
Abstract
Introduction
There were different studies done and found a highly variable level of COVID 19 prevention practice; however, there was no summarized evidence on the prevention practice of chronic disease patients in Ethiopia. This systematic review and meta-analysis aims to assess the pooled prevalence of COVID 19 prevention practice and associated factors among chronic disease patients in Ethiopia.
Method
Systematic review and meta-analysis were conducted using PRISMA guidelines. Comprehensive literature was searched in international databases. A weighted inverse variance random effect model was used to estimate pooled prevalence. Cochrane Q-test and I2 statistics were computed to assess heterogeneity among studies. Funnel plot and Eggers test were done to assess publication bias. Review manager software was used to identify determinants of COVID 19 prevention practice.
Result
Overall, 437 articles were retrieved and finally 8 articles were included in this review. The pooled prevalence of good COVID 19 prevention practices was 44.02% (95%CI (35.98%–52.06%). Being rurally reside (AOR = 2.39, 95% CI (1.30–4.41)), having educational status of cannot read and write (AOR = 2.32, 95% CI (1.22–4.40)), and poor knowledge (AOR = 2.43, 95% CI (1.64–3.60)) positively associated with poor practice.
Conclusion
Good COVID 19 prevention practices of chronic disease patients in Ethiopia was low. Rural residence, educational status of cannot read and write and poor knowledge was positively associated with poor practice. Therefore, policymakers and program planners should target those high-risk groups in improving their awareness to enhance their practice specifically focusing on those who are rural reside and with low educational status.
Keywords
Introduction
The 2019 Novel Corona Virus Disease is caused by the Severe Acute Respiratory Syndrome Corona Virus 2 and spread to many countries. 1 On January 30, 2020, the World Health Organization’s Emergency Committee considered it a global health emergency and declared it to be a pandemic in March 2020. 2 It was first identified as clusters of pneumonia cases that have been reported for unknown reasons in Wuhan, Hubei Province, China. 3
COVID-19 morbidity ranges from mild respiratory illness to severe complications characterized by acute respiratory distress syndrome (ARDS), septic shock, and other metabolic and hemostasis disorders and death.4–6 Most of the fatal cases and severe illnesses occurred in older adults and people who have underlying medical comorbidities like diabetes, cancer, hypertension, heart, lung, and kidney diseases.7–9 A systematic review of COVID-19 patients showed that individuals with hypertension, diabetes and cardiovascular and respiratory system diseases were the most vulnerable groups. 10 A large observational report, which was conducted on 1099 patients with COVID 19, showed that out of 173 patients with severe disease 23.7% had hypertension and 16.2% had DM. 11 Another study that recruited 52 severe COVID-19 patients indicated that out of 32 non-survived patients, 7 (22%) were DM patients. 12
Despite vaccines being prepared and distributed, there was no effective anti-viral drug to cure COVID 19 globally which was approved by WHO. Thus, patients with COVID 19 are being treated symptomatically. 13 WHO recommended Wearing a facemask, social distancing at least 1 meter, hand washing with soap and water, use of alcohol-based hand sanitizer, avoiding touching mouth, nose, and eye with unwashed hands, covering mouth and nose during coughing and sneezing, self-isolation during the feeling of sick and avoiding spending time in crowded places or in groups as modalities for COVID 19 prevention.14–16 Those Primary prevention strategies are practical and the best alternatives in resource-limited countries like Ethiopia. 17 However, these recommendations, which were hosted, to slow the spread of COVID 19 are unluckily neglected or deliberately ignored by some individuals. 18
Even though there is a strong recognition of public health importance of the prevention of COVID 19 by the Ethiopian government, there is still a need to emphasize on practice prevention measures to stop the nationwide spread of the virus. So far, in Ethiopia, different studies have been done on the practice of COVID 19 preventive measures among chronic disease patients and found a highly variable level of practice across the regions of the country.19–26 Up to the level of our knowledge, there is no systematic review and meta-analysis done in Ethiopia which can settle controversies arising from apparently conflicting individual studies on the prevention practice of chronic disease patients in Ethiopia; despite they are the main focus of intervention which increase the need to summarize the issue and intervene accordingly. Thus, this systematic review and meta-analysis aimed to assess the pooled prevalence of COVID 19 prevention practice and identify its associated factors among chronic disease patients in Ethiopia. The evidence from this systematic review and meta-analysis can be used for planning and implementation of an intervention to improve COVID 19 prevention practice among chronic disease patients. It identifies the important factors that are associated with COVID 19 preventive practice, therefore it contributes evidence input for preparing messages and materials for outreach and media campaigns to prevent and control COVID 19. This study can also serve as a baseline comparison since there is no systematic review and meta-analysis done on COVID 19 prevention practice of chronic disease patients globally. In addition, it may ignite a new insight for further studies that might be conducted on related topics.
