
Abstract
Background
Heart failure (HF) is a leading cause of hospitalization and mortality, and it poses a significant burden on healthcare systems globally. Obesity is a considerable risk factor for HF and contributes to increased cardiac stress and metabolic demands.
Methods
Data from the CDC WONDER database were examined from 1999-2020 for HF and HF with obesity-related mortality in adults aged 25 years and older at the time of death, using ICD-10 codes. Age-adjusted mortality rates (AAMR) per million persons were calculated.
Results
From 1999 to 2020, the overall AAMR for HF-related deaths in adults declined from 1627 to 1544 (AAPC: −0.49, 95% CI: −0.63 to −0.34), whereas AAMR for HF and obesity rose steadily from 10.7 in 1999 to 42.1 in 2020 (AAPC: 6.23, 95% CI: 5.50 to 6.82). The overall HF-related AAMR for both genders decreased from 1999 to 2020, with a more significant decline in women. In contrast, HF and obesity-related AAMRs significantly increased for both genders, with a more pronounced rise in men. HF-related AAMRs decreased for Whites, Hispanic or Latinos, and Asian/Pacific Islanders but increased statistically insignificantly for Black/African Americans and American Indian/Alaska Natives. HF and obesity-related AAMRs increased across all races from 1999 to 2020, with an overall AAPC of 6.23. The highest HF-associated mortality and HF and obesity-related rates were observed in the Midwest.
Conclusion
Overall, a declining trend in HF-related mortality could be seen. However, the increasing HF-obesity mortality despite a general decrease in HF death is concerning.
Introduction
Heart failure (HF) remains a leading cause of morbidity and mortality in the United States, with notable variations in mortality rates influenced by demographic factors such as age, race, gender, and geographic region. 1 Recent studies have underscored the critical role of comorbidities such as obesity in exacerbating HF outcomes. Obesity, a growing epidemic in the US, exacerbates the risk and severities of HF. Individuals with obesity are at a higher risk for developing HF due to the associated metabolic and cardiovascular stresses. The intersection of HF and obesity not only complicates disease management but also significantly influences mortality trends. Approximately 33% of the adult population is at risk for HF, with obesity being a key contributing factor. 2 Obesity is not only a significant risk factor for developing HF but also complicates its progression, leading to higher mortality rates.3,4 It is estimated that 11% of HF cases in men and 14% in women are connected to obesity. Due to an increased susceptibility to other HF risk factors or by causing hemodynamic and myocardial alterations that result in cardiac dysfunction, obesity may cause HF. There are cases of direct cardiac lipotoxicity, in which the buildup of lipids in the heart causes cardiac dysfunction that other HF risk factors cannot explain.. 5 Approximately 6.7 million Americans over age 20 have HF, with projections indicating this will rise to 8.5 million by 2030. The lifetime risk of developing HF is 24%, affecting about 1 in 4 individuals. HF prevalence is exceptionally high among the Black and Hispanic populations, who also face increasing mortality rates, especially in younger adults and those in rural areas. 6
The present study uses comprehensive Centers for Disease Control and Prevention (CDC) surveillance data to analyze and compare the trends and disparities in HF vs HF with obesity-related mortality in US adults from 1999 to 2020.
Methods
Study design
The mortality data were obtained from the death certificate information retrieved from multiple cause-of-death files using the Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research (CDC WONDER). 7 We extracted data from 1999 to 2020 for HF and HF with obesity-related mortality using codes from the International Classification of Diseases-10th Revision (ICD-10): I50 for HF and E66.0-E66.9 for obesity.8,9 The code I50 reliably identifies HF with reduced ejection fraction (EF) and HF with preserved EF using 50% EF as a cut-off with a high positive predictive value. 10 Obesity-related ICD-codes can also accurately identify patients with obesity in epidemiologic studies. 11 Hence, the codes used were accurate and reliable, giving valid results.
The dataset included cause-of-death information extracted from death certificates spanning all 50 states and the District of Columbia. Utilizing the Multiple Cause-of-Death Public Use record of death certificates, this study focused on identifying deaths attributed to both HF and HF with obesity. Such deaths were defined as those instances where HF and HF with obesity were concurrently reported anywhere on the death certificate, either as contributing factors or underlying causes of death.
This study exclusively included data from adults aged 25 years and older at the time of death. Institutional review board (IRB) approval was not sought because our research exclusively employed de-identified government-issued publicly available datasets readily available on the CDC website. Additionally, to uphold transparency and methodological robustness, the study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for reporting. 12
Data extraction
Data were extracted regarding population size, year of occurrence, geographical regions of demise, socio-demographic characteristics, urban-rural stratification, regional delineation, and state-specific categorization. Socio-demographic variables encompassed sex, age distribution, and racial and ethnic composition. In contrast, the spatial context of mortality encompasses various healthcare settings, including medical facilities (outpatient, emergency room, inpatient, death on arrival, or status unknown), home, hospice, and nursing home/long-term care facilities. Racial and ethnic classifications included Non-Hispanic (NH) White, NH Black or African American, Hispanic or Latino, NH American Indian or Alaskan Native, and NH Asian or Pacific Islander. These data are sourced from documented information on death certificates and have been previously utilized in analyses conducted on the WONDER. According to the U.S. Census Bureau definitions, regions were classified into Northeast, Midwest, South, and West.
