
Abstract
Background:
Heart failure patients often present with frailty and/or multi-morbidity, complicating care and service delivery. The Chronic Care Model (CCM) is a useful framework for designing care for complex patients. It assumes responsibility of several actors, including frontline providers and health-care administrators, in creating conditions for optimal chronic care management. This qualitative case study examines perceptions of care among providers and administrators in a large, urban health system in Canada, and how the CCM might inform redesign of care to improve health system functioning.
Methods:
Sixteen semi-structured interviews were conducted between August 2014 and January 2016. Interpretive analysis was conducted to identify how informants perceive care among this population and the extent to which the design of heart failure care aligns with elements of the CCM.
Results:
Current care approaches could better align with CCM elements. Key changes to improve health system functioning for complex heart failure patients that align with the CCM include closing knowledge gaps, standardizing treatment, improving interdisciplinary communication and improving patient care pathways following hospital discharge.
Conclusions:
The CCM can be used to guide health system design and interventions for frail and multi-morbid heart failure patients. Addressing care- and service-delivery barriers has important clinical, administrative and economic implications.
Keywords
Introduction
It is estimated that more than half a million Canadians are living with heart failure, 1 a chronic condition associated with high mortality and substantial morbidity. It is a growing illness due, in part, to improved survival, an increase in risk factor prevalence and an aging population, 2 with the fastest growth projected among individuals over 85. 1
As a disease of older adults, heart failure is associated with multiple morbidities. 3 One such morbidity is frailty, a disorder characterized by increased physiologic vulnerability to stressors that increases with age and, like heart failure, is most prevalent in the elderly. 4,5 Multi-morbidity and frailty in patients with heart failure are associated with worse health outcomes. 3,6 This complicates the development and progression of heart failure, and its management at all levels of care within the health system, including primary, secondary and tertiary care, resulting in a significant treatment burden on the patient and hindering an individualized approach to care, which has otherwise been shown to improve outcomes for this patient population. 3,6 –9 Empirical research from Canada and abroad on the design of heart failure care in local health systems highlight the need for a more integrated and coordinated approach to care and service delivery that puts patients and their preferences front and centre. 10 –13 Lack of such approaches has resulted in suboptimal care quality and hindered attempts to reduce mortality and rehospitalization for this population. 11 –13 Redesign of primary care specifically has been purported to close the quality gap between current practices and optimal standards. 14
The Chronic Care Model (CCM), proposed by Edward Wagner, provides a useful framework for the redesign of heart failure care. 15 Developed in response to the increasing prevalence of complex chronic conditions and the subsequent impact on local health systems, it is a framework for designing chronic illness care that assumes improvement in care involves patient-, provider- and system-level interventions. 15 It identifies six essential, interdependent elements that need to be considered for a health system to manage complex conditions: health-care organization, delivery system design, decision support, clinical information systems, self-management support and the community. These elements highlight the collective responsibility of patients, caregivers and their community; providers and administrators within their organizations; and policymakers within the health-care system in creating favourable conditions for optimal chronic care management. 15 The CCM has informed a number of interventions and care approaches for a range of chronic illnesses. 16,17 Interventions derived from the CCM recognize that individuals with one chronic illness, like heart failure, have other morbidities. 18
This qualitative study focuses squarely on frontline providers and administrators. We utilize semi-structured interviews with frontline providers and administrators from a large, urban health system to understand their perceptions of heart failure care for patients with frailty and/or multi-morbidity, and key changes, if any, required to improve health system functioning for this population. This study also examines the extent to which the design of heart failure care aligns with elements of the CCM and how we can use this model to understand and improve approaches to care and service delivery for heart failure patients with frailty and/or multi-morbidity.
Methods
Context and setting
This study took place at a large, urban health system in Ontario, Canada. This health system has a comprehensive cardiology program and one of the largest heart failure and heart transplant centres in North America. Ethics approval for this study was obtained from the Women’s College Hospital Research Ethics Board (2014-0035-B).
