
Abstract
Background
Multimorbidity estimates are expected to increase in India primarily due to the population aging. However, there is a lack of research estimating the burden of multimorbidity in the Indian context using a validated tool. We estimated the prevalence and determinants of multimorbidity amongst the adult population of the rural Uddanam region, Andhra Pradesh.
Methods
This community-based cross-sectional study was conducted as a part of an ongoing research program. Multistage cluster sampling technique was used to select 2419 adult participants from 40 clusters. Multimorbidity was assessed using Multimorbidity Assessment Questionnaire for Primary Care (MAQ-PC) tool, collecting information on 13 chronic diseases. Patient Health Questionnaire (PHQ-12) was used to screen for depression. Multiple logistic regression was conducted to identify the strongest determinants of multimorbidity.
Results
Of the 2419 participants, 2289 completed the MAQ-PC tool. Mean age (standard deviation) of participants was 48.1 (13.1) years. The overall prevalence of multimorbidity was 58.5% (95% CI 56.5-60.6); with 30.7%, 15.6%, and 12.2% reporting two, three, and four chronic conditions, respectively. Acid peptic disease-musculoskeletal disease (44%) and acid peptic disease-musculoskeletal disease-hypertension (14.9%) were the most common dyad and triad. Among metabolic diseases, diabetes-hypertension (28.3%) and diabetes-hypertension-chronic kidney disease (7.6%) were the most common dyad and triad, respectively. Advancing age, female gender, and being obese were the strongest determinates of the presence of multimorbidity. Depression was highly prevalent among the study population, and participants with higher PHQ-12 score had 3.7 (2.5-5.4) greater odds of having multimorbidity.
Conclusions
Our findings suggest that six of 10 adults in rural India are affected with multimorbidity. We report a higher prevalence of multimorbidity as compared with other studies conducted in India. We also identified vulnerable groups which would guide policy makers in developing holistic care packages for individuals with multimorbidity.
Keywords
Background
Multimorbidity, defined as the presence of two or more chronic diseases, is increasing globally.1,2 According to a systematic review of 39 studies, the pooled prevalence of multimorbidity was 36.4% (95% CI: 32.2- 40.6) in low and middle-income countries (LMICs) and 42.4% (95% CI: 38.9-46.0) among high-income countries. 3 Multimorbidity is a complex construct and goes beyond measuring counts of co-existing diseases to ascertaining weighted counts of diseases, measuring various body systems affected (complex multimorbidity), ascertaining the presence of concordant or discordant diseases, and determining clusters of physical and mental health disorders and chronic infectious diseases.1,4 Multimorbidity poses several challenges for the affected patients, such as declining functional status, impaired quality of life, need for multiple healthcare visits, and polypharmacy leading to economic burden, resulting in an overburdened health system.5–11
In LMICs, such as India, understanding the patterns of multimorbidity is essential, as it has implications for developing multimodal strategies that when implemented, would improve disease management.2,12 Of the studies available from India, the prevalence of multimorbidity has ranged from 18% to 83%.13–22 The wide gap in prevalence is due to inconsistencies in defining multimorbidity, different permutations of included morbidities, or an overestimation of prevalence due to the inclusion of self-reported morbidities. Most studies have focused on the elderly population,15–18 were conducted in health facilities,19,20 studied urban populations, 21 or explored multimorbidity amongst patients with non-communicable diseases.15,22 Few studies have explored the prevalence and correlation of multimorbidity amongst the rural population.13,22
We established a general population-based cohort in the Uddanam region of Srikakulam district in rural Andhra Pradesh, primarily to study chronic kidney disease (CKD). 23 Uddanam region is a rural area where the main occupation is farming and coconut and cashew harvesting. We surveyed this population to determine the prevalence of multimorbidity and its determinants, and the results are presented here.
