
Abstract
Introduction
Multimorbidity is associated with adverse clinical outcomes, including increased symptom burden and healthcare utilisation, particularly towards the end of life. Despite this, there is no accepted method to identify the point at which individuals with deteriorating health due to long-term conditions are nearing the end of life or might benefit from a palliative care approach – conceptualised as ‘Advanced Multimorbidity’. This scoping review explored how Advanced Multimorbidity is described and operationalised within the literature.
Methods
Multiple electronic databases and Grey Literature sources were searched following scoping review frameworks. Two reviewers independently performed screening and data extraction. Content analysis was used to examine the different descriptions of Advanced Multimorbidity. Stakeholder consultations were undertaken with clinicians, academics and public participants. Patient and public involvement was separately integrated throughout this review from conceptualisation, design and reporting.
Results
Forty-four different descriptions of Advanced Multimorbidity were identified from 38 publications. These varied in terms of the clinical conditions and descriptors used. Eighteen descriptions relied on a single indicator to identify Advanced Multimorbidity; 24 used a multidimensional approach. Stakeholder consultations highlighted the need for descriptions that are user-friendly and actionable.
Conclusion
The lack of a standardised definition of Advanced Multimorbidity risks variance in clinical and research practice, potentially affecting patient care. A consensus on defining Advanced Multimorbidity would enable better identification of patients who could benefit from a palliative care approach, ensuring more consistent and person-centred care, as well as supporting research and policy development.
Introduction
With the rising prevalence of people living with two or more long-term conditions, more commonly referred to as multimorbidity, there are concerns that healthcare services organised by specialism are not equipped to meet the needs of this growing population.1,2 Multimorbidity is associated with a range of adverse health outcomes, lower quality of life and increased utilisation of healthcare services throughout the life course.3–6 With increasing numbers of people living with multimorbidity, it follows that many more people are dying with and from multimorbidity. 7 This population experiences a wide range of symptoms, significantly impacting their quality of life as their health deteriorates.8,9 Healthcare utilisation towards the end of life for people with multimorbidity has been shown to be fragmented, punctuated with frequent unscheduled care contacts, and costly.10–12 The seemingly unpredictable nature of the multimorbidity illness trajectory makes identifying the end-of-life period challenging. A lack of consistent and proactive identification risks denying this group of patients and their caregivers honest conversations about their mortality and the opportunity to participate in future care planning with a view to aligning their care with what matters most to them – a key component of a palliative care approach which can be delivered by generalists and specialists alike.13,14
Increasingly it is being demonstrated palliative care is no longer exclusively a model of care for those at the very end of life, with a growing evidence base of the benefits of earlier integration of palliative approaches. 15 However, the optimal timing of when to integrate palliative care into the care of those with multiple health conditions remains unclear. Such identification and action could not only improve the appropriateness of care received by people whose life expectancy is likely to be limited, through the avoidance of potentially harmful, ineffective or unwanted treatments; but may also, from a health service perspective, increase the capacity to provide curative and preventative interventions for those more likely to benefit. In order to make a difference to the quality and nature of care that people with multimorbidity experience towards the end of life, we must be able to reliably identify the time when a palliative care approach should be considered and offered. 16
At present, there is no accepted definition to support clinical identification of when people with multimorbidity would benefit from a palliative care approach or are approaching the end of their lives. Advanced Multimorbidity is a term that could reasonably describe an individual with progressively deteriorating health due to their multiple long-term conditions. 17 Understanding how best to identify people with Advanced Multimorbidity would allow for a more reliable and coordinated approach to care which optimises quality of life with simultaneous planning for future deterioration.
Scoping review aim
This scoping review aimed to collate the available evidence on how people with Advanced Multimorbidity are described within the literature, with a view to identifying gaps in knowledge and making recommendations for future research.
Methods
This scoping review adhered to the Arksey and O’Malley framework for scoping reviews while referencing the Joanna Briggs Institute guidance and updates from Levac et al. – including refinement of the research question, ensuring appropriate expertise within the review team, and incorporating a more robust stakeholder consultation.18–20 It is reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR). 21 The protocol for this review has been published. 22
Scoping review methodology was chosen for this topic, given its role in conceptual mapping in healthcare, particularly in areas without universally agreed definitions. 23 In accordance with the scoping review guidance,18–20 this review followed the five stages detailed below.
