
Abstract
Background
Multidisciplinary Teams (MDTs) has been suggested as an intervention to overcome some of the complexities experienced by people with diabetes and comorbidities in terms of diagnosis and treatment. However, evidence concerning MDTs within the diabetes field remains sparse.
Objective
This review aims to identify and map available evidence on key characteristics of MDTs in the context of diagnosis and treatment in people with diabetes and comorbidities.
Methods
This review followed the PRISMA-ScR guidelines. Databases PubMed, EMBASE, and CINAHL were systematically searched for studies assessing any type of MDT within the context of diagnosis and treatment in adult people (≥ 18 years) with diabetes and comorbidities/complications. Data extraction included details on study characteristics, MDT interventions, digital health solutions, and key findings.
Results
Overall, 19 studies were included. Generally, the MDTs were characterized by high heterogeneity. Four overall components characterized the MDTs: Both medical specialists and healthcare professionals (HCPs) of different team sizes were represented; interventions spanned elements of medication, assessment, nutrition, education, self-monitoring, and treatment adjustment; digital health solutions were integrated in 58% of the studies; MDTs were carried out in both primary and secondary healthcare settings with varying frequencies. Generally, the effectiveness of the MDTs was positive across different outcomes.
Conclusions
MDTs are characterized by high diversity in their outline yet seem to be effective and cost-effective in the context of diagnosis and treatment of people with diabetes and comorbidities. Future research should investigate the cross-sectorial collaboration to reduce care fragmentation and enhance care coordination.
Introduction
Diabetes is a chronic disease that has a major impact on healthcare systems worldwide. In 2021, the number of adult people with diabetes was 537 million, which is estimated to reach 785 million by 2045. 1 People with diabetes have an increased risk of developing one or more chronic conditions in addition to their diabetes such as cardiovascular diseases, chronic kidney disease, or mental disorders.2,3 This is often referred to as comorbidity, which is defined as the co-occurrence of other chronic conditions in addition to an index condition (e.g., diabetes). When an individual has a co-occurrence of two or more chronic conditions (without an index condition), this is referred to as multimorbidity.4,5 Both terms will be used interchangeably throughout this review. However, the primary focus of this review is people with diabetes and comorbidities. The prevalence of people with diabetes and comorbidities varies between 40-95% based on different diabetes cohorts, thus mirroring the tendencies observed in people with single conditions and multimorbidity.2,6,7
When compared to single condition counterparts, people with diabetes and comorbidities are associated with poorer outcomes in terms of higher mortality and morbidity rates, polypharmacy (the intake of multiple drugs), depression, health-related quality of life (HRQOL), and higher healthcare utilization.2,4,8 Social inequality is also prevalent in people living with multimorbidity, where the prevalence of multimorbidity is consistently higher in the most socioeconomically deprived areas when compared to more affluent counterparts.9,10 Moreover, people with multimorbidity have more frequent hospital admissions with longer stays than people with single conditions, and the relationship between the number of chronic conditions and their associated costs due to increased healthcare utilization is almost exponential.4,11 Higher healthcare utilization combined with multiple pharmacological treatments, which is common among people with multimorbidity, lead to a higher treatment burden and places financial strain on both patients and healthcare. Also, diabetes is a complex disease that requires support across the healthcare landscape, and the management of people with diabetes and comorbidities is multifaceted and necessitates the involvement of different medical disciplines and healthcare providers.2,7,12
Most healthcare today is designed to treat single conditions rather than providing comprehensive, patient-centered care, which can lead to fragmented and sometimes contradictory care. 4 Consequently, a lack of communication between healthcare professionals (HCP) and between HCP and patients is experienced, which results in incoherent patient pathways leading to poor treatment outcomes, impaired HRQOL, and treatment dissatisfaction.7,13–15 Hence, there is a need for optimized prevention, management, and a reconfiguration of healthcare to achieve an appropriate balance of disease-oriented specialist care and patient-centered generalist care. 4 Reflecting the challenges of managing people with diabetes and comorbidities, potential interventions are also likely to be complex and multifaceted if they are to address the varied needs of the individual. Although an increasing number of studies have examined interventions for multimorbidity, evidence is still too limited to support any specific approach. 4 Multidisciplinary Teams (MDT), where HCP from different medical specialties meet and discuss the diagnosis, treatment, and overall patient-centered care, are suggested as one such approach.16–18 Previously, various MDT approaches have been applied in different diabetes settings with promising results in terms of improved glycemic control19–23 and other health-related outcomes.23–26 However, the evidence concerning MDTs within diabetes and comorbidity settings remains sparse. Digital health solutions have in recent years been recognized as a tool to support interventions for multimorbidity (e.g., MDTs) yet it remains uncertain to what extent digital health solutions have been applied to support MDTs throughout the literature. 27 Additionally, the characteristics of the MDT format remain to be uniformly defined across the literature. This lack of standardization leads to difficulties in comparing studies across settings and conducting high-quality evaluations of the MDT interventions to guide healthcare and policymakers.4,17 Thus, the above-mentioned considerations suggest the need for an additional review in the field to contribute to a more standardized definition of MDT and to identify knowledge gaps in this regard.