Methodology
Study design and participants
The study was conducted as a part of an ongoing research program - Study to Test and Operationalize Preventive Approaches for Chronic Kidney Disease of Undetermined Etiology (STOP CKDu) - in the Uddanam region of Srikakulam District of Andhra Pradesh, the details of which are published elsewhere. 24 Briefly, the study, focusing on ascertaining the prevalence and incidence of CKD in this area, is being conducted among the seven administrative regions (mandals). A total of 2419 subjects were recruited using a cluster sampling technique from 40 clusters (villages) in the defined area. The sample size was estimated assuming a prevalence of CKD of 10% in the low-prevalence clusters, a relative precision of 20%, a design effect of 2, and inflated to account for an estimated 25% loss to follow-up in the prospective component of the study. The cohort was set up in July 2018 to ascertain the incidence and progression factors of CKD in this region. All participants who were alive and still living in the region were approached between Nov 2021 and Feb 2022 to ascertain the patterns of multimorbidity and depression.
Data collection and study variables
Data was collected using a structured multimorbidity assessment tool. The questionnaire entails the assessment of self-reported (informed by the healthcare professional to participant) multimorbidity in which respondents reacted to a list of common chronic conditions. The development and validation of the tool and its components are published elsewhere. 25 For data collection we approached the selected participants at their homes. If, after two consecutive attempts, the participant was unavailable, we contacted them telephonically.
Each morbidity was categorised as present or absent, and summed up to get a cumulative score which was used to create dichotomized multimorbidity variable. Highly prevalent morbidities (prevalence > 5%) were further studied to find the most common dyads and triads. Further, we also constructed dyads and triads of cardio-metabolic morbidities (hypertension, diabetes, ischemic heart disease, heart failure, stroke, CKD). There were no missing variables.
Age, gender, education (no formal education, school education, college), and occupation (unemployed, sedentary work, manual worker/farmer) were also captured. Socio-economic status was calculated using a modified Kuppuswamy scale. 26 Data on current or past tobacco or alcohol consumption, anthropometric variables (height and weight), and blood pressure were determined for all recruited participants. Blood pressure was measured using an Omron Blood pressure monitor of model number (HEM-7121J-IN), three readings were recorded at five minutes intervals, and the average of three values was calculated.
Depression was measured using Patient Health Questionnaire (PHQ-12), a 12-item self-reported questionnaire. The response categories were further dichotomised as yes and no, such that the patient would be asked whether they felt each of the twelve symptoms and their frequency during the last two weeks. Depression was defined as a PHQ-12 score of above 4.
Data management and Statistical Analysis Plan
Data were entered in Microsoft Excel 2013 (v 15.0). Data cleaning and analysis were performed in STATA version 16. Frequencies and proportions were used as descriptive measures for categorical variables, with 95% confidence limits and mean with standard deviation for continuous variables. Bivariate analysis was done using Chi-square test. Logistic regression analyses were performed to estimate odds ratios (ORs) of factors associated with multi-morbidity. To conduct univariate and multivariate analysis, education (no formal education/any formal education), occupation (outdoor work/others including unemployed and sedentary workers), family income (monthly family income <INR 10,000/>INR 10,000) and socio-economic status (lower/middle including lower middle and upper middle SES) were recategorized as categorical variables. We present both un-adjusted and adjusted for age, gender, education, occupation, family income, socioeconomic status, tobacco, alcohol use, and Asia-specific body mass index categories 27 in the multivariate model.
Ethical statement
The study was approved by the institutional ethics committee of The George Institute India (#001/2017), and written informed consent was obtained from every participaticipant.
Results
The original cohort consisted of 2419 individuals, of which 2289 were eligible to be included in the study, giving a response rate of 94.6%. A total of 126 members of the original cohort had died, two participants had permanently emigrated, and two declined to participant in this study. Face to face interview were conducted for 2160 participants and the remainder (n=126) were contacted telephonically as they were unavailable at their home.
Characteristics of study participants.

