
Abstract
Background
The dynamics of working within multidisciplinary teams (MDTs) to manage diabetes and comorbidities remain underexplored. Investigating physicians’ experiences provide insights into the benefits and challenges of MDTs in this complex context, paving the way for improving current practices and shaping future interventions to better address the needs of this patient population.
Aim
To explore perceived benefits and barriers of MDTs in the management of people with diabetes and comorbidities among physicians.
Methods
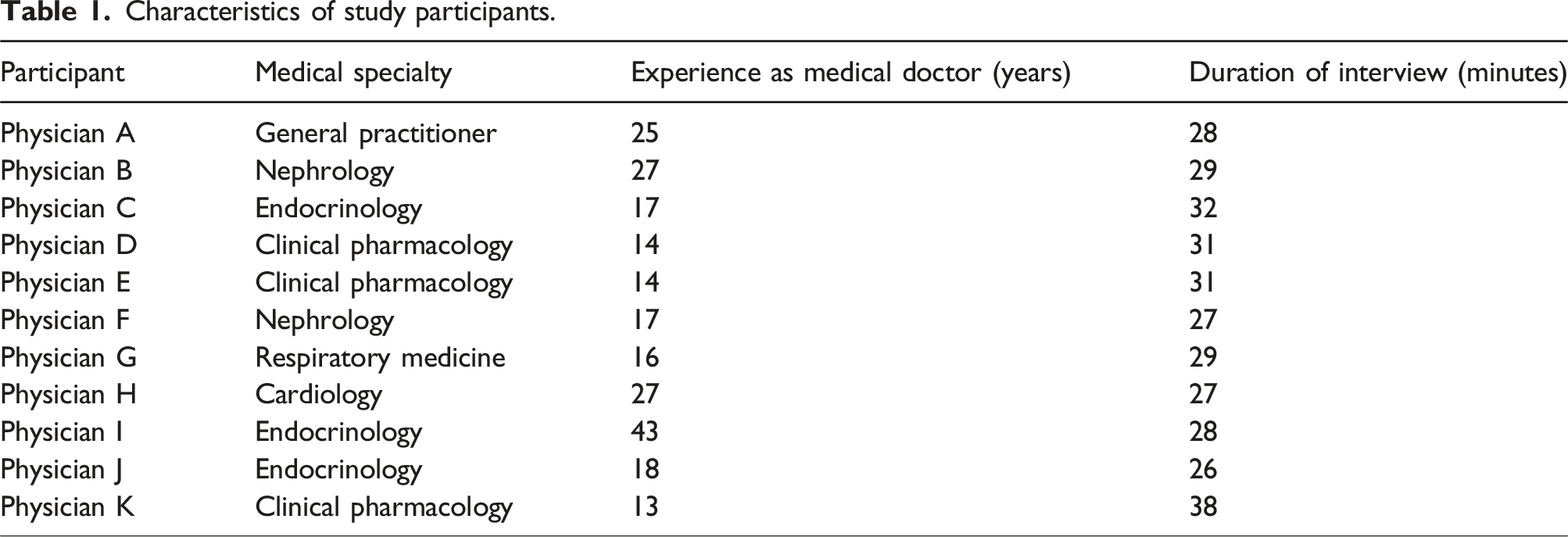
Eleven semi-structured interviews (duration 26-38 min) were conducted online among physicians. Criterion sampling of physicians from relevant medical specialties and with experience from MDTs were included. Interviews were analyzed using thematic analysis.
Results
Four major themes emerged from the thematic analysis: (1) benefits of MDT, (2) challenges related to MDT, (3) the need for MDTs and cross-sectorial work, and (4) prerequisites for successful MDTs. Improved professional learning and relationships, enhanced capacity leverage, and optimized treatment were some of the major benefits. Siloed healthcare systems and cultures and resource demanding MDTs were considered barriers. Composition and outline of the MDTs, including the role of general practitioners (GPs), were considered important aspects of MDTs. The increase in multimorbidity, polypharmacy, and complexity in patient pathways necessitates MDTs and cross-sectorial work.
Conclusion
Our findings indicate several benefits and barriers of MDTs. MDTs and cross-sectorial work are needed prospectively in healthcare and hold the potential to embrace some of the challenges encountered by people with diabetes and comorbidities. Understanding and incorporating experiences of physicians could inform future improvements in care management.