Scoping reviews are useful for systematically and rigorously identifying and mapping available evidence within a certain topic, field, or concept. 28 Contrary to systematic reviews, scoping reviews are more exploratory and flexible and aim to address more wide-ranging questions as opposed to more specific questions in systematic reviews. 29 Scoping reviews can be used to clarify key concepts/definitions or identify key characteristics related to a concept (i.e., MDTs in this case) in the literature within or across contexts.29,30 As such, a scoping review is deemed the most appropriate methodological fit for answering the review question and objectives in the present review.
Review Question
The review question of this scoping review is as follows: What characterizes MDTs in the context of diagnosis and treatment of people with diabetes and comorbidities?
The objectives of this scoping review are to summarize and map the available evidence on 1) key characteristics of MDTs, including how digital health solutions are applied to support the MDTs, 2) application of MDTs in clinical practice, and 3) effectiveness of MDTs on all patient-relevant outcomes.
Methods
This scoping review was conducted and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses extension for Scoping Reviews (PRISMA-ScR) guidelines 31 (see Appendix 1). A study protocol was prospectively registered on Open Science Framework, for details see https://osf.io/v8j34.
Eligibility Criteria
Participants
This scoping review considered studies that included adults (≥ 18 years of age), who were diagnosed with diabetes (type 1 or 2) and at least one additional comorbidity and/or complication. Comorbidity or complication was defined as a chronic disease or condition in addition to the diabetes diagnosis. Studies reporting mixed disease populations (e.g., diabetes, cardiovascular diseases, chronic kidney disease) were considered if an appropriate subgroup analysis was present. Studies that included people with gestational diabetes or prediabetes only were excluded.
Concept
This scoping review considered studies that evaluated or assessed any type of MDT. This included both MDT meetings, MDT conferences, and different clinical MDT approaches. The MDT composition had to consist of at least two different medical specialties to be included. Studies that only included one medical specialty or combined one medical specialty with different HCP such as dietitians, nurses, or pharmacists in the MDT were excluded.
The review considered all patient-relevant outcomes of the MDTs such as glycemic control, quality of life, cost-effectiveness, hospitalizations, and the number of comorbidities/complications, etc.
Context
This review considered studies that reported on MDTs in the context of either diagnosis and/or treatment for people with diabetes and comorbidities. MDTs in both primary and secondary healthcare settings were considered.
Types of evidence sources
The present review considered all primary, peer-reviewed research studies. This also included program descriptions related to MDT interventions. However, program descriptions that simply described the aim of a not yet developed MDT intervention were excluded. Secondary research studies, such as systematic reviews, were screened to assess the individual primary research studies included in these reviews. Studies available in full-text format and published in English, Danish, Swedish, or Norwegian were considered for inclusion.
Information sources
The systematic searches were performed in the databases PubMed, EMBASE, and CINAHL on 21 October 2021. A follow-up search was made on 23 June 2022 in the three databases to include the most recent publications. The searches were performed by one review author (JDA) with assistance from an experienced research librarian, who helped design and refine the searches. Additional citation searches and reference list searches of finally included key studies were carried out manually in SCOPUS and Google Scholar.
Search strategy
The search strategy in this scoping review followed the PRESS Guideline Evidence-Based Checklist developed by McGowan et al. to ensure quality in electronic search strategies. 32 Preliminary searches were performed in PubMed, EMBASE, and Google Scholar to identify search terms, keywords, and index terms to prepare the systematic searches. The search strategy was initially developed for PubMed and then adapted for the other databases. Block searches were performed with each block reflecting the population (P), the concept (C), and the context (C), respectively. The PCC strategy was also used to specify the searches and identify additional search terms. The systematic searches used index terms (e.g., MeSH in PubMed and Emtree in Embase) when appropriately combined with other search functions such as Boolean operators, truncation, phrase searching, and free text searching to further focus the searches. For full electronic search strategy, see Appendix 2.
