
Abstract
Background
Comorbidity among coronavirus disease-19 (COVID-19) patients contributes to increasing their susceptibility to severe illness. The objectives of this systematic review and meta-analysis were to assess the prevalence of comorbidities and their association in increased severity of disease and mortality in COVID-19 patients.
Methods
A thorough search of the literature was conducted using PubMed, Google Scholar, and other sources to include pertinent studies. Two independent authors extracted pertinent data using Microsoft Excel and exported it to Stata version 17 for meta-analysis. This review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Heterogeneity was assessed through I2 statistics, subgroup analysis for categorical variables, and meta-regression for continuous variables. Publication bias was assessed through funnel plot and Egger statistics. Furthermore, a meta-analysis was performed using a random-effects model to estimate the pooled odds ratio (OR) with 95% CI, which was used to assess the association between comorbidity and severity and/or mortality of COVID-19.
Results
A total of 62 studies with 611,646 patients were included. The pooled prevalence of comorbidity among COVID-19 was 53.9% (95% CI: 48.4–59.3). Comorbidity was significantly associated with severity of COVID-19. Specifically, hypertension (OR: 1.09; 95% CI: 1.03–2.51), diabetes mellitus (OR: 1.29; 95% CI: 1.07–1.56), and obesity (OR: 1.61; 95% CI: 1.46–1.76) significantly increased the odds of severe COVID-19. Furthermore, hypertension (OR: 1.14; 95% CI: 1.02–1.57), diabetes mellitus (OR: 1.39; 95% CI: 1.17–1.65), obesity (OR: 1.24; 95% CI: 1.15–1.32), chronic kidney diseases (OR: 1.62; 95% CI: 1.25–2.09), and chronic obstructive pulmonary diseases (COPD) (OR: 1.23; 95% CI: 1.15–1.32) were significantly associated with mortality of COVID-19 patients.
Conclusion
The pooled prevalence of comorbidity among COVID-19 was found slightly higher than that reported in previous systematic reviews, which ranged from 40.0% to 41.1%. Comorbidity increased the odds of severe COVID-19. Participants with hypertension, obesity, or diabetes mellitus had significantly increased odds of severe COVID-19. There is a need to have close follow-up of COVID-19 patients who have comorbidity.
Protocol registration
This systematic review and meta-analysis study was registered under the registration number CRD42023493170.
Introduction
Coronavirus disease-19 (COVID-19) is a disease caused by the coronavirus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). It often spreads between people who are in close contact. Worldwide, as of December 13, 2023, there are 772,386,069 confirmed cases of COVID-19, including 6,987,222 reported deaths. According to the World Health Organization (WHO) report, Europe is the highest priority with 277,379,680 confirmed cases, followed by the Western Pacific with 207,662,893 and the Americas with 193,158,876. According to WHO death reports, the US reported 2,975,353 deaths and Europe reported 2,257,825. 1
A global systematic review and meta-analysis (SRMA) found that the most common comorbidities among COVID-19 patients were hypertension (20%–22%), followed by diabetes (9%–11%) and cardiovascular diseases (5%–9%). Additionally, the study reported that the prevalence of cancer, chronic obstructive pulmonary disease (COPD), cerebrovascular disease, and chronic kidney disease among COVID-19 patients was approximately 3.9%, 3.1%, 3.0%, and 2.4%, respectively.2,3
Comorbidities among COVID-19 patients may contribute to increasing their susceptibility to severe illness. Previous reviews found significant associations between COVID-19 severity and comorbidities, such as chronic respiratory diseases, diabetes, hypertension, chronic kidney disease, and cardiovascular diseases. Obesity, cerebrovascular disease, COPD, malignancy, and chronic liver diseases were all risk factors for severe illness and mortality of COVID-19.4,5
People with severe disease and those needing hospital treatments should receive treatment as soon as possible. The consequences of severe COVID-19 include death, respiratory failure, sepsis, thromboembolism, and multi-organ failure, including injury of the heart, liver, or kidneys.6,7 In rare situations, children can develop a severe inflammatory syndrome a few weeks after infection. Some people who have had COVID-19, whether they have needed hospitalization or not, continue to experience symptoms. 8 These long-term effects are called long COVID (or post-COVID-19 condition). The most common symptoms associated with long COVID include fatigue, breathlessness, and cognitive dysfunction (for example, confusion, forgetfulness, or a lack of mental focus or clarity). Long COVID can affect a person’s ability to perform daily activities such as work or household chores. 9
Knowing who is more at risk of severe outcomes and/or death is useful to clinicians and health authorities to implement new strategies and initiatives for COVID-19 patients. Even though previously there were studies undertaken as primary research to assess the prevalence of comorbidities in COVID-19 patients, there is a discrepancy in the prevalence of comorbidities in COVID-19 patients. Previously undertaken systematic reviews and meta-analyses were based primarily on studies collected from the Chinese population. Thus, the findings might not be generalizable because of population differences in race and ethnicity. As a result, this SRMA was undertaken to assess the prevalence of comorbidities and their association with increased severity of disease and mortality in COVID-19 patients.