aOne participant was bedridden
Prevalence of individual chronic conditions and multimorbidity
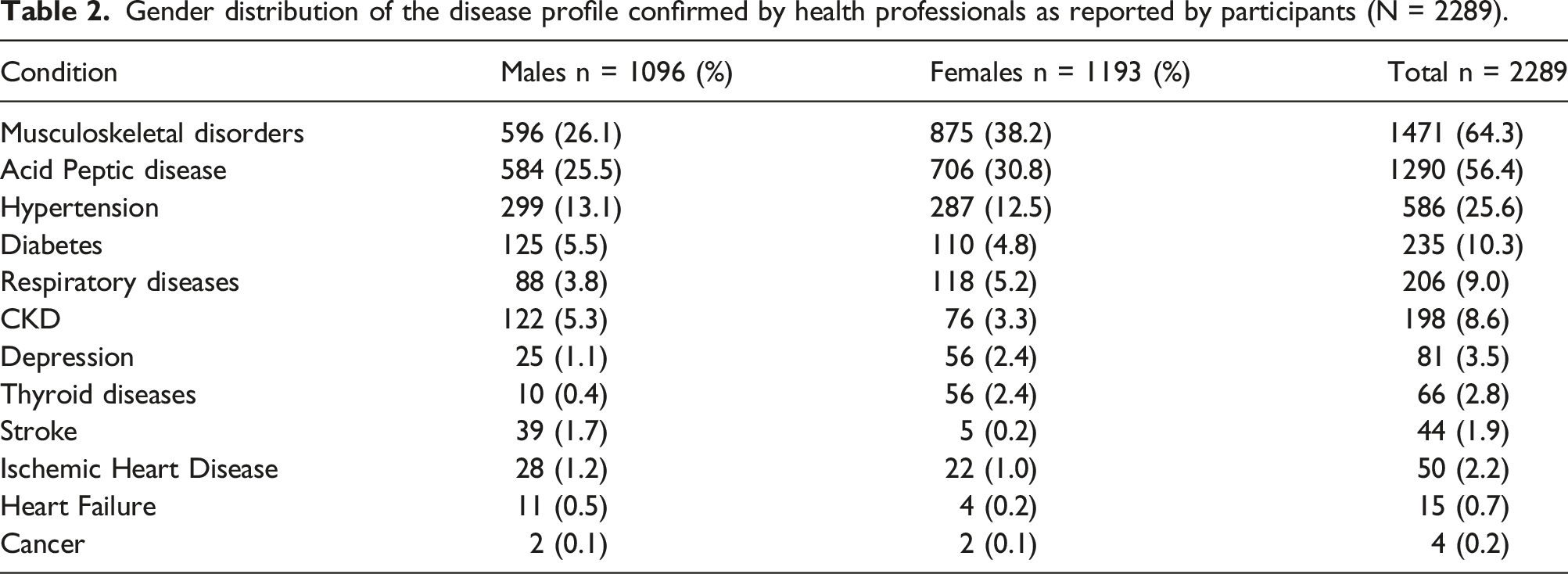
The number of health conditions per individual ranged from none to eight [Figure 1.] Of those reporting a chronic health condition, a majority (58.5%, 95% confidence interval [CI] 56.5-60.6) had more than one morbidity. Overall, the prevalence of a single chronic condition was 21.8% (95% CI 20.2-23.6). Dyads were more common (702, 30.7%) than triads (356, 15.6%), and a total of 282 (12.2%) had four or more conditions. A comparable proportion of males and females were affected with chronic conditions; however, a higher proportion of males were affected by stroke (Table 2 and supplementary table 1). At the time of data collection, 117, 5.1%, had been diagnosed with COVID (not included in multimorbidity counts). Proportion of participants with and without multimorbidity conditions among study population (n = 2289). Gender distribution of the disease profile confirmed by health professionals as reported by participants (N = 2289).