
Abstract
Objective:
To determine whether a bi-directional relationship exists between depression and HF within a single population of individuals receiving primary care services, using longitudinal electronic health records (EHRs).
Methods:
This retrospective cohort study utilized EHRs for adults who received primary care services within a large healthcare system in 2006. Validated EHR-based algorithms identified 10,649 people with depression (depression cohort) and 5,911 people with HF (HF cohort) between January 1, 2006 and December 31, 2018. Each person with depression or HF was matched 1:1 with an unaffected referent on age, sex, and outpatient service use. Each cohort (with their matched referents) was followed up electronically to identify newly diagnosed HF (in the depression cohort) and depression (in the HF cohort) that occurred after the index diagnosis of depression or HF, respectively. The risks of these outcomes were compared (vs. referents) using marginal Cox proportional hazard models adjusted for 16 comorbid chronic conditions.
Results:
2,024 occurrences of newly diagnosed HF were observed in the depression cohort and 944 occurrences of newly diagnosed depression were observed in the HF cohort over approximately 4–6 years of follow-up. People with depression had significantly increased risk for developing newly diagnosed HF (HR 2.08, 95% CI 1.89–2.28) and people with HF had a significantly increased risk of newly diagnosed depression (HR 1.34, 95% CI 1.17–1.54) after adjusting for all 16 comorbid chronic conditions.
Conclusion:
These results provide evidence of a bi-directional relationship between depression and HF independently of age, sex, and multimorbidity from chronic illnesses.
Keywords
Introduction
Depression and heart failure (HF) are highly prevalent chronic conditions. Depression affects over 350 million people worldwide and is currently the leading cause of disability from chronic illness. 1 HF affects approximately 5.7 million U.S. adults, and over 550,000 new cases of HF are diagnosed each year. 2,3 By 2030, it is estimated that more than 8 million Americans (1 in every 33 people) will have HF.
The co-occurrence of depressive symptoms or syndromes and cardiovascular disease, most notably coronary heart disease, is well-documented. 4 However, there is more limited data on the relationship between depression and HF. A meta-analysis of 27 observational studies found that the prevalence of depression in patients with HF ranges from 11% to 25% in outpatients and 35% to 75% in hospitalized patients, and appears to climb with increasing HF severity. 5 The importance of a depression-HF association rests in the observation that depression may result in greater functional decline, higher rehospitalization rates, and higher rates of premature death in patients with HF—including death by suicide. 6
Although depression is common in patients with HF, little information exists about the directionality of this relationship. Longitudinal studies have shown that depression may increase the risk of newly diagnosed HF, 7 –14 although others have shown no increased risk. 15,16 Longitudinal studies have also shown a significantly increased incidence of new-onset depression in people with HF, 17,18 thus documenting an association in the opposite direction. However, these findings are from separate cohorts. We are unaware of any large-scale cohort studies focused on the simultaneous investigation of the temporal association between depression and HF in a single cohort. To the best of our knowledge, there is no work to date that has leveraged longitudinal health record (EHR) data to study the associations between depression and HF.
We conducted an electronic health record (EHR)-based cohort study to test the hypothesis that, within a single community-based cohort, a bi-directional relationship exists between depression and HF. As an alternative to the use of clinical cohorts (which have good phenotyping but may lack sufficient sample size) and claims databases (which are large in size but have problems with case accuracy), we used EHRs with validated algorithms for identifying depression and HF. For depression, we considered the impacts of major depressive disorder and other depressive syndromes that are commonly encountered in routine treatment settings. 19,20 For HF, we investigated the association with new-onset depression—both overall, and in subgroups defined by preserved or reduced ejection fraction. 21
Methods
Study population
The study population consisted of patients 15+ years of age who were empaneled in Mayo Clinic (Rochester, MN) primary care practices (internal medicine, family medicine) for at least 1 month in calendar year 2006 (2006 Primary Care cohort). The 15+ years of age threshold was based on the average age of first onset of depression and on the rise in prevalence rates of non-congenital forms of HF beginning at age 15 years. 22,23 To ensure sufficient EHR data, eligible cohort members had to have at least one medical visit within 1.5 years after their index date and within the time frame between 1.5 years and 5 years before their index date. The Mayo Clinic Institutional Review Board approved the study prior to data collection.
Study cohorts
In order to examine the bi-directional association between depression and HF, two cohorts were extracted using EHRs from the health records of the 2006 Primary Care cohort members—a depression cohort and a heart failure cohort (see Figure 1). Each is described below, beginning with the depression cohort.

