
Abstract
Objective
The growing prevalence of chronic morbidity among Nepali older adults reflects the need for studies exploring the patterns and determinants for evidence-based public health strategies. This study evaluated chronic morbidity levels and the associated factors.
Methods
A cross-sectional study recruited 612 participants (≥ 60 years) from all three ecological regions in Gandaki province, Nepal. Chronic morbidity level was derived as the cumulated presence of eight chronic conditions: coronary heart disease, hypertension, stroke, diabetes, cancer, respiratory issues, musculoskeletal conditions, and depression, and then creating three groups: no morbidity, single morbidity and multimorbidity. Ordinal logistic regression analyzed factors associated with morbidity levels, and findings are presented in adjusted odds ratio (OR) and 95% confidence interval (CI). All ethical standards were properly followed.
Findings
About 40% of total participants reported having single morbidity, while 25% had multimorbidity. Participants above 70 years (OR: 1.68, CI: 1.18–2.38) and older women (OR: 2.34, CI: 1.53–3.58) reported odds of being in a higher morbidity category than their counterparts. Older adults without healthcare visits within a year had 90% lower odds (OR: 0.10, CI: 0.06–0.15) of being in a higher morbidity category.
Interpretation
This study underlines the importance of regular healthcare visits, recommending that older adults undergo timely screenings for early diagnosis and effective management. It also emphasizes the need for increased public awareness and health promotion initiatives focused on chronic disease prevention activities within the older population. Additionally, investigating gender-specific factors may provide deeper insight into effective public health interventions.
Introduction
Morbidity is the presence of disease or illness and other states of compromised physical, social, and mental well-being. 1 As individuals age, they become more prone to various chronic conditions and health challenges. 2 Multimorbidity, the state of coexistence of two or more diseases or medical conditions, studies the complex interplay of multiple health conditions within individuals. The World Health Organization has defined “multimorbidity” as the presence of multiple chronic conditions, such as cancer, cardiovascular, and chronic respiratory diseases, in a single person simultaneously, complicating treatment and significantly affecting quality of life. 3
Globally, one in three adults suffer from chronic disease, with half of them experiencing multimorbid conditions. 4 This prevalence stands notably higher for individuals 60 years and older, 5 particularly in low- and middle-income countries such as Nepal. 4 Previous studies in Nepali older adults reported a higher prevalence of multimorbidity, ranging from 13.9% to 22.8%.6–8 Similar trends were observed in bordering countries; India reported a prevalence of multimorbidity among older adults at 32.1%, 9 while China was at 50.5%. 10 Having multiple chronic conditions can decrease functionality and increase disability among older adults, leading to a lower quality of life and a higher risk of mortality. 11 This impacts individuals and their families12,13 and increases the use of healthcare services, thereby increasing healthcare costs. 14
The conceptual model for this study was built upon a comprehensive systematic review of the social determinants of multimorbidity patterns.
15
The model expanded on the social determinants of health model and emphasizes how socioeconomic inequalities, healthcare access, and structural barriers significantly influence population health outcomes. The review identified six main domains that shape multimorbidity patterns: sociodemographic characteristics, socioeconomic status, lifestyle and behavioral factors, living area characteristics, health service use, and social networks and relationships. These domains collectively offered a multifaceted lens for exploring the intricate interplay of social and behavioral factors that contribute to the development and progression of morbidity patterns across diverse populations.
15
The conceptual model is illustrated in Figure 1 below. Conceptual model depicting the relationship between assumed factors and chronic morbidity. Note. This conceptual model was adopted from Álvarez-Gálvez et al.
15

As Nepal continues to undergo demographic and epidemiological changes, the proportion of older adults with non-communicable diseases is anticipated to increase.16,17 However, most studies on morbidity in Nepal are confined to small geographical areas. While similar studies on factors contributing to chronic morbidity among older adults have been conducted in South Asia, this study offers valuable insights into the morbidity status at a regional level and inform implications for shaping health policy at the regional level. The study spans all three ecological regions, including both urban and rural municipalities in Gandaki province of Nepal, and aims to assess the burden of chronic morbidities and explore association with contributing factors.
Methods
This study is reported as per the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline (Checklist 1).