Background
Diabetes is a serious chronic disease that is estimated to affect 537 million people worldwide. 1 Having diabetes over time is often associated with several other conditions such as cardiovascular diseases, kidney diseases, respiratory diseases, and mental disorders.2,3 These additional conditions to diabetes are referred to as comorbidities where diabetes is considered the index condition.3,4 Multiple long-term conditions (MLTCs), or multimorbidity, are often defined as the co-occurrence of two or more chronic conditions in the same individual (without an index condition).5–7 Both terms will be used interchangeably throughout this study to emphasize the challenges of living with multiple conditions, however, the main focus remains on people with diabetes and comorbidities. Healthcare systems are increasingly challenged by the increasing prevalence and incidence of people with both diabetes and comorbidities with complex healthcare needs.3,7–9 Compared to single-condition counterparts, people with MLTCs experience higher mortality and morbidity rates, lower functional capacity, polypharmacy (intake of multiple drugs), and higher healthcare utilization.3,6,7,10,11 Social disparities are also prevalent among people with MLTCs with a higher prevalence of multimorbidity among socioeconomically deprived groups.9,12–14
In the modern-day healthcare system several challenges present for people with diabetes and comorbidities. Due to siloed healthcare systems, patient pathways are often fragmented and poorly coordinated hampering effective communication both within and across sectors.6,15,16 People with MLTCs commonly experience a high treatment burden in terms of understanding and complying with care plans.8,17 Engaging with different healthcare professionals (HCPs) and attending multiple appointments may negatively affect health-related quality of life and treatment satisfaction and lead to worsening of treatment outcomes.15,16,18,19
In light of these issues, there is a pressing need to reconfigure healthcare delivery to facilitate more integrated, patient-centered care and reduce care fragmentation. A potential solution is the implementation of multidisciplinary teams (MDTs), which offer a structured and integrated approach to healthcare delivery. MDTs are widely utilized across various areas of today’s healthcare system, providing collaborative consultation among HCPs. 20 Physicians play a pivotal role within these teams, serving as the key actors responsible for treatment decisions and the overall management of patient care. 20 In MDTs, physicians from various specialties collaborate to review patient cases, adjust treatments, and coordinate patient-centered care across primary and secondary settings.21–23 Their decisions are guided by clinical guidelines and their combined expertise, enabling a holistic approach that moves beyond the condition-specific focus of traditional healthcare systems.20,24 MDTs have shown promising outcomes in managing diabetes and multimorbidity, including improved glycemic control, reduced complications, enhanced mental health, increased cost-effectiveness, fewer hospital visits, and minimized blood sample requirements.24–27
Despite the promising results of the MDTs, the evidence regarding physicians’ perceptions of the MDTs in a diabetes and comorbidity setting remains sparse. To the best of our knowledge, only a limited number of studies have explored the perceived benefits and barriers among physicians toward MDTs in a diabetes setting.21–23 Two of the studies focused solely on type 2 diabetes and did not include any comorbidities in their study population.22,23 The consideration of comorbidities is crucial, as the presence of MLTCs significantly increase the complexity of the intervention. This is due to the need to address not only the intricate management of diabetes but also the management of other chronic conditions concurrently, resulting in a highly complex intervention.6,24 Thus, there is a need to explore the perspectives of physicians, the key actors in MDTs, to gain insights into opportunities and challenges associated with MDTs. Therefore, this study aims to explore the perceived benefits and barriers toward an MDT approach among physicians involved in the management of people with diabetes and comorbidities.
The findings from this qualitative study will inform the ongoing development of MDTs and potentially other multidisciplinary interventions or initiatives, including an ongoing feasibility trial aimed at increasing treatment coordination for people with diabetes and comorbidity. 25
Methods
Research design
This study employed qualitative research methodology, utilizing semi-structured expert interviews to gather data. Expert interviews are especially useful when the aim is to explore or generate data and knowledge within a very specific field of interest. 26 A hybrid phenomenological-hermeneutic approach was used to investigate the perceived benefits and barriers of MDTs from the perspective of physicians and to explore the phenomenon of MDTs in healthcare. 31 The phenomenological aspect primarily guided the initial stages of the study, including data collection through interviews and the processes of reading, transcribing, and coding the data. In the later stages of analysis, a hermeneutic approach was applied to relate the identified themes to the perceived benefits and barriers of MDTs. The study was guided by the Standards for Reporting Qualitative Research checklist. 27 A study protocol was prepared for the present study and registered at Open Science Framework before any data collection (https://osf.io/xe6y8).
