
Abstract
Background
Older people and people with dementia experience a high prevalence of multiple health conditions. The terms ‘comorbidity’ and ‘multimorbidity’ are often used interchangeably to describe this, however there are key conceptual differences between these terms and their definitions. This has led to issues in the validity and comparability of research findings, potentially inappropriate intervention development and differences in quality of health care.
Objective
To review how the terms ‘comorbidity’ and ‘multimorbidity’ are defined within peer-reviewed dementia research and propose an operational framework.
Design
A scoping review of definitions within dementia research was carried out. Searches took place across five databases: Academic Search Premier, CINAHL Complete, MEDLINE, PsycARTICLES and PsycINFO. PRISMA-ScR guidelines were followed.
Results
Content analysis revealed five key themes, showing significant overlap and inconsistencies from both within, and between, the comorbidity and multimorbidity definitions; 1. Number of conditions; 2. Type of health conditions; 3. The co-occurrence of conditions; 4. The inclusion of an index disease (or not); 5. Use of medical language. The analysis also revealed gaps in how the underlying concepts of the definitions relate to people with dementia living with multiple health conditions.
Conclusion
This scoping review found that current definitions of comorbidity and multimorbidity are heterogeneous, reductionist and disease-focussed. Recommendations are made on the design of research studies including transparency and consistency of any terms and definitions used. A syndemic framework could be a useful tool for researchers, clinicians and policy makers to consider a more holistic picture of a person with dementia’s health and wellbeing.
Introduction
Terms and definitions of multiple health conditions.

aNB various terms and definitions exist to describe multiple health conditions; the above are given here for illustration.
The lack of consensus around how to define these terms may cause conceptual and methodological differences in research. For example, researchers may differ in the number of conditions considered, the type of conditions considered relevant (e.g. physical, psychological, social health), or whether the research is centred around an index condition or whether all conditions are considered equally (see Table 1). This can create difficulties in making valid or reliable interpretations of findings across studies, and ultimately apply research into practice.
Dementia is a complex, neurodegenerative condition in which no two people may experience the same symptoms or progress in the same way. 17 Dementia is not a disease; it is a syndrome – an umbrella term for a cluster of symptoms which can be understood from a combination of biological, psychological and social perspectives. 18 There are over one hundred different types of dementia 19 that can affect different parts of the brain and result in both varying and overlapping symptoms from one type of dementia to another. 20 For example, a person diagnosed with Alzheimer’s Disease may experience difficulties with short term memory, judgement and planning, 21 whereas a person diagnosed with frontotemporal dementia may experience changes in personality, behaviour and movement problems. 22
In addition, the symptoms, behaviours or emotions that PwD experience may not always be caused by dementia, but can be due to other underlying or misdiagnosed conditions that may present with similar, overlapping symptoms as dementia, such as depression, diabetes or a urinary tract infection. 23 This is referred to as diagnostic overshadowing, where symptoms or behaviours are assumed to be caused by dementia. 24 It can be difficult for healthcare practitioners, carers and PwD themselves to identify what is thought to be caused by dementia, and what is the result of other underlying conditions. Furthermore, some behaviours experienced by PwD may not necessarily be caused by dementia or have a biological origin, but are due to unmet care needs.25,26
There are estimated to be between 850,000 to one million people living with dementia in the UK. 27 As of May 2022, dementia remained the leading cause of death in England. 28 There is a significant lack of support following a dementia diagnosis 29 as well as funding in comparison to other health conditions, such as cancer and coronary heart disease (CHD). 30 Yet dementia costs the health and social care system more than cancer, CHD and stroke combined. 30 PwD aged 65 or above are more likely to have a higher prevalence of multiple health conditions than those that do not have dementia. 31 However, PwD are less likely to receive primary, preventative health care 32 or receive treatment for other co-existing conditions, for example, older people living with dementia and cancer are less likely to be offered chemotherapy or diagnostic testing compared to those with cancer but without dementia. 33 Additionally, PwD often take multiple medications and are at risk of polypharmacy, 34 which has been linked to faster functional decline in PwD. 35 The National Institute of Health and Care Excellence (NICE) Multimorbidity guidelines state that the management of multimorbidity is more problematic in the presence of dementia and that careful consideration of any benefits or harms of interventions is required. 36 Overall, the above complexities of this syndrome warrant further investigation into how to conceptualise the ‘multimorbidity’ paradigm for people living with dementia.