Study design and assembly of cohort of patients who received primary care in the Mayo Clinic (Rochester, MN) 2006 Primary Care cohort. EHR = electronic health records; HF = heart failure. a A total of 11,711 pairs of individuals who met the algorithm definition of depression and paired non-depressed referents were identified. Of 11,711 pairs, 161 were dropped due to inability to match on all parameters, 398 were dropped due to having a HF diagnosis on or within the 5 years preceding the index date (considered to have prevalent HF), and 646 were dropped due to having zero days of follow-up. A total of 143 pairs were added back after rematching, bringing the total number of pairs in the depression cohort to 10,649. b A total of 8,288 pairs of individuals who met the algorithm definition of HF and paired non-HF referents were identified. Of the 8,288 pairs, 270 were dropped due to inability to match on all parameters, 2,474 were dropped due to having a depression diagnosis on or within the 5 years preceding the index date (considered to have prevalent depression), and 317 were dropped due to having zero days of follow-up. A total of 684 pairs were added back after rematching, bringing the total number of pairs in the HF cohort to 5,911.
Depression cohort
A validated EHR-based algorithm that utilized a combination of natural language processing and diagnosis codes was applied to identify cases of depression. The case definition of depression required the presence of an ICD-9 diagnosis code (296.2[0–6], 296.3[0–6], 296.82, 298.0, 300.4, or 311) and a depressive disorder term (major depressive disorder, major depression, depressive disorder, depression, dysthymic disorder, persistent depressive disorder, depressive disorder not otherwise specified [NOS], depressive disorder not elsewhere classified [NEC]) in the EHR text. We did not require the presence of an antidepressant drug ingredient term in the EHR text or electronic prescription records given that many depressed patients do not require pharmacotherapy and can be effectively managed using evidence-based psychosocial treatments.
24,25
The EHR-based definition of depression was first validated in the Primary Care cohort using a random sample of EHRs from 100 unique patients (50 cases and 50 controls), using manual records review as a gold standard (PPV 0.76, NPV 1.0). The algorithm was then applied to the EHR data from all cohort members through December 31, 2018. For people with depression, the index date was defined as the first date during this time window on which the algorithm definition was met. People with depression were matched (by age
Heart failure cohort
An EHR-based algorithm was also applied to the 2006 Primary Care cohort through December 31, 2018, to identify people with HF (see Supplemental Table 1). The HF algorithm, which utilized ICD-9 diagnosis codes (ICD-9 428), mentions of HF diagnoses in electronic inpatient and outpatient clinical notes, and ejection fraction measurements within 6–12 months of a HF diagnosis date, was developed and then validated on a sample of 6,922 records from the Mayo Genome Consortium (MayoGC)/eMERGE cohort. 26 Using manual review of medical records, the HF algorithm had a PPV of 0.94. 26 Where EF data were available, the HF algorithm was also used to further classify people with HF as having preserved (HFpEF) and reduced ejection fraction (HFrER), as defined by an EF cutoff of 50%. 27,28 The index date for people with HF was the first date on which the HF algorithm definition was met. People with HF were matched by the same parameters as for the depression cohort with a 2006 Primary Care cohort member that did not have HF. For people without HF, the index date was defined using the same procedures as for the depression cohort.
Endpoints
For the depression cohort, the endpoint of interest was newly diagnosed HF using the EHR-based HF algorithm described above. For the HF cohort, the endpoint of interest was newly diagnosed depression using the EHR-based depression algorithm. Therefore, persons in the depression cohort with evidence of HF (using the EHR-based HF algorithm) and persons in the HF cohort with evidence of depression (using the EHR-based depression algorithm) in the 5 years preceding the index dates were excluded.
Follow-up
Members of the depression and HF cohorts were followed longitudinally using EHR data from their respective index dates until the first of the following dates: (a) the end of the study (December 31, 2018); (b) date of death; (c) date that one of the study endpoints was reached (newly diagnosed HF in the depression cohort or newly diagnosed depression in the HF cohort); or (d) the last follow-up date, defined as the date of the last primary care visit.