Ethical considerations
In Denmark, interview studies do not require approval from an ethics committee as this type of research does not fall within the jurisdiction of the regional ethics committee (LBK number 1338 of 01/09/2020). Verbal and written information of the study objectives and legal rights, including storage of data, was given before initiating the interviews. Verbal and written informed consent were obtained from all participants before conducting the interviews. The study was conducted in accordance with the Declaration of Helsinki.
Study setting and recruitment
The present study was conducted online via Microsoft Teams at the Department of Health Science and Technology at Aalborg University, Denmark. Potential participants were identified through networking and snowballing methods, specifically targeting physicians with experience working in a hospital setting and within MDTs in the context of diabetes and comorbidities. Participants were recruited by email, phone, or face-to-face by request, and interview schedules were arranged by email correspondences between the interviewer and participant. Potential participants were recruited from a tertiary diabetes setting and university hospital in Aalborg (Region North Denmark), from a tertiary diabetes setting and university hospital in Odense (Region Southern Denmark), and from general practice in Region Southern Denmark.
The study used criterion sampling to recruit physicians who met the following criteria: • Danish speaking and understanding. • From a clinical medical specialty related to the management of diabetes and comorbidities, i.e., endocrinology, cardiology, nephrology, respiratory medicine, clinical pharmacology, or general practice. • Experience with MDTs specifically focused on managing diabetes and comorbidities, as well as attendance at previous MDT conferences.
Physicians meeting any of the following criteria were excluded: • Lack of experience with MDTs, or experience limited to MDTs from disease areas other than diabetes and comorbidities. • Belonging to medical specialties unrelated to the management of diabetes, such as neurosurgery.
Researcher characteristics and reflexivity
The corresponding author, JDA, a trained physiotherapist with four years of clinical experience in managing musculoskeletal and sports-related injuries, conducted all interviews. At the time of the study, JDA was a Ph.D. student at Aalborg University with prior knowledge of challenges and potential benefits of MDTs, gained through literature reviews and participation in three MDT conferences. JDA also possessed knowledge about the challenges and opportunities in the prevention and management of people with diabetes and comorbidities. JDA had minimal experience in interview-based research as this study was his first major endeavor in the qualitative research paradigm. Throughout the study, JDA was supervised by experienced qualitative researchers with extensive expertise in semi-structured interviews and thematic analysis. While JDA had no personal relationship with any of the participants, some of the participants were familiar with JDA from previous encounters in different contexts.
Data collection
Data were generated from semi-structured interviews with eleven physicians to explore the perceived benefits and barriers of MDTs and cross-sectorial work. Interviews took place between September and November 2023 and were conducted online using the Microsoft Teams platform (version 25017.203.3370.1174). We chose this method to increase flexibility and accessibility for both the interviewer and the participants. Each participant was interviewed once, and the duration of the interviews ranged from 26 minutes to 38 minutes. The interviewer conducted the interviews from an uninterrupted office, while the participants joined online from their respective locations.
Development of the interview guide
The interview guide was developed according to the five phases described by Kallio et al. 28 First, a preliminary assessment was conducted to determine the suitability of conducting a semi-structured interview. Based on the research questions in the present study, the use of a semi-structured interview guide was deemed appropriate. Second, the interview guide was constructed based on a combination of literature reviews and clinical insights. The third step involved outlining the main themes and follow-up questions for each theme in the preliminary interview guide. The fourth step included a pilot test of the interview guide involving an internal test with co-author SHL, an expert assessment with an experienced qualitative researcher, and finally field-testing with an external participant, who met the specified inclusion criteria. The final step included refining the interview guide based on the feedback from the pilot tests and producing the final version utilized for the interviews. 28
Data processing
The audio recorded interviews via Microsoft Teams were transcribed verbatim. The transcribed data was uploaded to NVivo 20, and the software was used during data analysis for generating initial ideas and codes, and subsequently for coding the data. To ensure anonymity among the included physicians they are presented as “Physician A, Physician B, etc.”. Both recordings and transcripts were stored on a safe server via Aalborg University.