In sum, there are many different terms and definitions used to describe people living with multiple health conditions. Indeed, this journal has renamed itself from the Journal of Comorbidity to the Journal of Multimorbidity and Comorbidity, in recognition of the distinction between comorbidity and multimorbidity as two separate concepts. 37 Furthering our understanding of these concepts will potentially help us to ‘improve research into the phenomenon of ill health in clinical care, epidemiology, and health services’, 4 improve intervention development 1 , as well as promote a shared language between healthcare practitioners and people living with multiple health conditions. 38 Given the complexity of dementia, it is important to review how to conceptualise the terms and definitions of living with ‘multiple health conditions’ in this group. Therefore, the overall aim of this review is to explore how ‘multiple health conditions’ are conceptualised in people living with dementia within published dementia research. The findings will be used to develop an operational framework that conceptualises the ‘multiple health conditions’ paradigm in PwD to guide future research, policy and clinical practice in dementia care.
The Population-Concept-Context framework (PCC) was used 39 to guide the focus of the review and to formulate the following research question: How is comorbidity and multimorbidity defined in relation to PwD within peer-reviewed dementia research and what are the key conceptual components that form these definitions?
Method
A conceptual mapping scoping review was conducted, which is ‘a scoping study designed to establish how a particular term is used in what literature, by whom and for what purpose’. 40 Unlike a systematic review, which aims to synthesise findings from a narrow range of quality-assessed studies, a scoping review is a systematic approach to mapping the research evidence of a particular field and identify gaps in the literature. 41
The Arksey and O’Malley 41 scoping review framework was used, which consists of the following five iterative steps: 1: identifying the research question, 2: identifying relevant studies, 3: study selection, 4: charting the data and 5: collating, summarising and reporting the results. Recommendations made by Levac et al. 42 that extend and clarify steps one to five of the Arksey and O’Malley framework were also incorporated. Particular attention was paid to the recommendations made on ‘balancing feasibility with breadth and comprehensiveness; using an iterative team approach to select studies and extract data; incorporating a numerical summary and qualitative thematic analysis; identifying the implications of the study findings for policy, practice, or research and adopting consultation as a required component of scoping study methodology’. 42 Finally, the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews [PRISMA-ScR] Checklist 43 was used to ensure all of the relevant aspects required of a high-quality scoping review were completed (see Supplementary file 1).
Search strategy
The search strategy was developed with support from an Information Specialist. Five databases were searched from inception to 22nd March 2022, using EBSCOhost: Academic Search Premier, CINAHL Complete, MEDLINE, PsycARTICLES and PsycINFO. These search engines were chosen as they cover multi-disciplinary research articles from nursing, allied health, medicine and psychology disciplines. The following search terms were used: “comorbid*” OR “co-morbid*” OR “multimorbid*” OR “multi-morbid*” AND “dement*” OR “alzheimer*”.
An initial search was carried out using EBSCOhost within the five databases outlined above, for each of the terms given in Table 1. ‘Comorbidity’ and ‘multimorbidity’ produced the most results – comorbid* produced 644, 957 results, and multimorbid* produced 18, 377 results (as of 22nd March 2022). Therefore, in order to balance feasibility and breadth of the review as recommended by Levac et al. 42 the search terms were restricted to ‘comorbidity’ and ‘multimorbidity’ (the field code for these search terms was retained as ‘optional’ in order to retrieve papers from any indexed field) and the other terms described in Table 1 were not included in this review. The dementia search terms however were limited to ‘TI’ (Title), in order to reduce irrelevant papers. Additionally, the papers were limited to retrieve English language only papers at the start of the search, as translation facilities were not available. The papers identified through EBSCOhost were imported to EndNote bibliographic software 44 and duplicate papers were removed.
Inclusion and exclusion criteria
The title and abstracts of the retrieved papers were screened by two authors (RD and EC) according to the PCC framework. 39 Articles were included if they involved people living with dementia (Population); investigated or discussed comorbidity or multimorbidity in dementia (Concept) and were any type of study (e.g. case study, review) written in English (Context). After excluding papers according to the above criteria, the remaining papers were discussed with the team of authors. As there were thousands of papers still left to review following this first stage of screening, a further criterion was set to only include papers that were peer-reviewed journal articles, excluding books, theses, protocols and grey literature (Context). This made the review more feasible whilst still balancing breadth within the scoping review as recommended by Levac et al. 42 In addition, a quality assessment of included papers is not usually carried out in a scoping review41,42 however the inclusion of peer-reviewed papers only should theoretically be research that is published of a high quality. 45
The full text of the remaining articles was reviewed. Papers were included for final review if they contained a definition of comorbidity and/or multimorbidity and the research aims explicitly addressed comorbidity or multimorbidity within the research. The British library were contacted to obtain the full text of papers that were not available online; authors were contacted directly if they were not available from the British library. No restrictions were placed on the type of study or year of publication since it was important to gather a broad scope of the definitions used in the literature. Citation tracking and a hand search of the references of the final review papers were checked according to the above inclusion and exclusion criteria.
