
Abstract
Introduction
Quality of life (QoL) is a vital healthcare indicator among people living with human immunodeficiency virus (PLWHA). Assessing the effects of comorbidities on QoL among PLWHA is of clinical and public health importance. This study compared the QoL of comorbid and non-comorbid PLWHA at St. Gerard’s Catholic Hospital (SGCH), Kaduna.
Methods
This was a prospective cross-sectional study of 178 conveniently selected and stratified comorbid PLWHA and 172 non-comorbid PLWHA receiving care at the facility. Data was collected using a structured, interviewer-administered instrument. The QoL scores were statistically compared using the Mann‒Whitney U test. P<0.05 was considered statistically significant for all the analyses.
Results
Most respondents were aged 35 – 54 years (65.2% and 66.4% for comorbid and non-comorbid patients respectively), were female (70.8% and 69.2% for comorbid and non-comorbid patients respectively) and married (67.4% and 59.3% for comorbid and non-comorbid patients respectively). For all QoL domains (perception of QoL and general health, physical health, psychological health, level of independence, social relationship, environment, and spirituality/religion/personal beliefs), there was evidence the distribution of values was significantly lower in the comorbid PLWHA compared to the non-comorbid PLWHA (p<0.001), with the largest difference seen for physical health. The mean physical health (interquartile range) was 9 (7-10) and 17 (15-19) for comorbid and non-comorbid PLWHA respectively. The most prevalent comorbidities among the PLWHA were hypertension 97 (54.49%) and diabetes 36 (20.22%).
Conclusion
Non-comorbid PLWHA had better QoL than comorbid PLWHA in all the QoL domains and the greatest difference was observed in physical health. Special efforts should be made to improve the QoL of comorbid PLWHA.
Background
Human immunodeficiency virus (HIV) is a chronic disease that affects all human races; however, recent developments in its treatment have led to remarkable outcomes. 1 Globally, HIV is the second-largest epidemic, with 37.7 million people living with it as of the year 2020. Approximately 39% of new cases are found in sub-Saharan Africa each year. In comparison, the prevalence of HIV in Nigeria is currently estimated at 1.4% and ranks fourth in the world in terms of HIV burden. 2 The prevalence of HIV in Kaduna State ranges between 1.1% and 1.4%. 3 The high prevalence of HIV in this region may pose substantial health challenges in the community, which may aggravate the presence of comorbidities.
Comorbidity in HIV has been defined as “a disease outside the scope of an acquired immunodeficiency syndrome-associated (AIDS-defining) illness”. 4 The comorbidities among people living with HIV/AIDS (PLWHA) include hypertension, diabetes mellitus, and hepatitis B, among others. Some of these comorbidities occur as a result of HIV infection, i.e., vascular and renal diseases, associated risk factors, potential coinfections (hepatitis C), or even antiretroviral toxicity (diabetes and liver disease).5-7 The risk of these comorbidities increases with increasing HIV severity. 4 The presence of comorbidities among PLWHA has been reported to impact their quality of care, quality of life (QoL), prognosis and cost of care, among other factors. In addition, it is considered one of the major causes of death and disability among this population of patients. 8
It is predicted that comorbidity with noncommunicable diseases (NCDs) will increase in developing countries, including Nigeria. 9 The patient needs associated with the increase in comorbidities can potentially overwhelm the fragile healthcare systems in these countries. Additionally, the funding of HIV/AIDS programs in these countries, which is primarily through international donor interventions without considering NCDs, has been noted: “would only end up in preventing death from HIV, but not death of the patients”. 10
In Nigeria, PLWHA continually receive suitable HIV care, treatment, and services. Notably, they have life expectancies almost similar to those of people living without HIV. 11 However, PLWHA with comorbidities have considerably lower QoL than non-comorbid PLWHA and the general population.12,13 QoL is a vital healthcare indicator among people living with chronic diseases, including HIV, and its measurement is important given the increasing incidence of NCDs in developing countries. 11
Therefore, comorbidities among PLWHA are not only of clinical importance but also critical public health concerns. 14 Thus, understanding their prevalence in developing countries is a priority for policy and practice.
Studies on QoL, particularly in Nigeria have often focused on HIV or comorbidities alone, thereby leaving a gap in understanding how comorbidities affect QoL of PLWHA compared to non-comorbid PLWHA.11,15-18 Thus, to address this gap, this study aimed to compare the QoL between comorbid and non-comorbid PLWHA and assess the prevalence of comorbid conditions among PLWHA at St. Gerard's Catholic Hospital (SGCH), Kaduna. This study is relevant for the formulation of policies that adequately address the emerging needs of PLWHA and accompanying comorbidities so that present care services can be improved by healthcare administrators and stakeholders.