Study design and settings
This research was based on a secondary data-analysis of community-based observational cross-sectional study across three districts in Gandaki province of western Nepal. Figure 2 below explicitly shows the study districts in three ecological regions of Nepal: Manang from the mountain, Tanahu from the hills, and Nawalpur from Tarai. Of all seven provinces, Gandaki province has the highest proportion of older adults with substantial ethnic heterogeneity.18,19 The demographic characteristics of this province and the study districts are presented in Supplemental Table 1. Study districts in three ecological regions of Gandaki Province, Nepal.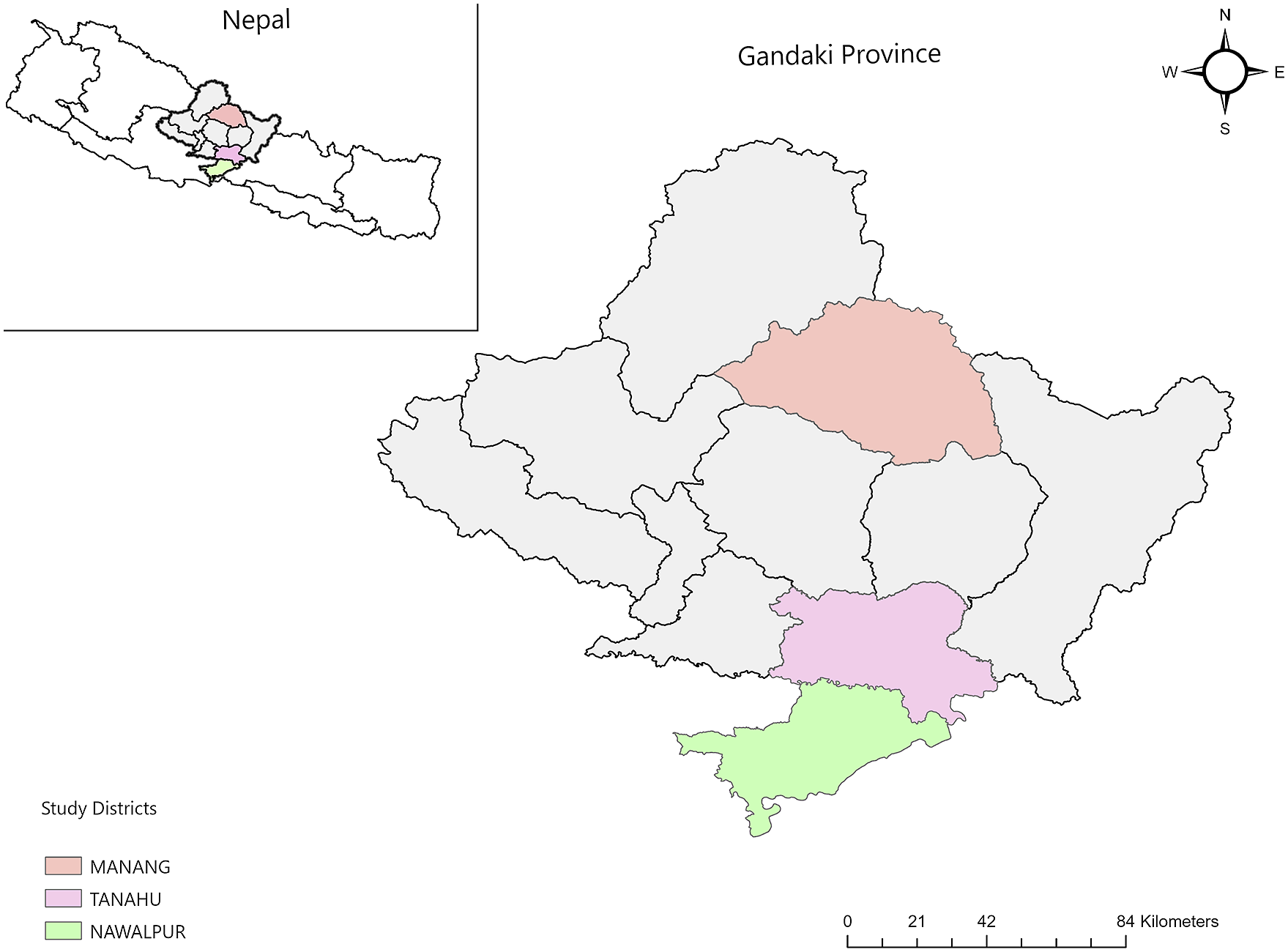
This study implemented a multi-stage stratified cluster sampling design. Initially, three districts, each representing a different topography, were randomly selected. After that, one urban and one rural municipality from each study district were randomly chosen using simple random sampling. However, only one rural municipality was randomly selected in Manang because all municipalities in Manang were rural. Then, wards were chosen randomly as primary sampling units, considering population proportion to size. Since the sampling frame was unavailable, every third household per cluster was randomly selected until the desired sample size of 22 households was achieved. Using a one-proportion sampling method in Stata MP 13.1, 20 an initial sample size of 194 was calculated based on an expected prevalence of 39% and 80% power of the study at 95% confidence interval. Adjustments for a cluster design effect (1.5), non-response rate (5%) and stratification effect (2) inflated the sample size to 614. To ensure equal allocation of 22 samples per cluster, the final sample size was rounded to 616. Details of sample distribution across study districts are in Supplemental Table 2.