Selection of sources of evidence
Following the systematic searches, all identified studies were collated and uploaded into RefWorks (RefWorks, RefWorks-COS, ProQuest RefWorks 2.0, 2010). Duplicates were checked and removed using the functions Exact match and Close match. Hereafter, titles, and abstracts were screened by one reviewer (JDA) supervised by another review author (SH) for assessment against the inclusion criteria. Studies that were potentially relevant were retrieved in full-text format and further assessed by one reviewer (JDA) supervised by another review author (SH) against the inclusion criteria. Any disagreement that occurred between the reviewers was resolved through discussion or by the inclusion of a third reviewer as arbiter. During the full review, reasons for the exclusion of studies were recorded and presented in a PRISMA flow diagram in the present review. 33
Data extraction
Data were extracted by one reviewer (JDA) using a template adapted from JBI. 28 The data extraction was supervised by another review author (SH). The extracted data were recorded in a standardized Microsoft Excel table developed in agreement with all the authors of this scoping review. Extracted data included details on study characteristics (first author, publication year, country, study population, study type, and sample size), details on the MDT intervention (settings, frequency, description, MDT composition, and context), and key findings concerning the review objective. In addition, details on whether digital health solutions were applied as part of the MDT intervention were recorded. Disagreements between the reviewers were resolved through discussion or by the inclusion of a third reviewer when needed.
Data analysis and presentation