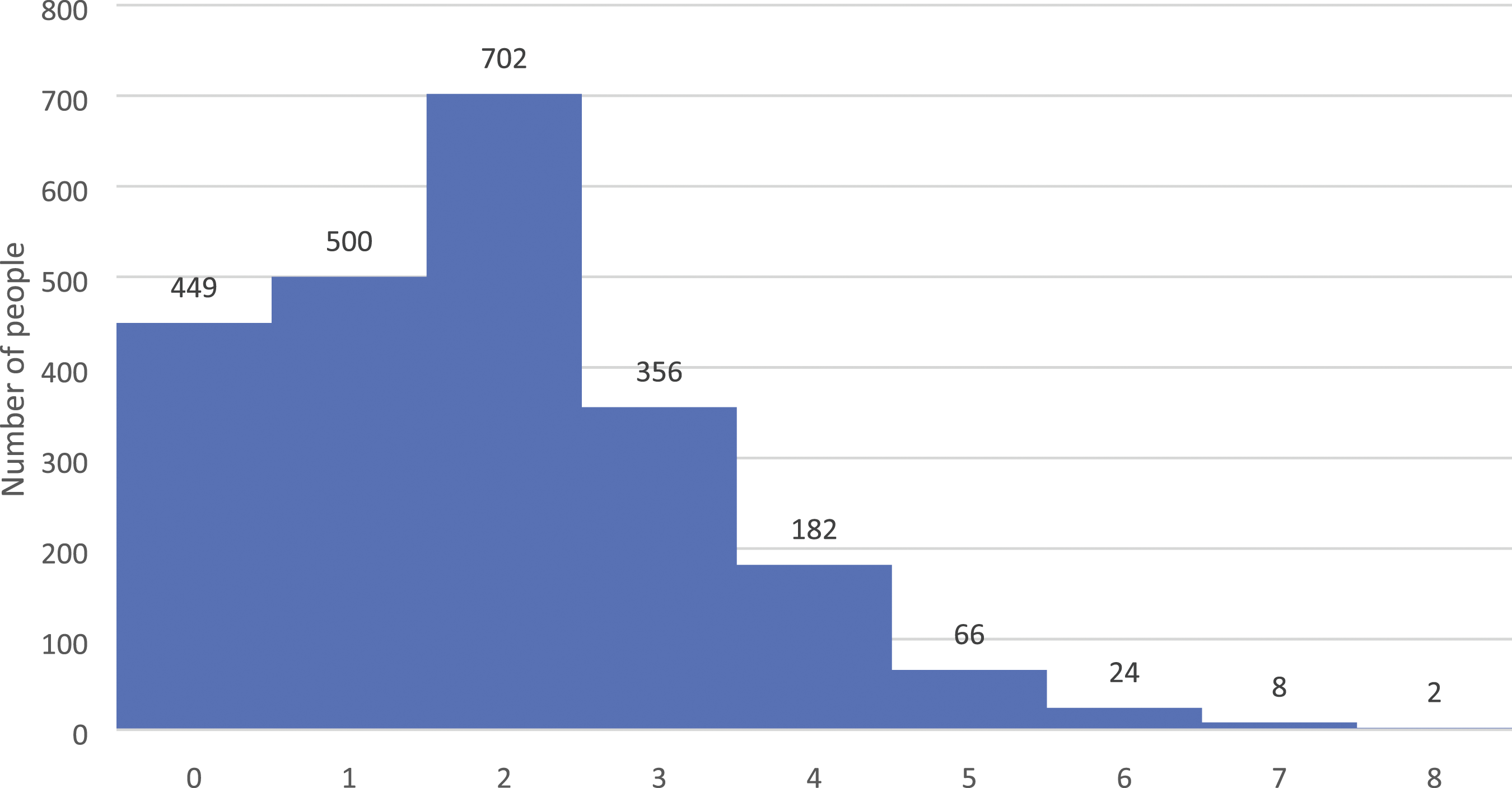
Patterns of multimorbidity
The combination of acid peptic ulcer disease (APD) and musculoskeletal disorders (MSD) was the most prevalent dyad (1005,44%), followed by acid peptic ulcer diseases and hypertension (HTN) (441, 19.3%), and musculoskeletal disorders and hypertension (426, 18.6%) [Figure 2a.]. Of the triads of multimorbidity, acid-peptic ulcer diseases (APD)-musculoskeletal disorders (MSD)-hypertension (HTN) ranked highest with 340 (14.9%) affected participants, followed by acid peptic diseases-hypertension-diabetes (199, 8.7%), and acid peptic diseases-musculoskeletal disorders-respiratory disorders (149, 6.9%) [Figure 2b.] (a): Tree map depicting burden of morbidity combinations among common dyads. (b): Tree map depicting burden of morbidity combinations among common triads.