Method
Study design and setting
A systematic review and meta-analysis were conducted on COVID 19 prevention practice among chronic disease patients in Ethiopia. Preferred Reporting Items for Systematic Review and Meta-Analysis guidelines were used (Supplementary Table 1). PRISMA is a protocol consisting of checklists that guide the conduct and reporting of systematic reviews and meta-analyses, which increase the transparency and accuracy of reviews in medicine and other fields. 27 Ethiopia is one of the low-income countries located in the horn of Africa with 2022 projected population of 123.4 million, 133.5 million in 2032 and 171.8 million in 2050. 28 For administrative purposes, Ethiopia is divided into 11 regions and 2 city administrations. Regions are further classified into zones, and zones are divided into districts. Finally, districts are divided into kebele (the smallest administrative division contains 2000 up to 3500 residents).
Search strategies and sources of information
We have checked the PROSPERO database (http://www.library.ucsf.edu/) and the resources on COVID-END (COVID-END) whether published or ongoing projects exist related to the topic to avoid any further duplication. Thus, the findings revealed that there were no ongoing or published articles in the area of this topic. Then this systematic review and meta-analysis was registered in the PROSPERO database with Id no of CRD42022322371. Comprehensive literature was searched using international databases PubMed, Google scholar, and African Online Journal to retrieve related articles from March 11 to 20, 2022. Grey literature was searched using Google. Search terms were formulated using PICO guidelines through the online databases. Medical Subject Headings (MeSH) and key terms had been developed using different Boolean operators ‘AND’ and ‘OR’. The following search term was used: “COVID-19 prevention practice” OR “COVID-19 response” AND “chronic disease patients” OR “hypertension and/or diabetes mellitus” AND Ethiopia.
Eligibility criteria
Studies that meet the following criteria are included in this systematic review. Studies that report the prevalence of COVID-19 prevention practice of chronic disease (diabetes mellitus, hypertension and HIV/AIDS) and its determinants in the English language, with out restriction in race, gender, or publication date (utill the last search day March 20, 2022) were included. Articles without full abstracts or texts and articles reported out of the outcome interest were excluded. Citations without abstracts and/or full-text, commentaries, anonymous reports, letters, editorials, reviews, and meta-analyses were excluded at each respective stage of screening.
Outcome measurements
This study has two main outcomes. The primary outcome was the prevalence of good COVID-19 prevention practice. It is defined as the proportion of participants who have good practice of the recommended COVID 19 prevention measures. Therefore, all included studies asked the study participants about the practice of each COVID 19 prevention strategies and categorized as good and poor. Thus, the response was analyzed and presented as the prevalence of good COVID 19 prevention practice. The secondary outcome was determinants of COVID-19 prevention practice.
Data extraction
All studies obtained from the considered databases were exported to Endnote version X8 software to remove duplicate studies. Then after, all studies were exported to a Microsoft Excel spreadsheet. All authors independently extracted the important data using a standardized data extraction form which was adapted from the Joanna Briggs Institute (JBI) data extraction format. For the first outcome (prevalence) the data extraction format included (primary author, year of publication, regions, study area, sample size, and prevalence of good COVID 19 prevention practice with 95% CI). We extracted data for the second outcome (associated factors of COVID 19 prevention practice) using a 2 by 2 table format. Finally, the log odds ratio for each factor was calculated using Review Manager (RevMan) software 5.4.
Quality assessment
To assess the quality of each study included in this systematic review and meta-analysis, the modified Newcastle Ottawa Quality Assessment Scale for cross-sectional studies was used 29 (Supplementary Table 2). Three Authors (AZ, AW, and TS) assessed the quality of each study (i.e. methodological quality, sample selection, sample size, comparability and the outcome, and statistical analysis of the study). In the case of disagreement between three authors; another three authors (AWK, EM, and MAZ) were involved and discussed and resolved the disagreement.