Stage 1 – Identifying the research question
Advanced Multimorbidity was operationalised as the time period when the care of people with multimorbidity might usefully begin to transition from aiming to reverse or treat chronic conditions alone to encompass alleviating suffering and addressing multidimensional needs – in line with a ‘palliative care approach’. 16 This description of Advanced Multimorbidity is in accordance with research into other advanced illnesses24–26 and aligns with previously described definitions of Advanced Multimorbidity.17,27
Inclusion & exclusion criteria.

Stage 2 – Identifying relevant studies
A search strategy was developed collaboratively with the University of St Andrews library service – Supplemental File 1. This comprised search terms relating to multimorbidity, advanced illness and palliative care. The databases Medline, EMBASE, CINAHL, Scopus and PsychInfo were searched for published articles. A Grey Literature search took place to identify unpublished work, indexed theses, clinical guidelines and policies. Databases were searched from inception through to date of first search (22nd May 2023). Searches were updated on 11th March 2024. Searches were limited to the English language. Forward and backward citation searching was performed in all final included reports.
Stage 3 – Study selection
Searches were combined and deduplicated using EndNote software. Titles and abstracts were independently screened by two authors (SPB and either LM or DW). All full texts were independently reviewed by SPB with secondary review by PB, LM or DW. Any discrepancies were reviewed by a third reviewer and discussions held to reach consensus.
Stage 4 – Charting the data
Data were extracted from each included report by two independent reviewers (SPB and PB, LM or DW) into an Excel spreadsheet, inductively. This comprised details of the citation, design and population as well as the description of Advanced Multimorbidity derived from the report.
Stage 5 – Collating, summarising and reporting the results
Study characteristics were descriptively reported. Content analysis allowed for analysis of descriptions across different source material types (research studies and Grey Literature) to make reproducible and valid inferences.29,30 An inductive content analysis approach was chosen as this allows for categorisation when there is limited prior knowledge about the phenomenon of choice, in this case, a lack of definition of Advanced Multimorbidity. 30 The content analysis process is described in Supplemental File 2.
Stakeholder consultation
Stakeholder consultations are now seen as a crucial component to scoping reviews.
19
Consultation exercises were held with clinicians, academics and public advisors to interrogate the initial findings of the review and to develop some consensus around concepts of Advanced Multimorbidity and the utility of these. These exercises included: • Clinicians and academics consulted during a 2024 Academic Departments of General Practice in Scotland (ADEGS) conference presentation using electronic surveys to prompt discussions during and after the presentation. • An online focus group with our Public Advisory Group, comprising of six public advisors with a variety of lived experiences as bereaved caregivers, to ensure that the research was meaningful to their lived experiences.
Both stakeholder events involved the lead author (SPB) presenting the scoping review findings and asking delegates to provide feedback, followed by open discussion. Findings were brought to wider scoping review team meetings which included Public Advisory Group members, to drive the focus of the analysis and interpretation.
Patient & public involvement
In addition to the stakeholder consultation exercises undertaken, the Public Advisory Group for this project contributed to designing the review question, commented on and helped to shape the reporting of the review results and contributed to the manuscript – with one member (PC) listed as a contributing author on behalf of the group.
Results
Study selection
Study characteristics.


PRISMA flowchart for Scoping Reviews.
Study characteristics
Included articles were published between 1992 and 2023, with the majority (33/38) published after 2014. Eighteen studies were quantitative; five were reviews; four used mixed methods research; four were qualitative; three were editorials; and two were case studies. Additionally, two palliative care needs assessment tools were identified in the Grey Literature. No policy documents or guidelines with a description of Advanced Multimorbidity were identified.
Most studies which listed a country of recruitment of participants (or in the case of editorials, for authors) (n = 37) focussed on only one continent (n = 30) – 18 were in Europe, 11 North America and one Asia. Seven studies included multiple continents. Twenty-one studies included the age of participants with a mean age across these studies of 78.5 years. Only four studies reported patient and/or public involvement in their research.7,27,31,32
Descriptions of advanced multimorbidity
Descriptions of advanced multimorbidity.

aSame description.
bSame description.