Statistical analysis
To analyze national trends in mortality associated with HF and HF with obesity, the crude mortality rate per 1,000,000 was calculated. This was achieved by dividing the number of deaths attributed to HF and HF with obesity by the total population in the specified year. These rates were used to investigate mortality patterns concerning age groups, with a 95% confidence interval (CI) used for statistical analysis. The Age-Adjusted Mortality Rate (AAMR) was determined by applying mortality rates specific to different age groups to the age distribution of the year 2000 standard population in the US. This method allows for equitable comparisons of mortality rates across various populations or periods. AAMRs were utilized to examine mortality patterns overall and categorized by sex, race/ethnicity, census region, states, and metropolitan/nonmetropolitan areas.
To examine national annual trends in mortality related to HF and HF with obesity, the study utilized the Joinpoint Regression Program version 5.0.2. This software was employed to compute Annual percentage changes (APCs) and Average Annual Percentage Changes (AAPCs) in AAMR, along with 95% CIs. This methodology enabled the identification of temporal variations in AAMR by fitting log-linear regression models. Joinpoint models begin with the simplest structure the data allows and progressively add joinpoints up to a user-specified maximum. While this maximum is an upper limit, not all analyses will reach it. The APCs were categorized as increasing or decreasing if the slope representing the mortality change significantly deviated from zero, as determined by 2-tailed t-testing. Statistical significance was defined as a p-value of less than 0.05.
Results
Between 1999 and 2020, HF-related mortality accounted for a total of 6,755,700 deaths in U.S. adults aged ≥ 25 years With overall AAMR of 1414.1 (1413.1 – 1415.2)
Annual trends in AAMR
From 1999 to 2020, the overall AAMR for HF-related deaths in adults aged 25- 85+ declined from 1627 to 1544 (AAPC: −0.49, 95% CI: −0.63 to −0.34) (Supplemental Table 1a, 1b, 2). Specifically, a notable decrease occurred between 1999 and 2012 (APC: −2.19, 95% CI: −2.50 to −1.91), followed by a moderate increase from 2012 to 2020 (APC: 2.32, 95% CI: 1.84 to 2.93) (Figure 1(a)). For 25-44 years of age, the overall AAMR for HF-related deaths increased from 29.3 in 1999 to 53.3 in 2020; it decreased from 1999-2012 (APC: −0.35, 95% CI: −0.85 to 0.15); increased till 2018 (APC: 4.97, 95% CI: 2.9 to 7.07); significantly spiked from 2018-2020 (APC: 15.56, 95% CI: 7.31 to 24.43) (Figure 2(a)). For 45-64 years of age, the overall AAMR increased from 319.9 in 1999 to 448.3 in 2020; decreasing from 1999 to 2011 (APC: −1.80, 95% CI: −1.99 to −1.60); increasing till 2018 (APC: 4.28, 95% CI: 3.78 to 4.8) and then sharply increasing from 2018-2020 (APC: 11.85, 95% CI: 9.07 to 14.71) (Figure 2(b)). For 65-85+ years of age the overall AAMR decreased from 7694.5 in 1999 to 6986.6 in 2020; it decreased exponentially from 1999 to 2011 (APC: −2.24, 95% CI: −2.52 to −1.97), then increased till 2020 (APC: 1.91, 95% CI: 1.36 to 2.46) (Figure 2(c)). (a) Overall and sex-stratified heart failure AAMRs per 1,000,000 in the United States, 1999 to 2020. (b) Overall and sex-stratified heart failure with obesity related AAMRs per 1,000,000 in the United States, 1999 to 2020. (a) Overall heart failure AAMRs per 1,000,000 in the United States, 1999 to 2020 – age group 25 to 44 years old. (b) Overall heart failure AAMRs per 1,000,000 in the United States, 1999 to 2020 – age group 45 to 64 years old. (c) Overall heart failure AAMRs per 1,000,000 in the United States, 1999 to 2020 – age group 65 to 85+ years old. (d) Overall heart failure with obesity related AAMRs per 1,000,000 in the United States, 1999 to 2020 – age group 25 to 44 years old. (e) Overall heart failure with obesity related AAMRs per 1,000,000 in the United States, 1999 to 2020 – age group 45 to 64 years old. (f) Overall heart failure with obesity related AAMRs per 1,000,000 in the United States, 1999 to 2020 – age group 65 to 85+ years old.