Data processing and analysis
The extracted Microsoft Excel spreadsheet format data was imported to STATA version 14 for analysis. Then weighted inverse variance random effect model was used to estimate the pooled prevalence of COVID 19 prevention practice in Ethiopia. Cochrane Q-test and I2 statistics were computed to assess heterogeneity among all studies. Accordingly, if the result of I2 is 0% to 40% it is mild heterogeneity, 40 to 70% would be moderate heterogeneity, and 70 to 100% would be considerable heterogeneity. 30 Funnel plot and Eggers test were done to assess publication bias. The p-value >0.05 indicated that there was no publication bias. Subgroup analysis was done based on the study region. Forest plot format was used to present the pooled prevalence of COVID 19 prevention practice with 95%CI. To identify determinants of COVID 19 prevention practice, we have used review manager software.
Patient and public involvement
In this study, neither patient nor the public was involved in the study design, conduct, reporting, or dissemination plans of our research.
Result
Overall, 437 articles were retrieved using our search strategy. International databases; PubMed, Google scholar, and African Journals Online were searched. Duplicates (249) were removed and 188 articles remained. After reviewing, (n=122) articles were excluded by title, and (n=31) articles were excluded by reading abstracts. Therefore, 35 full-text articles were accessed and assessed for inclusion criteria, resulting in the further exclusion of 27 articles due to the listed reasons. As a result, 8 studies fulfilled the inclusion criteria to undergo the final systematic review and meta-analysis (Figure 1). Flow chart of selection for systematic review and meta-analysis on COVID 19 prevention practice and its determinant among chronic disease patients in Ethiopia, 2022.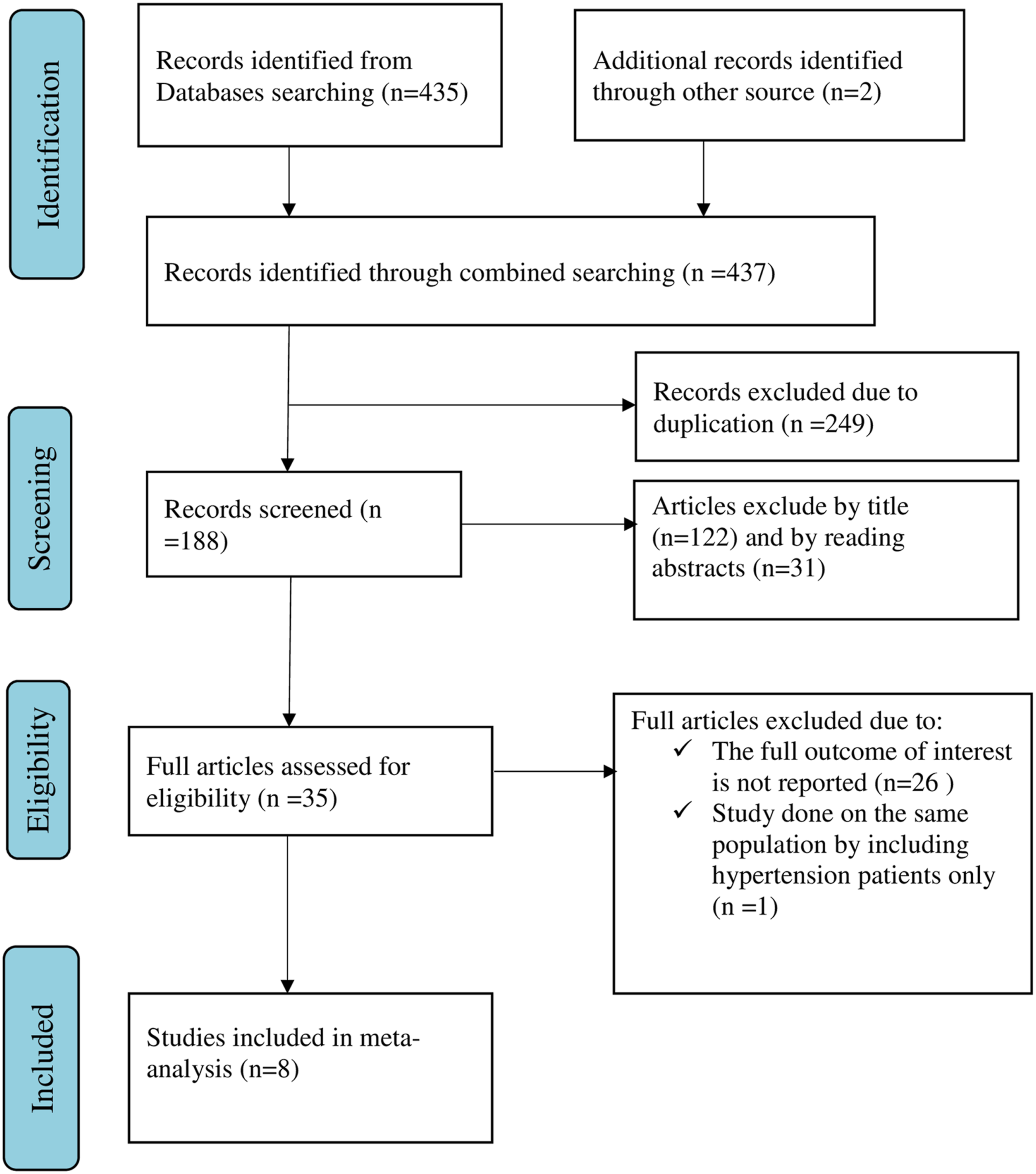
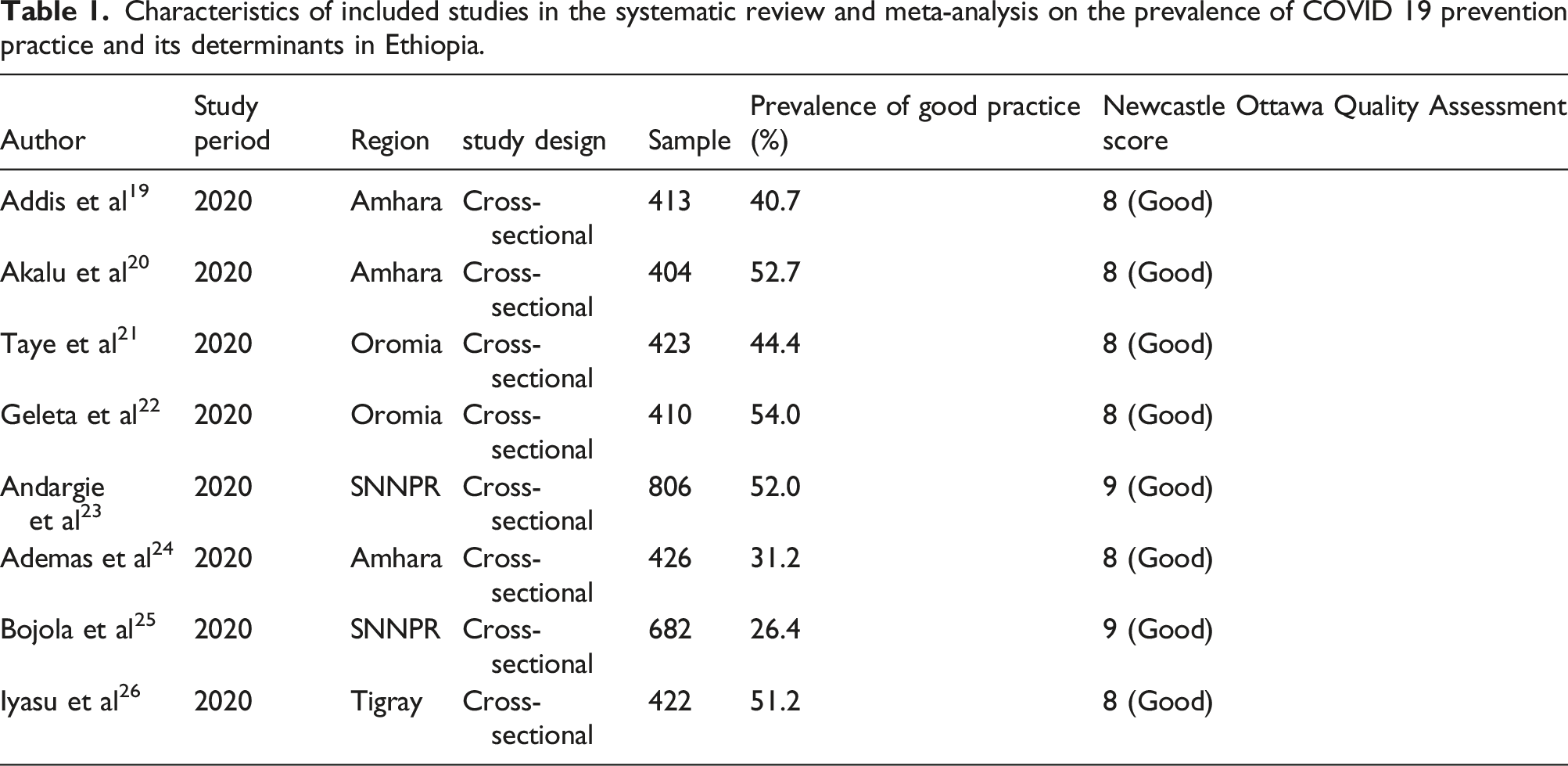
Characteristics of included studies in the systematic review and meta-analysis on the prevalence of COVID 19 prevention practice and its determinants in Ethiopia.
