
Abstract
Background
Multimorbidity is associated with increased mortality. Certain combinations of diseases are known to be more lethal than others, but the limited knowledge of how the chronology in which diseases develop impacts mortality may impair the development of effective clinical interventions for patients with multimorbidity.
Objective
To explore if in multimorbidity the chronology of disease onset is associated with mortality. Design: A prospective nationwide cohort study, including 3,986,209 people aged ≥18 years on 1 January 2000, was performed. We included ten diagnosis groups: lung, musculoskeletal, endocrine, mental, cancer, neurological, gastrointestinal, cardiovascular, kidney, and sensory organs. We defined multimorbidity as the presence of at least two diagnoses from two diagnosis groups (out of ten). To determine mortality, logistic regression models were used to calculate odds ratios (OR) and ratio of ORs (RORs).
Results
For most combinations of multimorbidity, the chronology of disease onset does not change mortality. However, when multimorbidity included mental health diagnoses, mortality was in general higher if the mental health diagnosis appeared first. If multimorbidity included heart and sensory diagnoses, mortality was higher if these developed second. For the majority of multimorbidity combinations, there was excess mortality if multimorbidity was diagnosed simultaneously, rather than consecutively, for example, heart and kidney (3.58 ROR; CI 2.39–5.36), or mental health and musculoskeletal diagnoses (2.38 ROR; CI 1.70–3.32).
Conclusions
Overall, in multimorbidity, the chronology in which diseases develop is not associated with mortality, with few exceptions. For almost all combinations of multimorbidity, diagnoses act synergistically in relation to mortality if diagnosed simultaneously.
Introduction
The prevalence of multimorbidity, defined as the co-occurrence of at least two chronic conditions in one person, 1 is increasing.2,3 In general practice, about one-third of patients have ≥4 chronic conditions, and many patients develop chronic conditions over the course of life. 4 The dynamics of multimorbidity mean that its prevalence increases with age,5–8 but at the same time, most people with multimorbidity are actually below 65 years of age. 9 It has long been established that multimorbidity confers an increased mortality risk,7,10,11 and that life expectancy decreases with the number of chronic conditions. 12 Accordingly, we earlier found a dose–response relationship between the number of chronic conditions and mortality. 7
The association between multimorbidity and mortality is more heterogeneous than the above broad characterization implies. Earlier, we showed that certain multimorbidity combinations conferred particularly high mortality. 7 However, some of these particularly detrimental combinations appear to differ between men and women, and are probably modified by various other factors.7,13 The development of multimorbidity may follow myriad trajectories in which some people stay free of chronic conditions until late in life, while others develop numerous conditions at a higher speed,14,15 for example, centenarians have a slower pace of developing multimorbidity than non-centenarians. 16 Furthermore, the unique trajectories have different implications, for example, a person with a mental health diagnosis that years later develops a lung disease due to smoking compared to a person that develops a mental health condition in the aftermath of heart disease. Both scenarios are central for the care delivered in general practice and contain both ongoing preventive work and also work into understanding of the nature and complications that can evolve because of new diseases. The need for understanding the implications of the development of multimorbidity in a life course perspective has been emphasized.10,17 Still, there is not much investigation into the temporal order in which the onset of diseases becomes multimorbidity and its consequences for mortality.
To improve health care for people with multimorbidity, interventions have to focus on areas of certain needs. By gaining knowledge about the association between disease chronology and mortality in multimorbidity, interventions not only can be targeted at combinations of certain diseases but also improve the timing of preventive measures.
Objective
This study has two objectives: 1. To explore if mortality differs among multimorbidity combinations with a different chronology. 2. To estimate the excess mortality from having multimorbidity (i.e., the joint effect of two conditions compared to the effect of the conditions individually) with different chronology.
