
Abstract
Background
Multimorbidity, having two or more chronic conditions, is a growing public health concern associated with substantial health and societal burdens. However, evidence on its impact on health-related quality of life (HRQoL) among U.S. adults remains limited. This study fills a major research gap by examining the association between multimorbidity and HRQoL among U.S. adults, a population often overlooked in prior research and provides evidence to inform policies aligned with national and global health goals for reducing the chronic disease burden.
Methods
A cross-sectional study was conducted among adults aged 18 to 64 years. Data from the Medical Expenditure Panel Survey was used in this study for years 2019 to 2021. The primary study outcome was the HRQoL; it was evaluated using the 12-item Veterans RAND 12. Descriptive analysis was used to describe the characteristics of the study sample. The adjusted relationship between Multimorbidity and HRQoL was assessed using the multivariable linear regression after other factors were adjusted in the regression analysis.
Results
The study sample consists of 30,827 adults. Multimorbidity was prevalent among 23.4% of adults. It was higher among women, unemployed, poor, and physically inactive adults. Adults with multimorbidity had a lower mean HRQoL score than those without multimorbidity (Physical health = 46.06 vs. 53.29, Mental health = 47.62 vs. 52.37). Results from the adjusted linear regression model found that adults with multimorbidity have a significantly lower HRQoL in both the physical domain (β = -2.658, p-value<0.0001), and the mental domain (β = -3.119, p-value<0.0001).
Conclusions
Multimorbidity has a substantial negative impact on both physical and mental aspects of HRQoL in U.S. adults. These findings highlight the need for targeted public health strategies and clinical interventions, such as promoting integrated chronic disease management to address the burden of multimorbidity. Future research should explore specific condition clusters most strongly associated with reduced HRQoL to better inform policy and care models.
1. Introduction
Multimorbidity, defined as a person having two or more chronic illnesses simultaneously, is highly prevalent among adults globally. 1 It differs from the notion of comorbidity, which describes an individual’s cumulative effects from additional conditions related to the index condition.2,3 A systematic review and meta-analysis of 126 studies involving nearly fifteen million individuals from 54 countries, including the United States, Canada, China, India, Brazil, the United Kingdom, Australia, and countries across Europe, Africa, and the Middle East reported a global multimorbidity prevalence of 37.2%. 4
Multimorbidity is a major global health issue that harms patient health, healthcare, and society,1,5–7 increases morbidity and mortality, and imposes markedly higher healthcare utilization and costs on healthcare systems and society.5–7 It is linked to more frequent hospitalizations and readmissions, 5 and a higher likelihood of death for those with multiple conditions. 6 Published studies from various regions, including the United States, Europe, and Asia, have reported that multimorbidity imposes a substantial financial burden on healthcare systems and societies.7–9 Moreover, multimorbidity is closely related to disability and poor Quality of Life.10–16 Health-Related Quality of Life (HRQoL) provides a comprehensive measure of illness burden that includes evaluations of a person’s physical, mental, and social aspects of life. 17 Multimorbidity significantly influences HRQoL, with numerous studies demonstrating that a higher number of chronic conditions is associated with markedly lower HRQoL scores..10–16,18 HRQoL is a crucial indicator for evaluating health and disease and the overall effects of long-term illnesses like multimorbidity. 19 Prior research across diverse populations including Canada, Belgium, China, Korea, and Australia10–16 has consistently demonstrated that individuals with multimorbidity report significantly lower HRQoL compared with those without multimorbidity. These findings highlight the broad and cumulative impact of multiple chronic diseases on daily functioning, mental health, and social participation.
Despite this growing body of evidence, there remains a paucity of research focusing on U.S. adults, particularly within the working-age population (18–64 years). Most prior U.S.-based studies have concentrated on older adults or specific disease groups, leaving a critical gap in understanding how multimorbidity affects quality of life among younger, economically active adults, a group at risk of productivity loss and long-term health deterioration. Addressing the growing burden of multimorbidity is also central to achieving global and national health objectives. In particular, Sustainable Development Goal 3 (SDG 3) emphasizes ensuring healthy lives and promoting well-being for all at all ages, including the reduction of premature mortality from non-communicable diseases through prevention and management strategies. Understanding how multimorbidity affects HRQoL among adults provides critical evidence to support these goals and inform policies aimed at improving population health and reducing health inequalities. The present study addresses this gap by examining the association between multimorbidity and HRQoL in a nationally representative sample of U.S. adults, while also comparing HRQoL outcomes between individuals with and without multimorbidity. By doing so, it provides valuable insights into how the cumulative burden of chronic diseases affects well-being beyond traditional clinical measures. Furthermore, this study extends previous research by exploring socioeconomic and demographic disparities in these associations, offering evidence that can inform targeted interventions and policies promoting person-centered and integrated care for adults managing multiple chronic conditions.