We computed a measure of completeness of follow-up for each cohort as a ratio of the total observed person-time and the total potential person-time, where potential person-time was the time from first medical visit until the event of interest, if one occurred, or the cut-off date where the latter was defined to be date of the last person in the cohort’s last medical visit. 29 For the depression cohort the measure of completeness was 82.1% (84.9% for depression cases and 79.7% for non-depressed referents); for the heart failure cohort, the measure of completeness was 92.1% (89.4% for HF cases and 85.8% for non-HF controls). Measures of completeness were 92.1% for the depression cohort and 104.5% for the HF cohort after reassigning the last date to 1 year earlier, indicating that much of the censoring occurred in the last year rather than being due to earlier loss to follow-up.
Covariates
Information on age at cohort entry, sex, education level, and self-reported race were retrieved electronically from the EHRs of all depression and HF cohort members. Education level was classified at seven levels: missing information on education, eighth grade or lower (or
Statistical analysis
Descriptive statistics were used to summarize the demographic and clinical characteristics of the study cohorts. The relationships between depression status at baseline and newly diagnosed HF during follow-up were assessed using marginal Cox proportional hazard models, beginning with univariable models. In the HF cohort, a similar approach was conducted to test the association between HF status at baseline and newly diagnosed depression during follow-up. Multivariable models were then fitted, adjusting for: (1) Charlson Comorbidity Index scores; (2) a subset of 16 comorbid chronic conditions that were selected using a step-wise approach (stepwise-adjusted model); and (3) all 16 chronic conditions and education level (fully adjusted model). For the HF cohort, fully adjusted marginal Cox modeling was repeated with follow-up time censored at 5 years, to investigate the impact of shorter survival time in HF patients on the HF-depression association. Stratified marginal Cox models were run to examine the risk of newly diagnosed depression in persons with HFpEF and HFrEF. All analyses were performed using SAS statistical software (version 9.4, Cary, NC: SAS Institute Inc.).
Results
Individuals with depression and newly diagnosed HF
The demographic and clinical characteristics of depressed cohort members and those without depression are summarized in Table 1. The depression cohort was predominantly middle-aged (mean age 49.5 years), Caucasian, and female. The mean duration of follow-up was similar between depressed and non-depressed cohort members (Table 1).
Characteristics of 10,649 people with depression and 10,649 people without depression in the 2006 Primary Care cohort.

There was no missing data for age, Charlson comorbidity index score, or sex; or for the 16 comorbid chronic illnesses.
a People with depression were matched with non-depressed 2006 Primary Care cohort members on age
b Refers to Charlson Comorbidity Index score (severity- and age-weighted sum of diseases).
c Unknown/missing race included 54 depressed cohort members and 172 non-depressed cohort who chose not to disclose their race.
d General equivalency degree (GED).
e Defined using International Classification of Diseases (ICD) and Hospital Adaptation of the International Classification of Diseases (HICDA) diagnosis codes, as shown in Supplemental Table 1.
In the depression cohort, there were a total of 1,418 individuals with depression and newly diagnosed HF, and 606 non-depressed individuals with newly diagnosed HF. There was a significantly higher risk of newly diagnosed HF in depressed cohort members (HR 2.36, 95% CI 2.15–2.58), as compared to people without depression (Table 2). As shown in Table 2, the risk of newly diagnosed HF in depressed cohort members remained high and statistically significant after adjusting for Charlson Comorbidity Index score.
Hazard ratios (HR) (95% CI) for the risk of newly diagnosed heart failure (HF) according to depression status in the 2006 Primary Care cohort.

The impact of depression on subsequent HF diagnosis was assessed using marginal Cox proportional hazard models.
a People with depression were matched with non-depressed 2006 Primary Care cohort members on age
b Comorbid conditions were defined using ICD-9, ICD-10, and HICDA diagnosis codes (see Supplemental Table 1). Covariates selected by step-wise algorithm included education level, hypertension, chronic pulmonary disease, atrial fibrillation, diabetes mellitus, cancer, osteoporosis, asthma, hyperlipidemia, dementia, hepatitis, chronic kidney disease, stroke/cerebrovascular accident, and arthritis.
c Comorbid conditions were defined using ICD-9, ICD-10, and HICDA diagnosis codes (see Supplemental Table 1). Covariates included in the fully adjusted model included education level, hypertension, ischemic heart disease, chronic pulmonary disease, atrial fibrillation, diabetes mellitus, cancer, osteoporosis, asthma, hyperlipidemia, dementia, hepatitis, chronic kidney disease, stroke/cerebrovascular accident, arthritis, diagnosed obesity, and schizophrenia.