Study design
This is a qualitative study inspired by case study methodology. Case study methodology has a number of theoretical interpretations. For the purpose of this research, we draw upon the scholarship of Stake and Simons. Case study research is an in-depth, practical investigation of a single case or collective cases to capture the complexity and uniqueness of a specific unit of analysis, whether a phenomenon, project, policy, institution, program, or system in practice. These “cases” exist within defined boundaries that allow the researcher to determine what will or will not be studied. 19,20
Our study focuses on a single, geographically bound case—a large, urban health system comprised of frontline health-care providers and administrators. Single case studies have the potential to provide convincing data to test or apply theories and models, such as the CCM. 19 Hence, for the purpose of this study, we have opted to focus squarely on an urban health system, but recognize that results may not be generalizable to other contexts, including rural health systems.
Both Stake and Simons posit that cases can be studied from different perspectives. In this study, we utilize semi-structured interviews to understand how providers and administrators perceive health care and service delivery for heart failure patients with frailty and multi-morbidity. As stated earlier, the CCM recognizes that providers and administrators within an organization have a responsibility in creating favourable conditions for optimal chronic care management. For the purpose of this study, patients and family caregivers were not included due to timing and funding constraints, although we recognize they, too, have a critical role in health-care redesign per the CCM. A follow-up study is underway concerning perceptions of heart failure care and service delivery among heart failure patients with frailty and/or multi-morbidity and family caregivers to derive a more fulsome picture of needs among this population and corroborate findings from providers and administrators in this study.
Sampling and data collection
Purposive sampling was used to identify health system leaders (providers and administrators) from a large, urban health system in Ontario, Canada, involved in the care and management of heart failure patients, either in a clinical management or in administrative capacity. For example, informants could include family physicians, specialists (including cardiologists and general internists), registered nurses, other allied health professionals, heart failure program managers, community care providers, or hospital executives with relevant experience in health-care delivery and design.
A list containing the names and e-mail addresses of providers and administrators working within our case of interest was provided by the principle investigator. A research assistant (RA) then recruited informants by e-mail, in which study goals and the principal investigator’s interests in quality of heart failure care were clearly articulated. An individual interview was arranged with each informant who responded expressing interest. Individual interviews were held in person at informant’s place of work, or over the phone, to accommodate availability and for convenience. Interviews were conducted by an RA academically trained in conducting semi-structured interviews. As a non-clinician, this RA entered interviews with limited presuppositions about the subject matter. Informed written consent was obtained from all informants prior to the interview. Each interview lasted between 15 min and 30 min, and took place between August 2014 and January 2016. This lengthy data collection period is a result of various scheduling conflicts and a follow-up e-mail recruitment process intended to obtain additional informants. Recruitment formerly ended following consensus among the research team that perceived thematic saturation had been achieved.
Our semi-structured interview guide (Appendix A in the online supplemental material) included guiding questions and prompts adapted from the “Innovate A-Fib Interview Guide,” a validated questionnaire developed by OpenLab at Toronto’s University Health Network. 21 Questions were tailored to understand approaches to heart failure care. For example, questions explore informant perceptions of care, whether positive or negative, for frail and multi-morbid heart failure patients (including perceived challenges experienced by patients and how patients flow through the health system), the value of assessing frailty and multi-morbidity and recommendations to achieve optimal care for these patients. The application of the CCM occurred at the point of analysis (further discussed below), and so informants were not expected to understand the CCM, they were not asked about the CCM during the interview process and they were not aware that the CCM would be applied to analyze findings. Given that semi-structured interviewing is an emergent process, not all guiding questions presented in Online Appendix A were asked of all informants and guiding questions did not preclude exploration of important topics raised by informants.
Data analysis
Interviews were audio-recorded and transcribed verbatim by an RA. Gaps in the transcripts were filled by member checking or contacting informants for clarification. Three transcripts were coded inductively by three RAs trained in qualitative data analysis using Microsoft Word. We opted not to use more advanced coding packages (e.g. NVivo) due to limited access and varying levels of proficiency among coders, and because the sophisticated analytic procedures available in more advanced software were not needed for the purpose of this study. The research team, comprising of the principal investigator, a qualitative social scientist and three RAs, met to review coding for inter-rater reliability and developed a coding framework, or codebook. Remaining transcripts were then divided among RAs and coded using the codebook as a guide.