2. Methods
2.1. Study design, study population and data source
A cross-sectional study was conducted among adults aged 18 to 64 years who are alive and have no missing data on HRQoL included in this study. We focused on adults aged 18 to 64 years to specifically examine the burden of multimorbidity and its impact on HRQoL among the working-age population, a group that has received less attention in previous research compared to older adults. This study used retrospective data of the Medical Expenditure Panel Survey (MEPS), a nationally representative survey of the United States (US) adults from 2019 to 2021 MEPS data files including data about households, medical conditions, prescribed medications, outpatient visits, etc.
2.2. Measures
2.2.1. Outcome: Health-related quality of life
HRQoL was measured in MEPS using the Veterans RAND 12 Item Health Survey (VR-12©), a self-administered tool that evaluate eight health dimensions (consisting of 12 items). These dimensions categorized into two key domains: the Physical Component Summary (PCS) and the Mental Component Summary (MCS). 20 The PCS assesses the following domains: physical functioning, role physical, bodily pain, and general health, while MCS comprises vitality, social functioning, role emotional, and mental health. The VR-12 is a reliable scale, the Cronbach’s alpha values for the two summary components of the VR-12, demonstrates good internal consistency, with approximately 0.85 for the PCS-12 and 0.83 for the MCS-12.21–24 Responses are measured on a five-point Likert scale ranging from “no, none of the time” to “yes, all of the time.”
2.2.2. Key independent variable
Data on chronic conditions are obtained from the MEPS medical condition files using the International Classification of Conditions, tenth Revision, Clinical Modification (ICD-10-CM) codes. Thirteen chronic diseases were used to define morbidity in this study, including heart disease, hypertension, diabetes, hyperlipidemia, asthma, chronic obstructive pulmonary disease (COPD), gastroesophageal reflux disease (GERD), arthritis, cancer, thyroid, anxiety, depression, and cancer. These chronic conditions were selected due to their high prevalence in US adults, which is defined as a prevalence of 2% or higher, and because of their related morbidity, mortality, and cost. Also, these prevalent diseases have been commonly used to define multimorbidity 25 and have been used by many published papers in defining multimorbidity.10,13,15,16
2.2.3. Other independent variables
Other independent variables that were measured included sex, race, age, marital status, region of residency, employment, level of education, poverty, perceived health, insurance, prescription drug coverage, and physical activity. Sex, age, race, marital status, region, employment, education, insurance, and prescription drug coverage were self-reported variables. Poverty status was determined using the federal poverty level ratio provided by MEPS. Perceived health was measured using a 5-point Likert scale ranging from excellent to poor; and Physical activity was assessed based on self-reported engagement in moderate or vigorous physical activities during a typical week.
2.3. Statistical analyses
Descriptive and inferential statistics (Chi-square statistics and independent group t-test) were used to describe the baseline characteristics and evaluate the unadjusted associations between them and multimorbidity. A linear regression model was used after adjusting for other covariates to evaluate the association between the multimorbidity and the HRQOL measures (PCS and MCS). Multicollinearity among independent variables was assessed using the Variance Inflation Factor (VIF). All VIF values were below 2.5, indicating no significant multicollinearity issues. Model performance was assessed using adjusted R2 values. Because analyses were conducted using survey-weighted linear regression accounting for the complex MEPS design, information criteria such as AIC were not directly applicable; therefore, model performance was evaluated using adjusted R2 and multicollinearity diagnostics (VIF). Results were considered statistically significant at a p-value < 0.05. We accounted for the complex survey design of MEPS by incorporating primary sampling units, strata, and person-level weights using survey procedures to ensure nationally representative estimates. SAS 9.4 (SAS Institute Inc. 2010) was used after accounting for the complex survey design of the MEPS.