Several chronic medical conditions in addition to depression were also associated univariately with increased risk of newly diagnosed HF (Supplemental Table 2). As shown in Table 2, the risk of newly diagnosed HF was significantly higher in depressed cohort members than non-depressed cohort members after adjusting for these chronic conditions in both step-wise and fully adjusted models.
Individuals with HF and newly diagnosed depression
Table 3 summarizes the demographic and clinical characteristics of cohort members with HF and those without HF. The HF cohort was predominantly elderly and Caucasian, with a nearly equal proportion of men and women. The mean duration of follow-up was similar between cohort members with HF and without HF (Table 3).
Characteristics of 5,911 people with heart failure (HF) and 5,911 people without HF in the 2006 Primary Care cohort.
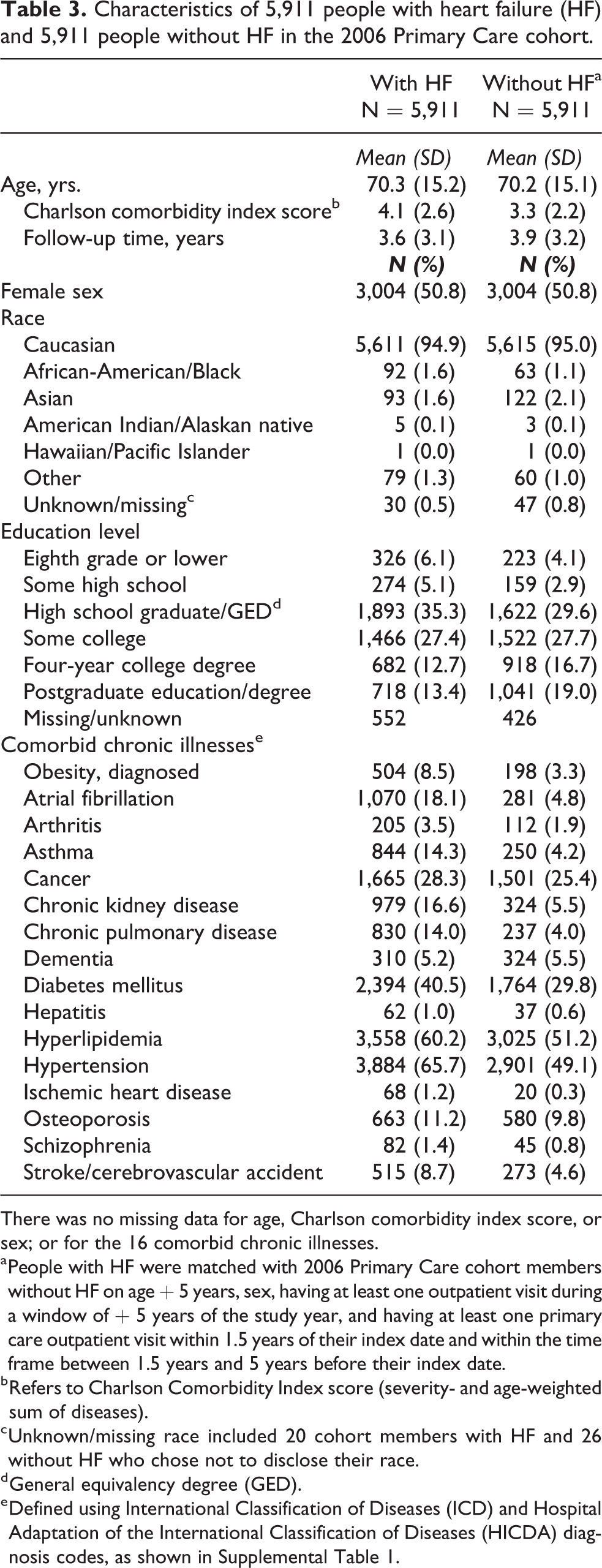
There was no missing data for age, Charlson comorbidity index score, or sex; or for the 16 comorbid chronic illnesses.
a People with HF were matched with 2006 Primary Care cohort members without HF on age
b Refers to Charlson Comorbidity Index score (severity- and age-weighted sum of diseases).
c Unknown/missing race included 20 cohort members with HF and 26 without HF who chose not to disclose their race.
d General equivalency degree (GED).
e Defined using International Classification of Diseases (ICD) and Hospital Adaptation of the International Classification of Diseases (HICDA) diagnosis codes, as shown in Supplemental Table 1.