The International Classification of Diseases (ICD)-9 code “Debility, unspecified”, was used in two different studies.33,34 Two studies performed secondary analysis of the same dataset using the same description – serious illness diagnosis with limited life expectancy (1 year or less as per physician assessment), functional impairment at baseline (Australian Karnofksy Performance Status <80%) and multimorbidity (Charlson Comorbidity Index ≥2 conditions)).35,36 Of note, this latter description was also used in two further studies.37,38 However as this was the same study team and same dataset as another included study 35 the decision was made to exclude these.
Whilst most studies only used one description, three studies used multiple descriptions (ranging from two to five descriptions) of Advanced Multimorbidity.27,39,40
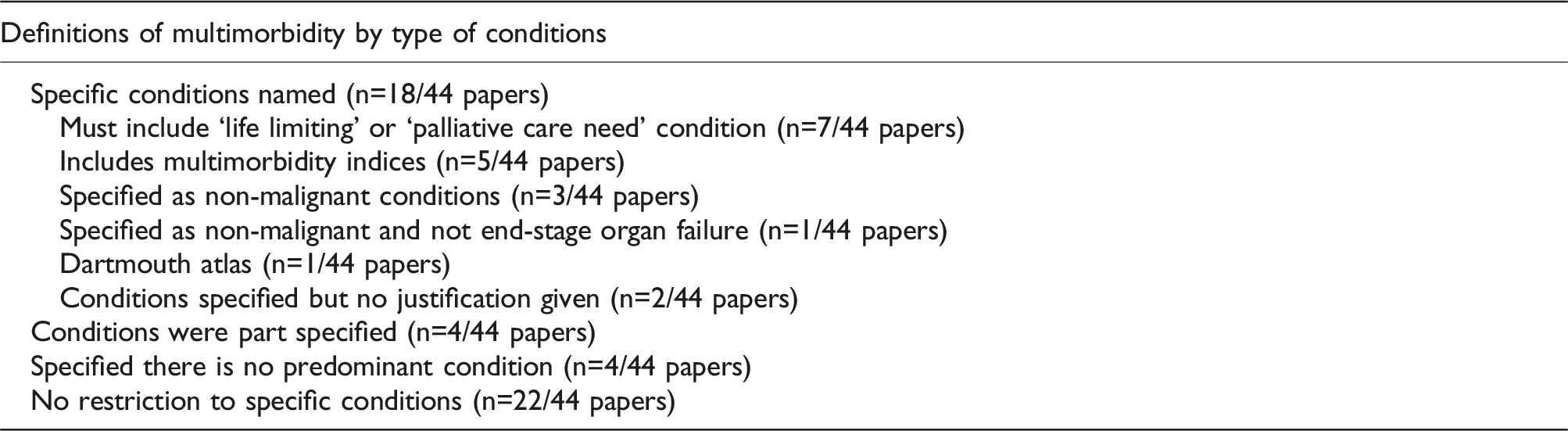
Types of conditions included in descriptions of advanced multimorbidity
Eighteen of the 44 descriptions used specific conditions in their description of Advanced Multimorbidity. Seven of these restricted their descriptions to only include conditions that were deemed to be ‘life-limiting’ or known to be associated with ‘palliative care need’.7,17,27,39 Five of these descriptions used multimorbidity indices – Charlson Comorbidity Index in three,35,36,41,42 Elixhauser Comorbidity Index in one 43 and one description amalgamated a number of indices. 44 Three descriptions specified that conditions must be non-malignant31,32,45 whilst another description specified that participants did not have cancer or end-stage organ failure as any of their conditions. 14 One description used conditions from the Dartmouth Atlas of Health Care report on Variation of End-of-Life Care. 46 The final two specified certain conditions, with no explicit justification for how these had been selected.47,48
Four descriptions part-specified conditions, e.g. at least one of the conditions had to be of a particular type – two of these, from the same study, 27 specified that one condition must be life-limiting and two49,50 specified participants must have at least one of the most prevalent chronic illnesses in the respective settings.
Additionally, four of the descriptions stipulated that there was no predominant condition which was driving a terminal decline prior to a diagnosis of Advanced Multimorbidity being made.14,33,34,51,52
Number of conditions required within descriptions of advanced multimorbidity

Approaches to the identification of advanced multimorbidity
Twenty-six descriptions took a multidimensional approach; incorporating a range of different indicators to identify and characterise Advanced Multimorbidity. These comprised between two and nine indicators per description. Palliative care needs assessment tools typically incorporated a greater number of indicators than research studies, with the Supportive and Palliative Care Indicators Tool (SPICT) 62 using six indicators, NECesidades PALiativas (NECPAL)49,51 using seven indicators and the Gold Standards Framework Proactive Identification Guidance 56 using nine indicators. There were 18 descriptions which used only one indicator to identify Advanced Multimorbidity.