Data analysis
The analysis on the transcribed data followed the six-step guide on thematic analysis described by Braun and Clarke. 29 A semantic approach was used where themes were identified within the explicit or surface meaning of the data. 29 As such, the data was organized and summarized to identify patterns in semantic content followed by interpretation of the themes. In the first step, JDA familiarized himself with the collected data, transcribed the data, read and re-read it to note interesting ideas. In the second step, JDA and SJB generated initial codes from the transcribed data, and JDA subsequently coded the entire dataset. In the third step JDA sorted the collated codes in a search for potential themes, and in the fourth step JDA reviewed the themes and checked whether the coded extracts aligned with the themes and whether the themes aligned with the entire dataset. When no new themes emerged, this process was ended (i.e., data saturation was achieved). This was carried out by JDA and supervised by SH. During the fifth step, themes were further specified and refined before being translated from Danish into English by JDA, finalized, and reported in the sixth step. 29
Trustworthiness and transparency
To enhance trustworthiness and transparency, the study followed the four aspects of credibility, transferability, dependability, and confirmability. To increase credibility, different participants with varied perspectives and experiences were included, ensuring representativeness of the collected data. Additionally, to enhance transferability, the study incorporated a double-center approach and included a discussion of transferability of the findings in the discussion section. Dependability was established through a comprehensive description of study procedures and analysis, including the use of semi-structured interviews and thematic analysis, thereby ensuring transparency and enabling potential replication. Before conducting the full thematic analysis, JDA discussed the initial findings with two co-authors (SH and SJB). Based on these discussions, JDA analyzed the remaining interviews and discussed the preliminary findings and themes with co-author SH. Afterwards, SH went through 25% of the coded data to verify the sub-themes and major themes to improve confirmability. To increase trustworthiness of the findings further, we followed the 15-step checklist of criteria for good thematic analysis as described by Braun and Clarke. 29
Results
Participant characteristics
Characteristics of study participants.
Synthesis and interpretation
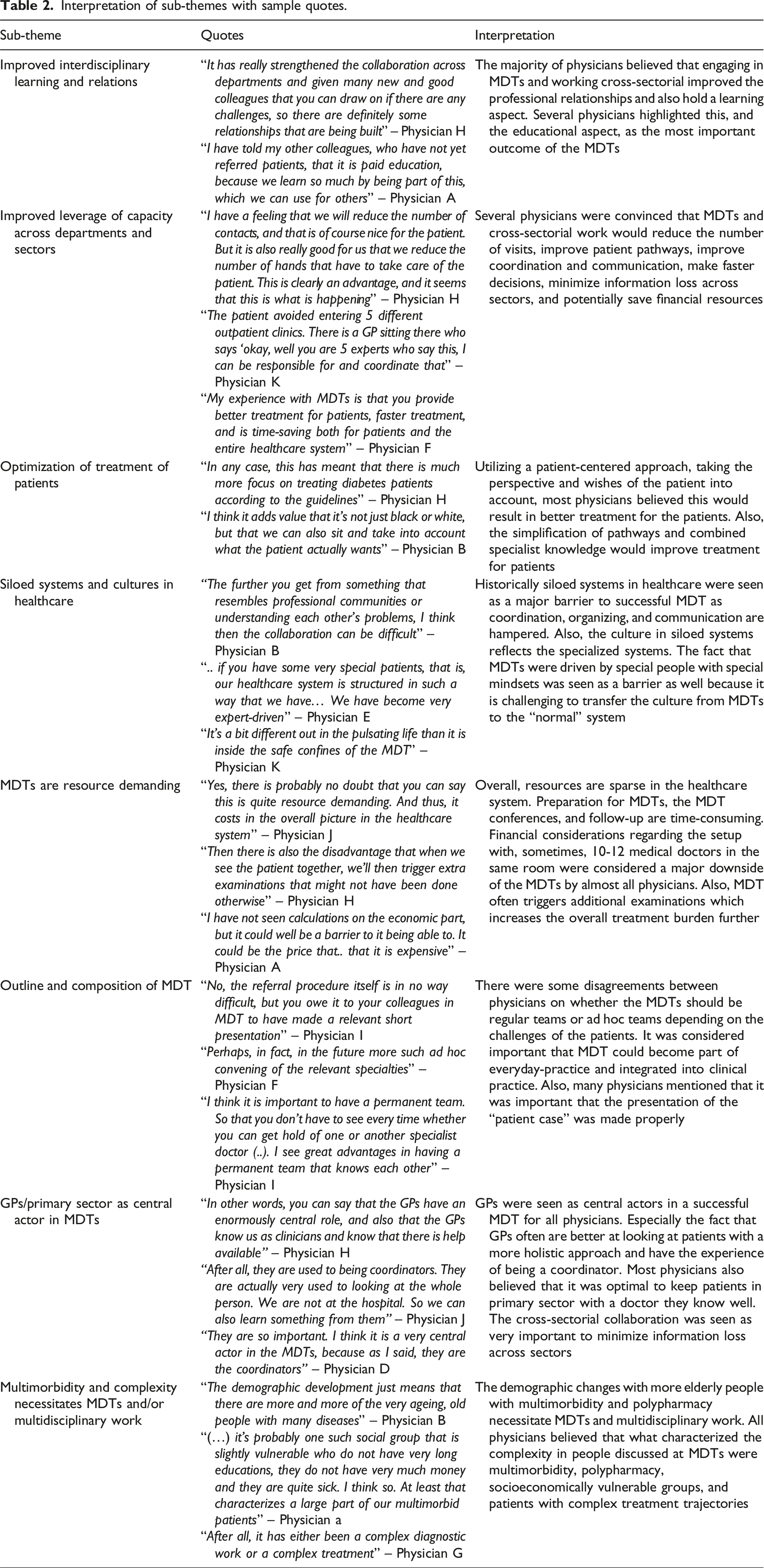
Four major themes emerged from the full thematic analysis: Benefits of MDT, Challenges related to MDT, Prerequisites for successful MDT, and The need for MDTs and cross-sectorial approach. Each major theme constituted 1-3 sub-themes illustrated in Figure 1. Major themes as well as sub-themes were based on descriptive semantic analysis of the thematic analysis. The findings from the major themes, including sample quotes, can be found below, and the findings from the sub-themes can be found in Table 2 with corresponding sample quotes and interpretations. Major themes with related sub-themes. Interpretation of sub-themes with sample quotes.
Benefits of MDT