A total of 533 people with HF and 411 people without HF had newly diagnosed depression during follow-up. There was a significantly higher risk of newly diagnosed depression for cohort members with HF (HR 1.40, 95% CI 1.24–1.59) than those without HF (Table 4). The higher risk of newly diagnosed depression in cohort members with HF remained statistically significant after adjusting for Charlson Comorbidity Index score (Table 4). As shown in Supplemental Table 3, several individual chronic medical conditions were also associated with newly diagnosed depression in univariable analyses. Significantly higher risks of newly diagnosed depression in cohort members with HF (versus those without HF) were observed after adjusting for these comorbid conditions in both step-wise and fully adjusted Cox models (Table 4). The main findings in the HF cohort were supported by fully adjusted Cox models censored at 5 years.
Hazard ratios (HR) (95% CI) for the risk of newly diagnosed depression according to heart failure status in the 2006 Primary Care cohort.

The impact of HF on subsequent depression diagnosis was assessed using marginal Cox proportional hazard models.
a People with HF were matched with 2006 Primary Care cohort members without HF on age
b Comorbid conditions were defined using ICD-9, ICD-10, and HICDA diagnosis codes (see Supplemental Table 1). Covariates selected by step-wise algorithm included education level, hypertension, chronic pulmonary disease, cancer, osteoporosis, asthma, hyperlipidemia, and arthritis.
c Comorbid conditions were defined using ICD-9, ICD-10, and HICDA diagnosis codes (see Supplemental Table 1). Covariates included in the fully adjusted model included education level, hypertension, ischemic heart disease, chronic pulmonary disease, atrial fibrillation, diabetes mellitus, cancer, osteoporosis, asthma, hyperlipidemia, dementia, hepatitis, chronic kidney disease, stroke/cerebrovascular accident, arthritis, diagnosed obesity, and schizophrenia.
Of the 5,911 people with HF, a total of 3,839 (65%) had EF data. Of these, 2,706 people with HF had EF
Discussion
Prior research has focused on the associations between newly diagnosed HF in depressed patients or on newly diagnosed depression in people with HF using separate, smaller cohorts. To our knowledge, this study is the first to simultaneously examine the temporal, bi-directional association between depression and HF within a single population using longitudinal data derived from EHRs. The findings from this well-characterized cohort of 10,649 patients with diagnosed depression, 5,911 patients with diagnosed HF, and equal numbers of matched non-depressed or non-HF patients, provided evidence of a bi-directional relationship between depression and HF. These bi-directional associations remained significant after adjusting for numerous general medical and mental health comorbidities, and for overall chronic disease burden.
Depression status and newly diagnosed HF
In our study, depression was strongly associated with an increased likelihood of newly diagnosed HF, after accounting for the potential effects of age, sex, and medical and psychiatric comorbidity. Although some have failed to demonstrate a significantly increased risk of HF in people with depressive disorders or symptoms, 15,16 our results are consistent with findings from the majority of longitudinal studies showing a significantly increased risk of HF in people with diagnosed major depression, 13 depressive syndromes, 8 and depressive symptoms. 7,9 –12,14
Our depression case definition included multiple unipolar depression diagnoses rather than focusing solely on major depression. This decision was based on evidence from epidemiological studies showing that clinically significant depressive symptoms are two to three times more prevalent than major depression across a variety of treatment settings, 20 and that the impact of depressive disorders on health status does not differ significantly between syndromal forms of depression. 33 –35 Depression severity, however, appears to impact the risk of HF and HF outcomes. A large prospective study of more than 62,000 adults showed that the risk of newly diagnosed HF increased with increasing depression severity. 9 Other studies have shown that all-cause mortality and the risk of rehospitalization are higher in people with HF and major depression than HF patients with minor or mild depression. 36,37 Although several cohort members in our study had depression scale scores that were available for abstraction, this information was not complete enough to conduct a valid analysis of HF risk by depression severity.
Regardless of how it is defined, depression is associated with co-occurring chronic illnesses that may be expected to increase the risk of HF. 38,39 Therefore, the association between depression and HF is subject to confounding by comorbidity. Our adjusted models included 16 common chronic conditions that often co-occur with depression and HF. 40,41 The association between depression and newly diagnosed HF remained significant after controlling for these conditions, and the strength of association between depression and newly diagnosed HF in our univariable model attenuated to only a minor degree in the adjusted models. Taken together, our findings suggest that depression increases the risk of HF independently of co-occurring chronic somatic and mental health conditions.