Codes were then analyzed thematically by the research team to identify themes and patterns that most comprehensively represent the data. An interpretive analysis of themes was then conducted, which is an approach in qualitative case study analysis involving the interpretation of qualitative data through the development of, or application to, conceptual categories. 22 In the context of this study, we sought to understand how key themes derived from the data may be understood in relation to the six elements of a health-care system that promote high-quality chronic disease care outlined in the CCM. 15 Drawing these relationships was an interpretive exercise by the research team, and so these relationships may not be exhaustive and additional relationships may be surmised.
Results
Twenty-five e-mails invitations were sent over the recruitment period. Twenty-one informants agreed to participate. As a result of cancellations and scheduling conflicts among 5 informants (2 community-based family physicians, 1 geriatrician and 2 registered nurses), 16 informants were interviewed. The informant group included seven cardiologists (three of whom work in an administrative capacity, for example, as heart failure program director or clinical division head), one family physician, three internists (one of whom works in an administrative capacity), one registered cardiovascular nurse, one advanced practice nurse practitioner specializing in heart failure care, one nephrologist, one rheumatologist and one hospital policymaker. Further demographic information on informants is presented in Online Appendix B. No informants dropped out of the study and no interviews were repeated.
Findings have been categorized into five themes representing current approaches to heart failure care for frail and/or multi-morbid heart failure patients. Themes were then assigned to one or more elements of the CCM (Table 1) to illustrate how incorporating elements of the CCM into the design of complex heart failure care might address shortcomings and challenges in current care approaches identified by informants. Drawing these relationships was an interpretive exercise by the research team, and so additional relationships may be surmised. To draw out inter-relationships between themes and CCM elements, Table 1 presents supplemental representative quotes from informants. These relationships are further unpacked in our discussion.
Relationships between elements of the CCM and themes from informant interviews.
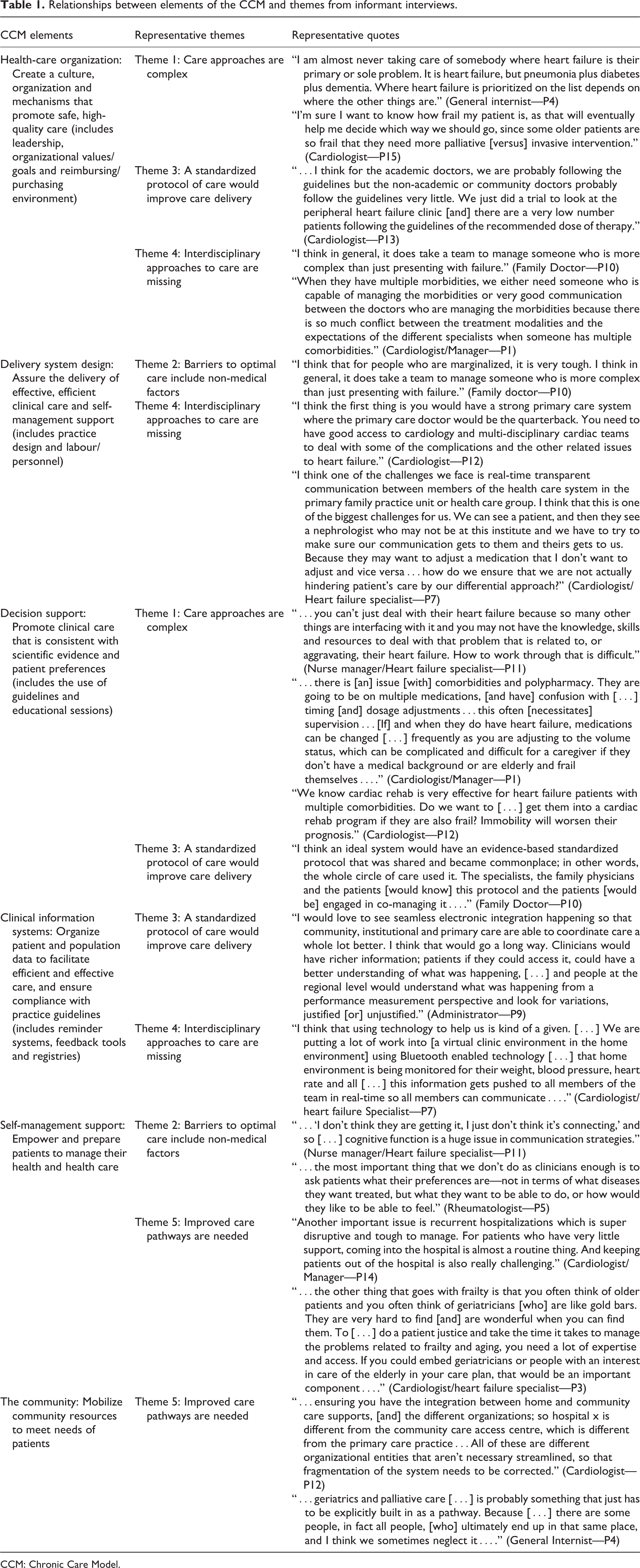
CCM: Chronic Care Model.