All physicians perceived the multidisciplinary work and the MDTs to yield positive outcomes. The interdisciplinary learnings on treatment options and professional knowledge were mentioned as major benefits of the MDTs and the multidisciplinary work. Particularly the strengthened professional and personal relationships were highlighted such as the security in taking responsibility for a treatment when having expert advice behind you: “It's something completely different when you sit in the same room and focus on helping the same patient (….) there is a lot of learning in that, but also the personal relationships with those inside the hospital who treat our patients, which I think is hugely important and I am really in favor of tearing down the walls between the sectors” – Physician A. ” And also, professional knowledge, I think I have learned a lot (…) my learning curve it has been increasing, that is... I have really, really learned a lot about how other professional groups or other specialties manage the problems, where other times, where you don't have the opportunity for MDT discussion, you sit by yourself” – Physician F.
The physicians highlighted how working across sectors and in teams was perceived to reduce hospital visits/contacts and reduce the number of patient pathways across sectors as part of improving coordination and simplifying treatment. Many physicians mentioned that often a patient has pathways in both primary and secondary care as well as in the municipality, where the same things are being discussed independently. Using MDTs, the patients only need to enter one sector (i.e. primary or secondary care) instead of two or three due to the improved communication and coordination of care. “I actually also think that it can reduce some hospital visits because if I have to think back on the last patient that I referred, I could well have sent him to 2 different outpatient clinics. Now it looks like we can manage it with one outpatient visit, which means it probably saves some money, and I could also imagine that it saves some consultations” – Physician A.
Several physicians addressed how the involvement of patients to incorporate their perspectives could be a way of optimizing treatment, acknowledging how patient and physician perspectives can differ to various degrees. Two main methods mentioned was utilizing patient-reported outcomes questionnaires and having the patient attend the MDT. Some physicians said that patient attendance on the MDT could affect the efficiency in the MDT. However, most physicians did find patient involvement important: “There can be enormous divergence in relation to what, I think this is general for the entire healthcare system, that the doctor sees one thing as a problem for the patient, where the patient sees something completely different as a problem for the patient” – Physician K.
Challenges related to MDT
Some of the major challenges to successful cross-sectorial collaboration and fruitful MDTs were rooted in the siloed systems in healthcare. Organizational challenges such as IT-systems lacking features for smooth information sharing between departments and complex and disease/department-specific booking systems were considered major barriers to successful collaboration. A disease-specific approach, in which care is focused on single diseases, was also identified as ill-suited for people with MLTCs, and several physicians called for a culture change among clinical workers towards a more patient-centered approach: “The system is not at all geared to work across departments and sectors. Our medical health record systems are silo-based. Our booking systems are silo-based. Our registration systems are silo-based, so you can say, there is something structural that prevents you from being able to work across departments” – Physician H.