We studied the effect of depression on HF risk across a relatively wide age range. In our study, the inter-quartile age range was 33–64 years—an important consideration given the relatively young age of onset for most depressive disorders, 42 and increasing recognition of HF in middle-aged and younger persons. 43 The increased risk of HF in depressed persons in our study is troubling given that the mean age and average duration of follow-up in our depression cohort was 49.5 and 6.3 years, respectively; yet, people at or above the age of 65 years account for over 80% of prevalent HF cases in the U.S. and Europe. 44 Indeed, depression has been hypothesized as leading to the earlier onset (or more rapid accumulation) of age-associated comorbidity, a proxy for accelerated aging, 45,46 than non-depressed persons. 47 Recent studies have also shown that depression is associated with shorter telomere length, 48 a measure of cellular aging, and that such effects appear to be most pronounced for people with more severe and chronic major depression. 49 A number of other biological mediators of aging are implicated in the pathophysiology of depressive syndromes and HF, inviting speculation about shared neuroendocrine, inflammatory, genetic, epigenetic, and cellular mechanisms 50,51 —important areas of potentially shared disease vulnerability that are in need of further study.
HF status and newly diagnosed depression
In our study, there was a significantly increased risk of newly diagnosed depression in people with HF, as compared to those without HF. The heightened risk of newly diagnosed depression in HF patients also occurred independently of age, sex, and medical and psychiatric comorbidity. The estimated associations between HF status and newly diagnosed depression from univariable models attenuated only slightly in step-wise and fully adjusted models. Taken together, these results established the independent and bi-directional association between depression and HF in this cohort.
There is surprisingly little evidence from longitudinal studies pointing to increased risk of developing depression in people with HF. Our results are consistent with those of a cohort study of 5,095 elderly adults that documented associations between HF and new-onset clinically significant depressive symptoms and syndromes as a composite endpoint, and depressive syndromes separately. 52 Others have documented a high incidence of newly diagnosed depressive syndromes or clinically significant depressive symptoms in people with HF, ranging from 6% (major depression) to 21% (depressive symptoms). 17,18 Our results add to a growing evidence base pointing to a heightened risk of newly diagnosed depression in people with HF.
The risk of newly diagnosed depression was significantly increased in people with HFpEF and those with HFrEF. Our findings are consistent with cross-sectional data showing that depression occurs commonly in patients with HFrEF and HFpEF, 53 and with the results of a longitudinal study showing that depression predicts worse outcomes in people with both HF subtypes—including increased risk of cardiac death and HF rehospitalization over 2 years of follow-up. 54 To our knowledge, this is the first longitudinal EHR-based study documenting the relationship between newly diagnosed depression in people with HFpEF and HFrEF, separately. In our study, the association between HF and newly diagnosed depression appeared to be stronger for the HFrEF individuals. It is presently unknown if HFrEF truly has a stronger relationship with depression than HFpEF, although several factors could account for such a finding. These include the strong associations between coronary artery disease and both depression and HFrEF, 55 and possible shared downstream effects of excessive neurohormonal and inflammatory activities that may serve as underlying pathophysiological factors for both depression and pathological cardiac remodeling associated with HFrEF. 56,57 Only 65% of people in our HF cohort had data on ejection fraction, which limits the conclusions one can draw from this study about the relationships between HF subtype (based on ejection fraction) and the risk of newly diagnosed depression.
Implications
The evidence of a bi-directional association between depression and HF in this study and the known adverse impacts of each condition on important longitudinal outcomes of the other highlight the important public health implications of our results. Both depression and HF are considered to be preventable and treatable conditions, suggesting that aggressively treating depression may reduce the occurrence of HF and vice-versa, provided that these illnesses are causally related. A bi-directional causal association seems plausible based on the existence of a number of potentially shared biological 58 –62 and behavioral factors in depression and HF that are related to pathophysiology and worse longitudinal outcome for both conditions. 63 –65 The importance of shared etiopathophysiological mechanisms and outcome-modifying factors between depression and HF rests in the possibility that early interventions for one condition may also prevent or provide benefit for the other. For instance, the occurrence of depression in people with HF negatively impacts adherence to medication, cardiac rehabilitation, and other forms of treatment; 65 and there are important potential “downstream” impacts on healthcare use and costs of care that are in need of further investigation. However, there are still well-known challenges that remain with respect to leveraging existing treatment modalities for reducing depressive symptoms in HF patients and showing benefit for HF-specific outcomes when depressive symptoms improve or remit. 66,67 In addition, though well-tolerated, flexibly dosed sertraline (50–200 mg daily) failed to demonstrate significant antidepressive benefit versus placebo over 12 weeks of treatment in 469 depressed HF patients (New York Heart Association functional class II to IV) who participated in the Sertraline Against Depression and Heart Disease in Chronic Heart Failure (SADHART-CHF) Trial. 68 Such observations may weaken a causal link between depression and HF. Additionally, it has yet to be convincingly demonstrated that reduced HF symptoms leads directly to improvement in depression when the two conditions co-occur. In this work, we were able to establish bi-directional associations between depression and HF, but not causality given the observational study design. We were also unable to assess the effects of successful treatment of depression on the risk of newly diagnosed HF, or vice-versa, in this study.