3. Results
3.1. Characteristics of the study sample
Characteristics of the study sample (n=30,827)¸ medical expenditure panel survey 2019-2021 number and row percentage of characteristics by multimorbidity among adults.

Asterisks (*) represent significant differences by Multimorbidity from chi-square tests, ***P <0.001; **0.001 ≤ P <0.01; *0.01 < P ≤0.05.
Wt: weighted; Rx: Medication; Wid./Div./Sep.: widowed, divorced, and separated.
3.2. Association between multimorbidity and HRQoL
Health-related quality of life scores by multimorbidity.

***P <0.001; **0.001 ≤ P <0.01; *0.01 ≤ P <0.05. SD: Standard Deviation.
3.3. Factors related to health-related quality of life among adults
Adjusted multivariable linear regressions on health-related quality of life.
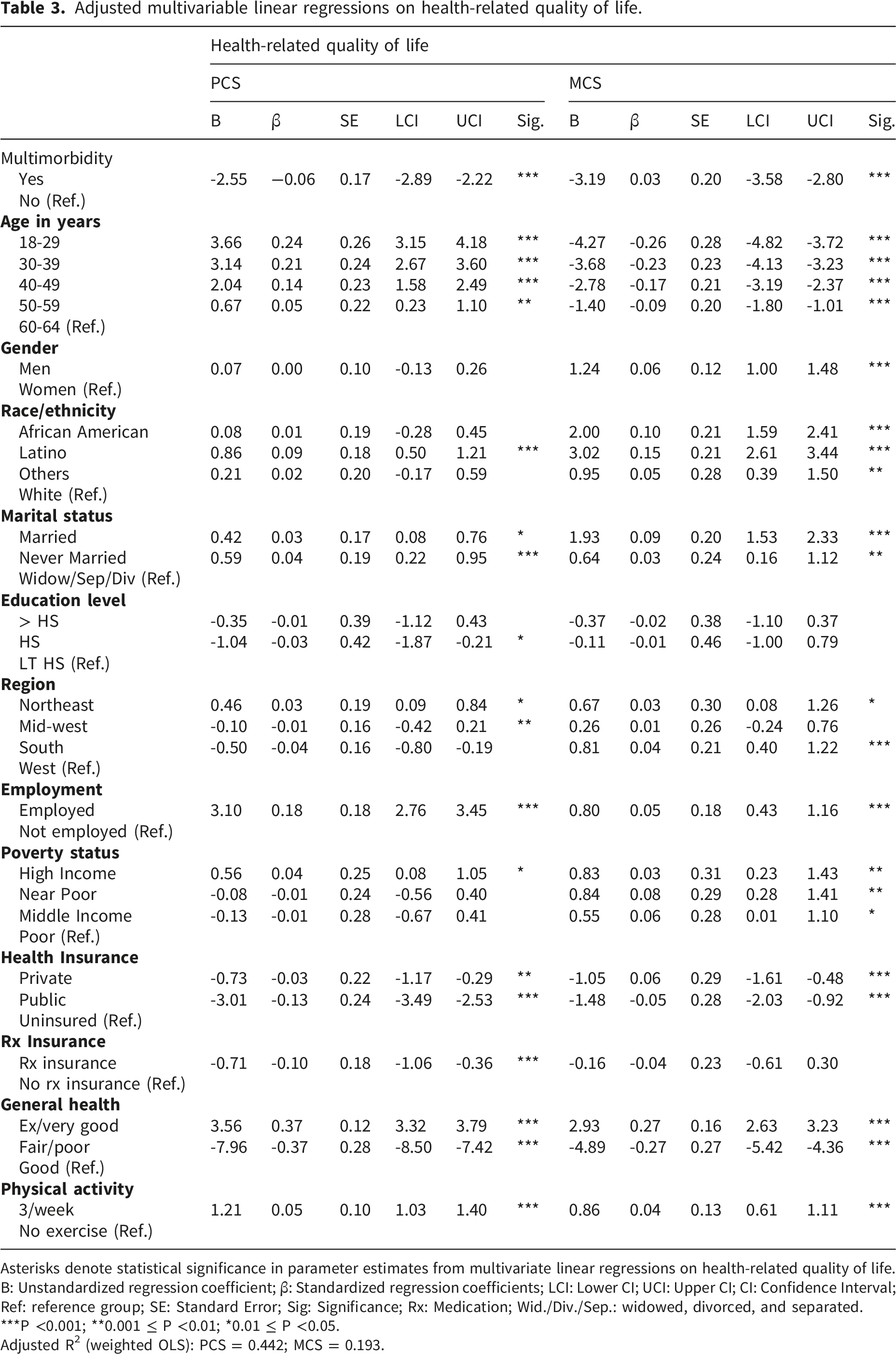
Asterisks denote statistical significance in parameter estimates from multivariate linear regressions on health-related quality of life.