Methods
Study setting
Kaduna is one of the most cosmopolitan states in Nigeria; it harbours people from all parts of the country and is easily accessible from all the geopolitical zones of the country. The study was conducted at the ART Clinic of SGCH, Kaduna, located in Kaduna South Local Government Area of Kaduna State, northwestern Nigeria. Despite being a faith-based secondary healthcare facility, it caters to the healthcare needs of people within the Kaduna metropolis and neighbouring communities, irrespective of religious belief, ethnicity, and socioeconomic or educational status. It also serves as a referral centre for different primary healthcare facilities in Kaduna South. The ART Clinic was established in 2006 and provides comprehensive HIV services, including diagnosis, counselling, treatment and prevention of HIV. 15 It operates outpatient clinics Mondays through Fridays and serves a population of 3,874 PLWHA.
Study population and eligibility criteria
All PLWHA who were at least 18 years of age, were accessing HIV care at the facility, consented to participate in the study and completed the questionnaire were included, with or without comorbidities. However, those who did not meet these criteria were excluded from participation in the study.
Study design
This prospective, cross-sectional study involved a sample of PLWHA attending the ART clinic of SGCH during the study period.
Description of the study instrument
The data collection instrument for this study was the World Health Organization Quality of Life assessment instrument (WHOQOL-BREF), which was developed and validated by the WHOQOL Group and is available in different languages. 19 The WHOQOL-HIV BREF instrument comprises 26 items that measure the following six broad domains: physical health, psychological health, social relationships, level of independence, spirituality and the environment. It assesses individuals’ perceptions in the context of their culture and value systems and their personal goals, standards and concerns. 20 For this study, sociodemographic information and the presence of comorbidities were also added. The instrument has been validated in Nigeria and has reported Cronbach's alpha values ranging from 0.70 to 0.90 for various domains, which indicates excellent internal consistency. 21
Sample size determination
A sample size of 350 was determined using the Raosoft online sample size calculator available online at https://www.raosoft.com/samplesize.html. 22 The calculation was performed with a 5% margin of error, 95% confidence level, a response distribution of 50% and a population size of 3,874 PLWHA attending the facility based on the hospital records.
Sampling technique
PLWHA who consented to participate in the study were stratified into comorbid and non-comorbid sampling frames to avoid selection bias. A convenient sampling technique was subsequently used to select the required number of patients from the two strata.
Data collection
Data from PLWHA who met the eligibility criteria and provided consent were collected using the WHOQOL-HIV BREF questionnaire. Through the supervision of the principal researcher, trained research assistants administered the questionnaire from May 2023 through October 2023. Data on comorbidities were collected from the respondent’s medical records.
Data analysis
The data collected were analysed and categorized into domains as described by the originator of the tool, WHOQOL. The WHOQOL-HIV-BREF scores for both groups were not normally distributed (Shapiro‒Wilk test, p < 0.05); therefore, a statistical comparison of the median scores of the QoL domains among the comorbid and non-comorbid PLWHA was conducted using the Mann‒Whitney U test. The Mann‒Whitney U test, interquartile range and effect size, rank-biserial correlation (r), were computed to explore the potential association between comorbidities and QoL. The effect size ranges from -1 to 1 in magnitude, and the higher the value is, the larger the size of the effect. A positive (+) or negative (-) sign indicates the direction of the difference, in which the positive values indicate that the comorbid group tends to have higher ranks, while negative values indicate the non-comorbid group has higher ranks. Generally, r>0.5 or r<-0.5 indicates a large effect, in other words, a large difference in the distributions of the two groups. A 2-tailed asymptotic p ≤ 0.05 was considered statistically significant for all the analyses. The results were expressed descriptively in tabular form. All analyses were performed using Statistical Package for Social Sciences (SPSS) version 26.
Ethics
Ethical approval was granted by the Health Research and Ethics Committee of SGCH, Kaduna (approval no. SGCH/NHREC/11/04/2023). All participants provided informed written consent prior to their participation in the study.
Results
Sociodemographic information of the patients enrolled in the study, n = 350.