Overall, incorporating elements of CCM into the design of complex heart failure care could address challenges in current approaches to care for this population. Key changes to improve health system functioning for complex heart failure patients that align with the CCM include closing knowledge gaps, standardizing treatment, improving communication between interdisciplinary providers and improving patient care pathways following hospital discharge.
Theme 1: Care approaches are complex
Informants understood that frailty and multi-morbidity affect heart failure treatment and outcomes. Several acknowledged that if a patient does not die from heart failure, they may likely succumb to, or be rehospitalized for, complications from another morbidity, such as diabetes, chronic kidney disease, or chronic obstructive lung disease.
As a result, frailty and multi-morbidity affect the extent to which clinicians are able to adhere to guideline-recommended therapy for each individual morbidity a patient with heart failure presents with. These patients are usually prescribed a complex combination of medications; however, pharmacological decisions should aim to avoid adverse effects, including drug contraindications resulting in rehospitalization. Heart failure clinicians who work in siloes or lack access to care teams that include pharmacists and general internists may be unaware of how to proceed pharmacologically when a heart failure patient is frail and/or multi-morbid. …you can’t just deal with their heart failure because so many other things are interfacing with it and you may not have the knowledge, skills and resources to deal with that problem that is related to, or aggravating, their heart failure. How to work through that is difficult. (Nurse manager/Heart failure specialist—P11)
For older heart failure patients with frailty and multi-morbidity, careful compliance with prescribed medication is important. However, for patients with age-related cognitive impairment like dementia or limited health literacy, communicating medication instructions is challenging. As a result, patients may be unable to understand or remember, and therefore comply with, these instructions. In such cases, the role of the family caregiver as a member of the patient’s care team becomes critical. …there is [an] issue [with] comorbidities and polypharmacy. They are going to be on multiple medications, [and have] confusion with […] timing [and] dosage adjustments…this often [necessitates] supervision…[If] and when they do have heart failure, medications can be changed […] frequently as you are adjusting to the volume status, which can be complicated and difficult for a caregiver if they don’t have a medical background or are elderly and frail themselves…. (Cardiologist/Manager—P1)
Adding to this complexity are patient preferences. Informants noted an important facilitator to optimal care is acknowledging patient preferences when patients with heart failure present with more than one morbidity. These preferences include their need and desire for lifestyle interventions, not just surgical or pharmacological interventions, and acknowledgement of patient characteristics such as culture and gender. …the most important thing that we don’t do as clinicians enough is to ask patients what their preferences are—not in terms of what diseases they want treated, but what they want to be able to do, or how would they like to be able to feel. (Rheumatologist—P5)
Theme 2: Barriers to optimal care include non-medical factors
Informants understood that medical conditions do not exist in isolation of the social determinants of health. For frail and multi-morbid heart failure patients, not having access to nutritious food, transportation to reach a hospital for follow-up appointments and/or community, social, and family support means effective provider management and self-management of heart failure and other morbidities is difficult. I think that for people who are marginalized, it is very tough. I think in general, it does take a team to manage someone who is more complex than just presenting with failure. (Family doctor—P10) …“I don’t think they are getting it, I just don’t think it’s connecting,” and so […] cognitive function is a huge issue in communication strategies. (Nurse manager/Heart failure specialist—P11)
Theme 3: A standardized protocol of care would improve care delivery
According to the informants, there is no standard of care in place so that patients flow through care in the same way, nor is there a shared, validated, evidence-based, heart failure-specific standardized protocol for the whole circle of care that distinguishes high-risk from low-risk patients with heart failure. The difference between what is considered mild, moderate, or severe heart failure has implications on treatment, and a standardized protocol for such categories would be helpful. I think an ideal system would have an evidence-based standardized protocol that was shared and became commonplace; in other words, the whole circle of care used it. The specialists, the family physicians and the patients [would know] this protocol and the patients [would be] engaged in co-managing it…. (Family doctor—P10) I would love to see seamless electronic integration happening so that community, institutional and primary care are able to coordinate care a whole lot better. I think that would go a long way. Clinicians would have richer information; patients if they could access it, could have a better understanding of what was happening, […] and people at the regional level would understand what was happening from a performance measurement perspective and look for variations, justified [or] unjustified. (Administrator—P9) …I think for the academic doctors, we are probably following the guidelines but the non-academic or community doctors probably follow the guidelines very little. We just did a trial to look at the peripheral heart failure clinic [and] there are a very low number patients following the guidelines of the recommended dose of therapy. (Cardiologist—P13)
Theme 4: Interdisciplinary approaches to care are missing
The majority of informants identified the importance of an interdisciplinary team to follow heart failure patients through their disease trajectory, both within and outside a hospital setting.