Extracted data were handled by descriptive analysis by one author (JDA), supervised by two co-authors (SH and MHJ), where frequency counts of different concepts, populations, and locations of studies were carried out using Microsoft Excel. Following the descriptive analysis, each study was analyzed thematically according to three different themes reflecting the review question and objective: 1) key characteristics of MDTs, including the use of digital health solutions, 2) application of MDTs in clinical practice, and 3) effectiveness of MDTs on different patient-relevant outcomes. The characteristics and results of the individual studies are presented in tabular format and presented in a visual format concerning each theme answering the review question.
Results
Selection of sources of evidence
The systematic searches resulted in 9,423 records, of which 4,631 were duplicates (Figure 1). After screening the remaining 4,792 records on title and abstracts, 4,639 were excluded as irrelevant. Of the 152 records included for full-text reading, 137 were excluded, mainly because they did not include an MDT intervention (n = 81) or focused on a wrong target population (n = 18). Another five records were identified through citation and reference searches of which one was excluded due to a wrong target population. In total, 19 studies were included in this review, for further details see Figure 1. PRISMA flow diagram.
33

Characteristics of sources of evidence
Characteristics of sources of evidence.
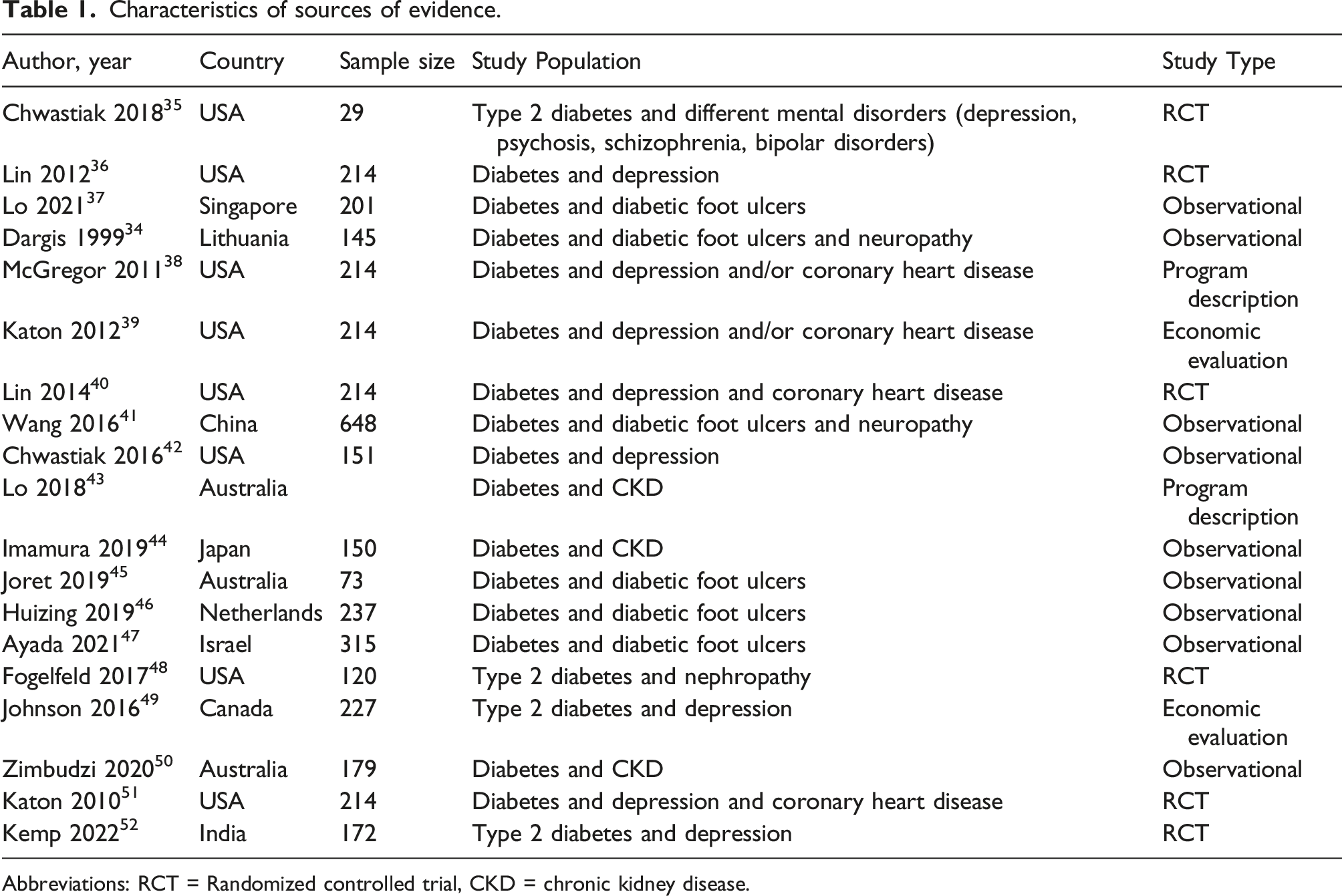
Abbreviations: RCT = Randomized controlled trial, CKD = chronic kidney disease.
Results of individual sources of evidence
Results of individual sources of evidence.
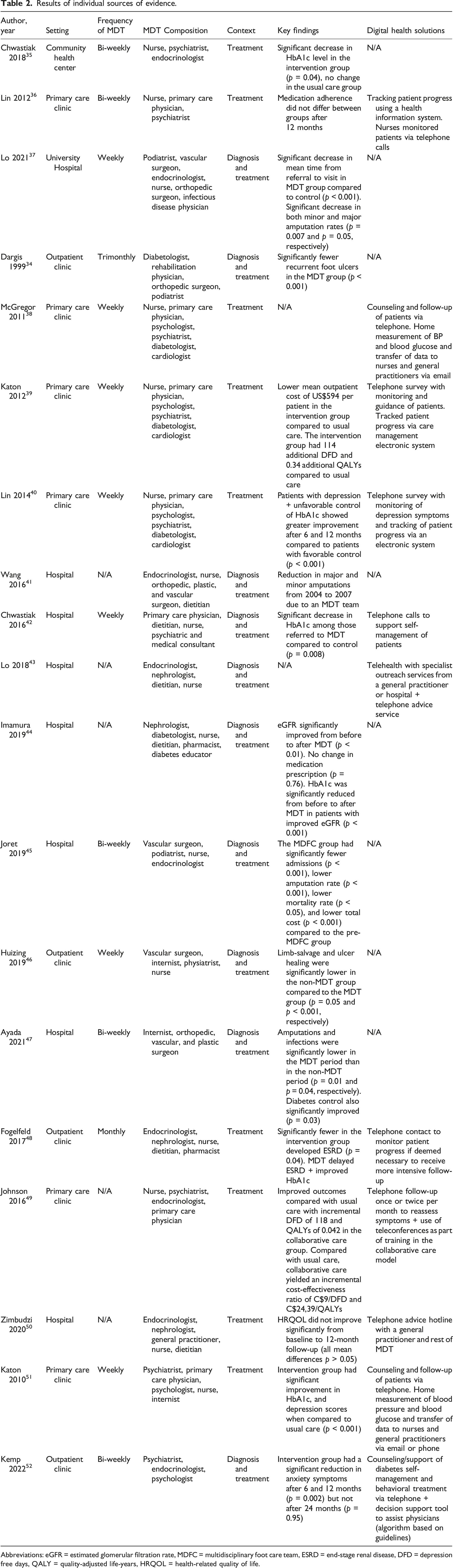
Abbreviations: eGFR = estimated glomerular filtration rate, MDFC = multidisciplinary foot care team, ESRD = end-stage renal disease, DFD = depression free days, QALY = quality-adjusted life-years, HRQOL = health-related quality of life.