Methods
Search strategy
This SRMA was conducted and reported following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 10 The protocol for this SRMA is registered in the International Prospective Register of Systematic Reviews (PROSPERO) under the registration number CRD42023493170.
A comprehensive literature search was performed using PubMed, Google Scholar, and other sources to identify relevant studies. To incorporate pertinent research the following search terms were used in PubMed(((((((((((((“epidemiology”[MeSH Subheading]) OR (“epidemiology”[MeSH Terms])) OR (“prevalence”)) OR (“prevalence”[MeSH Terms])) AND (“comorbidity”)) OR (“Underline diseases”)) AND (“severity”)) OR (“mortality”)) OR (“death”)) OR (“ICU admission”)) OR (“mechanical ventilation”)) AND (“COVID-19”)) OR (“novel corona”)) OR (“SARS COV2”). Furthermore, in Google scholar the following search term was used to include studies “prevalence” and “comorbidities” and “severity” or “mortality” and “COVID-19.”
Mendeley was used as reference manager to handle duplicate and for citation. Papers published from inception to December 12, 2023 were included for screening using title, abstract and full text.
Eligibility criteria
Two independent reviewers (BZ and NT) initially screened all article titles and abstracts to determine their relevance to the SRMA. Following this, the full texts of the articles were reviewed by the same two reviewers. This full-text review was conducted according to pre-specified inclusion and exclusion criteria to ensure the consistency and rigor of the selection process. Disagreements between reviewers were resolved through discussion.
Inclusion criteria
For this SRMA, we included only COVID-19 patients as the study population. This review included studies conducted globally in both facility-based and community-based settings. To ensure consistency and feasibility in data extraction, only studies published in English were included. Although this may introduce a potential risk of language bias, the majority of research on COVID-19 and comorbidities is published in English-language journals. Additionally, studies published from inception through December 12, 2023, were considered, allowing for a comprehensive and up-to-date synthesis of the available evidence. Studies reporting the prevalence of comorbidities and/or their association with disease severity and/or mortality in COVID-19 patients were included in the meta-analysis.
Exclusion criteria
Articles with no epidemiological information (prevalence) were excluded. Additionally, experimental studies, duplicate publications, systematic reviews, meta-analyses, case reports, case series, and studies conducted in a population group that was not generalizable were excluded.
Outcome measure
The primary outcome of SRMA is to estimate the prevalence of comorbidity in COVID-19 patients. The secondary (additional) outcome is to estimate the association of comorbidity with the severity and mortality of COVID-19 patients. The clinical presentation of severe disease is characterized by shortness of breath, hypoxemia, acute respiratory distress syndrome requiring mechanical ventilation, multi-organ failure, and death. 11
Quality assessment
Two authors (BZ, NT) independently assessed the methodological quality of included studies. For quality assessment of included studies standardize Newcastle-Ottawa quality assessment scale for cohort studies and case control studies was used. 10 Any disagreements during the quality assessment process were resolved through discussion.
Data extraction process
Microsoft excel was prepared for data extraction as a template. Two authors (BZ, NT) independently extract data and any disagreement was solve by scientific merit. Information’s were extracted from study includes name of primary author, year of publication, country, study design, patient characteristics, sample size, prevalence of comorbidity (hypertension, diabetic mellitus, cardiovascular disease, cerebrovascular disease, renal diseases, asthma, chronic obstructive pulmonary disease with COVID-19 patients, and odds ratio (OR) of association of comorbidity with severity and or mortality of COVID-19 patients. The mean age with corresponding standard deviation of participants was extracted. In cases where the mean age was not available, the median age with interquartile range was used as a substitute. When both mean and median age were reported, the mean age was used for consistency, unless there was evidence of significant age distribution skewness.