Data charting and analysis
A data charting form was developed to extract relevant data from the articles. 39 The charting form was used to extract data on two articles initially, then reviewed and updated iteratively following discussion with the team of authors. Data were extracted on the study characteristics (authors, year and location); the type of research design (e.g. case study, review); the aim of the research; the comorbidity and/or multimorbidity definition used; the reference given for the definition (if one was used); whether the reference given was in the field of dementia; the number and age of PwD (if applicable) and the number and type of health conditions researched in PwD (if reported). Inductive content analysis was used to analyse the definitions. This method was chosen as it is a systematic and flexible approach that allows the researcher to describe and quantify phenomena and extract meaning from textual data into content-related categories. 46 Content analysis was conducted following three main phases: preparation, organisation and reporting.
Phase 1: Preparation
The comorbidity and multimorbidity definitions were extracted from the papers and split into two separate tables to be analysed independently. The comorbidity definitions were analysed first; they were read several times to allow the author (RD) to make sense of the data and identify units of analysis. This consisted of words or phrases that had some meaning or relevance to the research question and reoccurred across the definitions. This process was repeated for the multimorbidity definitions.
Phase 2: Organisation
Open coding was carried out on the comorbidity definitions, and categories were developed where units of analysis reoccurred across the definitions. Numerical counts of the categories were made to enable comparisons between the data. The categories were then grouped into higher order headings. This process was repeated for the multimorbidity definitions.
Phase 3: Reporting
The final list of headings were developed by the author (RD) and then discussed with the team of authors (EC, EW and AH). The higher order headings were compared and contrasted across the comorbidity and multimorbidity definitions and described narratively.
Consultation
Arksey and O’Malley 41 and Levac et al. 42 recommend consulting with key stakeholders in order to glean insights beyond those found in the literature, thereby improving the methodological rigour of the scoping review process. The consultation therefore acts as a form of knowledge transfer, and provides the opportunity to share additional sources of information, perspectives, validation and meaning. The content analysis of the definitions were presented by the lead author (RD) to a special interest group in multimorbidity, who are also health and social care practitioners with many years’ experience of working with PwD and their supporters. A discussion of the findings took place and any additional insights or observations made from the consultation group members were documented by RD. The feedback from the consultation along with the content analysis of the definitions were used to co-create an operational framework that conceptualises the ‘multiple health conditions’ paradigm in PwD.
Ethics approval
Not applicable
Results
Figure 1 summarises the flow of the screening process. Initial searches found 8894 papers. Following the screening of titles, abstracts and full texts, 30 papers were included for final review that contained a definition of comorbidity or multimorbidity in relation to PwD. PRISMA Flow Diagram.
47

Study and participant characteristics
The majority of the papers were European (N = 24). Nearly two thirds of the study designs were observational (N = 18), ten of which were cohort studies, six were cross-sectional and two case control studies. Eight papers were reviews, two were case studies, one was a mixed methods study and one was an exploratory, qualitative study. The median (IQR) number of PwD recruited in the studies was 579.5 (6405.5) and the mean age (SD) was 80.4 years (± 4.4). Further details and references of the study and participant characteristics are available in supplementary files 2 and 3.
Comorbidity and multimorbidity research aims and definitions
Of the 30 papers reviewed, 23 papers aimed to explore or discuss comorbidity in PwD and only six papers had the specific research aim of exploring multimorbidity in PwD. One paper 48 uses both terms interchangeably within their research aim. Of the 23 papers that aimed to explore comorbidity, 15 papers provided a definition for comorbidity, five papers provided definitions for both comorbidity and multimorbidity, and three papers provided a definition for multimorbidity, even though the study aim was to research comorbidity.49–51 Of the six papers that aimed to explore multimorbidity in PwD, five papers provided a definition for multimorbidity, and one paper provided definitions for both multimorbidity and comorbidity (see Supplementary file 3 for references pertaining to detailed study characteristics).
Comorbidity definitions.

*a priori indicates this is the researchers own definition.
†National Institute for Health and Care Excellence
Multimorbidity definitions.

*a priori indicates this is the researchers own definition.
†National Institute for Health and Care Excellence
Analysis of comorbidity and multimorbidity definitions
Content analysis of the extracted definitions revealed five key themes, showing significant overlap and inconsistencies from both within, and between, the comorbidity and multimorbidity definitions.