Content analysis of advanced multimorbidity descriptions
Eleven discrete categories of indicators were identified within the 44 included descriptions of Advanced Multimorbidity: • Global assessments were in 17/44 descriptions, which encompassed holistic assessments of the patient’s health overall ○ 12/17 used practitioner assessment ○ 4/17 used self-identification ○ 3/17 used assessment tools • Functional assessments were in 16/44 • Age was in 15/44 • Pattern of healthcare utilisation was in 15/44 • Type of conditions was in 12/44 • Nutritional status was in 7/44 • Symptom burden was in 7/44 • Caregiver strain was in 5/44 • Clinical syndromes were in 3/44 • Benefit eligibility was in 2/44 • Responsiveness to treatments was in 2/44
Figure 2 summarises the interaction between the various indicators in the descriptions of Advanced Multimorbidity. As this figure shows, the most prevalent use of indicators overall within descriptions was using a single indicator approach of only condition type (n = 6), global assessment (n = 6) and age (n = 6). The most prevalent multidimensional descriptions all featured age plus either functional assessment (n = 3), holistic assessment (n = 3) or pattern of healthcare utilisation (n = 2). The remaining definitions each used different indicators either on their own or in combination. This figure details the various indicators included in the descriptions, with the number of definitions which involved each indicator and the frequency of particular combinations of indicators within the definitions.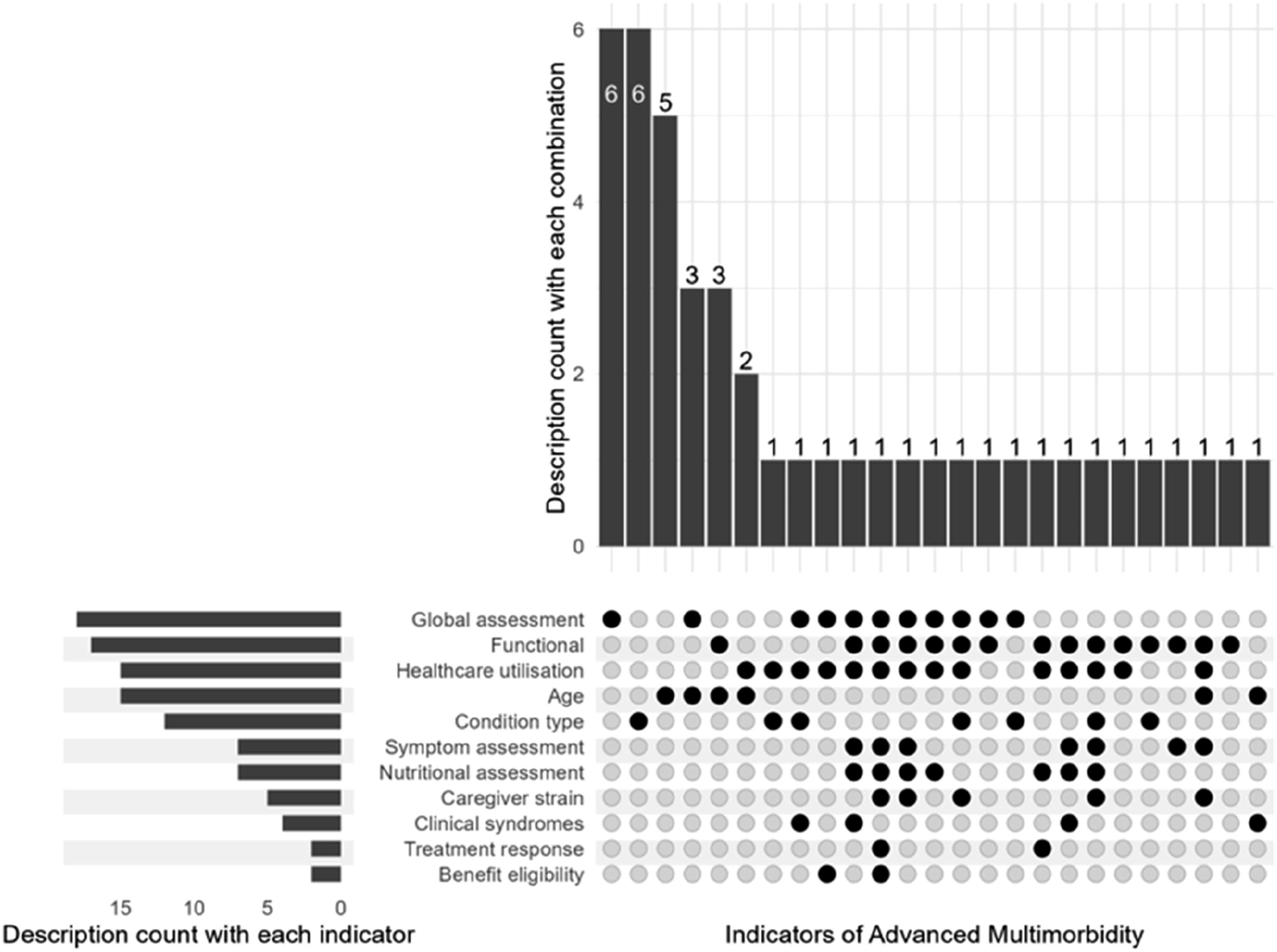
Supplemental File 2 describes in more detail how each of these indicators were used in the various descriptions of Advanced Multimorbidity.
Stakeholder consultation
Six public members and thirty-three clinicians and academics participated in stakeholder consultations. Most clinicians and academics felt that there was a role in defining Advanced Multimorbidity – 26 voted ‘yes’, three voted ‘maybe’, and six did not answer. Public advisors all agreed that a description could be useful, but expressed that one description may not suit everyone and were concerned a single description may be too restrictive and may exclude some individuals. Stakeholders felt that a description could be beneficial to a wide range of groups, citing patients, families, bereaved caregivers, healthcare professionals, researchers, healthcare systems and policymakers. Clinicians and academics felt an optimal description should be concise, uncomplicated, contain measurable indicators and ensure some focus on quality of life. Whilst public advisors felt that clinicians should be the ones to drive decisions around identifying Advanced Multimorbidity, they felt it was important that such descriptions were “user-friendly” and accessible and acceptable to patients and those close to them.