Of the 19 included studies, 11 studies (58%) applied some form of digital health solutions as part of the MDT intervention. All the studies used telephone-based support, telecounseling, or telemonitoring of patients (11 studies, 100%). Additionally, tracking of patient progress via electronic systems (2 studies, 18%), home measurements with a transfer of data (2 studies, 18%), and decision support system (1 study, 9%) were applied as part of the MDT interventions.
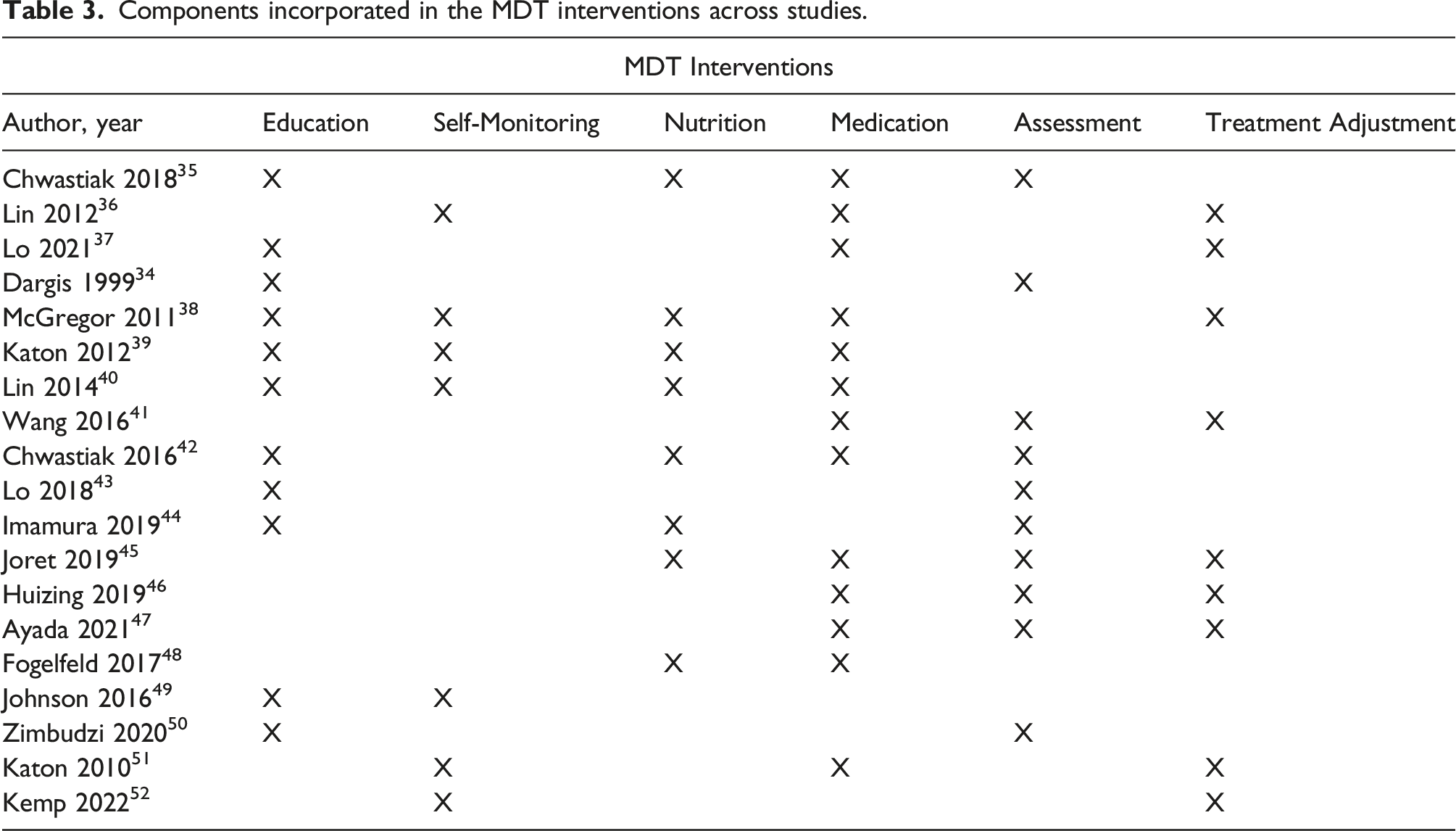
Components incorporated in the MDT interventions across studies.