Strengths and limitations
Our EHR-based cohort study had notable strengths. People with depression and HF were carefully matched to unaffected referent patients in each of the study cohorts, and our analyses robustly accounted for physical and mental health multimorbidity. The data source for this study permitted the simultaneous testing of two hypotheses—that depression was associated with newly diagnosed HF and that HF was associated with newly diagnosed depression—in a single population of patients receiving medical care in routine primary care settings. The use of EHRs allowed for the comprehensive ascertainment of study data that spanned the full range of medical care for each cohort member, and permitted access to information with sufficient detail to accurately define people with depression, people with HF, and confounding factors that included a wide range of chronic illnesses.
There were also limitations to our approach, in addition to those already discussed. The data for our study consisted of information in EHRs (including free text and diagnosis codes). Although the records were comprehensive, they were not collected for research purposes, and are thus subject to misclassification. However, misclassification in this study was likely to be non-differential, so any resulting bias would be toward the null. Our study cohorts were selected from calendar year 2006, which assured reasonably complete data from the electronic health records and an adequate amount of follow-up time. Secular trends in the diagnosis, treatment and prognosis of depression and HF, however, could have impacts on the strength of association between these two conditions as a function of time, although we anticipate that such effects may have been minimized, at least partially, by matching on calendar year at index date. We lacked complete access to data on important covariates, such as smoking, body mass index, and dietary/health behaviors. We used level of education as a broad measure of socioeconomic status, given the lack of a more direct measure. 69 Future studies of the relationship between depression and HF will need to account for the potential effects of more nuanced indicators of socioeconomic status given its predictive effects on the development of both conditions. 70,71 We did not have complete data on lifetime depression. Therefore, the algorithms used to define depression may have identified recurrences of depression rather than new cases. 72 Future studies with sound psychiatric assessments and follow-up starting in early adulthood are needed to better-establish a link between depression and HF. Associations in the other direction (depression to HF) are less-problematic given that HF is non-episodic and emerges later in life. The discrepancy in follow-up times between the depression and HF cohorts also warrants further discussion because of the reasonably high likelihood that it reflects differences in survivorship. Although we demonstrated a significant association between HF and newly diagnosed depression, we did not have data on comparative death rates between the study cohorts, which may have been helpful for determining if depletion of susceptible persons (for developing a diagnosed episode of depression) may have led to an underestimation of the risk of newly diagnosed depression in the HF cohort. Only a small number of depression and HF cohort members in our study had diagnosed ischemic heart disease at baseline, which may have resulted in an underestimation of the relationship between depression and HF in either direction. 73,74 However, our findings in adjusted models that included ischemic heart disease were in accord with separate models that adjusted for Charlson Comorbidity Index scores, the latter of which included myocardial infarction and correlated conditions such as peripheral vascular disease, cerebrovascular disease, and diabetes with evidence of end organ damage. Our cohort consisted of mainly Caucasian individuals actively receiving primary care services within a single healthcare system located in southeast Minnesota. Therefore, our findings may not generalize to non-care-seeking individuals, or to more racially and ethnically diverse populations residing elsewhere. And finally, although the association between depression and HF appeared to be stronger in the depression cohort than the HF cohort, this may reflect differences in survivorship between the two cohorts. Therefore, our results should not be interpreted as conclusive evidence of a difference in the strength of associations between these very different groups of patients.