Participants who were 60 years or older, a permanent member of the household, and able to establish effective two-way verbal communication in the Nepali language were eligible for the interview. For more than one eligible older adult present in a single household at the time of the interview, only one was randomly selected and interviewed. Proxy interviews were not permitted.
Ethical consideration
The Institute of Medicine, Tribhuvan University’s Institutional Review Committee granted this study’s ethical approval with reference no. 194/(6-11)E2 076/077. Additionally, written permission was obtained from the Social Development Ministry of Gandaki province, referencing no. 1019/075-076, to conduct the study in that region. All participants received comprehensive oral and written information about the study’s purpose and were clearly articulated that their participation was completely voluntary. Further, they were informed that they could withdraw from the study at any point if they felt uncomfortable during the interview process. For those unable to read and write, the consent form was discussed with their trusted individuals, followed by written consent using signatures or thumbprints. Participants were interviewed one-on-one at home to maintain their privacy and minimize the interruptions.
Data collection
The original semi-structured questionnaire in English was translated into Nepali by bilingual experts, and back-translation was also performed to check the accuracy of the questionnaire. Three health science students who co-authored this paper and two local research assistants with past experiences in the field participated in a full one-day training session. This training covered comprehensive aspects of the study, including the questionnaire, interviewing techniques, data collection, safety procedures, and the critical importance of ethics and consent in research. A pilot survey was conducted among 30 older adults in Kathmandu Metropolitan City ward no. 26, following minor typo corrections and a revision of the language tone to enhance clarity. Thus, 612 participants were interviewed face-to-face using paper-based surveys between January and February 2020, with a response rate of 99.4%.
Variables
Dependent variable
Participants were asked whether they were told by a health professional or diagnosed with these eight conditions: coronary heart disease, hypertension, stroke, diabetes, cancer, respiratory disorders, musculoskeletal conditions, and depression. Responses were coded 1 for yes and 0 for no. The total sum of these self-reported conditions determined the range of disease conditions, from 0 to 8, which was grouped into “no disease” for a score of 0, “single morbidity” for a score of 1, and “multimorbidity” for a score of 2 or more. The state of morbidity, defined by these three categories of chronic morbidity, was the dependent variable in this study.
Independent variables
The independent variables were grouped into six main domains, as depicted in the conceptual framework (Figure 1). Sociodemographic characteristics included age, gender, marital status, ethnicity, and disability. Socioeconomic status comprised of education, occupation, and monthly family income. Lifestyle and behavioral factors were measured using smoking status, alcohol consumption, and regular exercise performance. Living area characteristics covered an ecological region, municipality, living arrangement, and family migration history. Health service use included healthcare visits and health insurance enrollment. Social networks and relationships contained participation in social activities and a history of misbehavior.
Sociodemographic factors
Age was right-skewed and was therefore dichotomized into “60 to 70 years” and “Above 70 years.” Participants were “female” or “male” by gender. Participants who were “unmarried,” “divorced,” “widowed,” or “separated” were grouped into “without a partner,” while the other category was “currently married.” Ethnicity was recategorized as “Brahaman/Chhetri,” “Adivasi/Janajati,” and “Others.” 21 As such, “Hill Brahman/Chettri” and “Tarai/Madhesi Brahman/Chettri” were grouped into “Brahaman/Chhetri”; “Newar,” “Hill Janajati,” and “Tarai Janajati” formed the “Adivasi/Janajati,” and “Hill Dalit,” “Tarai/Madhesi Dalit,” and “Muslims” were categorized as “Others.” Nepal’s Gazette 2074 defined the disability status as “person with disability means a person who has long-term physical, mental, intellectual or sensory disability or functional impairments or existing barriers that may hinder his or her full and effective participation in social life on an equal basis with others.” 22 Participants without any disability were grouped as “without disability,” while those who had at least one disability were grouped as “with disability.”