Data analysis
Data extraction was performed using a pre-prepared Microsoft Excel template and then exported to Stata version 17 (Stata Corp., College Station, TX, United States) for meta-analysis. The overall estimated prevalence was pooled using a random-effects model, which assumes variability in effect sizes across studies and considers the included studies as a random sample from a larger population. A study characteristics table was used to present the details of the included individual studies. The results of this systematic review and meta-analysis were presented in a forest plot. The inverse variance method (DerSimonian–Laird estimation) was applied, where the weight assigned to each study was the inverse of its variance. 12
In a meta-analysis, variations in effect sizes across studies are expected due to sampling variation. However, when the observed variation exceeds what can be attributed to sampling alone, it indicates between-study heterogeneity. In this SRMA, heterogeneity was assessed both graphically using a Forest plot, a graphical representation used in meta-analysis to display the effect sizes of individual studies along with their confidence intervals (CIs), and objectively through the I2 statistic which quantifies the percentage of total variation across studies that is due to heterogeneity rather than chance. I2 values indicate the degree of heterogeneity 25%: Low heterogeneity, 50%: Moderate heterogeneity, 75%: Substantial heterogeneity. 13
To identify sources of heterogeneity, a subgroup meta-analysis was performed based on geographical region, sample size, and publication year. This approach aimed to reduce random variations among the point estimates of the primary studies. The overall prevalence estimates were then calculated separately for each subgroup. A data-driven approach using the median split was applied to determine the cutoff for subgroup analysis based on a continuous variable. Additionally, studies were categorized according to their geographical region of origin. Meta-regression was performed with publication year, sample size, and age as moderator covariates, and prevalence of comorbidity as the dependent variable to identify potential sources of heterogeneity. Publication bias was explored graphically by funnel plot and objectively by Egger tests.
14
Asymmetry in the funnel plot and/or P-values < 0.05 indicate the presence of publication bias. The standard error of prevalence (SEP) for comorbidities was calculated using the formula
Results
Study selection and identification