COVID 19 prevention practice of chronic disease patients in Ethiopia
The pooled prevalence of good COVID 19 prevention practice among chronic disease patients in Ethiopia was 44.02% (95%CI; 35.98%-52.06%), with the Cochrane heterogeneity index (I2 = 96.5%), P = 0.000, showing substantial heterogeneity of different studies (I2>50%). The finding was presented using a forest plot (Figure 2). The Pooled prevalence of good COVID 19 prevention practice among chronic disease patients in Ethiopia, 2022.
Publication bias
In this systematic review and meta-analysis, a funnel plot was done to check the presence of publication bias at a significance level of less than 0.05. The Egger’s regression test was not statistically significant P = 0.227 (p > 0.05) confirming no evidence of publication bias, as presented by the funnel plot (Figure 3). Funnel plot showing the symmetric distribution of articles on COVID 19 prevention practice among chronic disease patients in Ethiopia, 2022.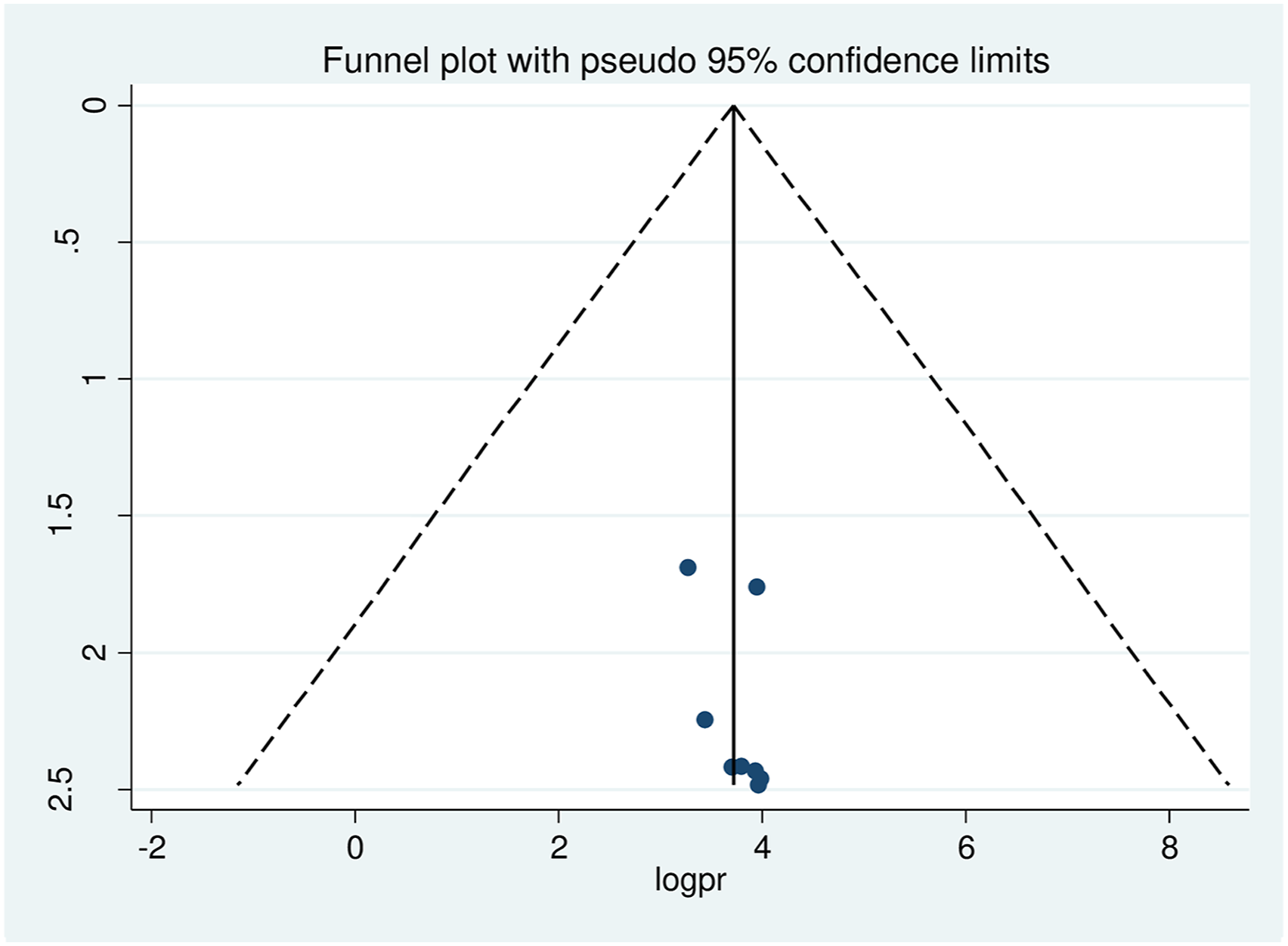
Subgroup analysis of COVID 19 prevention practice of chronic disease patients
The finding of subgroup analysis by region showed that the pooled prevalence of good COVID 19 prevention practice among chronic disease patients was highest in the Tigray region (51.18%; 95% CI: (46.42-55.95), I2 = 0%, p = 1), followed by Oromiya (49.08%; 95% CI: (45.71-52.46), I2 = 86.7%, p = 0.006), then Amhara (40.82%; 95% CI: (38.13-43.51), I2 = 95.2%, p = 0.000) and least SNNPR (38.65%; 95% CI: (36.27-41.04), I2 = 99.1%, p = 0.000) (Figure 4). forest plot showing Subgroup analysis of COVID 19 prevention practice and its determinant factors among chronic disease patients by region in Ethiopia, 2022.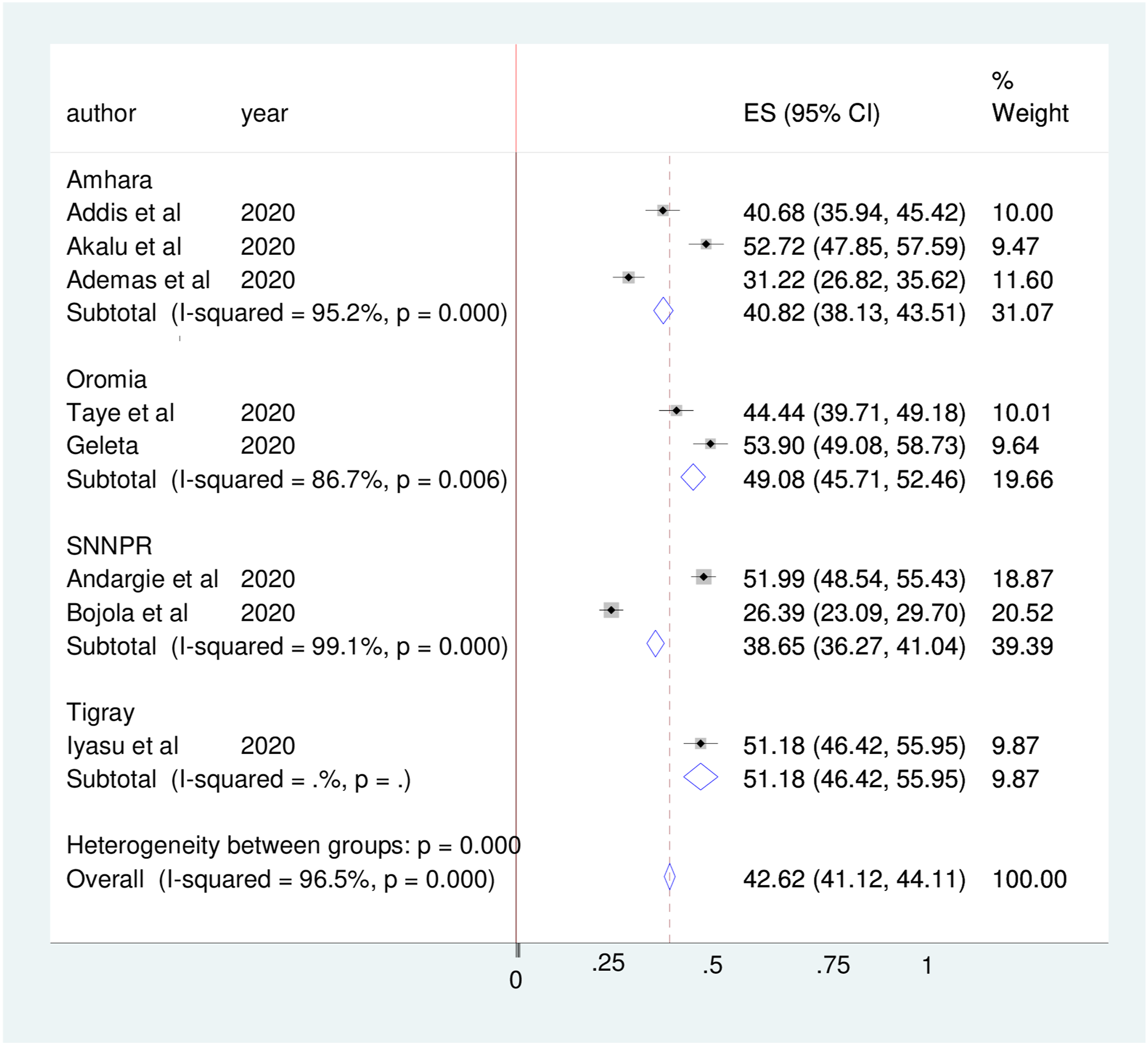