Socioeconomic status
The participants’ educational status was divided into three categories: “no education,” “non-formal education,” and “formal education.” Individuals unable to read or write were classified as having “no education,” those who underwent training outside of traditional schools, especially adult education for literacy, were labeled with “non-formal education,” and those attending formal educational institutions were designated as having “formal education.” In terms of occupation, individuals engaged in agriculture, homemaker, or unemployed were categorized as “homemaker/agriculture/unemployed” as the frequency of unemployed was very low. Those involved in business or service or participating in wage labor or other income-generating activities were classified as “business/service/other.” Monthly family income in Nepali rupees was converted to United States dollars (US$) using a conversion rate of $1=NPR 118.51, the average conversion value in 2020. 23
Lifestyle and behavioral factors
Smoking and alcohol consumption statuses were assessed as “never,” “former,” and “current or occasional.” Regular exercise performance was assessed by asking “Do you perform exercise regularly?” and was measured as “yes” or “no.”
Living area characteristics
Manang from the mountain, Tanahu from the hill, and Nawalpur from the Tarai represented the three ecological regions of Gandaki province. The Government of Nepal’s Gazette 2073 predefined studied municipalities as urban or rural. 24 Living arrangements included “only with spouse,” “son/daughter-in-law,” “daughter/son-in-law,” and “other relatives.” The fourth category, “other relatives,” comprised “grandchildren,” “nephew/niece,” “brother/sister,” and “others.” The family migration history was assessed by asking if either of the family members had migrated from another place within or out of the country to the current location. The responses were “yes” or “no.”
Health service use
Healthcare visits were measured by asking if participants visited medical institutions within a year. The health insurance enrollment was assessed by asking if participants had enrolled in any health insurance program. The responses to these questions were “yes” or “no.”
Social networks and relationships
Participants were asked if they ever participated in any social activities held in the community within the last year, and they responded either “yes” or “no.” The history of misbehavior was measured overall as any instances encountered within the family or the community and responses were recorded as “yes” or “no.”
Data management and analyses
Demographic, socioeconomic, and health characteristics of study participants.

Note. n=counts, %=percentage, Md=median, Q1=first quartile, Q3=third quartile. #Others included Hill Dalits, Tarai Dalits and Muslims.

Heatmap illustrating co-occurrence of chronic diseases in study participants.
Bivariate relationship of assumed factors with morbidity status.

Note. df = degrees of freedom;
1Kruskal-Wallis one-way analysis of variance; rest all Pearson Chi-square test of independence.
Factors associated with odds of higher morbidity.

Note. PE=parameter estimate; SE=standard error; OR=adjusted odds ratio; CI=confidence interval; concordance-statistics, c=0.76.
1Others included Hill Dalits, Tarai Dalits and Muslims.
Results
Participant’s characteristics
Table 1 below depicts the participant’s characteristics. Sociodemographic characteristics indicated that the majority of the participants were between 60 and 70 years old (56.7%), female (57.2%), and currently married (62.9%). The largest ethnic groups represented were Adivasi/Janajati (46.4%) and Brahaman/Chhetri (41.2%). Approximately 44% of participants were with disabilities. By socioeconomic status, over three-quarters of participants had no education (79.7%) and were either homemakers, involved in agriculture, or unemployed (87.1%). The median monthly family income was $126.6 (Q1=67.5, Q3=253.1). Among lifestyle and behavioral factors, the majority of participants were currently or occasionally smoking (42.0%), had never consumed alcohol (50.0%), and did not perform regular exercises (77.8%).
Regarding living area characteristics, participants mostly lived in the Tarai region (57.2%) and urban municipalities (68.1%). Most lived with their son/daughter-in-law (67.0%) and had no family migration history (64.4%). Interestingly, while 73.2% visited healthcare institutions within a year under the health service use domain, 91.7% of participants were not enrolled in any healthcare insurance plans. Variables related to social networks and relationships indicated that 58.2% did not participate in any community social activities in the past year, and 28.4% reported having a history of misbehavior over their life course.