A total of 2792 studies were initially identified through searches in Google Scholar, PubMed, and manual reference screening. After removing 1099 records prior to screening, 1693 records remained for initial review. Of these, 180 were excluded based on title and abstract screening. The remaining 1513 reports were sought for full-text retrieval, from which 540 were excluded. Subsequently, 973 full-text reports were assessed for eligibility, leading to the exclusion of 911 studies. In the end, 62 studies fulfilled the eligibility criteria and were included in this systematic review and meta-analysis. The search and selection process adhered to PRISMA guidelines (Figure 1). PRISMA flow diagram for selection of studies.
Characteristics of included study
Summary of baseline characteristics of included studies in Systematic review and meta-analysis (n = 62).
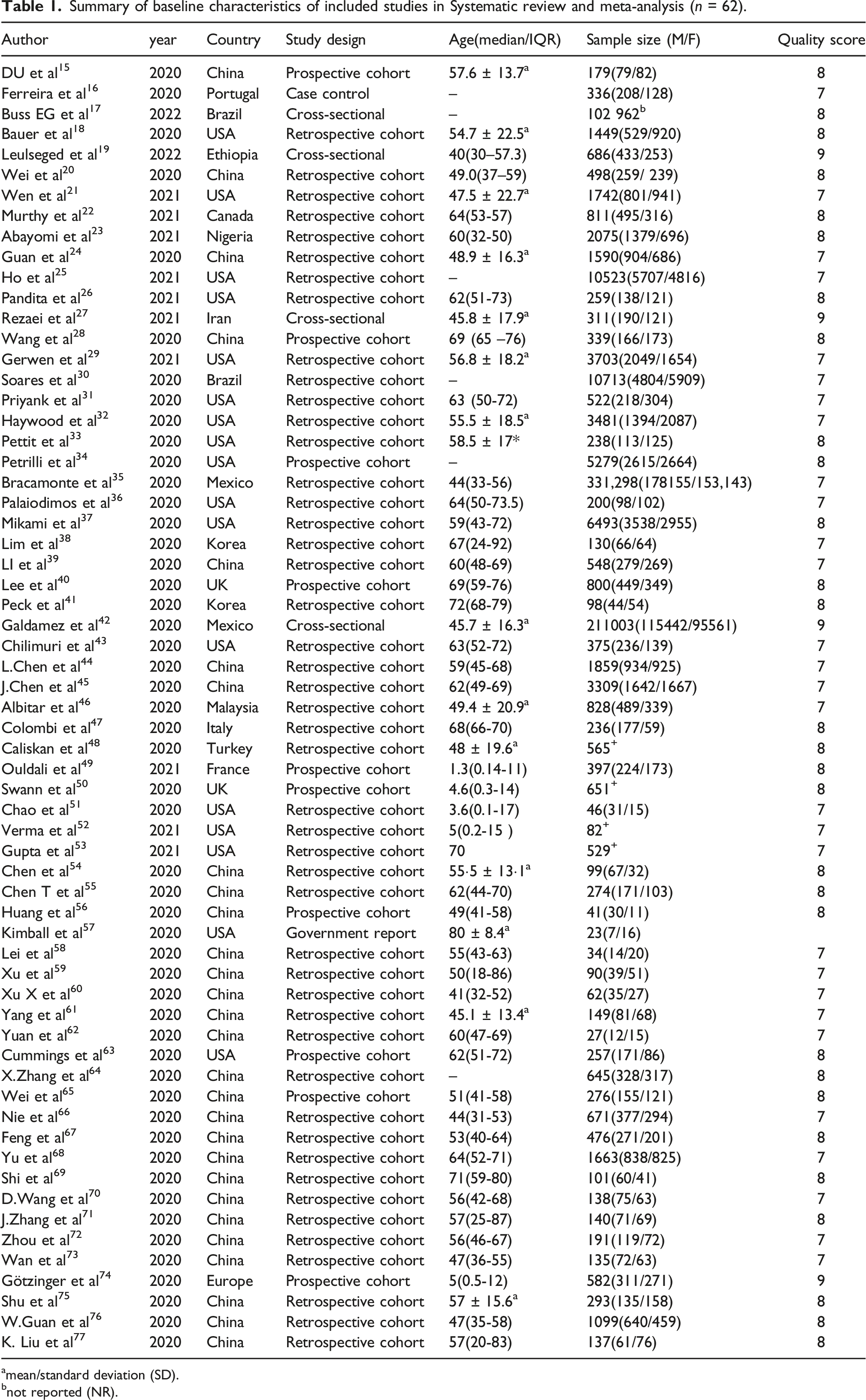
amean/standard deviation (SD).
bnot reported (NR).
Quality of included study
Newcastle-Ottawa scale (NOS) was used to assess the methodological quality of included study. The NOS score ranges from 6 to 9. The mean of NOS score for cohort study (prospective and retrospective) was 8 star and for cross-section was about 9 star. While the majority of the studies included in the meta-analysis were of high quality, some studies lost points primarily for the reasons of some studies did not report all relevant outcomes, limited control over confounding variables, and the methods used to measure outcomes were not sufficiently detailed.
Prevalence of comorbidity
In this SRMA, the pooled prevalence of comorbidity was estimated with DerSimnian-Liard estimation, and weights are from a random-effects model. In this review, the pooled prevalence of comorbidity (at least one) in COVID-19 patients was 53.9%. Regarding heterogeneity, the I2 was 99.9% with a P-value <0.001, which indicates substantial heterogeneity in the comorbidity (Figure 2). Forest plot of pooled prevalence of comorbidity in COVID-19 patients based on random effect model.
Regarding specific comorbidities, according to this meta-analysis, the highest prevalence of comorbidities among COVID-19 patients was hypertension (32.5%), followed by hyperglycemia, obesity, diabetes mellitus (DM), and cardiovascular diseases which were 29.3%, 23.4%, 18.3%, 11.5%, respectively (Figure 3). The lowest prevalence of comorbidities among COVID-19 patients was found in HIV/AIDS (1.02%) (Table 2). Forest plot of pooled prevalence of different comorbidities in COVID-19 patients based on random-effect model. Summary of pooled prevalence of comorbidities in COVID -19 patients.

Sub-group analysis
Summary of sub-group analysis of pooled prevalence of different comorbidities among COVID-19 patients.