On examining the cardiometabolic multimorbidity, diabetes-hypertension was the most prevalent (148,28.3%) dyad, followed by hypertension-chronic kidney disease (120, 22.9%) and diabetes-chronic kidney diseases (44,8.4%). Of the total study population having triads of metabolic multimorbidity, diabetes-hypertension-chronic kidney diseases ranked highest with 34 (7.6%) affected participants, followed by diabetes-hypertension-ischemic heart diseases (15,3.3%), and diabetes-hypertension-stroke (15,3.3%) [supplementary table 2].
Age and multimorbidity
The prevalence of multimorbidity increased with advancing age [Figure 3.]. Amongst individuals between the ages of 18 and 30 years, only 29 (2.0%) of the population were found to have multimorbidity, which increased to 411 (28.5%) in those 40 - 50 years old. Age wise distribution of the morbidities among study cohort.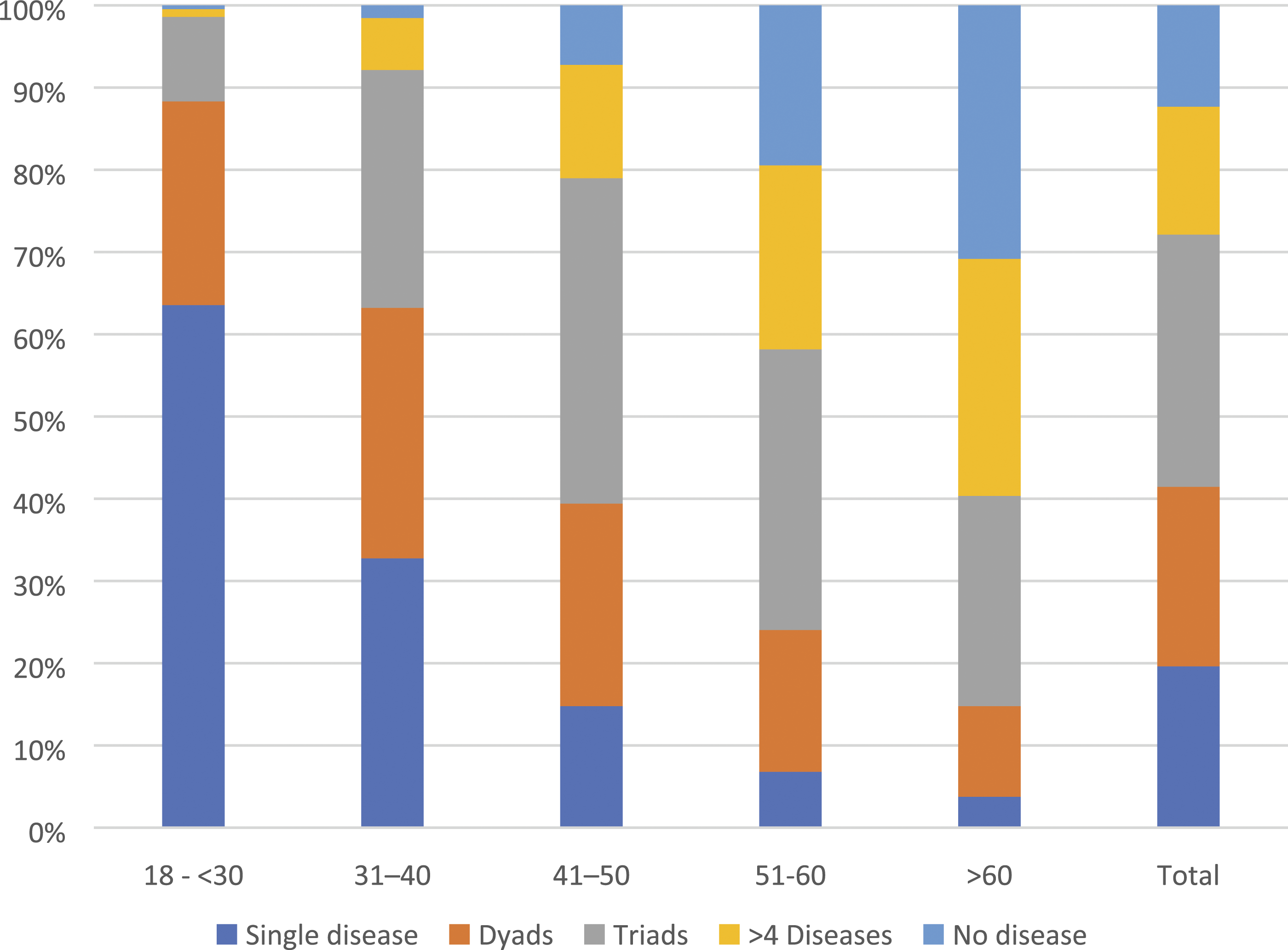
Depression
Distribution of symptoms of depression in the study population.