Type of health conditions
73% (N = 16) of comorbidity definitions48,52–66 and 53% (N = 8) of multimorbidity definitions48–51,62,65,67,68 did not provide a description of the specific types of conditions they intended to explore. 27% (N = 6) of comorbidity definitions67,69–73 and 40% (N = 6) of multimorbidity definitions69,71,74–77 described the presence of ‘chronic’ or ‘long-term’ conditions, as part of the concept. Only one multimorbidity definition considered both chronic and acute conditions within the concept. 53
Looking beyond the definitions, and only at studies that included participant data, 15 studies measured or identified specific conditions within a population of PwD49,50,52,54,56,57,60,62,64–66,68,69,71,75 and five studies recorded any condition in a person with dementia58,61,63,74,76. The majority of these conditions appeared to be chronic and varied greatly between studies (see supplementary files 2 and 3 for further information). Eight studies used the International Classification of Diseases, Ninth Revision Clinical Modification [ICD-9-CM] 78 and the International Classification of Diseases, Tenth Revision 79 [ICD-10],49,50,58,62,63,71,72,75 six studies used comorbidity indexes, such as the Charlson Comorbidity Index (CCI)52,57,60,64,65,68, three studies used electronic health records61,69,74 and one study used death certificates, 56 in order to identify and code conditions in PwD.
Co-occurrence of conditions
36% (N = 8) of comorbidity definitions described the simultaneous, ‘co-occurrence’ or ‘co-existence’ of conditions within an individual.48,55,56,59,60,64,65,73 Similarly, 67% (N = 10) of multimorbidity definitions described the ‘co-occurrence’ of conditions48,51,53,62,65,68,71,74,75,77 14% (N = 3) of comorbidity definitions described a temporal aspect to the definition, where the presence of one condition may influence the onset of another, or occur during the course of one condition52,58,73 and 13% (N = 2) of multimorbidity definitions referred to the idea that health conditions ‘may or may not be linked by a causal relationship’ 65 or ‘which may or may not directly interact with each other’. 48
Biomedical use of language
100% (N = 37) of the comorbidity and multimorbidity definitions used medical language, for example ‘disease’, ‘condition’, ‘health/medical condition’, ‘pathology’, ‘disorder’, ‘clinical condition’, ‘ailment’, ‘somatic’, ‘diagnosis’ and ‘symptoms’. However, only two comorbidity definitions referred to mental health within the concept; Aldridge and Harrison Dening 80 provided ‘schizophrenia’ as an example and Heun et al. 61 described it as a ‘mental disorder’. Similarly, only two multimorbidity definitions referred to mental health within their definitions, framed as ‘psychiatric conditions’.48,53
The number of conditions
There were inconsistencies within comorbidity definitions regarding how many conditions constituted comorbidity. 32% (N = 7) of comorbidity definitions implied that comorbidity is the presence of a condition in addition to an index disease (not necessarily dementia) within a person, indicating the co-existence of two conditions48,55,57,59,62,70,71. However, 27% (N = 6) of comorbidity definitions stated ‘two or more’ or ‘more than one’53,54,63,67,69,72 and 14% (N = 3) stated ‘several’, ‘multiple’ or ‘an accumulation’52,56,71. 27% (N = 6) of comorbidity definitions do not specify a number58,60,61,64–66. In contrast, 67% (N = 10) of the multimorbidity definitions stated ‘two or more’48–51,65,67,69,71,74,76 and 33% (N = 5) stated ‘multiple’ or ‘several’.53,62,68,75,77
The inclusion of an index disease
55% (N = 12) of comorbidity definitions described the inclusion of one condition as an ‘index disease’ that ‘assumes a central place’48,52,53,58,59,62,63,65,66,69,71,73. Although not explicitly stated within the definitions, seven papers identified dementia as the primary index disease elsewhere within the research48,52,58,59,62,65,73 however one paper explicitly excluded dementia as the primary index condition within the definition 69 and one paper chose to explore comorbidities across three index conditions; diabetes, dementia and stroke. 71 33% (N = 5) of multimorbidity definitions described multimorbidity as where ‘one condition is not necessarily more central than the other’ or that there is ‘no consistent dominant index disorder’ 48,51,53,65,71 67% (N = 10) multimorbidity definitions did not make a distinction as to whether one condition assumed a central place or whether conditions were considered equally.