Meta –regression
Summary of meta-regression of different covariates with the prevalence of comorbidity among COVID-19 patients.

Publication bias assessment
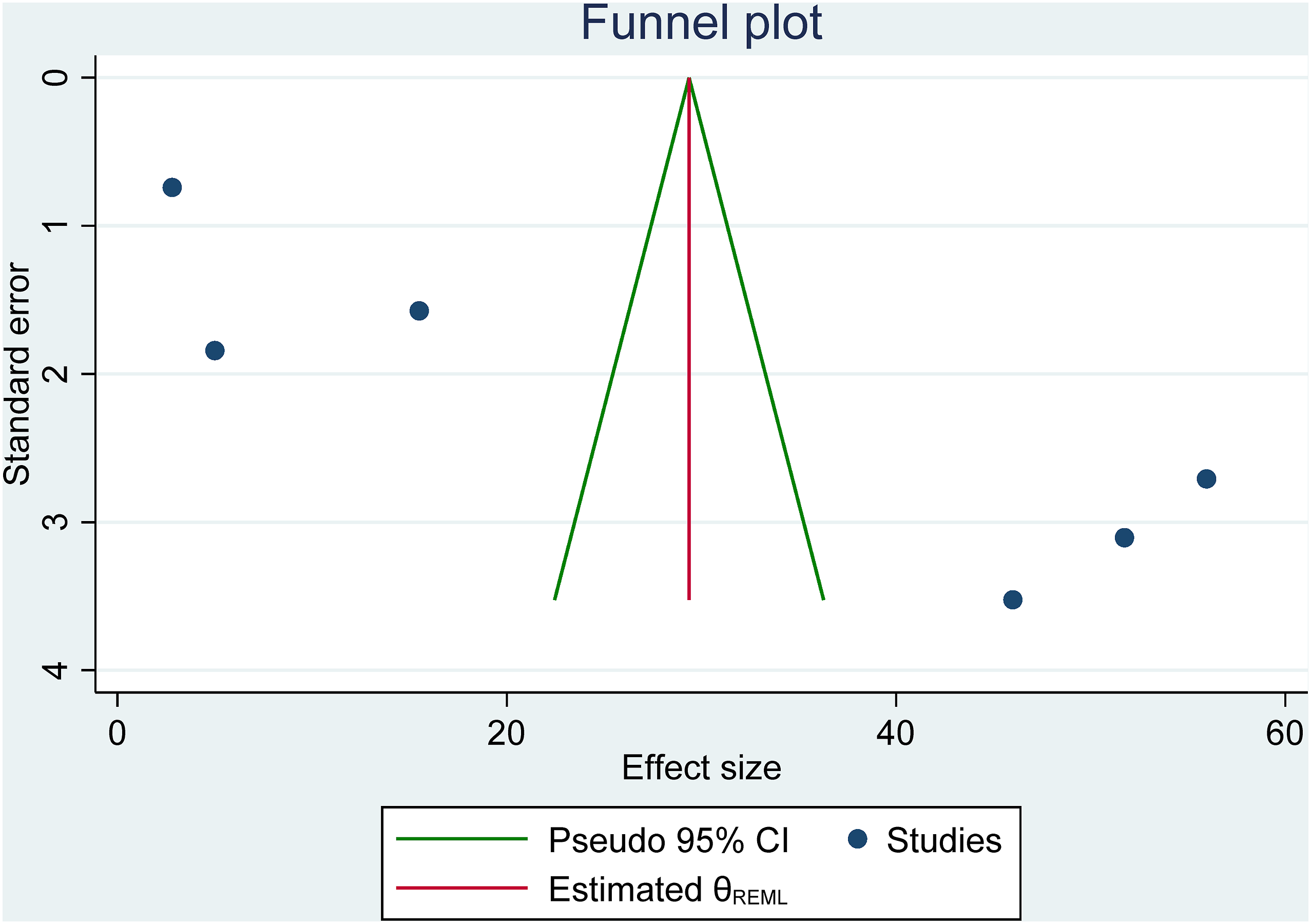
Publication bias was assessed using a funnel plot, which revealed asymmetry, indicating the presence of publication bias (Figure 4). Egger’s test indicated statistically significant publication bias for the prevalence of hyperlipidemia (p <0.001) (Figure 5), chronic liver disease (p < 0.016), cancer (p < 0.001), COPD (p < 0.003), asthma (p < 0.001), chronic lung disease (p < 0.012), cerebrovascular disease (p < 0.015), and HIV/AIDS (p < 0.014) (Table 5). Although no significant publication bias was detected for most comorbidities, the results should be interpreted with caution. The potential underrepresentation of smaller studies with non-significant or negative findings could lead to an overestimation of effect sizes. Furthermore, Egger’s test can be influenced by the number of studies included in the analysis, as well as by between-study heterogeneity. It is important to note that Egger’s test may not be fully