Sensitivity analysis
A random-effect model result showed that; no single study has influenced the overall pooled prevalence of COVID 19 prevention practice among chronic disease patients in Ethiopia (Figure 5). Sensitivity analysis of the prevalence of COVID 19 prevention practice and its determinant factors among chronic disease patients in Ethiopia, 2022.
Determinants of COVID 19 prevention practice among chronic disease patients
Factors associated with COVID 19 prevention practice among chronic disease patients in Ethiopia.

Discussion
COVID 19 is a highly contagious disease; a person can be infected after contact history with a known corona virus-infected person or from any other unknown source of infection.31–33 COVID 19 patients with chronic diseases were more likely to experience severe symptoms and faced a higher risk of mortality. They have also a high chance of being infected in case of contact with a possible source of infection. As a result, chronic disease patients are expected to follow the standard COVID 19 prevention precaution even with slowed transmission rate in the community. 34 Primary prevention strategies are practical and the best alternatives in resource-limited countries like Ethiopia for chronic disease patients as well as for the general population. 17 The poor practice of those primary prevention measures among the populations especially vulnerable groups like chronic disease patients may contribute to the further spread of the pandemic. 35
Ethiopia is one of the Sub-Saharan African countries which are severely affected by the COVID 19 pandemic and the pandemic imposed physical and psychological problems among chronic disease patients. 36 This systematic review and meta-analysis assessed the pooled prevalence and determinants of COVID 19 prevention practice among chronic disease patients in Ethiopia. The pooled prevalence of good COVID 19 prevention practice among chronic disease patients was 44.02% (95%CI; 35.98%-52.06%). The finding was consistent with SRMA done in Ethiopia by Abebaw Gedef Azene et al (41.62%) 37 and Birhaneselassie Gebeyehu Yazew et al (52.83%). 38 However, the finding is lower than SRMA done in Ethiopia among health professionals in which the pooled prevalence of good COVID 19 prevention practice was 59.7%. 39 It is also much lower than SRMA done by Bhagavathula and his colleagues in which the pooled prevalence of good COVID 19 prevention practice was 73%. 17 The discrepancy from the former study (SRMA in Ethiopia) might be due to the difference in the study population and study period. Since the previous SRMA was conducted on health professionals and at the beginning of COVID 19 pandemic and everybody had given attention to prevention measures and good prevention practice is higher in that SRMA. 37 The discrepancy from SRMA done by Bhagavathula and his colleagues may be due to socio-demographic differences; since the former study is global which includes the developed nation that makes the prevalence of prevention practices is high. This finding implies that a strong effort should be made to increase the COVID 19 prevention practice of chronic disease patients so as to decrease their morbidity and mortality that resulted from the pandemic.