Discussion
The term “Advanced Multimorbidity” was chosen as the basis of this scoping review, recognising that it mirrors widely accepted clinical language used in other end-stage conditions such as advanced cancer 69 and advanced organ failure70,71 and reflects the chronic, incurable nature of such conditions. It has also already been used in previous research.17,27 Advances in treatments for both malignant and non-malignant conditions mean that many people are living longer with their incurable conditions,71,72 including multimorbidity. Whilst longer lives are often desirable, living with Advanced Multimorbidity is known to carry burdens for patients and their unpaid caregivers. 17 A palliative care approach has been shown to offer a range of meaningful benefits for people with advanced illness, but the challenge stands about how and when people with multimorbidity, whose burdens may be particularly high, and/or who may be nearing the end of life, can be reliably identified. A palliative care approach is known to benefit many individuals, not only those who are close to the end of their lives – with improvements in quality of life, healthcare utilisation and associated financial burden.15,73 However, much of the evidence base for the design and benefits of such palliative care approaches is limited to patients with single or discrete conditions, particularly cancer.73,74 The evidence base for the benefits of palliative care approaches in non-malignant and/or multiple conditions is more mixed, with less evident impacts on quality of life. 75 However, this difference may be more reflective of an underdevelopment of palliative care interventions for people with non-malignant disease and resultant less available evidence for symptom management in such groups, compared to e.g. pain management in cancer. 76 There remains a further paucity of evidence for implementing palliative care approaches for people with multimorbidity – despite evidence that this group has palliative care needs. 54 However, prior to developing palliative care interventions that could benefit those with Advanced Multimorbidity, we need to first establish how best to identify individuals who could benefit from such an approach. Understanding current definitions is foundational to this aspiration.