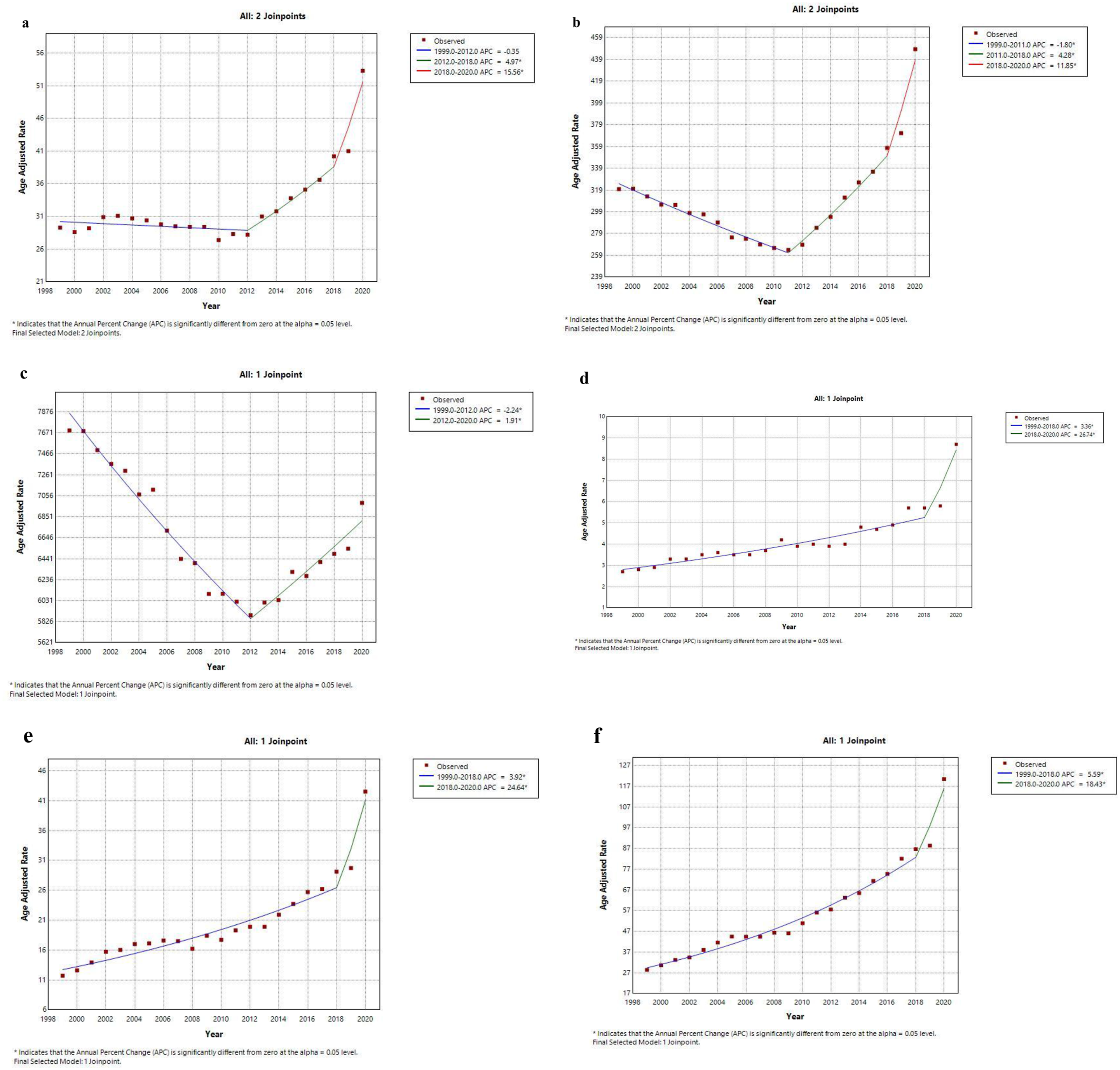
Conversely, rates for HF with obesity-related mortality rose steadily from 10.7 in 1999 to 42.1 in 2020 (AAPC: 6.23, 95% CI: 5.50 to 6.82) (Supplemental Table 1), with an increase from 1999 to 2018 (APC: 4.77, 95% CI: 3.90 to 5.48) and a sharper rise from 2018 to 2020 (APC: 21.19, 95% CI: 10.41 to 26.69) (Figure 1(b)). For 25-44 years of age, the overall AAMR for HF with obesity-related deaths increased from 2.7 in 1999 to 8.7 in 2020; it increased slowly from 1999 to 2018 (APC: 3.36, 95% CI: 2.78 to 3.94) followed by a steep incline till 2020 (APC: 26.74, 95% CI: 9.04 to 47.31) (Figure 2(d)). For 45-64 years old, the overall AAMR increased from 11.7 to 42.5 in years 1999-2020; trends showed a steady increase till 2018 (APC: 3.92, 95% CI: 3.32 to 4.53) before rising exponentially from 2018 to 2020 (APC: 24.64, 95% CI: 8.94 to 42.6) (Figure 2(e)). For age groups 65-85+ the overall AAMR from 1999 to 2020 increased exponentially from 28.4 to 120.4; the rise was steady till 2018 (APC: 5.59, 95% CI: 5.18 to 6.01) followed by a sharp increase from 2018 to 2020 (APC: 18.43, 95% CI: 9.42 to 28.19) (Figure 2(f)).