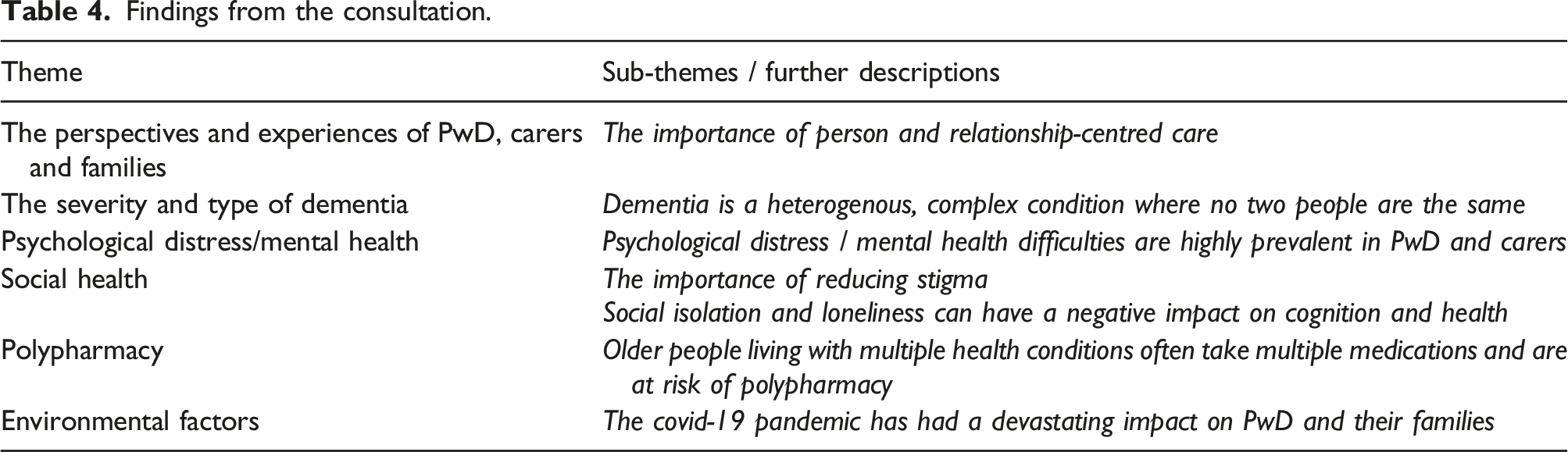
Consultation
Findings from the consultation.
Discussion
This scoping review found that the definitions used in the dementia literature are heterogeneous, reductionist and disease-focussed, with considerable overlap and inconsistencies from both within and between the different definitions. Crucially, there were many elements and concepts missing from these definitions that failed to capture aspects that are important to consider in the health and wellbeing of PwD.
Type of health conditions
Limited details were reported on the types of health conditions considered within the various definitions, and consequently within the overall study. There was a reliance on the use of classification systems such as the ICD-9-CM, 78 the ICD-10 79 and electronic health records. However, there are limitations to using these methods of measuring comorbidity or multimorbidity. For example, the ICD-10 has over 70,000 codes 79 and the more recent version, ICD-11, has over 120,000 codes; 18 how do researchers decide on which ones to use? None of the studies in this review provided a justification for how or why they chose these conditions, or why they chose to use certain methods to measure comorbidity or multimorbidity over others (e.g. the choice to use ICD-10 codes, the CCI or electronic health records). The lack of clarification reported in studies on the types of conditions included and the reasons behind their choices may have implications for research reproducibility and comparability; what one researcher considers a ‘condition’ another may not, for example ‘substance misuse’. 87
Acute, ‘short-term’ conditions, such as urinary tract infections or pneumonia are common in PwD, but can often go undetected, either because the person with dementia is unable to report the symptoms or because the healthcare professional or carer mistakes those symptoms as symptoms of dementia. 88 If left untreated, acute illnesses can lead to serious health issues, for example a urinary tract infection left untreated can lead to delirium (the symptoms of delirium can be very similar to those of dementia). 89 The onset of delirium can speed up the progression of dementia, and some people never fully return to their previous cognitive ability.90,91 Furthermore, the rate of mortality is high in PwD following acute illness; 92 indeed, the recent Coronavirus 2019 (COVID-19) pandemic has shown that PwD are at an increased risk from contracting the virus, including an increased risk of hospitalisation, psychological and cognitive decline and mortality.93–95 The results from this scoping review found that comorbidity and multimorbidity definitions mainly included ‘chronic’ or ‘long-term conditions’, which can be defined as ‘a condition that cannot, at present, be cured but is controlled by medication and/or other treatment or therapies’. 11 However, the detection and treatment of acute conditions in PwD is paramount to prevent further decline and mortality, and should be considered along with chronic conditions within the concept.