One-fourth (25.0%) of participants reported having multimorbidity, 40.2% reported a single morbidity, and 34.8% reported no morbidity.
Prevalence of single and co-occurrence of disease
The heatmap diagram below (Figure 3) illustrates the prevalence of self-reported single disease or co-occurrence of pairs of diseases in the studied population. Each cell in the heatmap represents the percentage of participants diagnosed with either a single disease (a diagonal line, where the row and column represent the same disease) or two distinct diseases (where the row and column represent different diseases). The color gradient, ranging from blue (0%) to yellow (30%), visually conveys the degree of occurrence for single disease or pair of diseases.
The top 3 prevailing diseases among older adults in this study were musculoskeletal disease (34.5%), hypertension (28.6%), and respiratory disease (16.5%). These three disease pairs made the highest percentages of co-occurrence; when counted together ranked highest for hypertension and musculoskeletal disease at 10.5% followed by musculoskeletal and respiratory disease at 5.6% and then by hypertension and respiratory disease at 5.1%. All other diseases reported low paired prevalence, with stroke and cancer showing the lowest value of pairs with other diseases.
Bivariate descriptives
Table 2 below presents the bivariate assessment. Age [
Covariates of chronic morbidity levels
Table 3 below details the results of the final adjusted ordinal regression. The score test for the proportional odds assumption
Among participants of age above 70 years, the odds of being in a higher morbidity category (increasing morbidity) rather than a lower category were 1.68 times the odds (OR: 1.68, CI: 1.18–2.38) for older adults aged 60 to 70 years after controlling for all other variables in the model. Females reported greater odds of having higher morbidity (OR: 2.34, CI: 1.53–3.58) when compared to their male counterparts, holding all other covariates in the model constant. While disability variable only approached significance at p=0.059, compared to those without disability, those with disability showed greater odds of reporting higher morbidity (OR: 1.38, CI: 0.99–1.93). Similarly, the municipality variable was close to significance at p=0.068. Compared to the older adults living in rural municipalities, those who resided in urban areas reported 43% higher odds of increasing morbidity (OR: 1.43, CI: 0.97–2.10). Interestingly, compared to those who visited healthcare services within the last year, those who did not showed 90% lower odds of being in higher morbidity (OR: 0.10, CI: 0.06–0.15).
Discussion
This study examined the status of chronic disease burden and the association between different factors of chronic morbidity levels among older adults in Gandaki province, Nepal. About 40% of the participants self-reported having a single chronic disease, while one-fourth (25.0%) reported having two or more chronic conditions. Previous studies in Nepal reported the prevalence of single chronic condition ranging from 48.9% to 66.5%, while multimorbidity ranging from 13.9% to 22.8%.6–8 The ordinal regression model showed that age, gender, and healthcare visit had significant associations with chronic morbidity status, while disability status and municipality type approached significance at p=0.059 and p=0.068.
Among the various disease combinations observed in the study population, musculoskeletal disease showed the highest co-occurrence with other chronic conditions. Specifically, 10.5% of participants had both musculoskeletal issues and hypertension, while 5.6% experienced a combination of musculoskeletal and respiratory problems. While a previous study from eastern Nepal did not explicitly state a pair of diseases, the study reported the highest prevalence rates for hypertension and osteoarthritis among older populations. 8 Another study in rural Nepal reported a higher prevalence of these two disease conditions. 6 These findings highlight the critical need for integrated geriatric care and early healthcare interventions to address the significant burden of chronic morbidities, particularly musculoskeletal, hypertension, and respiratory problems, in the older Nepali population.
Age group was a significant factor, showing higher odds of chronic morbidity among the higher age categories. This finding aligns with the well-established understanding of medical science and epidemiology. 29 However, it is also important to recognize that chronological age is not a direct cause of chronic disease, 30 neither aging itself is a disease. 31 Instead, it is associated with an increased risk of disease due to the cumulative impact of various social, economic, and health-related factors throughout a person’s life.30,31 Consequently, higher age is consistently associated with increased odds of multimorbidity.6–8 For example, in previous studies, multiple chronic conditions were observed across 30% of adults between 45 and 64 years, 65% between 65 and 84 years, and 82% of those aged 85 and above.4,11
Chronic diseases are more prevalent in older adults as a result of the natural aging process and the physiological changes that accompany it. Moreover, gender differences have been observed in the presence of chronic disease and multimorbidity among the older population. In this study, older women were associated with higher odds of having higher chronic morbidity compared to older men, which was consistent with previous studies.8,14,32 Biomedical literature indicates that women experience higher rates of morbidity compared to men, with increased incidences of chronic physical and psychiatric conditions.33,34 Particularly in Nepal, historically, patriarchal structures have prevailed in the society, influencing various aspects of life for women, including inadequate access to resources and decision-making. 35 Therefore, women may have lower access to health services, causing delayed preventive measures and leading to a higher rate of chronic morbidity than older men.