Most of the respondents in both groups were within the age of 35 – 54 years which accounts for 65.2% and 66.4% for comorbid and non-comorbid patients respectively. Most respondents in both categories of PLWHA were females [comorbid 126 (70.8%) and non-comorbid 119 (69.2%)] and Christians [comorbid 150 (84.3%) and non-comorbid 150 (87.2%)]. The majority of them were married; 120 (67.4%) comorbid respondents and 102 (59.3%) non-comorbid respondents and only 1 (0.6%) and 3 (1.7%) of the comorbid and non-comorbid respondents, respectively, attended tertiary education.
Statistical associations between the sociodemographic variables of comorbid and non-comorbid PLWHA receiving care at SGCH, Kaduna (n=350).

P values were assessed using the Chi-square test, and p values <0.05 were considered statistically significant.
Comparison of quality-of-life domains between comorbid and non-comorbid PLWHA receiving care at SGCH, Kaduna (n=350) using the Mann‒Whitney U test.

P values were expressed as 2-tailed asymptotic values and p < 0.05 were considered statistically significant, where U represents the Mann‒Whitney U test, IQR represents the interquartile range, and the negative (-) sign on “r” indicates that median scores for non-comorbid patients are higher than the corresponding values for comorbid patients.
Comorbidities observed among comorbid PLWHA receiving care at SGCH, Kaduna (n=178).
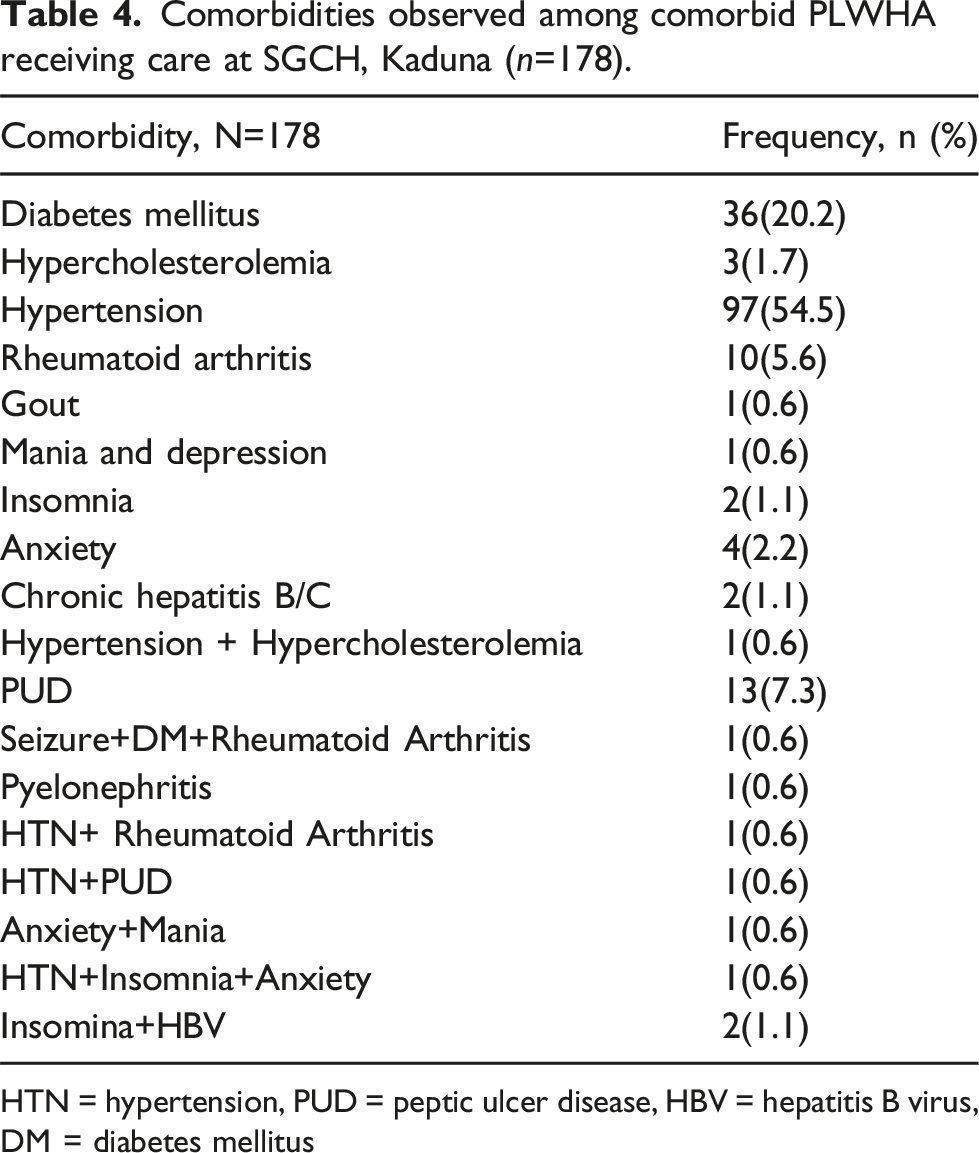
HTN = hypertension, PUD = peptic ulcer disease, HBV = hepatitis B virus, DM = diabetes mellitus
Discussion
Most respondents in both categories were females. In addition to females having a high prevalence of HIV in Nigeria, possibly because of early sexual debut, they do readily present themselves for studies, likely because of their unemployed status, as they are not required to fend for the family in the study setting, they have the luxury of time to participate in a study.16,23 The high number of Christians in both categories of respondents might not be unrelated to the fact that the facility is a Christian faith-based hospital.