AAMR stratified by sex
Between 1999 and 2020, men had significantly higher HF-related AAMRs than women (Overall AAMR: Men: 1652, 95% CI: 1650-1654; Women: 1245, 95% CI: 1244-1246). This trend was similar for HF with obesity-related mortality rates (Overall AAMR: Men: 21.8, 95% CI: 21.6-22.0; Women: 19.7, 95% CI: 19.5-19.8) (Supplemental Table 4
The overall HF-related AAMR for both men and women decreased from 1999 to 2020, with a more significant decline in women (Men: AAPC: −0.26, 95% CI: −0.40 to −0.12; Women: AAPC: −0.83, 95% CI: −0.99 to −0.67). From 1999 to 2012, the AAMR decreased for both genders (Men: APC: −2.00, 95% CI: −2.30 to −1.73; Women: APC: −2.45, 95% CI: −2.78 to −2.16), followed by a significant increase until 2020 (Men: APC: 2.61, 95% CI: 2.11 to 3.21; Women: APC: 1.86, 95% CI: 1.27 to 2.56) (Figure 1(a), Supplemental Table 2).
In contrast, HF with obesity-related AAMRs significantly increased for both men and women from 1999 to 2020, with a more pronounced rise in men (Men: AAPC: 7.27, 95% CI: 6.57 to 7.86; Women: AAPC: 5.36, 95% CI: 4.59 to 5.95). Specifically, the AAMR for both genders showed a steep increase from 1999 to 2018 (Men: APC: 5.79, 95% CI: 4.95 to 6.53; Women: APC: 3.96, 95% CI: 3.01 to 4.66), which became even steeper until 2020 (Men: APC: 22.38, 95% CI: 12.02 to 27.56; Women: APC: 19.68, 95% CI: 8.41 to 25.55) (Figure 1(b), Supplemental Table 2).
AAMR stratified by race/ethnicity
Significant variability in HF-related deaths was observed among different racial/ethnic groups from 1999 to 2020. Overall, the HF-related AAMRs were highest among Black or African Americans, followed by Whites, American Indian or Alaska Natives, Hispanic or Latinos, and Asian or Pacific Islanders (Overall AAMR: Black or African American: 1531, 95% CI: 1527 to 1534; White: 1459, 95% CI: 1458 to 1460; American Indian or Alaska Native: 1335, 95% CI: 1319 to 1351; Hispanic or Latino: 93.1, 95% CI: 92.8 to 93.4; Asian or Pacific Islander: 64.1, 95% CI: 63.7 to 64.5) (Supplemental Table 3a). Similarly, the highest AAMRs for HF with obesity-related mortality were observed in Black or African Americans, followed by Whites and Hispanic or Latinos (overall AAMR: Black or African American: 33.7, 95% CI: 33.1 to 34.2; White: 20.6, 95% CI: 20.4 to 20.7; Hispanic or Latino: 12.7, 95% CI: 12.3 to 13.1) (Supplemental Table 3b).