B: Unstandardized regression coefficient; β: Standardized regression coefficients; LCI: Lower CI; UCI: Upper CI; CI: Confidence Interval; Ref: reference group; SE: Standard Error; Sig: Significance; Rx: Medication; Wid./Div./Sep.: widowed, divorced, and separated.
***P <0.001; **0.001 ≤ P <0.01; *0.01 ≤ P <0.05.
Adjusted R2 (weighted OLS): PCS = 0.442; MCS = 0.193.
Factors positively associated with good HRQoL included: sex, race/ethnicity, marital status, employment, perceived general health, and physical activity. For instance, adults who were employed had a higher HRQoL in both physical health summary score (PCS: B = 3.10, p-value<0.001) and mental health summary score (MCS: B = 0.185, p-value<0.001) compared to unemployed. Factors negatively associated with good HRQoL comprised of age group, education level, poverty status, and health insurance. For example, adults with higher income levels had higher HRQoL in both physical and mental health summary scores (PCS: B = 0.56, MCS: B = 0.83, p-value<0.001) compared to those with lower income.
4. Discussion
This study investigated the link between multimorbidity and HRQoL outcome using MEPS data. The results show a negative relationship between multimorbidity and lower HRQoL outcomes. In particular, the study showed that multimorbidity was linked to worse mental and physical domains of HRQoL, with the mental domain being affected more than the Physical domain.
Our findings align with those of prior research. A Belgian study that included 7,509 patients (18 years of age or older) investigated the effects of multimorbidity on the outcome of HRQoL and came to the identical conclusion that multimorbidity had a significant detrimental impact on the mental and physical aspects of HRQoL. 11 Similarly, research employing data from the China Health and Retirement Longitudinal research, which included 9227 adults over 45, demonstrated a significant decline in HRQoL with multimorbidity. 26 Our results also align with the results of research conducted on 1,007 Australians utilizing data from the Australia Survey on household, income, and labor dynamics found a link between multimorbidity and worse scores on the HRQoL physical and component scales (β = − 6.527; Standard Error [SE] = 1.579; β = − 3.765; SE = 1.590). 13 Numerous systematic reviews consistently documented an inverse relationship between multimorbidity and HRQoL, further reinforcing our results.27–29
Beyond multimorbidity itself, socioeconomic status and lifestyle factors were also associated with HRQoL. Importantly, these associations should be interpreted cautiously given the cross-sectional design. While lower income and unemployment were associated with poorer HRQoL among adults with multimorbidity, the direction of these relationships is likely bidirectional, as multimorbidity may both contribute to and result from socioeconomic disadvantage. Chronic illness can impair work capacity and income stability, while socioeconomic stressors may increase vulnerability to multiple chronic conditions. Our findings therefore reflect associations rather than causal effects and underscore the complex, reciprocal pathways linking multimorbidity, socioeconomic status, and quality of life.
There is scientific evidence from a systematic review of 97 studies that lower income was related to multimorbidity and worse HRQOoL; those with higher income were more likely to belong to the “relatively healthy” class. 30 Furthermore, unemployment has been shown to increase the risk of multimorbidity, highlighting the interplay between socioeconomic status and health outcomes. 30 Physical activity has been associated with HRQoL. Literature suggests that moderate exercise is linked to a higher life expectancy in adults with multimorbidities. 30 At the same time, physical activity lessens the impact of multimorbidity on the patient’s quality of life. 31
4.1. Implications
4.1.1. Practical implications
Our research revealed that one out of four adults suffers from multimorbidity. The burden of multimorbidity is significant for healthcare systems traditionally structured on single diseases. 1 Given this burden, a holistic approach to patient management is essential. Healthcare systems should integrate multimorbidity care, prioritizing early evaluation and comprehensive management, as recommended by the National Institute for Health and Care Excellence (NICE) guidelines. 31
4.1.2. Public implications
There is a pressing need for targeted preventive strategies to reduce multimorbidity and enhance HRQoL, especially in vulnerable populations. Public health initiatives should focus on promoting healthy lifestyles, physical activity, and early intervention programs to mitigate the development and progression of chronic diseases.