reliable when there are fewer than 10 studies, as is the case for some of the analyses presented. Therefore, the results of Egger’s test should be interpreted with caution, and the possibility of publication bias should be considered in the context of the study characteristics and heterogeneity. Funnel plot of publication bias assessment of prevalence of comorbidity among COVID-19. Funnel plot on prevalence of hyperlipidemia among patients with Covid-19. Summary of the association between different comorbidities and mortality of COVID-19.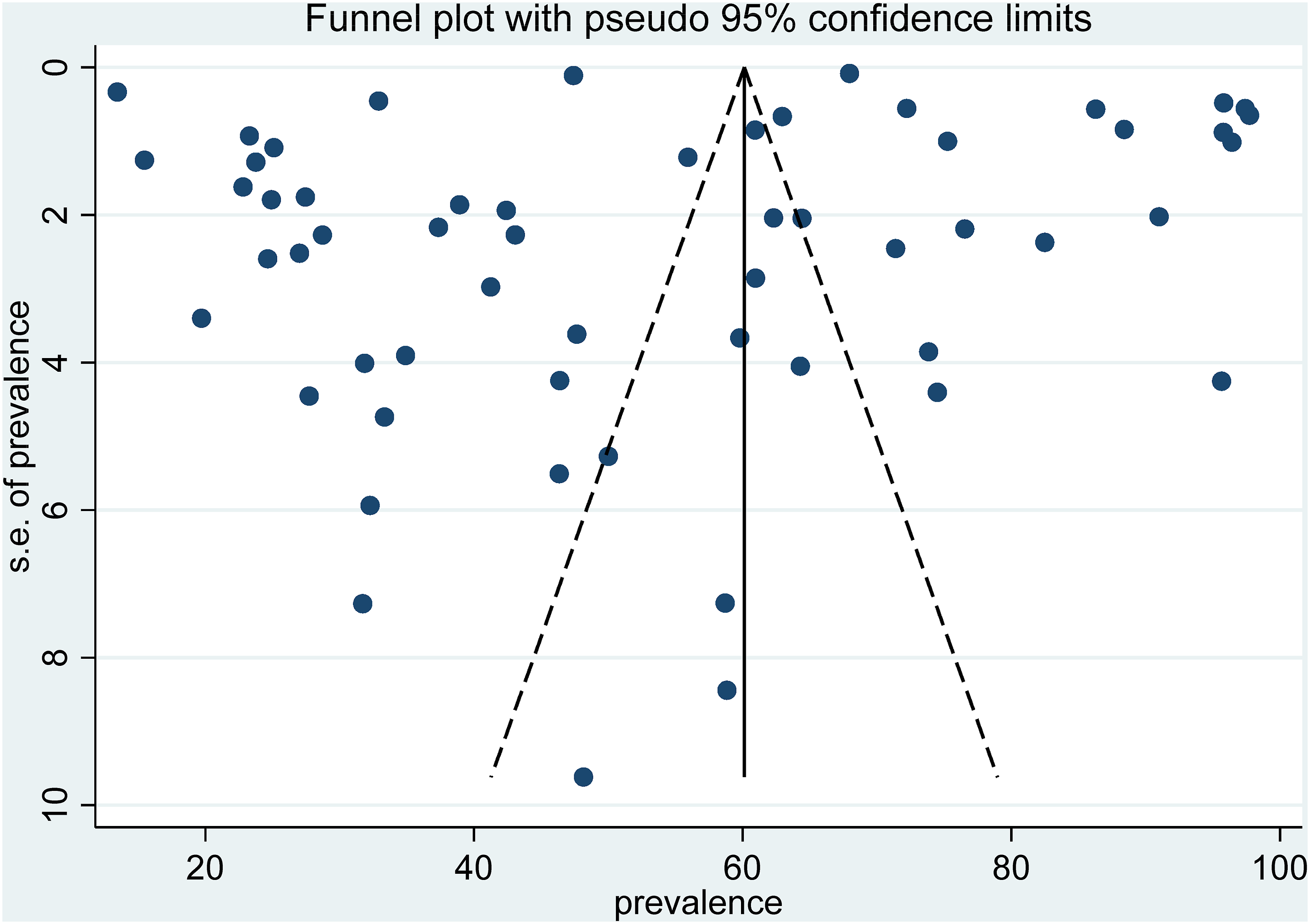

Association between comorbidity and severity of COVID-19
In this meta-analysis, comorbidity (pooled OR 1.61, 95% CI 1.03-2.51) was significantly associated with the severity of COVID-19. Specifically, hypertension (pooled OR 1.09, 95% CI 1.02, 1.17), DM (pooled OR 1.29, 95% CI 1.07, 1.56), and obesity (pooled OR 1.61, 95% CI 1.46, 1.76) were significantly associated with the severity of COVID-19 (Figure 6). Forest plot illustrate the association between different comorbidities and severity of COVID-19 diseases based on random-effect model.