From 1999 to 2020, HF-related AAMRs decreased for Whites (AAPC: −0.35, 95% CI: −0.48 to −0.23), Hispanic or Latinos (AAPC: −0.58, 95% CI: −0.88 to −0.35), and Asian or Pacific Islanders (AAPC: −0.73, 95% CI: −0.95 to −0.45). However, the AAMRs for Black or African Americans and American Indian or Alaska Natives showed a statistically insignificant increase (Black or African American: AAPC: 0.22, 95% CI: −0.07 to 0.44; American Indian or Alaska Native: AAPC: 0.18, 95% CI: −0.23 to 0.48). Conversely, HF with obesity-related AAMRs increased across all races from 1999 to 2020, with an overall AAPC of 6.23 (95% CI: 5.50 to 6.82). The increase was marked from 1999 to 2018 (APC: 4.77, 95% CI: 3.90 to 5.48), becoming even steeper until 2020 (APC: 21.1, 95% CI: 10.4 to 26.6) (Figure 3(a) and (b)). (a) Heart failure related AAMRs per 1,000,000 deaths for each race (Hispanics, American Indians, Whites, Asians, and Blacks) in the United States, 1999 to 2020. (b) Heart failure with obesity related AAMRs rate per 1,000,000 deaths for each race (Hispanics, Whites, and Blacks) in the United States, 1999 to 2020.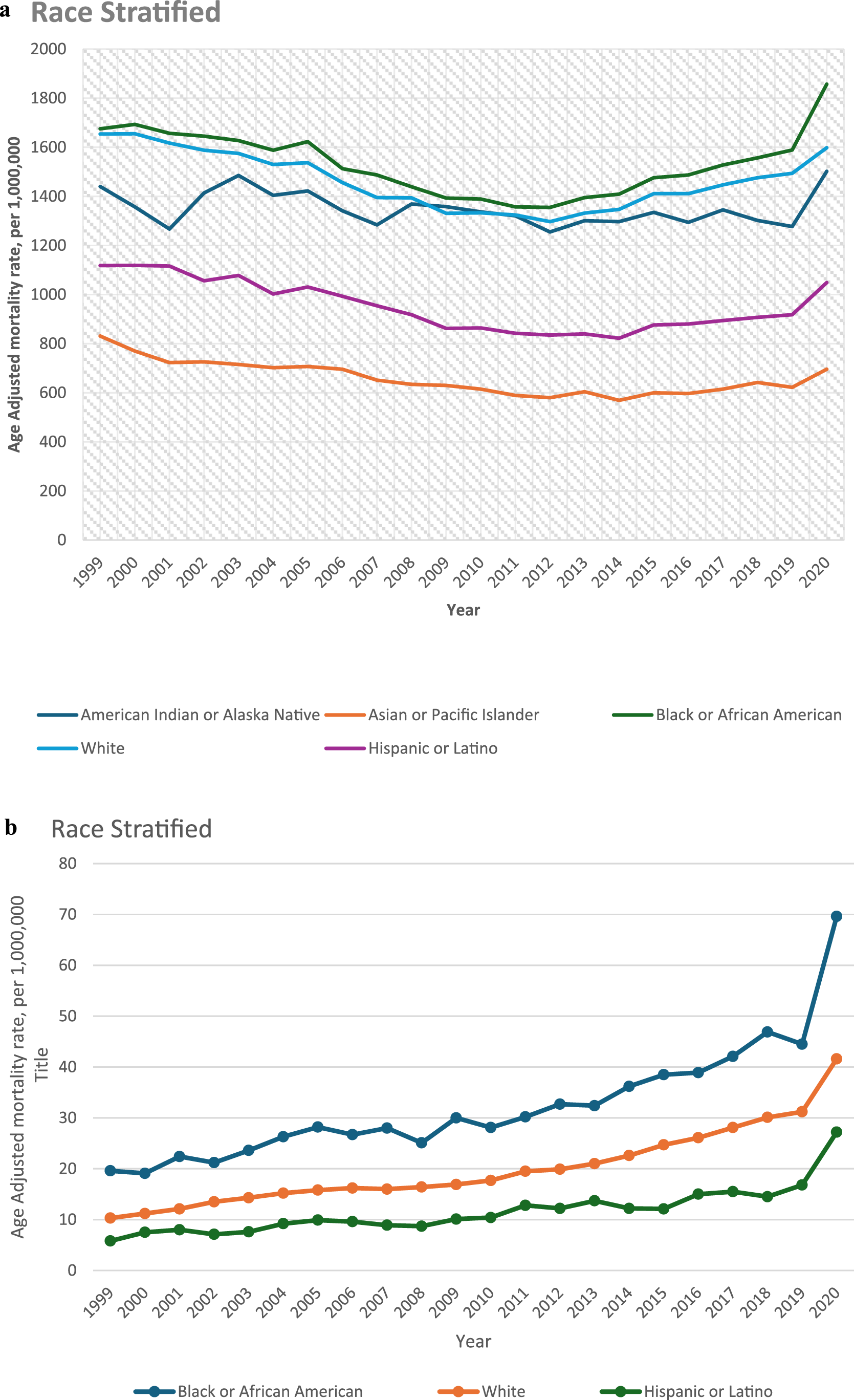
AAMR stratified by geographical regions
Census regions
From 1999 to 2020, highest HF-associated mortality rates were observed in the Midwest (AAMR: 1545, 95% CI: 1542 to 1547), followed by the South (AAMR: 1446, 95% CI: 1445 to 1448), the West (AAMR: 1336, 95% CI: 1333 to 1338), and the Northeast (AAMR: 1278, 95% CI: 1275 to 1280). Similarly, HF with obesity-related mortality rates were highest in the Midwest (AAMR: 23.19, 95% CI: 22.9 to 23.4), followed closely by the West (AAMR: 23.16, 95% CI: 22.8 to 23.4), then the South (AAMR: 21.2, 95% CI: 21.0 to 21.4), and the Northeast (AAMR: 14.5, 95% CI: 14.3 to 14.8) (Supplemental Table 5).