4.1.3. Policy implications
While this study does not provide causal evidence on the effectiveness of integrated care models, the observed association between multimorbidity and poorer HRQoL highlights the potential relevance of coordinated, patient-centered approaches for individuals managing multiple chronic conditions. This could involve a shift towards value-based healthcare models, where providers are incentivized based on improvements in HRQoL. Such a system would prioritize comprehensive care and proactive management of multiple chronic conditions, ultimately leading to improved patient well-being and a more efficient use of healthcare resources. In addition, funds for multimorbidity education and research and a healthcare system reform to facilitate its management are desperately needed. A reallocation of resources is necessary to support multimorbidity education, research, and comprehensive care models. Policymakers should also focus on developing equitable interventions to reduce the disproportionate burden of multimorbidity among low-income and unemployed populations. In alignment with global health frameworks, these findings contribute directly to the achievement of Sustainable Development Goal 3 (SDG 3)
4.1.4. Research implications
Unlike prior studies focusing on older populations, our analysis identifies multimorbidity-related disparities in working-age adults, revealing an under recognized burden in this demographic. Understanding that multimorbidity encompasses a spectrum of health conditions, future research should identify specific disease combinations that significantly impact HRQoL. This will aid in developing tailored patient management strategies and filling existing knowledge gaps. Further studies should also examine the role of factors such as pain and disability in the multimorbidity-HRQoL relationship, which were not evaluated in this study.32,33 More longitudinal studies are required to establish causality and assess the long-term impact of multimorbidity on health outcomes.
4.2. Study limitations
One of the study’s several drawbacks is that it merely looked at associations between variables; it is not causative. The use of cross-sectional design limits the possibility of establishing causality. Additionally, it is impossible to rule out confounding variables that were not measured on MEPS. For example, this study did not incorporate significant clinical characteristics that may have influenced the association between multimorbidity and HRQoL, such as the severity and duration of the chronic illnesses. In addition, we have not controlled for some risk behaviors, such as alcohol intake and smoking, which both affect the multimorbidity and HRQoL. This underscores the need for more comprehensive studies in our field. Additionally, there may be more than one factor involved in the complicated mechanisms that underlie the association between multimorbidity and HRQoL, such as pain and disability, which have not been evaluated in this study. Further, MEPS relies on self-reported information, which introduces the risk of reporting bias. Multimorbidity was defined using a binary threshold of two or more chronic conditions, which does not capture variation in disease severity, duration, or specific combinations of conditions. This approach may mask important heterogeneity within the multimorbidity group, as different conditions and clusters of conditions may have unequal effects on HRQoL. Although this definition is consistent with prior population-based studies and aligns with the study’s objective of estimating the overall burden of multimorbidity, future studies incorporating condition counts, severity indicators, and disease clustering methods are needed to more fully characterize heterogeneity and its impact on HRQoL.
5. Conclusions
This research contributes to the growing body of evidence on the negative impact of multimorbidity on HRQoL, reinforcing the urgent need for comprehensive healthcare strategies to address this burden. Additionally, this study highlights the need for policy reforms to facilitate a holistic approach to multimorbidity management. Future research should explore longitudinal trends, investigate causal relationships, and assess the effectiveness of interventions tailored to multimorbidity patients.
Footnotes
Consent to participate
This study used a secondary database; thus, patient consent was waived for this research.
Consent for publication
This study used a secondary database; thus, patient consent was waived for this research.
Authors’ contributions
Funding
This research was supported by the Ongoing Research Funding Program, (ORF-2026-1128), King Saud University, Riyadh, Saudi Arabia.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Institutional review board statement
No ethical review or approval is required as this study used an openly accessible secondary database.