Only a few of the respondents had a tertiary education, with the majority having a primary education. This is lower than the findings reported in Zaria, Kaduna State, and could be attributed to poor socioeconomic level, low literacy level in the study environment and possibly because the facility is a secondary healthcare hospital; those possessing tertiary education might prefer to receive their care from tertiary facilities where experts are in abundance or utilize the differentiated service delivery model.17,24
Age and education are statistically associated with the presence of comorbidity because, with advancing age, one becomes more susceptible to being diagnosed with a chronic disease. 17 Those with higher education levels could have less chronic disease than those without education or with only primary education. Education can be associated with compliance with advice on a healthy lifestyle, thereby reducing the propensity of one being affected by a chronic disease. 18 Similarly, those with a lower income do not have the financial ability to live a healthy lifestyle, properly manage stress and meet basic needs of life. Therefore, they are at risk of developing a chronic disease. Those with a higher income can afford to modify the risk factors for chronic disease and, as such, are less vulnerable to developing a chronic disease. 25
Our findings revealed that non-comorbid respondents had a higher distribution of scores in all the QoL domains compared to comorbid respondents and a statistically significant association between the presence of comorbidity and low QoL was observed. The difference could be due to the burden of severe symptoms associated with chronic diseases, which impairs QoL. 26 The presence of two or more chronic diseases negatively affects the QoL of PLWHA.13,27 Similarly, the effect of comorbidity on the QoL of PLWHA depends on the severity of their symptoms. 28 Chronic diseases were found to reduce QoL among PLWHA, particularly by diminishing their physical QoL. 29 This plausibly explains why the difference in the physical domain of the QoL among the two categories in this study was greater than that in the other domains and why it also had the lowest scores in the comorbid PLWHA.
In this study, the domain with the highest median score among comorbid PLWHA was social relationships, followed by psychological health, level of independence, environment and spirituality/religion/personal beliefs. In contrast, the non-comorbid PLHWHA had the highest median score on the physical health and spirituality/religion/personal beliefs domains. Findings from a similar study in Jordan reported that the respondents had better QoL scores in the spirituality/religion/personal beliefs domain, psychological health domain and physical health domain. 30 The scores of non-comorbid PLWHA partly mirrored the findings from North Central Nigeria, where the respondents had high scores in the psychological, physical and spiritual domains. 31 The high scores observed in social relationships reflect the emotional, financial and safety support that families, especially spouses, offer to their HIV-positive partners living with comorbidities, as married persons enjoy high social support. 11 Similarly, non-discrimination, no stigmatization, wide acceptance in the community and the availability of social support may also be responsible for the improved score of the social relationship domain.32,33 The role of social support in improving QoL, as reported by Mengistu and colleagues, was also observed in this study. 34
Although religion was found to improve the QoL of PLWHA in Southeast Nigeria, the high score in the spiritual domain of comorbid PLWHA could be explained by the perception that people are more religious and spiritual when challenged with problems beyond their capacity.35,36 This may also indicate a good perception of religion because, in a similar study in Jordan, the respondents recognized the role of spirituality in improving QoL and supported the integration of spiritual support in HIV/AIDS care, even though this integration was not obtainable in this study’s setting. 30
The results indicate that non-comorbid PLWHA had a significantly higher distribution of scores across all QoL domains than comorbid PLWHA, with large effect sizes observed for all domains. These findings suggest that the presence of comorbidities has a substantial negative impact on the QoL of these patients, which may affect their treatment outcomes. Furthermore, the significant differences across all QoL domains emphasize the need for integrated care approaches that address both HIV and comorbid conditions.