In addition, PwD may also experience ‘borderline’ conditions and ‘episodic’ conditions. Borderline conditions are not clinically diagnosed, yet people are often told by healthcare professionals that they are ‘borderline diabetic’, or their blood pressure is ‘borderline’. 96 There is a lack of clinical diagnosis here, yet some kind of action or treatment is required for the person to improve and potentially recover (the opposite to the definition of ‘chronic’). Likewise, some people may experience ‘episodic’ conditions, such as certain types of cancers or depression, in which a course of treatment is required and the person may recover. For example, a person diagnosed with early-stages of prostate cancer may undergo a radical prostatectomy, and then be cancer-free. Or a person experiencing depression may receive counselling or treatment and their symptoms may improve (depression is very common in PwD 97 ). These are serious conditions which if left untreated, could result in further decline or death. Excluding them from concepts such as comorbidity and multimorbidity due to not fitting into the ‘chronic’ or ‘long-term’ caveat is a significant oversight in the context of dementia.
Co-occurrence of conditions
The idea of ‘simultaneous’ or ‘co-occurring’ conditions implies that people experience health conditions at the same time. However, some health conditions may act as a prodrome to the onset of another condition, some can occur later as a consequence of developing a condition and some may occur completely independently. For example, research evidence has demonstrated that depression in later life can act as a prodrome to developing dementia, it can occur as a consequence of dementia, or it can be a completely separate condition to dementia in its own right. 98 Studies have also found that other conditions increase the risk of dementia. For example, diabetes increases the risk of developing mild cognitive impairment (MCI) and progression from MCI to dementia. 99 Likewise, PwD appear to experience a higher prevalence of brain diseases, infections and eating disorders compared to age-matched control subjects 48,52,58,61,65,73
In addition, research has found that people’s symptoms, experiences or conditions can fluctuate from day to day. 96 For example, a person living with arthritis and diabetes may find that their arthritis is the most troublesome condition on one day, perhaps due to an increase in pain, and then on a different day find that managing their blood glucose levels are more problematic. Other days they may find they are managing both conditions well. This resonates with Leder’s 100 phenomenological work on the ‘dys’-appearing body, in which he distinguishes between bodily ‘dis’-appearance, where one is not aware of their body and its functions, and bodily ‘dys’-appearance, where one is very much aware of their body and perceives it as ‘ill’ or ‘bad’. Similarly, the Shifting Perspectives Model 101 posits that people’s perspectives of chronic illness ‘shift in the degree to which illness is in the foreground or background of their “world.”’. 101 Health status, therefore, is not a static concept that can be described as ‘simultaneous’ or ‘concurrent’ – it is a process that fluctuates, with peaks and troughs of improvements and decline. Definitions of comorbidity or multimorbidity should therefore avoid the use of describing conditions as ‘simultaneous’ or ‘co-occurring’, and include the potential for interaction or causation within the concept. See, for example, the two multimorbidity definitions that referred to the idea that health conditions ‘may or may not be linked by a causal relationship’ 65 or ‘which may or may not directly interact with each other’. 48
Biomedical use of language
The use of medical language implies the sole inclusion of pathological or physical health conditions, and arguably excludes other potential health aspects within the concept, such as psychological or social factors, which are important indicators in a person’s overall health and wellbeing. For example, the renowned biopsychosocial model of health, developed by George Engel 102 stated that interactions between biological (genetic make-up), psychological (mental health and behaviours), and social factors (e.g. culture and relationships) determine the cause, manifestation, and outcome of wellness and disease. However, this review found that the definitions used predominantly biomedical language, with a notable lack of psychological and social health inclusion.
The use of language here is relevant for two reasons. Firstly, the medical language used promotes the biomedical stance that a person’s overall health can be reduced to distinct disease entities that are biological in nature. However qualitative research on older adults living with multiple health conditions has shown that some people reject this notion of ‘illness’ and view their health in terms of how it affects their everyday life, rather than a list of diseases. 96 Research has found that mental health problems are highly prevalent in both PwD and carers,103,104 and how psychological distress experienced by carers can have a negative impact on the physical health outcomes of PwD. 105 Additionally, social isolation and loneliness has been found to negatively affect cognition and mental health in PwD, as observed from the social restrictions and lockdowns due to the COVID-19 pandemic. 95 The importance of promoting psychological and social health in PwD has been widely documented through research and policy,106–109 however the results from this scoping review show that these areas are neglected from current concepts of comorbidity or multimorbidity in dementia research.
Secondly, the use of language is important because low health literacy is linked to poorer health outcomes. Older people, black and ethnic minority groups, those without English as a first language, those with low job or education status and those in the poverty trap have low health literacy skills. 38 Additionally, PwD often experience cognitive issues such as the ability to recall and store information, sustain attention and make decisions. 18 It is important therefore that healthcare practitioners adapt their communication style and use language that is person-centred, easy to understand and follow, and holistically considers the patient’s perspectives of their health and wellbeing.