Association between comorbidities and mortality of COVID-19
In this meta-analysis, hypertension (pooled OR, 1.14, 95% CI 1.01-1.28), obesity (pooled OR1.24, 95% CI 1.15-1.32), COPD (pooled OR 1.23, 95% CI 1.15-1.32) (Figure 7), DM (pooled OR, 1.39 95% CI 1.17-1.65), and chronic kidney disease (pooled OR 1.62, 95% CI 1.25-2.09) were significantly associated with mortality of COVID-19 Forest plot illustrate the association between different comorbidities and mortality COVID-19 based on random-effect model.
Disccussion
In this SRMA, the main objective was to assess the pooled prevalence of comorbidity and its association with the severity and mortality of COVID-19.
According to this meta-analysis, the pooled prevalence of comorbidity among COVID-19 patients was 53.9% (95% CI 35.9-59.7). This finding is higher than previous systematic reviews and meta analyses which ranged from 40% to 41.1%.78,79 The possible reason for this discrepancy might be because of the geographical region. For example, previously undertaken SRMA were their included studies were conducted in China, while in this review the included studies were undertaken in North America, China, Africa, and Europe.
Regarding sub-group analysis, the prevalence of comorbidity ranges from 31% (in Africa) to 75% (in North America). The possible reason for this discrepancy might be because difference in lifestyle.
Regarding specific comorbidities, according to this meta-analysis, the most prevalent of comorbidity among COVID-19 patients was hypertension which was 32.5 percent (95% CI 30.7, 34.3). This finding is in contrary to the findings of a previously conducted SRMA. For example, the prevalence found in this study is slightly lower than that reported in a previous SRMA (39%). 80 This discrepancy may be due to differences in study selection criteria, particularly the populations included. The earlier SRMA excluded children with COVID-19, whereas the present analysis includes both adults and children. Moreover, this finding is much higher than the findings of other previous systematic reviews and meta-analyses which were ranged from 14% to 23%.3,78,81–83 The possible reason for this discrepancy might be because of the number of primary studies included. For example, in the previous reviews, the number of primary studies included ranged from 12 to 41, while this review includes 62 primary studies.
In this meta analysis, the pooled prevalence of hyperlipdemia among COVID-19 patients was recorded 29.3% (95% CI 12.6, 46.1). Likewise, the finding is in acordance with prior SRMA that showed the pooled prevalence of hyperlipidemia among COVID-19 were 26.4%. 11
The pooled prevalence of obesity among COVID-19 patients was 23.4% (95% CI 18.2, 28.7). Likewise, prior SRMA revealed that the prevalence of obesity among COVID-19 patients was about 27.9%. 11
The pooled prevalence of DM among COVID-19 patients was 18.3% (95% CI: 17.1,19.5), which contrasts with the findings of a previous SRMA that reported a higher prevalence of 31%. 84 The possible explanation for this difference might be because of the number of primary studies included. Accordingly, the included primary studies of the prior SRMA was 24, while this SRMA includes 62 primary studies.