The lack of transferability from the MDTs to the outside system or the general healthcare system was experienced as a challenge in implementing some of the abovementioned benefits of MDTs: “I actually experience that something that is decided at MDT when that has to go into the normal system. Well, then it becomes much more difficult to implement. It may well be that we agree in that room about what needs to happen. But that's not what the system is normally geared for... so it becomes a bit of a small oasis in a huge system” – Physician H.
The resources associated with MDTs such as the time allocated to preparation, the MDT conference, and follow-up were considered a downside by almost all of the physicians. Moreover, many physicians mentioned that the number of participants in the MDTs was often too high, and some physicians even believed that it resulted in misuse of time for some of their colleagues if they just had to sit there and state that ‘everything is normal’ in a healthcare system where time is a scarce resource: “It's a big setup that we're running now, and I’m not sure that It's so sustainable in terms of how to.. that is, by gathering so many people in one room to go through relatively few patients” – Physician E.
Prerequisites for successful MDT
The outline and composition of the MDTs such as number of participants, frequency of meetings, and participating medical specialties were considered important by most physicians. However, there was some disagreement on this topic. Some physicians believed the ability to assemble the MDT based on the challenges of the patient was the optimal solution whereas others prioritized the regular teams with well-known faces: “(…) run the concept as it is, and then with access to put the MDT conference together based on what kind of problems the patient has” – Physician H. “Because it is precisely the fact that we get together that also makes us stay in our group. In other words, that the group exists has some synergy effect in relation to our collaboration, so if it is triggered ad hoc, then I think that the ownership of the MDT will be waived” – Physician E.
Elements to consider were how the MDTs can be anchored in clinical practice. Some physicians discussed the benefits of having the MDTs integrated into everyday practice for an easier adaptation, and as a means to expand MDTs to other specialties and colleagues: “I think that there needs to be a greater focus from the hospitals, at least from the university hospitals, and a greater dialogue in the executive board, as to how we get this rooted in everyday life” – Physician I.
Another important prerequisite for successful MDTs and cross-sectorial collaboration in general is the involvement of GPs/primary care. GPs were considered an essential element in both current and future MDTs as part of improving coordination and communication across sectors by all physicians. Many physicians considered GPs as the main coordinators and stated that they are used to look at patients in a holistic frame opposite to what is done at the hospitals. Some physicians meant that GPs were the most central actors in MDTs, and ideally, all patients in MDTs should be referred from general practice. “I think that MDT has no actuality or relevance if GPs are not involved, because it is from us that the patients must come” – Physician A.
Some physicians believed that keeping the patients in the primary sector was a major priority because the GPs are the ones who know the patients and their preferences. This aligns well with some of the expressions above considering the GP as the central actor who then refers to the specialists: “I think that's basically a good idea in terms of keeping patients out in general practice, because that is the real exercise... that I would like to support to save the system, that we help where the patients are, with the GP who can take care of it, but with some specialist advice” – Physician C.
The need for MDTs and cross-sectorial collaboration
The demographic changes with an increasingly ageing population with MLTCs were pointed out as major reasons why MDTs and cross-sectorial work are necessary. As GPs are gatekeepers to the healthcare system the increasingly ageing population will require smoother collaboration with specialists and the secondary sector to reduce the burden: “There is no doubt that these patients with multi-organ diseases, which are going to take up a lot of space over the next years and decades, will actually require the GPs to be able to spar with a multidisciplinary team” – Physician I.
The growing number of people characterized by multimorbidity, polypharmacy, complex treatment trajectories, and a low socioeconomic status (SES) was mentioned by all physicians as reasons why there is a need for more MDTs prospectively. Many people with MLTCs were considered vulnerable and low on resources in terms of managing their own conditions which necessitates collaboration across departments and sectors to reduce care fragmentation and improve coordination: “And some of the patients are also some vulnerable patients… they listen a lot to what the doctors say, they don't really have an overview of partly what medicine they get, but also why they might get it, and they can be socially disadvantaged or resource-poor” – Physician J.
Discussion
This study explored the perceived benefits and barriers towards MDTs and cross-sectorial work among physicians in the management of diabetes and comorbidities. We found a high level of convergence between the perceived perspectives of the physicians suggesting that there is shared agreement on many of the benefits and challenges related to MDTs as well as the need for MDTs and the potential of the intervention to overcome some of the challenges in care for people with MLTCs.