Overall, the AAMR associated with HF-related deaths declined in all the regions from 1999 to 2020 (Northeast: AAPC: −0.77, 95% CI: −0.94 to −0.59; Midwest: AAPC: −0.30, 95% CI: −0.50 to −0.10; South: AAPC: −0.49, 95% CI: −0.64 to −0.33; West: AAPC: −0.52, 95% CI: −0.76 to −0.28). Contrarily, throughout the study period, the AAMRs associated with HF with obesity-related deaths exhibited a steep incline in all the regions (Northeast: AAPC: 6.39, 95% CI: 5.80 to 6.94; Midwest: AAPC: 6.20, 95% CI: 5.53 to 7.00; South: AAPC: 6.35, 95% CI: 5.48 to 7.06; and West: AAPC: 5.34, 95% CI: 4.27 to 6.18) (Figures 4(a) and 4(b)). (a) Heart failure related AAMRs per 1,000,000 Stratified by Regions in the United States, 1999 to 2020. (b) Heart failure with obesity related AAMRs per 1,000,000 Stratified by Regions in the United States, 1999 to 2020.
Rural-urban classification
Nonmetropolitan areas consistently had higher AAMRs associated with HF-related deaths compared to the metropolitan areas from 1999 to 2020, with overall AAMRs of 1753 (95% CI: 1750 to 1756) and 1342 (95% CI: 1340 to 1343), respectively. A similar trend was observed for HF and obesity-related mortality rates, with nonmetropolitan areas having an overall AAMR of 29.6 (95% CI: 29.2 to 29.9) compared to 19.0 (95% CI: 18.9 to 19.2) in metropolitan areas (Supplemental Table 6).
Both nonmetropolitan and metropolitan areas exhibited significant declines in HF-related AAMRs from 1999 to 2020 (Nonmetropolitan: AAPC: −0.38, CI: −0.54 to −0.22; Metropolitan: AAPC: −0.52, CI: −0.64 to −0.38). Conversely, AAMRs associated with HF and obesity sharply increased in both nonmetropolitan and metropolitan areas over the same period (Nonmetropolitan: AAPC: 6.49, CI: 5.83 to 7.02; Metropolitan: AAPC: 6.24, CI: 5.57 to 6.83) (Figures 5(a) and 5(b)). (a) Heart failure related AAMRs per 1,000,000 Stratified by Urbanization in the United States, 1999 to 2020. (b) Heart failure with obesity related AAMRs per 1,000,000 Stratified by Urbanization in the United States, 1999 to 2020.
States
HF-related AAMRs varied significantly among U.S. states from 1999 to 2020, ranging from 869 (95% CI: 857 to 881) in Hawaii to 2335 (95% CI: 2321 to 2350) in Mississippi. States in the top 90th percentile for AAMRs included Arkansas, Kentucky, West Virginia, Oklahoma, and Mississippi, which had roughly double the AAMRs of states in the lower 10th percentile like Hawaii, Florida, District of Columbia, Arizona, and Nevada (Figure 6(a), Supplemental Table 7, 8 and 9a). Similarly, HF with obesity-related mortality rates also showed wide disparities, from an AAMR of 10.1 (95% CI: 9.5 to 10.7) in Massachusetts to 40.6 (95% CI: 38.9 to 42.2) in Oklahoma. States in the top 90th percentile included Mississippi, Wyoming, Oregon, Vermont, and Oklahoma, which had about twice the AAMRs of states in the lower 10th percentile, such as Massachusetts, Connecticut, Nevada, New York, and Florida (Figure 6(b), Supplemental Tables 8 and 9b). (a) Heart failure-related AAMRs per 1,000,000 Stratified by State, 1999 to 2020 Heat Map. (b) Heart failure with obesity related AAMRs per 1,000,000 Stratified by State, 1999 to 2020 Heat Map.
Interestingly, the top five states by AAMRs for HF and HF with obesity-associated mortality rates overlapped only in Mississippi and Oklahoma. Conversely, Nevada and Florida appeared in the bottom five states for both, suggesting that HF with obesity-related mortality rates do not strictly correlate with HF-related mortality rates alone. Figure 7 is a central illustration displaying mortality Trends in HF and HF with obesity in the United States from 1999-2020, with a further illustration of racial and geographical disparities (Figure 7). Central Illustration: Mortality Trends in HF and HF with obesity in the United States from 1999-2020, with a further illustration of racial and geographical disparities.