Terminology around multimorbidity is evolving at pace and can be confusing. There is undoubtedly some overlap, in practice, in what is understood to be ‘Advanced Multimorbidity’ and ‘complex multimorbidity’ – with this latter term associated with various working descriptions and ultimately describing when multiple long-term health conditions severely impact health. 77 It is said that complex multimorbidity can apply at any point in the life course, and indeed it has been used to encompass a wide range of outcomes from work productivity, disability and quality of life. Whilst it is not a term that is used in any consistent way clinically, it has been proposed as a means to identify those who would benefit from multimorbidity-focussed care. 77 Advanced Multimorbidity, as conceptualised in this review, differs in that it relates to individuals and populations who, by nature of their illness burden and/or proximity to death, may benefit from a palliative care approach.
The publications included in this scoping review were all relatively recent, reflecting both a surge in multimorbidity research and increased awareness of the relevance of palliative care beyond single illnesses such as cancer.78,79 There were no end-of-life care guidelines which specifically mentioned how to identify or treat people with multiple long-term conditions, although two palliative care needs assessment tools were identified that specified multimorbidity56,62 and one further tool was applied to a population with multimorbidity. 51 There were few studies which integrated patient and public involvement in their research. This was surprising given the increasing calls from the public, researchers and funding bodies alike to support such activities in recent years, driven by an understanding that collaborative approaches strengthen research relevance, quality and impact. 80
Age is heavily featured in many of the descriptions of Advanced Multimorbidity in the included studies, perhaps understandably, given that people typically accumulate conditions with advancing age. However, any reliance on age within a working definition could unhelpfully exclude individuals living with Advanced Multimorbidity at a younger age; a phenomenon associated with socioeconomically deprivation, with more deprived individuals shown to both develop multiple long-term conditions earlier81,82 and to have poorer health trajectories with earlier onset and more rapid progression of multimorbidity. 83
There were also descriptions which focussed on particular condition types to describe Advanced Multimorbidity, mainly encompassing conditions typically recognised as associated with palliative care needs, such as cancer and organ failure. 84 Whilst this disease-focused epidemiological approach has often been adopted in palliative care research, particularly around population estimates, 84 the feasibility and validity of its prospective application to individuals is unknown. Such a disease-specific approach risks excluding those without ‘typical’ palliative conditions yet with a cumulative disease burden, which means they could benefit from a palliative care approach.
Many of the descriptions included took a multidimensional approach, encompassing a broader, more holistic assessment of patients. The identified palliative care tools (NECPAL, 51 SPICT 62 and the Gold Standards Framework 56 ) used the highest number of indicators in their descriptions – perhaps reflective of these being utilised in clinical practice rather than in epidemiological research. Many of the commonly used indicators, such as functional assessment, healthcare use and type of condition, can typically be obtained from routinely collated healthcare data, which may have influenced the researchers’ choice in selecting them. There was little emphasis on utilising patient-reported outcomes, such as patient self-identification of advanced illness, symptom assessments and measures of caregiver strain, as a marker of Advanced Multimorbidity. Such assessments have become standard in clinical practice, yet are not routinely utilised for research purposes. In certain fields, such as Oncology, it has been shown that patient-reported outcome measures can be used to identify those who have specialist palliative care needs. 85 However, proactive use of measures of patient need requires identification that a person may benefit from such an assessment, knowledge of the assessment itself and time and resources to complete the assessment effectively. Nonetheless, our public and clinical stakeholders recommended that future measures of Advanced Multimorbidity should encompass patient and/or caregiver measures relating to quality of life.
The heterogeneity of descriptions described in this review echoes the lack of consistency in how people with multimorbidity are identified in clinical practice.
86
Greater consensus and standardisation of descriptions of Advanced Multimorbidity would allow for several potential benefits including: • Identification of people who may benefit from symptom assessments, consideration of their psychological and social needs and future care planning discussions • Shared decision-making opportunities supporting rationalisation and optimisation of current treatments with resultant reduction in medicalisation (a so-called Realistic Medicine’ approach
87
) for many
Furthermore, this could in turn improve system capacity to deliver preventative and potentially curative treatments for those who would benefit. Such a standardised approach to defining and identifying people with Advanced Multimorbidity would be relevant across a vast range of clinical specialities and teams, including, but not limited to, primary care, specialist palliative care and geriatric medicine, to align their practices in a way that is not currently the case. Future research, including prospective clinical studies and retrospective, epidemiological studies would also benefit from consistency of definition.