The main benefits included the improved professional learning and relational aspects that were strengthened. Working in MDTs and cross-sectorial was perceived to improve the leverage of capacity such as reducing the number of contacts/visits for patients through better coordination and communication. The simplification of patient pathways was highlighted as well as the involvement of patients and their preferences that MDTs enabled. The main barriers toward MDTs and cross-sectorial work were disease-specific organization with a correspondingly disease-specific culture towards care delivery which hamper effective coordination and communication both within and across primary and secondary care. Many physicians experienced difficulties when transferring decisions made in the MDTs to the outside healthcare system due to certain cultural and organizational shifts. MDTs were perceived as resource demanding in terms of time allocated to preparation, the MDT itself, and follow-up tasks as well as financial considerations. Time is, arguably, the scarcest resource in the healthcare system, so taking away time that could be spent on treating other patients was seen as a barrier for many physicians. Discussions on the importance of the outline and composition of the MDTs, and the role GPs/primary care should take in the MDTs were considered essential prerequisites for a successful MDT prospectively. Finally, the need for working in MDTs and across primary and secondary care were highlighted based on the increasing number of people with multimorbidity, polypharmacy, and complex patient pathways.
Comparison with existing literature
To the best of our knowledge, the number of studies that have explored the perspectives of physicians or HCPs on the management of people with multimorbidity is limited.17,23,30 Also, in the context of diabetes and comorbidities, there has been limited research exploring physicians and HCPs’ perspectives on management. Previous studies have either only included people with type 2 diabetes and no comorbidities,22,23,31 only explored the patients’ perspectives,31–33 or focused broadly on multimorbidity.17,30,34
Overarchingly, the findings of the present study are in line with many of the above-mentioned studies. It also reveals a consistent alignment between the findings of the present study and the dimensions of integrated care as outlined in the Rainbow Model by Valentijn et al. 35 The perceived benefits and barriers identified among physicians resonate with various dimensions of integrated care, showcasing the relevance of the model in understanding and contextualizing the challenges and opportunities associated with MDTs and cross-sectoral work. For example, the identified benefits, such as improved professional learning, strengthened relational aspects, and enhanced patient pathways, correspond to the integrative functions of care delivery, professional integration, and functional integration as described in the Rainbow Model. 35 Similarly, the barriers related to disease-specific culture, resource demands, and coordination difficulties reflect the challenges associated with normative integration and system integration within the Rainbow Model framework. 35
In the present study it is described how both the patients and HCPs see the MDTs as a necessity to deliver optimal care as diabetes management with its comorbidities is too complex for one physician to manage.22,31 The need for different medical specialties to be present to create a holistic approach and embrace the challenges of different comorbidities was highlighted in our study. This finding is supported in different studies where the holistic approach and continuity of care from a regular team was emphasized to deal with complexity.17,23,33,36 In terms of delivery of care there was some disagreement between physicians in the present study concerning a regular team who knows each other versus a flexible ad hoc team. This exemplifies one of the many considerations regarding the outline of the most optimal MDT setup and might differ between physicians’ perspectives and between healthcare facilities.
As the burden of disease of the patient increases, the treatment burden will increase correspondingly setting higher standards for coordination and communication. 6 In Denmark, the healthcare system is traditionally characterized by a high degree of specialization with a high level of disease-specific focus. 22 As such, the culture within departments at the hospitals follows this way of working and thinking hampering multidisciplinary work and affecting working efficiently across primary and secondary care.20,22 Inadequate coordination and poor communication are often perceived as part of the fragmented care delivered across departments and sectors for people with MLTCs.17,30 This finding is highlighted in several studies where both HCPs and patients found this to be a major system-wide challenge.17,30,33,34,37 Capacity and resource constraints are commonly mentioned barriers to coordination and communication due to fragmented care. 17 This finding is backed up by the present study where coordination was experienced as hampered if collaborating specialties were far away from your own and available time was limited. In the present study, a major aspect of improving coordination and communication across primary and secondary care was the involvement of GPs as coordinators. Reviews by Sinnott et al. and Damarell et al. highlight the crucial role of GPs in managing multimorbidity. They emphasize the challenges of fragmented care caused by the involvement of various medical specialties, which leads to poor communication and lack of coordination between secondary and primary care.34,38 Despite these reservations, the GPs appreciated the input from specialists and the discussions of complex patients. Additionally, the need for a generalist view to support the specialist view was underlined. 34 Some of the mentioned benefits of working in MDTs and cross-sectorial were the improved interprofessional learning and relationships. This is supported by findings in Pati et al. where networking with seniors, peers, and specialists resulted in more confidence to manage the patients themselves. 21 Additionally, the relationships that are forged leads to improved coordination and more security in taking responsibility for treatment when complexity in management can be discussed with peers.17,22
Clinical implications
To address some of the challenges mentioned above, almost all physicians believed that more integrated care and MDTs with focus on multimorbidity instead of comorbidity is a necessity to deal with the increasing number of people with multimorbidity, polypharmacy, and complex patient pathways. The change of focus from the current disease-specific comorbidities to multimorbidity is deemed crucial to reconfigure healthcare to a more patient-centered and holistic system to embrace complexity in patients.36,38 Findings from the present study could be used to inform ongoing or future interventions aiming to address challenges related to the management of people with MLCTs. Previous studies have demonstrated a range of positive outcomes when HCPs are working in coordinated MDTs39–41 but evidence is still limited specifically on MDT interventions. From a clinical perspective, working in MDTs holds both benefits and barriers that needs to be addressed in future research to ensure optimal implementation with special emphasis on the most optimal outline and setup of these teams. Future research should further focus on how to develop and implement clinical guidelines specifically designed for people with MLTCs.
