.
Several limitations inherent to this study design must be acknowledged. The retrospective nature of the analysis, combined with the use of national prevalence estimates as a comparator rather than matched control subjects, limits the ability to draw causal inferences. Potential confounding variables such as age, ethnicity, body mass index, medication use, or duration of disease were not accounted for due to constraints in the dataset. While stratification by sex provided useful insights, the relatively small sample sizes within each subgroup may limit the generalizability of the findings. Additionally, reliance on chart-documented diagnoses may result in misclassification if conditions were underdiagnosed or inconsistently reported. This study did not include data on recurrence rates, vestibular test results, or symptom duration, which would have strengthened the analysis.
Future prospective studies should aim to control confounding factors that may influence the observed association between BPPV and systemic health conditions. To enhance reliability and specificity, laboratory-confirmed markers of thyroid and metabolic function such as serum levels of thyroid hormones, thyroid-stimulating hormone, thyroid autoantibodies, fasting glucose, and hemoglobin A1c should be incorporated. Additionally, there is a growing need to explore the underlying mechanistic pathways that may link metabolic and endocrine dysfunction with vestibular pathology. To validate and expand upon the preliminary findings reported in current literature, large-scale, multicenter studies involving diverse and adequately powered populations will be essential for validating these findings and exploring their broader clinical implications. Incorporating imaging, vestibular function testing, and patient-reported outcomes could provide a more comprehensive understanding of how systemic conditions interact with vestibular dysfunction.
Conclusion
The results of this study suggest that systemic endocrine and metabolic conditions may contribute to the pathophysiology of BPPV. Specifically, individuals with BPPV demonstrated significantly higher odds of both hypothyroidism and diabetes mellitus compared to national prevalence estimates, reinforcing emerging evidence that BPPV may be influenced by broader systemic health factors rather than functioning as an isolated peripheral vestibular disorder.
The inclusion of both endocrine and metabolic-bone health variables permitted a more comprehensive evaluation of potential risk factors. While the association with hypertension and osteoporosis did not reach statistical significance, non-significant trends in both variables, particularly in subgroup analyses, suggest that additional exploration may still be warranted. The observed sex-based differences in comorbidity patterns also point toward potential hormonal or physiological modifiers that could influence vestibular vulnerability.
These findings underscore the importance of maintaining a heightened awareness for coexisting thyroid and metabolic disorders when managing patients with BPPV. Incorporating simple screening questions or considering referrals for medical evaluation may be especially valuable in cases of recurrent or treatment-resistant vertigo. For vestibular specialists and otolaryngologists, this study supports a more integrative approach to care that includes attention to systemic health status alongside canalith repositioning maneuvers. Clinicians should maintain a heightened level of vigilance for coexisting thyroid and metabolic disorders when managing this patient population.
Future research should prioritize prospective, longitudinal, multicenter study designs that include laboratory-confirmed diagnoses and account for confounding variables such as age, BMI, sex hormones, and medication use. Exploring whether targeted management of comorbid conditions can reduce the frequency or severity of BPPV episodes represents a promising direction for improving long-term patient outcomes.
Footnotes
Acknowledgements
This study would like to acknowledge Dr. James S. Atkins, MD as the attending physician at the clinic. Dr. Atkins was the primary provider responsible for these patients care. This study would also like to acknowledge Dr. Rebecca Firpi, PT, DPT as an evaluating and treating physical therapist at the clinic. Dr Firpi was responsible for evaluating patients with various vestibular disorders including suspected BPPV and subsequently treating them.
Ethical considerations
This study was approved by the AdventHealth Research Institute Internal Review Board (IRBNet# 1614564).
Consent to participate
This study was a retrospective chart review study with no risk to patients. The primary investigator requested a Waiver of HIPAA Authorization and was approved by the AdventHealth Research Institute Internal Review Board. Informed consent was not required.
Author contributions
RA is the primary investigator on this study. She originally proposed the study, conducted the patient chart review, extrapolated and deidentified relevant patient data, and prepared the data for statistical analysis. AV is the corresponding author on this study. He primarily conducted statistical analysis and interpreted the results, crafted tables and figures, and formulated conclusions. Both authors made a significant contribution to the concept, design, acquisition, analysis or interpretation of data, were involved in drafting the article or revising it critically for important intellectual content, approved the final version of the article for publication, and agreed to be accountable for all aspects of the work and resolved any issues related to its accuracy or integrity.
Funding
This study did not receive or require funding.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available at ![]() . For additional requests please contact the corresponding author.
37
. For additional requests please contact the corresponding author.
37