Figures in parentheses are percentages.
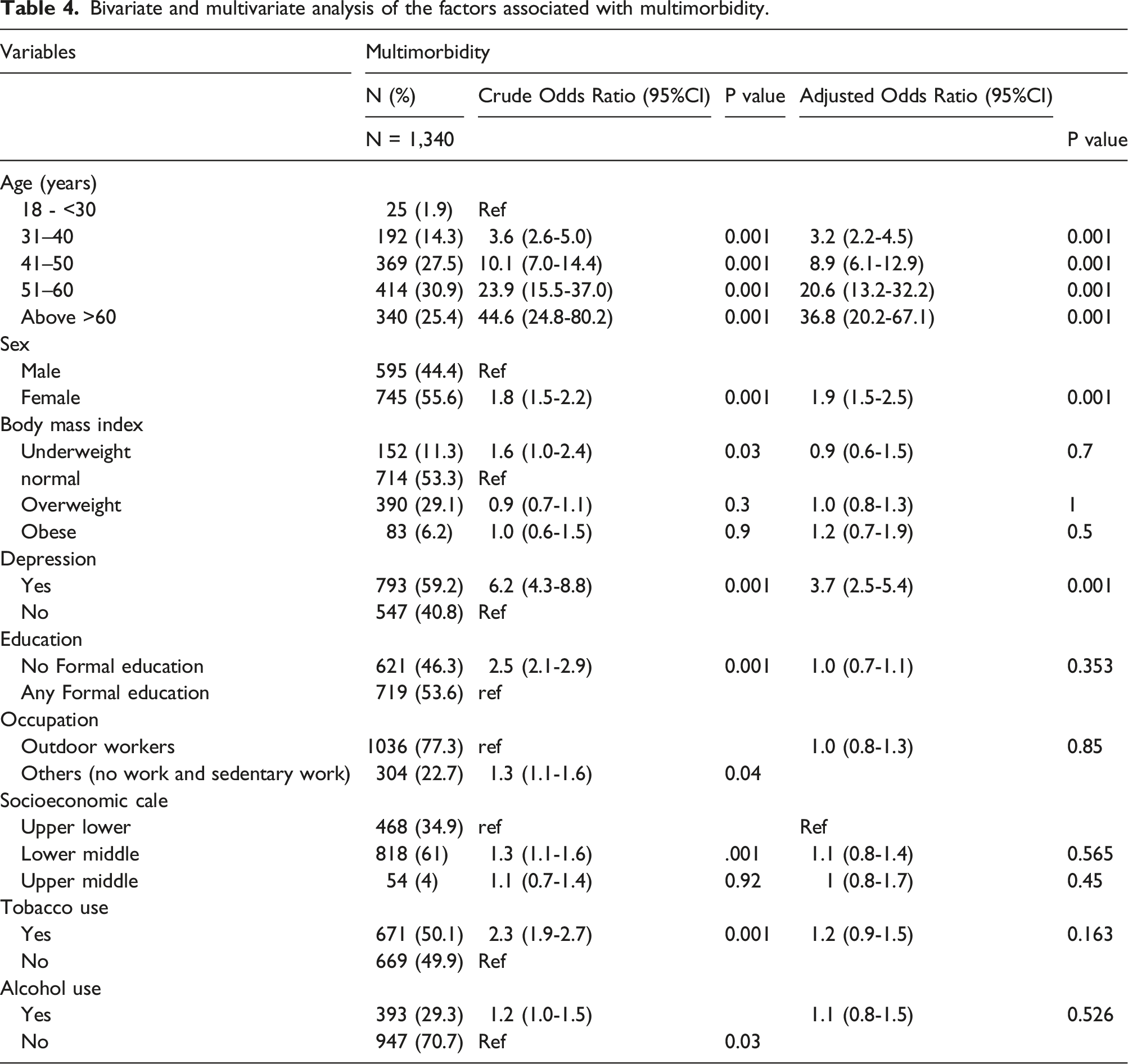
Factors associated with multimorbidity
Bivariate and multivariate analysis of the factors associated with multimorbidity.