While the definition of “interdisciplinary” varied among informants, it could include a combination of health-care providers, allied health practitioners and community health practitioners; for example, family physician, cardiologist, general internist, psychiatrist, pharmacist, nurse, dietician, community services coordinator, social worker, occupational/physical therapist and the patient’s family/caregivers.
An interdisciplinary approach would address treatment and communication gaps identified in themes 1 and 3. For both patients and providers, this would facilitate a smoother care transition between various care pathways, including primary to secondary care (theme 5). When they have multiple morbidities, we either need someone who is capable of managing the morbidities or very good communication between the doctors who are managing the morbidities because there is so much conflict between the treatment modalities and the expectations of the different specialists when someone has multiple comorbidities. (Cardiologist/Manager—P1) I think the first thing is you would have a strong primary care system where the primary care doctor would be the quarterback. You need to have good access to cardiology and multi-disciplinary cardiac teams to deal with some of the complications and the other related issues to heart failure. (Cardiologist—P12)
Informants suggested clinical information systems to alleviate time-related challenges in communication between health-care providers; for example, portals or web-based access to information (a virtual environment) involving all members of the health-care team and interdisciplinary telemedicine. I think that using technology to help us is kind of a given. […] We are putting a lot of work into [a virtual clinic environment in the home environment] using Bluetooth enabled technology […] that home environment is being monitored for their weight, blood pressure, heart rate and all […] this information gets pushed to all members of the team in real-time so all members can communicate…. (Cardiologist/heart failure Specialist—P7)
Theme 5: Improved care pathways are needed
Finally, informants advocated for several improved care pathways, including the pathway between primary and secondary care, between the patient’s emergency room visit and hospital admission and between hospital discharge and home/community, long-term or palliative/end-of-life care. Informants highlighted that the goals of an improved care pathway include preventing or reducing unnecessary readmission, characteristic among heart failure patients who present with frailty and multi-morbidity. Reducing readmission would minimize health-care utilization and thus cost to the health-care system. …ensuring you have the integration between home and community care supports, [and] the different organizations; so hospital x is different from the community care access centre, which is different from the primary care practice…All of these are different organizational entities that aren’t necessary streamlined, so that fragmentation of the system needs to be corrected. (Cardiologist—P12)
Frequently mentioned among informants was improving the care pathway for frail geriatric patients by ensuring that those with relevant expertise, namely geriatricians, are part of their heart failure care team. …geriatrics and palliative care […] is probably something that just has to be explicitly built in as a pathway. Because […] there are some people, in fact all people, [who] ultimately end up in that same place, and I think we sometimes neglect it…. (General internist—P4)
Discussion
Informants in our study acknowledged that frailty and multi-morbidity must be considered in the design of heart failure care. Issues in care design for this complex population stem from non-standardized approaches to care, poor interdisciplinary communication between providers, uncoordinated care transition processes and insufficient recognition of social dimensions of health in care delivery. These findings corroborate observations of care approaches for complex and multi-morbid heart failure patients in other local health systems. For example, non-standardized approaches to care is a result of knowledge gaps around age-tailored treatment and pharmacological best practices 23 and how to effectively use virtual care and health information technology to document data and improve outcomes. 24 –26 Furthermore, care approaches are siloed due to poor interdisciplinary communication, 26 –29 limited patient and caregiver involvement in care planning and recognition of patient preferences 10,28,30 and suboptimal coordination in care pathways, particularly from acute settings to the community or palliative/end-of-life care, 11,28,31 contributing to rehospitalization among complex heart failure patients. 13,32