In this study, participants who did not visit healthcare facilities in the past year were associated with lower odds of increased chronic morbidity than those who had visited healthcare facilities. This indicates older adults with higher chronic morbidity may have regularly visited health facilities due to their conditions for the treatment rather than promotive and preventive health care services utilization. 36 On the contrary, lower healthcare utilization could reflect varying health statuses: positive aspects, such as better overall health influenced by healthy lifestyle behaviors leading to low experiences of morbidities; 37 or negative ones, such as barriers to accessing preventive healthcare like geographic, financial, or cultural obstacles, 38 which might mean that only those with more severe conditions seek medical care. 39 Previous studies showed that more than 30% of older adults with chronic disease do not utilize healthcare services,38,39 suggesting that symptom-less older adults could underutilize the healthcare services than those with comorbidities. 38 Similarly, in the lack of regular health checkups, older adults may have more undiagnosed conditions, potentially leading to lower reported rates of chronic morbidity. Additionally, preferences for traditional or self-care practices over modern healthcare services could play a role, which was not discussed in this study. 39 Thus, this warrants further investigation to better understand the role of healthcare utilization, taking into account the broader social and cultural contexts in predicting chronic morbidities.
Older adults residing in urban municipalities had higher odds of reporting an increased level of chronic morbidity compared to those in rural areas, but the relationship was statistically approaching significance. Although place of residence was not significant in our study, previous studies have found that urban residence was associated with multimorbidity among older adults.7,8 When ethnicity was excluded from the final regression analysis, urban residence became a statistically significant predictor. As both municipality type and ethnicity were statistically significant in bivariate analysis, ethnicity may moderate the relationship between urban living and multimorbidity in older adults. On top of that, few studies found that ethnic minorities are at the highest risk of having multimorbidity. 8 Indeed, caste and ethnicity have traditionally been rigid social constructs in Nepali society, which still persists, especially among older generations. Particular groups such as Dalits and some ethnic minorities have long faced systemic oppression and exclusion based on their caste and ethnicity. 40 Previous studies showed that privileged ethnicity was associated with higher odds of utilizing health services and higher out-of-pocket health expenditures,36,38 and higher concentration of privileged ethnic groups in urban areas. 41 However, a recent study also suggested that higher ethnic diversity may promote a better overall quality of life among older adults. 42 Therefore, future studies should consider these aspects to understand better and assess the complex interplay between ethnicity, urban-rural residence, and morbidity patterns among older adults in Nepal.
The finding on the influence of urban residence on multimorbidity aligns with other studies suggesting that urban living for older adults may be associated with higher chronic morbidity due to pollution, stress, sedentary lifestyle, unhealthy dietary habits, and other factors related to urban living conditions.8,43 Conversely, many rural communities in Nepal are situated in remote, hard-to-reach areas, making it challenging for older residents to access healthcare facilities. 44 Thus, negligence in routine health check-ups among older adults in rural areas may have led to the underdiagnosis of chronic conditions among rural participants.45,46
Disability status in this study was close to significance, which suggests a potential interaction of disability status with other variables, which might have diluted the main effect of disability on levels of morbidity in this study. Earlier studies identified disability as a consequence of one or more chronic diseases, 47 although this relationship can also go bi-directional. 48 Furthermore, the association underscores the compounded challenges faced by individuals with disabilities, who may have higher levels of social isolation, 49 increased vulnerability to chronic conditions, 50 and limited access to healthcare. 51 Thus, this relationship is complex and warrants further investigation into studying the role of disability status in predicting chronic morbidities.