Conclusion
This large, well-controlled cohort study using longitudinal EHR data provides evidence that the relationship between depression and HF is bi-directional, and that it occurs independently of age, sex, and multimorbidity from common chronic illnesses. The risk of newly diagnosed depression appears to be increased in people with HFrEF and in people with HFpEF.
Supplemental material
Supplemental Material, sj-docx-1-cob-10.1177_2235042X20984059 - Bi-directional association between depression and HF: An electronic health records-based cohort study
Supplemental Material, sj-docx-1-cob-10.1177_2235042X20984059 for Bi-directional association between depression and HF: An electronic health records-based cohort study by William V Bobo, Euijung Ryu, Tanya M Petterson, Kandace Lackore, Yijing Cheng, Hongfang Liu, Laura Suarez, Martin Preisig, Leslie T Cooper, Veronique L Roger, Jyotishman Pathak and Alanna M Chamberlain in Journal of Comorbidity
Supplemental material
Supplemental Material, sj-docx-2-cob-10.1177_2235042X20984059 - Bi-directional association between depression and HF: An electronic health records-based cohort study
Supplemental Material, sj-docx-2-cob-10.1177_2235042X20984059 for Bi-directional association between depression and HF: An electronic health records-based cohort study by William V Bobo, Euijung Ryu, Tanya M Petterson, Kandace Lackore, Yijing Cheng, Hongfang Liu, Laura Suarez, Martin Preisig, Leslie T Cooper, Veronique L Roger, Jyotishman Pathak and Alanna M Chamberlain in Journal of Comorbidity
Supplemental material
Supplemental Material, sj-docx-3-cob-10.1177_2235042X20984059 - Bi-directional association between depression and HF: An electronic health records-based cohort study
Supplemental Material, sj-docx-3-cob-10.1177_2235042X20984059 for Bi-directional association between depression and HF: An electronic health records-based cohort study by William V Bobo, Euijung Ryu, Tanya M Petterson, Kandace Lackore, Yijing Cheng, Hongfang Liu, Laura Suarez, Martin Preisig, Leslie T Cooper, Veronique L Roger, Jyotishman Pathak and Alanna M Chamberlain in Journal of Comorbidity
Supplemental material
Supplemental Material, sj-docx-4-cob-10.1177_2235042X20984059 - Bi-directional association between depression and HF: An electronic health records-based cohort study
Supplemental Material, sj-docx-4-cob-10.1177_2235042X20984059 for Bi-directional association between depression and HF: An electronic health records-based cohort study by William V Bobo, Euijung Ryu, Tanya M Petterson, Kandace Lackore, Yijing Cheng, Hongfang Liu, Laura Suarez, Martin Preisig, Leslie T Cooper, Veronique L Roger, Jyotishman Pathak and Alanna M Chamberlain in Journal of Comorbidity
Supplemental material
Supplemental Material, sj-docx-5-cob-10.1177_2235042X20984059 - Bi-directional association between depression and HF: An electronic health records-based cohort study
Supplemental Material, sj-docx-5-cob-10.1177_2235042X20984059 for Bi-directional association between depression and HF: An electronic health records-based cohort study by William V Bobo, Euijung Ryu, Tanya M Petterson, Kandace Lackore, Yijing Cheng, Hongfang Liu, Laura Suarez, Martin Preisig, Leslie T Cooper, Veronique L Roger, Jyotishman Pathak and Alanna M Chamberlain in Journal of Comorbidity
Footnotes
Acknowledgement
We are indebted to Richard S Pendegraft, Department of Health Sciences Research, Mayo Clinic, Rochester, MN, USA, for his invaluable assistance with the electronic extraction of data needed to complete the study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: WVB’s research has been supported by AHRQ, NIMH, and the Mayo Foundation for Medical Education and Research. He has contributed chapters on the treatment of bipolar disorders to UpToDate. LTC’s research has been supported by NHLBI and the Mayo Foundation for Medical Education and Research. VLR’s research has been supported by NHLBI, PCORI and the Mayo Foundation for Medical Education and Research. JP’s research has been supported by NIH, AHRQ, PCORI, NSF, Weill Cornell Medicine BioVentures, American Heart Association and Merck Pharmaceuticals. He is the founder of and has equity ownership at Iris OB Health Inc. The remaining authors declare no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by AHRQ grant R01HS023077 and the Mayo Clinic Foundation for Medical Education and Research. The funders had no role in the study design, management, analysis, interpretation of study data; or preparation, review, or approval of the manuscript; or decision to submit the manuscript for publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.