Strengths and limitations
This review was conducted in accordance with scoping review guidance and a pre-published protocol, ensuring it was both comprehensive and robust. 22 The only deviance from the protocol was in refining the research question to reflect the heterogeneity of studies included and to move away from describing definitions from research, policy and practice, as it was recognised no articles were identifiable from the latter two sources. It captured a wide variety of evidence sources, including Grey Literature. Despite this, no guidelines were identified which focussed specifically on care for people with Advanced Multimorbidity. This may have been due to the study eligibility criteria excluding more general end-of-life care guidelines, as these lacked a specific mention of multimorbidity. Such guidelines may indeed be applicable to those with Advanced Multimorbidity, but were out-with the scope of this review. Furthermore, studies examining multimorbidity (or comorbidity) in specific disease groups were excluded to maximise the generalizability of the findings to those with Advanced Multimorbidity. There may be further lessons to learn about how multimorbidity affects the end-of-life period in people with specific index conditions, such as dementia, cancer or organ failure. Attempts were made to synthesise the findings to provide a usable descriptor for Advanced Multimorbidity. However, the lack of consistency across the included studies was prohibitive. Therefore, this review has focussed on detailing and categorising the various descriptors instead. A further strength of this review is in the incorporation of stakeholder consultations and involvement of our Public Advisory Group from conceptualisation through to output to ensure this work is meaningful and relevant to patients and caregivers.
Conclusion
This review has highlighted a lack of consistency around how people with Advanced Multimorbidity are defined, described, and thus understood, both in clinical practice and research. Such heterogeneity of approach risks the under-identification of people who may benefit from discussions around future care planning and the consideration of a palliative care approach. In turn, this risks variation in care including poor care experiences and outcomes for many.
The reported definitions which were multidimensional in approach, combining multiple concurrent measures, offer considerable appeal and may be more likely to lead to a greater number of people being identified, whilst also supporting a more holistic assessment of individuals’ needs.
Further research in this important area is a necessity if we are to ensure that people living with Advanced Multimorbidity are to access the palliative care they need. Such research must include input from a variety of stakeholders, including people with lived experience, clinicians, researchers and policymakers. Future work could look to evaluate the predictive value of existing descriptions and develop novel multidimensional descriptors with person-centred, measurable variables included, building on the evidence gathered by this review. This could be aided further by consideration of multimorbidity as a broad concept, instead of distilling this down to discrete conditions co-existing. Furthermore, validation of future ways to identify those with Advanced Multimorbidity should be undertaken in diverse populations. Once robust methods of identifying Advanced Multimorbidity are established, the challenge for researchers, policymakers and clinicians lies in developing robust palliative care interventions fit to meet the needs of this diverse group. Ultimately, future work needs to be focused on delivering improvements in care as, in the words of a member of the studies’ Public Advisory Group: “it’s not just about defining something, it’s about improving the end of life for people”.
Supplemental Material
Supplemental Material - Descriptions of advanced multimorbidity: A scoping review with content analysis
Supplemental Material for Descriptions of advanced multimorbidity: A scoping review with content analysis by Sarah P Bowers, Polly Black, Lewis McCheyne, Darcy Wilson, Rose S Penfold, Liam Stapleton, Pam Channer, Sarah E E Mills, Linda Williams, Frances Quirk, and Jo Bowden in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
Author PC is a representative of our Public Advisory Group and part of the Fife Community Advisory Council within the University of St Andrews – we are immensely grateful for their ongoing commitment and guidance to this work. We are extremely grateful to Vicki Cormie, Senior Librarian at University of St Andrews, for her support and guidance in the development of the search strategy and to our public advisory team who have provided their expert lived opinion to the development of this scoping review. Particular thanks also to Rosie Dunn for her guidance on using content analysis within scoping reviews.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SPB is a current Editorial Fellow with the Journal of Multimorbidity & Comorbidity. SPB, PB and RSP are all fellows on the Multimorbidity Doctoral Training Programme for Health Professionals, which is supported by the Wellcome Trust (223499/Z/21/Z).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SPB, PB and RSP are all fellows on the Multimorbidity Doctoral Training Programme for Health Professionals, which is supported by the Wellcome Trust (223499/Z/21/Z). In order to meet institutional and research funder open access requirements, any accepted manuscript arising shall be open access under a Creative Commons Attribution (CC BY) reuse licence with zero embargo.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.