Synthesis of results
Figure 2 illustrates the findings with the three different themes related to the review question and objectives of the review. Visualization of key characteristics of MDT, application of MDT, and the effectiveness of MDTs. Abbreviations: eGFR = estimated glomerular filtration rate, ESRD = end-stage renal disease, HRQOL = health-related quality of life.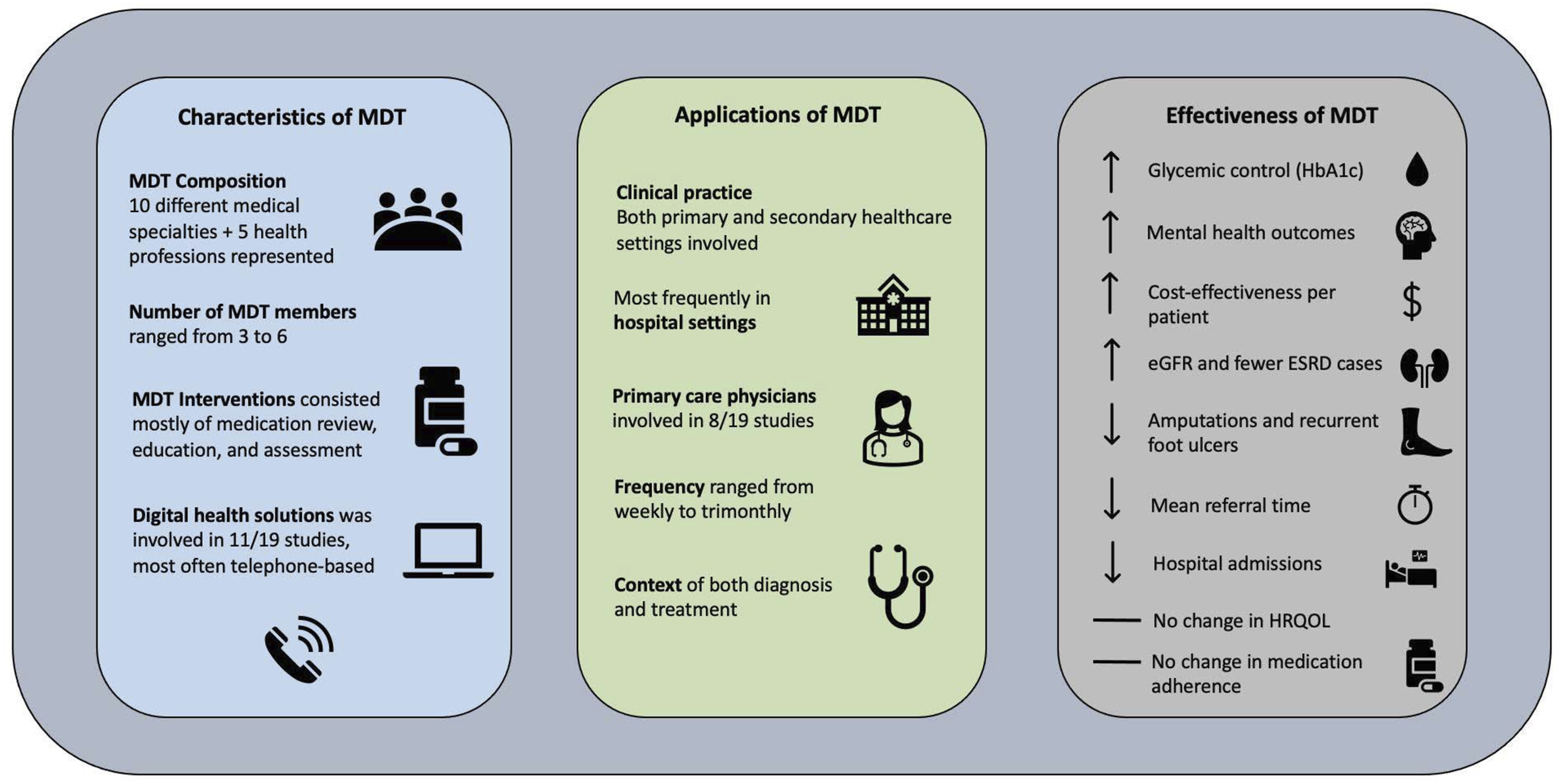
Discussion
This scoping review aimed to map the available evidence on the key characteristics of MDTs in the context of diagnosis and treatment in people with diabetes and comorbidities. This included how digital health solutions were applied to support the MDTs, the applications of MDTs in clinical practice, and the effectiveness of MDTs on different patient-relevant outcomes. A central finding in the present review was that the MDT compositions and functions in the context of diagnosis and treatment in people with diabetes and comorbidities were highly diverse and can be carried out in several ways. However, four overall elements were characteristic of the MDTs: teams were composed of both medical specialists and HCP of different team sizes; interventions spanned elements of medication, assessment, nutrition, education, self-monitoring, and treatment adjustment; digital health solutions were incorporated in over half of the studies to support MDT interventions; MDTs were carried out in both primary and secondary healthcare settings with varying frequencies. The number of different medical specialties and healthcare professions involved in the MDTs reflect the diversity of these teams. This diversity might be partly explained by the fact that MDTs are a relatively novel approach within diabetes management, and a lack of previous intervention studies means that the interventions have rarely been evaluated systematically and thereby not contributed to refining and standardizing the MDT intervention. Contrary, diversity in these teams can be viewed as a necessity to embrace the complexity and heterogeneity of people with diabetes and comorbidities and therefore needs to remain flexible. 17 This further highlights the challenges regarding defining a standardized MDT setup that works equally well in different settings and could also explain the lack of high-quality evaluations of MDTs within the diabetes field to date.