The study revealed hypertension, diabetes and rheumatoid arthritis as the most prevalent comorbidities among PLWHA. This is in sharp contrast to a study in New York City, which reported chronic pulmonary diseases and renal disease as the most prevalent conditions among PLWHA. 37 In the United Kingdom, hepatitis, mental health disorders and cardiovascular disease are the most prevalent comorbidities. 4 In developing countries, cardiovascular diseases occur in more than one-third of PLWHA attending clinics. 38 Obimakinde and colleagues reported hypertension, arthritis and tuberculosis as common comorbidities in southwestern Nigeria. 17 This could be due to variations in the study setting and the sample population included in the studies. 38
A higher prevalence of comorbidities among PLWHA was reported in Ethiopia. 39 The low prevalence of hypertension, diabetes mellitus and other comorbidities among the respondents might be due to the small number of doctors attending to the patients, as there were only two doctors in the facility. The acute shortage of doctors could result in missed diagnoses coupled with the language barrier between the doctors and the patients. While only patients with complaints during clinic visits are attended to by the doctors, patients fail to recognize symptoms of chronic diseases due to low literacy levels, which may lead to poor health-seeking behaviour and patients' refusal to report symptoms and denial of the diagnosis of a comorbid condition due to pill burden and the financial burden associated with the management of chronic diseases. These are not far-fetched considering the poverty in the area and the number of pills taken for HIV and opportunistic infections despite the availability of fixed-dose combinations and the dispensing of free antiretroviral medicines to patients, many lack health insurance.40-42
Recognizing the prevalent comorbidities and their associations with poorer QoL among PLWHA highlights the importance of prioritizing chronic disease management in the provision of care and services for such people. The insights gained should therefore facilitate the design of efficient, effective and tailored interventions to prevent and manage comorbidities among PLWHA while also improving their QoL, especially that of comorbid PLWHA. Future research should focus on developing targeted interventions that increase the overall well-being of comorbid HIV patients, thereby improving their QoL and overall well-being.
The presence of comorbidities among PLWHA often leads to a decreased QoL, which may lead to increased healthcare costs and resource utilization. This will assist policymakers in adopting integrated care models that address both HIV and other chronic conditions simultaneously. In addition, this ensures that healthcare resources are distributed based on the complexity of patient needs.43,44
Limitations and strengths of the study
A convenience sampling method was used in this study, which may introduce selection bias and limit the generalizability of the findings to a wider population sample of PLWHA. While the sample size of 350 is arguably adequate for statistical analysis, it might nevertheless not be large enough to fully capture the full diversity of PLWHA, especially those with rare comorbid conditions. The cross-sectional nature of this study may restrict our ability to infer causality between comorbidities and QoL in these patients. Additionally, the use of self-reported data for QoL assessments may lead to response bias, as participants either overreported or underreported their QoL due to social desirability. Confounding variables such as adherence to antiretroviral therapy and nutritional status were not accounted for in this study, which could influence QoL outcomes. Even though the WHOQOL-HIV BREF instrument has excellent validity in Nigeria, cultural differences can still exist and influence how participants interpret and respond to QoL questions, which may affect the validity of the results.
Despite these limitations, our study has the following strengths. Though the cross-sectional nature of the study provides only snapshots of differences in QoL between comorbid and non-comorbid PLWHA at specific times, as a prospective study, it reduces recall bias and provides more accurate data as events occur. In addition, the WHOQOL-HIV BREF questionnaire, a well-validated instrument for measuring QoL among PLWHA was used. This instrument assesses several domains of QoL and therefore offers a global perspective on the participants' overall health. The study also contributes to the broader understanding of how comorbidities impact the QoL of PLWHA in a Nigerian context.
Conclusion
The study revealed that non-comorbid PLWHA had better QoL than did comorbid PLWHA in all aspects of the QoL domains, and the greatest difference was observed in physical health. A higher median score of QoL domains among comorbid PLWHA was observed in social relationships, spirituality/religion/personal beliefs and overall perceptions of QoL and general health domains, whereas physical health had the lowest score. Among the non-comorbid PLWHA, the highest median score reported was in the physical health, psychological health and independence domains, and the lowest score was in the social relationship domain. Hypertension, diabetes mellitus and rheumatoid arthritis are the most common comorbidities observed in the facility. We therefore recommend the integration of chronic disease management into HIV/AIDS care, and special efforts should be made to improve the QoL of comorbid PLWHA.
Footnotes
Acknowledgements
We would like to thank the research assistants who conducted the data collection of the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.