Regarding the association of comorbidity with the severity of COVID-19, the odds of severe COVID-19 among COVID-19 patients with comorbidity were 1.61(OR 1.61 95% CI 1.03, 2.51) times higher than their counterparts. This might be because comorbid conditions like hypertension, DM, obesity, and smoking are generally linked to pro-inflammatory or chronic inflammation states, vascular endothelial damage, and dysfunctional homeostatic systems, which can result in cytokine storm, multi-organ failure, and acute respiratory distress syndrome.85,86
Further, the association of specific comorbidity with the severity COVID-19, the odds of having severe COVID-19 diseases among COVID-19 patients with hypertension 1.61 times (OR 1.61, 95% CI: 1.02, 1.57) higher than their counterparts. The finding is in line to a previously undertaken meta-analysis.79,81,87 This might be because Renin-angiotensin system inhibitors expression increased that end up with severe COVID-19. 88
The odds of severe COVID-19 among DM were increased by 29 % (OR 1.29, 95% CI: 1.07, 1.56) as compared to their counterparts. The finding is in accord with the previous SRMA79,84,89 that illustrated DM were significantly increased the odds of the severity of COVID-19 compared to their counterparts. This might be because DM cause endothelial damage that end up with higher viral load.
In this SRMA, obesity was found to be significantly increase the odds of severe COVID-19. Accordingly, the odds of severe COVID-19 among obese people are 1.61 times (OR 1.61, 95% CI: 1.46, 1.76) higher than their counterparts. Likewise, the previous SRMA have reported consistent finding. 90 This might be because obesity affects the inflammatory response and end up with release of pro-inflammatory cytokines.91,92
Regarding the association between comorbidities and COVID-19 mortality, the odds of having COVID-19 mortality among DM patients were 1.39(OR 1.39, 95% CI 1.17–1.65) times higher than their counterparts. The finding is in line to the previous SRMA(89). This might be because DM cause endothelial damage that result in multi organ failure.
According to this meta-analysis, obesity was found significantly associated with the mortality of COVID-19. The odds of mortality of COVID-19 patients with obesity 1.24 times (OR 1.24, 95 % CI 1.15-1.32) higher than their counterparts. This finding is consistent with the prior SRMA. 90 This might be because obesity may alter the function of immune cell that result in weekend immunity system and higher viral replication. 93
Chronic kidney diseases was significantly associated with mortality of COVID-19. Accordingly, the odds of COVID-19 mortality among chronic kidney diseases increased by 62% (OR 1.62, 95% CI 1.25-2.09) compared to COVID-19 patients without kidney diseases. This finding is consistent to the prior SRMA.80,94
The odds of having COVID-19 mortality among COPD were 1.23(OR 1.23, 95% CI: 1.15-1.32) times higher than their counterparts. This might be because COPD cause perfusion/ ventilation mismatch. 95
Limitations of the study
This SRMA has certain limitations. First, the small sample size of the selected articles could have potential influence on the pooled estimates. Additionally, all selected studies were published in English, which may introduce language bias. The other is sub-group analysis does not address the source of heterogeneity. The quality of studies varied, and incomplete or inconsistent reporting of key data may have introduced bias or limited the accuracy of our estimates. Furthermore, there is a potential for publication bias. Despite our efforts to include all available studies, smaller studies with non-significant or negative results may be underrepresented in the published literature.
Conclusion
In this SRMA, the pooled prevalence of comorbidity was 53.9%. Particularly, the highest pooled prevalence of hypertension (32.5%), hyperlipidemia (29.3%), obesity (23.4%), and DM (18.4%) was observed among COVID-19 patients. Regarding geographical region, the highest prevalent of comorbidity was identified in North America (75.2%), followed by Europe (50.9%). Administrators, stakeholders, and healthcare professionals will be able to make more informed clinical decisions regarding COVID-19 patients with comorbidities with the assistance of the current meta-analysis.
Footnotes
Ethics approval
This systematic review and meta-analysis does not have direct or indirect involvement of human or animal. So, Ethical Approval from IRB was non-applicable.
Author contributions
BZ conceptualization and methodology; BZ, NT collect and curate the data; BZ analyze and interpretation; BZ, NT wrote the original draft; BZ wrote the review and edited.
Funding
None
Declaration of conflicting interests
The authors declare that they have no competing interests
Data Availability Statement
All data generated during this study are will be made available on corresponding author upon reasonable request.