Overarchingly, the effectiveness of the MDTs in this review is considered positive, ranging from improved glycemic control35,40,42,44,48,51 and improved mental health outcomes40,49,51,52 to a reduction in amputations and recurrent foot ulcers.34,37,41,45–47 Additionally, a decrease in hospital admissions, 45 reduction in mean time from referral to visit, 37 and improved CKD outcomes44,48 were observed. These results align well with other studies evaluating MDT approaches in people with diabetes only.20,21,25,53–55 The finding that HRQOL did not change because of the MDT intervention is consistent with a recent systematic review that did not find any significant changes in HRQOL in patients with multimorbidity when evaluating an MDT approach in primary and secondary healthcare settings. 56 However, the interventions in this study did not match the criteria for the MDT interventions in the present review exactly and can therefore not be compared directly. Based on current evidence, it is not indicated that MDT interventions are associated with improved HRQOL as outcome in multimorbid patients. Poor HRQOL, however, is an outcome that is consistently associated with multimorbidity, so future research investigating interventions that can improve HRQOL would be beneficial. 4 Based on this scoping review, the introduction of an MDT in the management of diabetes and comorbidity seems to be cost-effective.39,49 This is consistent with previous studies focusing on patients with diabetes and comorbidities,57,58 which also found an MDT approach to be cost-effective compared with controls. These results might suggest that adding comorbidities to the diabetes diagnosis does not complicate or impair the functioning of the MDTs, which could pave the way for more cost-effective, multidisciplinary management of people with diabetes and comorbidity.
The different components of the MDT interventions in the present review align well with a recent Cochrane review, where it was reported that interventions for people with multimorbidity predominantly included components of care coordination, education, self-management support, and medicines management. 59 Medication review or adjustment was the most frequent component of the MDT interventions in this review. This finding is expected though as multimorbidity is strongly associated with polypharmacy, and therefore must be adjusted accordingly to avoid adverse events.60,61 Hence, intensification of medication adjustment seems an important part of the management of people with diabetes and comorbidities. Again, the many different components that are incorporated into the MDT interventions across studies reflect the diversity of these teams.
The inclusion of digital health in 58% of the included studies suggests that digital health solutions are already, and could prospectively, be integrated into the MDTs and further contribute to positive treatment outcomes. Two recent systematic reviews and meta-analyses e.g., reported that digital health solutions provided moderate improvements in measures of disease control 27 and the experience of care 62 in people with diabetes and comorbidities but not in overall health status. This might suggest that digital health solutions are most efficient when used in combination with other interventions or specific components of an intervention, and not as the intervention itself in patients with diabetes and comorbidities. This finding could be due to the diversity of challenges experienced in this group of patients, which is often very heterogeneous and complex. 27 Moreover, the amount and quality of evidence were also reported to be very limited in both studies and further research in this area is needed to determine the most optimal incorporation of digital health solutions in the MDTs.