Discussion
In this first of a kind study that examined the prevalence and patterns of multimorbidity among the Indian rural agricultural population, we found that six out of ten adults are affected by multimorbidity, with over 80% of the adult population reporting one chronic condition for which they had sought medical care. Age, female gender, and being obese were the strongest determinants of the presence of multimorbidity. Depression was also common, more so in the population with multimorbidity. Further, most of the common metabolic disorders were evenly distributed among both genders, except stroke (3.5% in males and 0.4% in females) and heart failure (1.0% in males and 0.3% in females). On the other hand, the females showed a higher proportion of suicide ideation compared to males (21.1% v 31.3%).
There are few studies on the burden of multimorbidity in India, especially in rural communities. The prevalence of multimorbidity in the population we studied was higher than those reported from rural populations with similar age profiles (39% to 55%).20,28,29 A nationally representative study (Longitudinal Aging Study from India) reported a multimorbidity prevalence of 24.1% amongst those above the age of 60 years. 18 Similar estimates of multimorbidity have been reported from LMICs such as Ghana 30 and Brazil. 31 Together, these findings highlight the growing burden of multimorbidity, which is no longer limited to wealthier countries and affluent segments of society.
Studies limited to selected population groups such as patients recruited from healthcare setting, or elderly population, report higher prevalence. Soji et al estimated the prevalence of multimorbidity to be 74% among patients with diabetes in Kerala. 22 Khan et al determined that 83% of the older adults (age 60 years and above) in Punjab had multimorbidity. 17 Similarly, in China, Wang et al. reported that 90.5% of the rural elderly population has multimorbidity. 32 Aging and the presence of chronic conditions are shown to increase the occurrence of multimorbidity.33–36
An important source of variation that influences the prevalence of multimorbidity is inconsistencies in the definition of variables and the lists of chronic conditions. To overcome these challenges and assess multimorbidity comprehensively, we used the MAQ-PC tool, which is validated for Indian settings and has been shown to have high internal reliability measures. 25 Further, we used a standardised operational definition of multimorbidity from the list of the 13 most common chronic conditions and studied a wider age group.
Acid-peptic disease and musculoskeletal disorders were most frequently associated together and in combination with other chronic disease conditions. Acid peptic disease is a commonly used term that collectively includes digestive system disorders with common symptomology, such as gastro-oesophageal reflux disease (GERD), peptic ulcer disease, gastritis, and duodenitis. Clusters of multimorbidity with acid peptic diseases have been reported by Pati et al, 37 Dutta et al, 38 and Kshartri et al. 39 The high prevalence of APD possibly attributed to the lifestyle and dietary preferences of the rural agricultural population (predominantly rice-based diet, consumption of caffeinated drinks, and/or tobacco use).40,41 Furthermore, APD can often develop or worsen as a side effect of commonly used drugs, such as non-steroidal anti-inflammatory drugs (available over the counter and used rampantly as pain killers), calcium channel blockers, beta-blockers, routinely prescribed for musculoskeletal disorders and hypertension.42,43
As expected, diabetes and hypertension were the most common dyads among metabolic disorders in both males and females. Notable was the high prevalence (17.3%) of CKD in this population, which ranked second and third highest in combination with hypertension and diabetes, respectively. Triads of diabetes, hypertension and chronic kidney diseases were the most prevalent. This finding is unique to the current cohort.