In this SRMA, subgroup analysis by region showed that good COVID 19 prevention practice among chronic disease patients was higher in the Tigray region (51.18% followed by Oromiya (49.08%) then Amhara (40.82%) and least SNNPR (38.65%). This finding is consistent with SRMA done by Birhaneselassie Gebeyehu Yazew et al in which their sub-group analysis by region revealed that good COVID 19 prevention practices among the general population were higher in the Tigray region. 38 This finding suggests that a special focus should be given to chronic disease patients in SNNPR to increase their COVID 19 prevention practice.
Regarding determinants of COVID 19 prevention practice, this SRMA found that chronic disease patients from the rural residence were 2.39 times more likely to have poor COVID 19 prevention practice as compared to urban dwellers. This finding is similar to a national study in which being a rural resident has a probability of 43.0% not practicing COVID-19 prevention. 40 This finding implies effort should be made to increase COVID 19 prevention practices of chronic disease patients by specifically targeting rural dwellers.
Our SRMA also revealed that Patients having an educational status of cannot read and write were 2.32 times more likely to have poor COVID 19 prevention practice as compared to patients having secondary and above education. This finding is consistent with a study on COVID 19 prevention practice in a low-resource African setting in which, having no formal education is associated with poor practice. 41 This finding may have resulted from a lack of awareness about the pandemic among patients who cannot read-write; which makes them have poor COVID 19 prevention practices.
In this SRMA we have found that chronic disease patients having poor knowledge about COVID 19 were 2.43 times more likely to have poor COVID 19 prevention practice as compared to patients having good knowledge. This finding is similar to several studies done in Ethiopia in a different population42–45 and a large-scale study in Indonesia 46 in which knowledge was positively associated with COVID 19 prevention practice. This finding implies while we increase our patient's knowledge regarding COVID 19 it will improve their prevention practice; so we should strengthen our effort to increase knowledge of chronic disease patients so as to improve their practice.
Not standing with its finding, this SRMA has limitations. First, there were limited studies to include (eight) in this SRMA. The absence of a similar previous study makes it difficult to compare our findings with other findings. Finally, our search strategy found limited studies especially no studies from Addis Ababa, Dire Dawa, Afar, Gambella, Sidama, Hariri, Somali and Benishangul-Gumuz regions and this calls into question the national representativeness of our study.
Conclusion
The pooled prevalence of good COVID 19 prevention practice of chronic disease patients in Ethiopia was low, which indicates focused and carefully planned intervention should be designed and implemented to raise the magnitude of good prevention practice so as to prevent and control the pandemic and decrease their morbidity and mortality. Rural residence, educational status cannot to read and write and poor knowledge was positively associated with poor COVID 19 prevention practice. Good COVID prevention practice among chronic disease patients is crucial to prevent the pandemic and decrease its fatal consequences. Therefore, policymakers and program planners should target improving public awareness and in turn enhance COVID 19 prevention practice.
Supplemental Material
Supplemental Material - COVID 19 prevention practice of patients with known chronic illness in Ethiopia: A systemic review and meta-analysis
Supplemental Material for COVID 19 prevention practice of patients with known chronic illness in Ethiopia: A systemic review and meta-analysis by Amare Zewdie, Ayenew Mose, Tadesse Sahle, Abebaw Wasie Kasahun, Elyas Melaku and Melkamu Aderajew Zemene in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - COVID 19 prevention practice of patients with known chronic illness in Ethiopia: A systemic review and meta-analysis
Supplemental Material for COVID 19 prevention practice of patients with known chronic illness in Ethiopia: A systemic review and meta-analysis by Amare Zewdie, Ayenew Mose, Tadesse Sahle, Abebaw Wasie Kasahun, Elyas Melaku and Melkamu Aderajew Zemene in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgement
We would like to thank all authors of the primary studies which are included in this systematic review and meta-analysis.
Author contributions
AZ conceived the idea and participated in data extraction, analysis, and draft writing. AM, TS AWK, EM, and MAZ participated in the data extraction, analysis, preparation of the manuscript, and revision. All authors read and approved the final version of the manuscript to be considered for publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional review board statement
Not applicable. This systematic review and meta-analysis used and analyzed information obtained from pre-existing studies.
Availability of data and materials
The result of this SRMA was extracted from the data gathered and analyzed based on the stated methods and materials. All the relevant data are within the paper.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.