The number of conditions and the inclusion of an index disease
There was variation in the number of conditions that warrant ‘comorbidity’ or ‘multimorbidity’ (i.e. the co-existence of just two conditions, versus more than two, versus ‘multiple’ / ‘several’). There was also ambiguity and discrepancies from both between and within the various comorbidity and multimorbidity definitions regarding whether there is an index disease or not (and how researchers decide on which condition to explore as the primary index condition if they do). These inconsistencies make it difficult to replicate research findings or make cross comparisons across data sets. 1
As aforementioned, an index disease refers to a primary condition of interest. 8 However, the primary condition of interest may differ depending on the aims of the research, the type of healthcare practitioner, or whether they work in a specialist or generalist setting. For example, if a patient was diagnosed with dementia, diabetes and heart disease, a specialist such as an endocrinologist would consider diabetes as the primary index disease, with comorbid dementia and heart disease. In contrast, a generalist working in primary care would have a more holistic, person-centred approach, and would focus on the overall health of the individual, listening to their priorities and preferences for treatment. However, the majority of health care is designed around the singular index disease model, meaning people living with dementia and/or multiple health conditions often experience fragmented care. 110
The primary condition of interest may also differ according to the perspectives of the person experiencing multiple health conditions or the person’s family or carer. For example, a person living with dementia, arthritis and diabetes may consider their primary index condition to be arthritis, which is causing them pain and discomfort. In contrast, the carer may consider the diabetes as the primary condition, due to difficulties in administering medication or managing their diet. Indeed, PwD and carers have voiced that dementia is not always the biggest concern; ‘It was acknowledged that people are often living with multiple conditions, not just dementia. Other conditions can be more debilitating than dementia, and can affect end of life planning’. 111 It is important therefore that the perspectives and experiences of PwD, carers and families are considered in order to provide person and relationship-centred care.26,112,113
As previously discussed, people may experience fluctuations in relation to their symptom severity when living with multiple health conditions, and some health conditions can be mistaken for others (i.e. diagnostic overshadowing). Therefore, research conducted on multiple health conditions, underpinned by a definition describing the inclusion of a primary index condition that ‘assumes a central place’, may not be appropriate (however this would depend on the research aims).
There have been calls to action in order to standardise comorbidity and multimorbidity definitions going back as far as 1996 5 . Over twenty years later, Nguyen et al. (2019) state: ‘The need for a consistent operationalisation of multimorbidity is evident. It will enable more accurate estimations of disease burden and, consequently, more effective disease management and resources distribution’. 114 However, despite attempts to standardise definitions3,5,7 or operationalise a measurement of multimorbidity 115 the results from this scoping review demonstrate that there is still a lack of consensus around how to define these concepts, at least within peer-reviewed dementia research.
It is difficult to determine conclusively why inconsistencies between the terms and definitions exist, however it is possible that differences may occur due to variations in subjective views according to professional discipline (e.g. biomedical, psychological or social care practitioners), what researchers believe counts as a ‘health condition’ or due to the aims of the research. Additionally, although translations have been attempted across different countries for these terms and definitions 3 the application and accuracy of these terms and definitions may vary internationally. A singular term or definition therefore may not be appropriate to explain such a complex area. However, an operational framework could be a useful approach when a standard definition does not suffice to explain a phenomenon of interest. 116
The findings from the consultation along with the gaps highlighted from the content analysis of the definitions, led to the development of a syndemic framework during an iterative process. A syndemic (synergistic-endemic) approach to health acknowledges that conditions do not just exist in parallel, and involves the interaction and consequences of biological, social, environmental, economic and lifestyle factors; 117 ‘Syndemics involve the adverse interaction between diseases and health conditions of all types (e.g. infections, chronic non-communicable diseases, mental health problems, behavioural conditions, toxic exposure, and malnutrition) and are most likely to emerge under conditions of health inequality caused by poverty, stigmatisation, stress, or structural violence’. 118 Dementia is increasingly being recognised as a syndemic disorder, given that PwD commonly live with several conditions or symptoms, the interaction of which can have greater consequences that singular conditions alone.119,120
Drawing from the results of this scoping review, in conjunction with syndemic theory, a syndemic framework is proposed in order to provide a more useful way of conceptualising ‘multiple health conditions’ in PwD, to be used by researchers, healthcare professionals and policy-makers (see Figure 2). Syndemic framework of health in dementia.