The most common comorbidity in addition to diabetes in this review was mental disorders. This might be surprising as comorbidities have traditionally been viewed primarily as physical diseases or conditions.63,64 Diabetes comorbidities of physical character often share the same underlying pathophysiologic profiles or care management goals, which are also known as diabetes-concordant comorbidities. 64 However, diabetes-discordant comorbidities have no direct relationship with diabetes in terms of pathophysiologic profile and are often harder to manage when compared to concordant comorbidities and single conditions. 64 Nonetheless, people with diabetes and mental disorders often share reciprocal susceptibility and a high degree of comorbidity, and the mental disorders are often inadequately managed because of a lack of training, guidelines, or initiatives in this regard.26,42,63 Thus, the focus on the management of mental disorders as a comorbidity in the present review seems justified.
Finally, future directions of the management of people with diabetes and comorbidities point toward more organizational change, incorporating MDTs across healthcare settings and increasing focus on patient-centered care.59,65 The findings from this scoping review complement the overall elements of a framework developed to describe models of care for multimorbidity. 65 Based on the results of the present review, many of the elements described in the model are represented in the MDTs already, suggesting the challenges of determining the most optimal MDT setup lie elsewhere. In this review, most of the studies were applied in secondary healthcare settings in hospitals, whereas primary care physicians were involved in 42% of the studies. However, the studies which included primary care physicians already took place in primary care. None of the included studies had cross-sectorial settings, where both secondary and primary healthcare were combined and collaborated. One possible solution prospectively could be the facilitation of work relationships across healthcare sectors to deliver more unfragmented, multidisciplinary care for patients. People with diabetes and comorbidities rarely fit in one specialized location due to the complex and heterogeneous nature of their conditions. Thus, future development or updates of existing intervention models, such as MDT interventions, should take the cross-sectorial collaboration and fragmentation of care perspective into consideration.
Limitations
In our study protocol, we chose to define the MDT as consisting of at least two medical specialties. As such, this could have led to the exclusion of potentially relevant studies as a great number of studies only reported one medical specialty (81/137) combined with different HCP as part of the MDT. Also, our broad definition of MDT could have contributed to the highly diverse outline of the MDTs in this present review.
We also chose to include participants with both type 1 and 2 diabetes. However, in most of the included studies there was no distinction between the two types which means no subgroup analysis was possible. This makes the conclusion on whether the effectiveness of the MDT interventions is the same regardless of diabetes type more difficult.
Mainly one review author (JDA) was responsible for screening and data extraction processes in the present review. Although supervised by another review author (SH) this approach could have increased the risk of confirmation bias.
The largest sample of studies was conducted in North America (47%). Although the healthcare systems in North America and Europe share some similarities, there are also great differences. The MDT format differs to some extent as MDTs in Europe are mainly meeting and/or conference based, whereas it is more of an MDT approach in North America. Although there were studies in this scoping review from Australia and Asia as well, there were only two studies conducted in Europe. As previously mentioned, mental disorders were the most common comorbidity in our review. However, eight of the nine included studies that investigated mental disorders were conducted in North America. This finding, combined with the concentration of studies in North America, might hamper the external validity and make it harder to generalize the findings to a European context.
Conclusions
MDTs are characterized by high diversity and can be carried out in several ways in terms of settings, number of team members, medical specialist compositions, incorporation of digital health solutions, and frequencies. The heterogeneity of the MDTs generally reflects the challenges in standardizing the MDT intervention, which could explain the lack of high-quality evaluations of the intervention to date. Implementing MDTs could prospectively be a valid approach in the context of diagnosis and treatment of people with diabetes and comorbidities. Future research should investigate the cross-sectorial collaboration opportunities to reconfigure healthcare to promote a more optimal balance between patient-centered generalist care and condition-oriented specialist care to enhance care coordination and reduce care fragmentation.
Supplemental Material
Supplemental Material - The multidisciplinary team in diagnosing and treatment of patients with diabetes and comorbidities: A scoping review
Supplemental Material for The multidisciplinary team in diagnosing and treatment of patients with diabetes and comorbidities: A scoping review by Jonas D Andersen, Morten Hasselstrøm Jensen, Peter Vestergaard, Vigga Jensen, Ole Hejlesen and Stine Hangaard in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - The multidisciplinary team in diagnosing and treatment of patients with diabetes and comorbidities: A scoping review
Supplemental Material for The multidisciplinary team in diagnosing and treatment of patients with diabetes and comorbidities: A scoping review by Jonas D Andersen, Morten Hasselstrøm Jensen, Peter Vestergaard, Vigga Jensen, Ole Hejlesen and Stine Hangaard in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
We would like to thank research librarian Connie Skrubbeltrang for her assistance in terms of refining and focusing the systematic literature searches.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent statement
This is a scoping review/review article, no ethics committee or institutional board approval nor written consent have been obtained.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.