Several chronic disease models and principles exist to guide the design of effective chronic disease care. Beyond the CCM, other models and principles include the Stanford Model, Improving Chronic Illness Care, the Community-based Transition Model, the Ariadne principles and Innovative Care for Chronic Conditions. 33,34 Previous reviews of literature evaluating some of these models note the CCM as being the most widely used and most effective in improving health outcomes and health system practices for people living with one or more chronic diseases. 33 In another review focused squarely on the effectiveness of CCM elements, employing some combination of elements of the CCM resulted in improvements in health system practices and health outcomes for people living with one or more chronic diseases in 75 of the 77 studies. 35 While the CCM does call for structural change that recognizes the role of the patient, it has its limitations, particularly concerning outcomes that matter to patients (e.g. reducing patient work and improving patients’ capacity). 36 Overall, though, when considering its role in achieving health system goals and improving disease-specific outcomes for patients with one or more morbidities and its recognition of the various health system actors involved in chronic disease management, 18 the CCM serves as a useful model to both interrogate current approaches in complex heart failure care and inform future approaches.
From the relationships presented in Table 1, we can see a disconnect between informant-identified themes and favourable conditions for optimal chronic care management outlined in the elements of the CCM. However, these relationships also reveal opportunities in terms of how to fill gaps in care delivery with interventions and approaches that better align with these elements. For example, consideration of self-management support in the design of heart failure care may address challenges concerning non-medical factors that hinder optimal care (theme 2) and improve care pathways for patients who otherwise have little support in navigating the health system on their own.
Noteworthy in Table 1 is that themes may be framed by one or more elements of the CCM. For example, challenges associated with non-standardized approaches to care, for example, physician variation in uptake of guidelines concerning recommended doses of therapy (theme 3) can be framed by three CCM elements: health-care organization, which is concerned with promoting safe and high-quality care; decision supports, which is concerned with promoting evidence-based clinical care; and clinical information systems, which is concerned with the organization of data in ensuring compliance with practice guidelines. In a systematic review of studies of diabetes care programs featuring elements of the CCM, interventions featuring four or fewer CCM elements were found to improve patient outcome measures, suggesting no single element of CCM is essential for improving patient outcomes. 37 In a more recent systematic review of the effectiveness of integrated care interventions in reducing demands on the acute care sector, interventions comprising of multiple components of the CCM were significantly more effective than single component interventions at reducing admission and readmission rates, length of hospital stay and emergency room visits. 17 This suggests that limitations in the design of heart failure care could be addressed by incorporating at least one of the CCM elements.
Heart failure interventions and care approaches informed by elements of the CCM are emerging in acute and community settings. Based on empirical research from local health systems, these interventions are yielding positive results, including reduced morbidity and mortality rates 38,39 ; a lower risk of hospital readmission 38,40 ; improved self-care practices among patients 40 –42 ; productive interactions between patients and their medical teams 41 ; improved care coordination as a result of telemonitoring approaches 41 –43 ; reduction in direct hospital costs 43 ; and greater cognizance of elder patient needs, particularly in transitioning to home, a long-term care facility or palliative care. 44
System redesign for chronic illness has important economic incentives. Of particular concern to informants is the rising cost of heart failure care, particularly when frailty and multi-morbidity are factored in. It is estimated that hospital admissions for which heart failure is the primary diagnosis will cost CAD$720 million by 2030, and CAD$2.8 billion when admissions for which heart failure is a secondary diagnosis are considered. 45 The CCM recognizes that it may be cost-effective to risk-stratify chronic illness and target interventions to high-risk individuals. 37 Through informant interviews, we know that frailty and multi-morbidity impact heart failure severity and treatment trajectory, and so the CCM is a useful framework from a cost savings perspective when implemented for complex chronic illnesses in which illness severity varies greatly (e.g. congestive heart failure and asthma). When interventions are informed by the CCM, a health system may see immediate cost savings through reduced hospital and emergency department use. 46
The CCM is a useful framework for complex chronic illnesses like heart failure, as it supports informant visions of what an ideal health system should look like for heart failure patients who are frail and multi-morbid. However, its full implementation will not be quick or easy. Few health systems have achieved complete implementation of the CCM. This article’s findings will hopefully serve as a launching pad from which future work will follow around how elements of the CCM can be implemented to begin redesigning the system in which these patients receive care. Specifically, examining the ways in which the various components of the CCM interact when implemented is a key direction for future research and will help to clarify implementation strategies that stand to be most effective for heart failure patients living with frailty and/or multi-morbidity.