This syndemic framework does not serve to replace the comorbidity or multimorbidity definitions, rather to enhance our understanding and reflect on what is important when conducting research or providing care to a person living with dementia and multiple health conditions.
Strengths and limitations
In order to make the review feasible 42 only peer-reviewed journal articles were included, and books, theses, policies and grey literature were excluded. Therefore, some definitions may have been missed. Additionally, concepts of other terms used to describe people living with multiple health conditions, such as ‘long-term conditions’ or ‘patient complexity’, were not explored. This review focussed on the terms and definitions and did not review the methods or evaluation tools that may have been used by some studies, for example, CCI or ICD-10 codes. 79 As aforementioned, other potential reasons to further explain conceptual differences across definitions could be due to differences in research aims (e.g. risk factor assessment, outcome prediction, effectiveness of interventions), in the time-scales considered, in data availability and professional discipline. A full-scale analysis comparing these features with the authors’ definitions was beyond the scope of this review. However further analysis could be carried out in the future by extracting some of the data available from Supplementary file 3. Finally, the majority of papers found in the review were European (N = 24); we were only able to include English language papers as translation facilities were not available. This review had several strengths, however. Firstly, the review was conducted in a highly systematic approach, following comprehensive scoping review guidelines including Arksey and O'Malley, 41 Levac et al., 42 Joanna Briggs Institute [JBI] 39 and the PRISMA-ScR Checklist. 43 The screening process and review of included papers were discussed as a research team, ensuring high content validity. Additionally, the scoping review findings were discussed in consultation with dementia experts, in order to enhance our understanding further and create a useful framework that may help researchers, clinicians and policy-makers reflect beyond simplistic definitions.
Implications for research and practice
The key recommendations from this review are: • To clearly state which health conditions are chosen to be researched and give clear reasons as to why they were included or excluded. • To give a clear rationale as to why a particular method of measuring comorbidity or multimorbidity is chosen over another, for example if a researcher wishes to use the Charlson Comorbidity Index or ICD-11 codes.
18
(Lee et al., 2021 provide a list of multimorbidity instruments that can be used to measure against specific outcomes).
121
• To use the syndemic framework proposed from this review to reflect on the choices made when carrying out health-related research. • To be consistent with any terms and definitions used, recognising the distinction between comorbidity and multimorbidity, as highlighted by Harrison et al.
37
but to also acknowledge the limitations posed (as highlighted from this review) when you use these terms and definitions.
Future research could explore PwD and carers’ perspectives on the language and definitions used to describe living with multiple health conditions as well as review and validate the syndemic framework. Further qualitative research is also required to explore the experiences of PwD and their carers living with other multiple health conditions.
Conclusion
This is the first scoping review to examine the definitions used to describe comorbidity and multimorbidity in dementia research. This scoping review found that current definitions of comorbidity and multimorbidity are heterogeneous, reductionist and disease-focussed, and fail to accurately reflect the health and wellbeing of people with dementia. A syndemic framework of health could be more usefully applied in health research, rather than reducing health into single disease entities. Although this research has concentrated on the field of dementia, the framework could be adapted to all health issues, and acts as a source of reflection for health and social care researchers.
Supplemental Material
Supplemental Material - Conceptualising comorbidity and multimorbidity in dementia: A scoping review and syndemic framework
Supplemental Material for Conceptualising comorbidity and multimorbidity in dementia: A scoping review and syndemic framework by Rosie Dunn, Eleanor Clayton, Emma Wolverson and Andrea Hilton in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Conceptualising comorbidity and multimorbidity in dementia: A scoping review and syndemic framework
Supplemental Material for Conceptualising comorbidity and multimorbidity in dementia: A scoping review and syndemic framework by Rosie Dunn, Eleanor Clayton, Emma Wolverson and Andrea Hilton in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - Conceptualising comorbidity and multimorbidity in dementia: A scoping review and syndemic framework
Supplemental Material for Conceptualising comorbidity and multimorbidity in dementia: A scoping review and syndemic framework by Rosie Dunn, Eleanor Clayton, Emma Wolverson and Andrea Hilton in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
We would like to thank Fiona Ware, Information Specialist, for her advice on the literature search and Rosie Connell, graphic designer, for her help in designing the syndemic framework illustration.
Author contributions
RD conceptualised the study, conducted the literature search, screening of articles, analysis, developed the syndemic framework and drafted the article. EC assisted in the literature search, screening of articles, reviewed the analysis and syndemic framework, critically edited the manuscript and approved the final version. EW and AH contributed to the design of the study, reviewed the analysis and syndemic framework, critically edited the manuscript and approved the final version.
Declarations of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.