After adjusting for other variables in the regression analysis, the significance of alcohol consumption status and participation in social activities was lost, but other studies conducted in Nepal have indicated potential associations between these variables and morbidity status in older adults. Interestingly, previous studies from eastern Nepal showed that without a history of alcohol consumption exhibited higher odds of multimorbidity, a finding that seems counterintuitive.6,52 However, a systematic analysis from the Global Burden of Disease Study 2020 explained that limited alcohol consumption may show a marginal protective effect against certain conditions, such as cardiovascular diseases, particularly among old age groups. 53 Therefore, future research should integrate patterns and levels of lifestyle and behavioral factors such as smoking, alcohol consumption, and tobacco use over time through longitudinal studies to infer causality between these two variables. Additionally, alcohol consumption varies highly among different ethnic groups in Nepal. 54 Therefore, it might be useful to test the moderating role of ethnicity in determining the association between alcohol consumption and multimorbidity in Nepal.
Engaging in social and cultural activities has demonstrated positive effects on the overall health and well-being of older adults.55,56 However, the relationship may be bidirectional, as individuals with more health conditions or morbidities might engage less frequently in such activities. Therefore, this study underscores the need for careful and thorough investigation into this dynamic. Likewise, there are some other potential confounders such as diet and physical activity not controlled in this study, which are predictive of morbidities in older adults, that should be considered in future studies.
Study implications
The findings from this study have several implications for public health interventions in Nepal. Given the higher morbidity in urban areas, targeted public health interventions are needed to focus on the older urban population. Strategies could include improving access to healthcare, particularly preventive health services, promoting healthier urban environments, and addressing lifestyle factors contributing to higher chronic morbidity among older adults. However, preventive health studies are needed to determine whether older adults in rural areas can access and utilize preventive health services. It is generally recommended for individuals to have an annual routine health check-up after age 40 to prevent adverse health outcomes. 57 Thus, programs aimed at preventing and managing chronic conditions should strategically target high-risk populations, integrate preventive measures across various sectors, and empower individuals to take control of their health, as these conditions often accumulate and are diagnosed in later years. 29
The higher prevalence of chronic morbidity among women highlights the need for gender-sensitive health initiatives that address the specific health needs of older women. Ensuring equitable access to healthcare and supporting health-related burdens could be beneficial. Also, lower chronic morbidity for those with no healthcare visit in the previous year is tricky. It hints towards either unmet healthcare utilization or existing preference for traditional healthcare practices, which warrant thorough investigation and policy interventions. Additionally, enhancing support systems for older adults with disabilities is crucial. This could involve improving accessibility to healthcare facilities, providing assistive devices, and ensuring social inclusion to reduce morbidity associated with disability.
Study strengths and limitations
This study employed a comprehensive sampling method to cover all three ecological regions of Gandaki province, Nepal, with an impressive response rate. It used a rigorous methodology to examine the progression of chronic diseases from no morbidity to single and multiple chronic conditions. However, there are some limitations to acknowledge.
The findings are specific to Gandaki Province and may not apply to all older adults in Nepal, but they offer relevant insights that could be relevant to other provinces with similar ecological and societal contexts across the country. The cross-sectional design restricted the ability to infer causality between the studied variables and morbidity. Self-reported data on chronic conditions may be subject to recall or social desirability bias. Routine healthcare visits are uncommon in Nepal, and many individuals may remain unaware of their disease status until it becomes severe, potentially leading to an underestimation of chronic conditions and multimorbidity due to underutilization of healthcare services. Employing longitudinal methods will be crucial for obtaining comprehensive results.
Supplemental Material
Supplemental Material - Chronic morbidity levels and associated factors among older adults in western Nepal: A cross-sectional study
Supplemental Material for Chronic morbidity levels and associated factors among older adults in western Nepal: A cross-sectional study by Aman Shrestha, Krishna Prasad Sapkota, Isha Karmacharya, Lirisha Tuladhar, Preeti Bhattarai, Pratik Bhattarai, and Bharat Kafle in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgments
We express our sincere appreciation to the Social Development Ministry and the local authorities in Gandaki province for their unwavering support throughout this study. We also acknowledge the participants who graciously devoted their time and provided invaluable insights into this study.
Author contributions
AS, BK, KPS and PB1 conceptualized the study; BK supervised the fieldwork; BK, PB1, and PB2 were responsible for fieldwork; AS analyzed the data; AS and KPS interpreted the findings; AS, IK, LT and KPS wrote the first draft of the paper; all co-authors made critical revisions of the manuscript and approved the final version of the manuscript. Note. PB1: Preeti Bhattrai; PB2: Pratik Bhattarai.
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.