Limitations
Study informants are from a large academic hospital system within a large urban centre, so these results may not be generalizable to other settings across Ontario, Canada, or elsewhere, including rural settings, community hospitals and developing countries where heart failure outcomes may differ. 47 To that end, although we present a strong need for interdisciplinary care teams in theme 4, no community care providers were interviewed in this study despite recruitment efforts. Furthermore, patients and caregivers were not interviewed for this study due to research funding constraints. A follow-up study on the perception of heart failure care among frail and/or multi-morbid heart failure patients and caregivers is underway to provide a fulsome understanding of care and service delivery needs among this population. Finally, given the duration allotted for data collection, there was a concern that the design of heart failure care and service delivery may have changed; however, upon member checking with informants and confirmation with co-authors, no such changes have occurred and findings from this study still hold.
Conclusion
Existing research on the design of heart failure care tests and assesses clinical outcomes, interventions or processes in heart failure care to reach conclusions about their clinical effectiveness. This study is unique because it qualitatively examines the design of heart failure care for frail and multi-morbid patients from the perspective of providers and administrators in a local health region. From a patient perspective, improving the design of health-care delivery for this population may improve health outcomes, and from a health system perspective, reducing the high rate of rehospitalization characteristic of this population could generate future cost savings. Beyond heart failure, many system-related challenges hindering optimal care for complex disease populations can be addressed through interventions that are informed by elements of the CCM. Thus, these findings present useful learning lessons for the care of other complex chronic disease populations. To that end, these findings may be useful in informing health system redesign efforts in Ontario and other jurisdictions across Canada and the world, which are increasingly moving toward more integrated systems of health-care delivery.
Supplemental material
Supplemental Material, HF_Manuscript_(Journal_of_Comorbidity)_-_Appendix_A_NEW_Jan28,2020 - Improving the design of heart failure care from the perspective of frontline providers and administrators: A qualitative case study of a large, urban health system
Supplemental Material, HF_Manuscript_(Journal_of_Comorbidity)_-_Appendix_A_NEW_Jan28,2020 for Improving the design of heart failure care from the perspective of frontline providers and administrators: A qualitative case study of a large, urban health system by Husayn Marani, Hayley Baranek, Howard Abrams, Michael McDonald, Megan Nguyen, Juan Duero Posada, Heather Ross, Toni Schofield, James Shaw and R Sacha Bhatia in Journal of Comorbidity
Supplemental material
Supplemental Material, HF_Manuscript_(Journal_of_Comorbidity)_-_Appendix_B_NEW_Jan28,2020 - Improving the design of heart failure care from the perspective of frontline providers and administrators: A qualitative case study of a large, urban health system
Supplemental Material, HF_Manuscript_(Journal_of_Comorbidity)_-_Appendix_B_NEW_Jan28,2020 for Improving the design of heart failure care from the perspective of frontline providers and administrators: A qualitative case study of a large, urban health system by Husayn Marani, Hayley Baranek, Howard Abrams, Michael McDonald, Megan Nguyen, Juan Duero Posada, Heather Ross, Toni Schofield, James Shaw and R Sacha Bhatia in Journal of Comorbidity
Footnotes
Authors’ note
Requests for underlying research materials may be directed to the corresponding author, Dr. Sacha Bhatia, at sacha.bhatia@wchospital.ca.
Author contributions
HB conducted and transcribed interviews. HM, HB and MN analyzed transcripts. HM prepared the manuscript. JS and SB supervised analysis and offered insight on theoretical frameworks for analysis. HA, MM, JDP, HR and TS critically reviewed the manuscript. All authors approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Innovation in Quality Award from the Division of Cardiology in the Department of Medicine at the University of Toronto.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.