Discussion
HF is a significant public health concern in the United States, with rising mortality rates post 2012 after an initial decline from 1999 till 2011. There are differences according to age, race/ethnicity, and geography. Using data from CDC WONDER, we looked at mortality trends and differences in HF and HF with obesity mortality in the adult US population (1999-2020). The results show an alarming disparity. HF with obesity-related mortality increased considerably throughout the study period, while overall HF mortality declined in the USA. Our findings align with the studies done previously.13,14 Consistent with our results, previous studies showed a trend of HF mortality decreasing from 2000 to 2011 but increasing steadily till 2015; these findings were noted in both genders and all races except NH American Indians/Alaska Natives. 15 The post-2012 increase in HF-related mortality may be partially attributed to unintended consequences of the Hospital Readmissions Reduction Program (HRRP) implemented in 2012, which has been associated with increased mortality rates despite successfully reducing readmissions, as hospitals may have compromised patient outcomes to avoid readmission penalties.16,17 Additionally, the reversal of trend in HF-related mortality may represent a lack of management of potential chronic comorbidities leading to the development of HF. The Framingham Heart Study observed that the incidence of HF was significantly higher in patients with hypertension and that the increase in 1-unit BMI was attributable to 5-7% increase in HF risk.18,19 Similarly, diabetes mellitus was associated with an 80% increased risk of HF in the NHANES (National Health and Nutrition Examination Survey) Epidemiologic Follow-Up Study. 20 Also shown in previous studies is that the age-adjusted hospitalization rates and mortality rates for HF decreased steadily in the years 1991-2015. 21 These offer insights into the already established trends and help reinforce previously found patterns.
Our analysis reveals notable variations in death rates among both genders. These results display a significant divergence from the typical trend in healthcare research. Men continuously showed greater death rates than women in our investigation of HF mortality.22,23 This increase in gender difference may be explained by several cohort-specific characteristics, such as men’s higher prevalence of HF with lower ejection fraction, which is linked to worse outcomes. This observed discrepancy may be attributed to men’s higher incidence of comorbid conditions, specialized care, and hospital admissions.24,25 Race and ethnicity significantly influenced outcomes, with Black or African Americans experiencing the highest overall HF-related mortality rates, as observed in previous studies as well. 26 These disparities raise concerns about unequal access to healthcare and quality among different racial groups, warranting further exploration of contributing factors such as socioeconomic status and healthcare accessibility. 27
Geographically, the Midwest consistently demonstrated the highest mortality rates for both HF and HF with obesity, followed by the South. 28 Moreover, nonmetropolitan areas exhibited higher mortality rates compared to metropolitan regions, reflecting the challenges rural populations face in managing complex medical conditions like HF due to limited access to specialists and advanced medical care. 29 Studies reveal that African Americans living in rural regions are far less likely than those living in cities to get screenings for cervical cancer and cholesterol, which highlights a severe inequity of access to preventive healthcare. 30 In rural locations, especially in counties with a majority of African Americans, which are frequently designated as Health Professional Shortage locations, these inequities are exacerbated by higher rates of poverty and less access to healthcare. With only 18% of adults identifying as African American, Hispanic, or of another race, compared to 40% in urban regions, the rural population is likewise less racially and ethnically varied. The South has the highest percentage of rural respondents (41%). 31 Due to their higher rates of poverty and already restricted access to healthcare, African American communities are disproportionately affected by the closure of rural hospitals, which exacerbates existing disparities. 32
Our findings align with previous research on several vital aspects. For instance, similar to our results, Sciomer et al. reported significant disparities in HF outcomes based on sex and age, indicating worse outcomes for men. 33 Our findings regarding place of death are consistent with recent work by Ali et al., who observed a doubling of home-based deaths and a post-2017 decline in hospice deaths among HF patients across the United States. 34 Our results corroborate existing literature regarding the elevated HF-related mortality rates among Black or African Americans, often linked to disparities in healthcare access and quality. 35 Our analysis spans two decades, providing a quantitative perspective on HF and HF with obesity-related mortality trends, unlike other studies with a shorter timeframe or focus on specific regions. This broader scope enables a more detailed examination of demographic disparities. Our research exhibits a significant increase in HF with obesity-related mortality, demonstrating the expanding influence of the obesity epidemic on HF outcomes.
The obesity pandemic that is currently spreading in the United States is likely a major contributing factor, as obesity is a proven risk factor for HF. Obesity impacts heart function and myocardial infarction risk through hemodynamic changes, neurohormonal activation, and ectopic fat deposition, among other mechanisms. 36 Our study helps decode some of the relationship by reporting mortality trends over two decades in the US.