Strengths and limitations
The interviews in the current study were conducted online via Microsoft Teams. This approach increased flexibility and accessibility for both the interviewer and the participants. Accessibility was important due to the relatively significant geographical distance between the interviewer and several participants. However, the use of Microsoft Teams might have resulted in less nuanced interviews as it is plausible that physical face-to-face interviews had elicited more varied discussions and better capture of non-verbal communication. 42 A strength of the present study was the several steps taken to increase study validity. First, we developed a study protocol to increase transparency. Second, we adhered to the 15-step checklist of criteria for good thematic analysis. 29 Third, several authors were involved in the different elements of the study process from design of protocol, interview guide, field testing of the interview guide, and development of codes to validation of themes. Finally, we included a high number of sample quotes to increase confirmability.
A potential limitation might be the short duration of interviews. The median duration of interviews was 29 minutes which, arguably, can be considered a short amount of time to conduct an in-depth interview. However, since this was expert interviews on a specific field of interest, the time allocated to introduction of the different topics was shorter, thereby reducing overall duration. We included eleven physicians which is a relatively low number of participants that might reduce the transferability of findings to other settings. Despite the low number of participants, data saturation was reached which can be explained by the relatively specific area of interest and a high degree of information power in the sample. 43 Interviewing more physicians might have revealed other perceived experiences or different aspects than we report. Additionally, considering that MDTs constitute a rather specific field of interest, it is quite context-specific which might add to the lack of transferability. Moreover, several participants represented the same geographical area which might bias the perceived benefits and barriers towards MDTs based on the culture in that specific part of Denmark. By including participants from another region in Denmark, making it a double-center study, we aimed to minimize this bias. Finally, the purpose of an expert interview is to gain knowledge and experiences regarding a very specific field of interest. However, this study focused exclusively on physicians (who are the key actors in MDTs), which may limit the ability to fully capture the multifaceted nature of managing diabetes and comorbidities. Including other HCPs could have provided a more comprehensive understanding, as the management of these conditions is inherently complex and requires input from multiple disciplines.
Conclusion
In this study, the perceived benefits and barriers toward MDTs and cross-sectorial work were explored among physicians. Our findings indicate that there are several benefits in terms of improved leverage of capacity across departments and sectors, improved interdisciplinary learning and relationships, and optimized treatment for patients. Contrary, there are some barriers to successful MDTs in siloed healthcare systems and the fact that MDTs are rather resource demanding. Prerequisites for a successful MDT concern the outline and composition of the MDTs, and the role of GPs/primary care. MDTs and cross-sectorial work are needed in future healthcare systems and are considered to hold potential as an intervention to embrace some of the challenges encountered by people with diabetes and comorbidities.
Footnotes
Acknowledgements
We thank all the participants who agreed to participate and share their perspectives and experiences to enable this study.
Statements and declarations
Funding
This research was funded by the Novo Nordisk Foundation as part of the Programme for Co-morbidities to Diabetes – Multidisciplinary Team Conferences launched across the five Steno Diabetes Centers in Denmark.
Conflicting interests
Some of the interviewed participants in this study was associated with the research and work related to the Programme for Co-Morbidities to Diabetes – Multidisciplinary Team Conferences. The research, part of two PhD studies, carried out by authors JDA and SJB originates from this programme as well.
Data availability statement
Data can be made available from corresponding author upon reasonable request.