Understanding multimorbidity patterns is crucial for developing successful policies tailored to the local context in a way that efficiently utilises available resources to develop disease and population-specific approaches. Interventions can be made efficient when they target the most common multimorbidity clusters. Currently, the Indian national program for non-communicable diseases primarily focuses on diabetes and hypertension, 44 however, musculoskeletal conditions, gastrointestinal disorders, respiratory diseases, and CKD management are yet to be incorporated as priorities.
Consistent with other studies, we also found an age gradient for multimorbidity. Various authors have documented the compounding of multimorbidity with advancing age, with the burden rising after the age of 45 years.1,20,33–35,45,46 The long-standing accumulation of risk factors due to environmental exposure, sedentary lifestyle, poor dietary or behavioural practices, and gradual functional and physiological decline make the aging population susceptible to a constellation of morbidities.47,48
Females had a higher prevalence of multimorbidity. This gender disparity can be due to higher exposure to risk factors like poor nutrition, physical inactivity, 49 and socio-cultural barriers which impede their access to healthcare. 50 It has been suggested that females are more likely to report morbidities while self-reporting. 51 These finding suggest the need to develop better tools to understand the determinants and age and gender-specific interventions for managing complex multimorbidity. There were other differences between the two sexes – for example, the higher prevalence of stroke and heart failure in males and suicidal ideation in females. Apart from biological reasons, possible causes for this could include differences in lifestyle, health seeking behaviour, and/or medication adherence.
Our study also shows a high prevalence of depression, with nearly one-fourth of the population having suicidal thoughts. Gender disparity with a female preponderance of suicidal behaviour can be attributed to a higher prevalence of mental health disorders (such as depression), psychological distress (due to domestic violence), social constraints (lack of financial independence), or poor emphasis on suicide prevention among them. Patients with multimorbidity have a higher risk of depression than those with no disease or single morbidity.52,53 Depression and multimorbidity are complex phenomena and show bidirectionality. Multimorbidity and depression both present an economic burden on the patients. 54 Early identification and timely management of depression among patients with multimorbidity is necessary to improve health outcomes and quality of life.
The principal strength of our work is that we conducted a population-based multimorbidity survey in an area identified to be at high risk of developing one chronic condition (CKD). We used a validated tool for the rural Indian population to assess the pattern and burden of multimorbidity. Our operational definition of multimorbidity was based on the definition from the Academy of Medical Sciences. 1 We collected information on conditions that were important to patients and relied on confirmation of the diagnosis via medical and treatment records.
A few limitations also need to be recognised. Firstly, due to the cross-sectional design, no causal inference can be established as the time of onset of diseases could not be explored. Secondly, our study was not powered to accurately estimate the prevalence and/or subgroup differences of each chronic condition, so the findings should be confirmed in larger studies. Thirdly, since the prevalence of depression was high, reporting bias may be present; however, attempts were made to verify self-reported data whenever possible. Finally, we measured morbidities based on self-reporting of confirmation from a doctor, which is influenced by health seeking behaviour and likely leads to underestimation of multimorbidity burden.
Conclusions
The burden of multimorbidity is high in the rural population of the Uddanam region, which has policy implications. Understanding the burden of multimorbidity will guide policymakers to develop a robust healthcare system that explores potentially causal associations among multiple coexisting conditions and targets the constellation rather than singleton diseases. Identification of risk factors suggests the need to develop targeted approaches for high-risk groups.
Supplemental Material
Supplemental Material - Patterns of multimorbidity among a community-based cohort in rural India
Supplemental Material for Patterns of multimorbidity among a community-based cohort in rural India by Balaji Gummidi, Vaishali Gautam, Oommen John, Arpita Gosh and Vivekanand Jha in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
We thank the participants for their patience while conducting the study. We also acknowledge the support from Government of Andhra Pradesh
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Government of Andhra Pradesh (GoAP) (grant no. 38248/CKD/NCD/2017).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.