Our analysis of state-level data further reveals a complex relationship between mortality from HF and HF with obesity. States exhibiting high HF-related mortality rates do not always correspondingly show high rates of HF with obesity-related mortality, suggesting that distinct factors influence outcomes for each condition. 37 The contrasting trends in mortality rates necessitate further investigation into the demographic, ethnic, and geographic factors that underlie these patterns, aiming to develop targeted interventions to reduce death rates and address healthcare disparities. 38
Additionally, it is necessary to include the worldwide pandemic COVID-19 that might have potentially affected our AAMR trends during the years 2019-2020 in this discussion. Studies found that the rate of hospitalization due to HF decreased significantly in these years; but the length of stay and readmission rates in 30 days were prominently higher than average. 39 Additionally, it has been observed pre-existing heart failure increases the risk of a more severe clinical course of COVID-19 and eventual in-hospital mortality; also, COVID-19 noted in previous studies potentially causes acute de novo heart failure through myocardial injury triggered by an exaggerated inflammatory response.40,41 Furthermore, early months of the pandemic posed additional challenges, as limitations in COVID-19 testing and coding likely caused under-recognition of the virus’s contribution, which could have been misclassified as mortality associated to heart failure.42,43 Moreover, due to physical inactivity and sedentary lifestyle during the pandemic, the obesity rates increased exponentially. 44 These two facts combined could explain the trend we have noticed in our study that shows a sharper increase in HF with obesity-related mortality in the pandemic years.
Further studies should examine the fundamental causes of the increased mortality rates from HF with obesity, paying particular attention to regional and demographic differences. Longitudinal studies are crucial to assess the effects of obesity control programs on HF outcomes over time. Investigating how healthcare access and socioeconomic factors shape these patterns will also be critical. To guarantee equal access to high-quality healthcare, targeted measures must address the particular difficulties faced by communities living in nonmetropolitan areas.
Conclusion
Our study investigated HF-related mortality rate discrepancy based on age, race/ethnicity, and geography using a national dataset, correlating that with obesity mortality in the adult US population. We observed a higher mortality in male gender, black or African American population, non-metropolitan areas, and Midwest states. Our analysis indicated a significant link between HF and obesity, which is considered a public health concern. Notably, our temporal analysis revealed divergent mortality trends over the study period (1999-2020), with overall HF mortality initially declining but subsequently increasing after 2012, while HF-obesity mortality demonstrated a consistent upward trajectory throughout the entire study period. Based on these findings, we recommend implementing comprehensive obesity management strategies in HF care, including mandatory integration of structured weight loss interventions into HF treatment protocols and establishment of community-level obesity screening programs targeting high-risk regions, particularly non-metropolitan areas and states with elevated HF with obesity-related mortality rates. These evidence-based policy measures are essential to address the growing burden of HF with obesity-related mortality and reduce persistent health disparities. This study sheds light on the national trends over the last two decades, trying to guide healthcare policymakers to maintain their efforts towards an efficient and equitable system.
Limitations
Certain restrictions apply to this study. Dependence on CDC mortality data may result in omitting critical clinical variables, such as comorbidities or particular treatment approaches. Regarding the observed changes in HF and HF with obesity-related mortality, causal inferences are limited by the retrospective character of the investigation. The dataset for the years 1999-2020 was analyzed only and since newer data is available, we recommend future follow-up studies to assess whether the observed trends continued beyond this point. The data pool was taken from CDC WONDER’s Multiple Cause of Death section. Hence, it does not stratify HF and/or obesity based on underlying causes. Furthermore, any errors in death certificate reporting could impact the accuracy of death rates. Using ICD-10 code E66 could be insufficient in portraying the entire spectrum of obesity-related risk. It captures only those instances where obesity was documented explicitly, with consensus existing in the literature that ICD codes underreport the potential prevalence. 11 Lastly, large demographic categories may mask significant differences within specific subgroups. There was presence of suppressed or unreliable data due to low death counts in certain specific subgroups (Non-Hispanic American Indians and Non-Hispanic Asian) leading to exclusion from temporal analysis. Future research endeavors should incorporate more comprehensive datasets and examine these influential elements comprehensively.
Supplemental Material
Supplemental Material - Trends and disparities in heart failure and heart failure with obesity mortality among U.S. adults: A 1999–2020 analysis of geographic, gender, and racial variations using CDC WONDER data
Supplemental Material for Trends and disparities in heart failure and heart failure with obesity mortality among U.S. adults: A 1999–2020 analysis of geographic, gender, and racial variations using CDC WONDER data by Faizan Ahmed, Tehmasp Rehman Mirza, Sherif Eltawansy, Zaima Afzaal, Areeba Ahsan, Hira Zahid, Kainat Aman, Mushood Ahmed, Hritvik Jain, Abdullah Naveed, Omar Kamel, Aman Amanullah, Nisar Asmi, Farman Ali, Adnan Bhat, Paweł Łajczak, Ogechukwu Obi, Naveen Baskaran, Mian Zahid Khan Kakakhel, Ayesha Samad and Haitham Dib in Journal of Multimorbidity and Comorbidity.
Footnotes
Funding
This article received no specific grant from public, commercial, or not-for-profit funding agencies.
Declaration of conflicting interests
There is no conflict of interest to disclose.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article [and/or] its supplementary materials.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.