Material and methods
Study design and population
The study included the entire Danish adult population (aged ≥18 years) on 1 January 2000 (baseline). The cohort was previously created
7
and extracted from the Danish Civil Registration System (CRS)
18
and was prospectively followed for 15 years until 31 December 2014 (Figure 1). At baseline, background characteristics age, sex, socioeconomic status (family income, highest completed education, work status, and assets), degree of urbanization, and cohabitation status were identified. To estimate the level of multimorbidity at baseline, information on all diagnoses leading to either inpatient or outpatient care contacts was obtained from the Danish National Patient Register (NPR) in the ten years before baseline (1 January 1990 until 31 December 1999). If patients migrated or were lost to follow-up during this period, they were excluded (Figure 1). Fifteen-year all-cause mortality was our outcome. Also emigration and loss to follow-up in the 15 years after baseline led to exclusion. The population through study.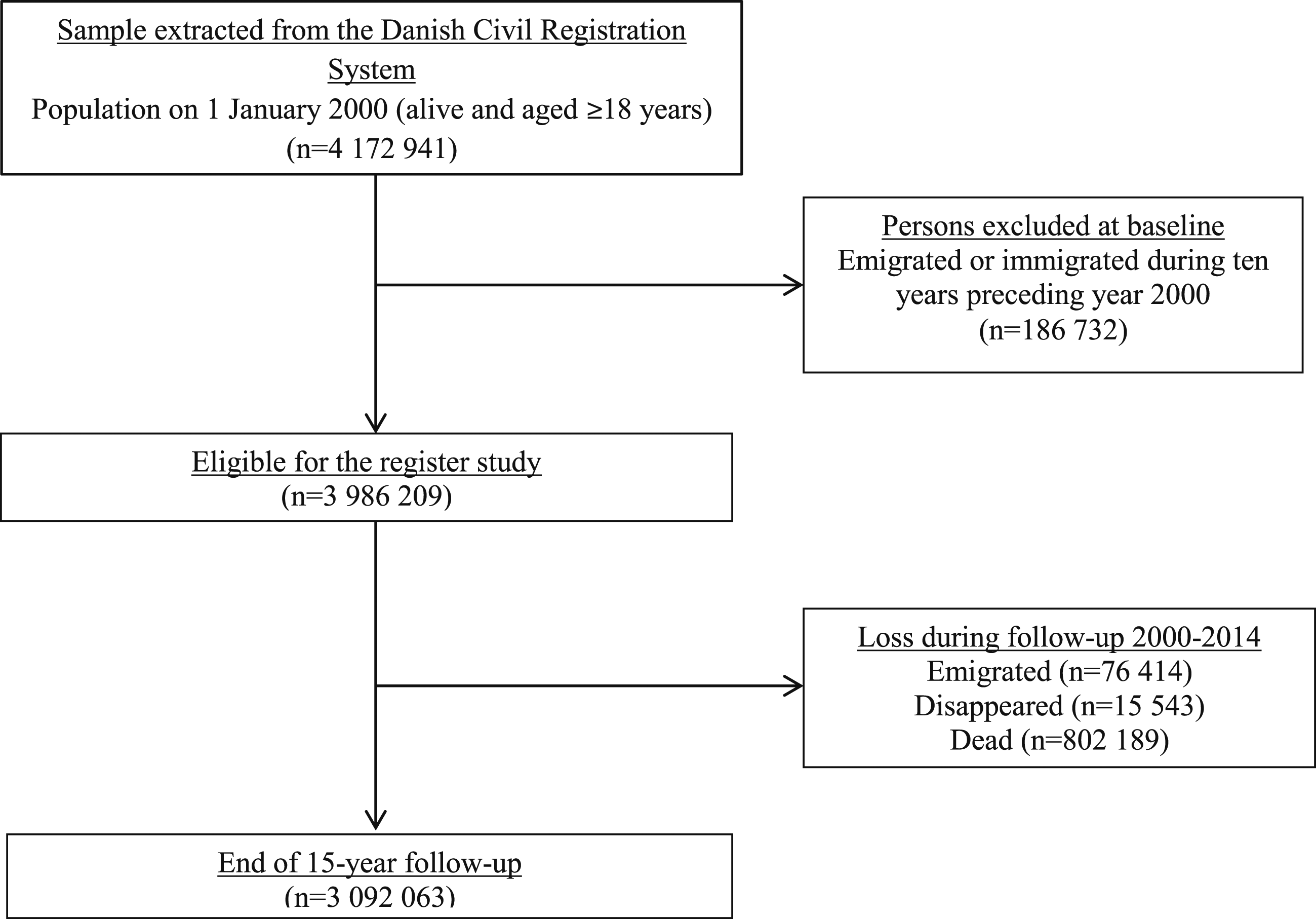
Nationwide registries
All (live) born children, as well as new residents in Denmark, receive a unique personal identification number, which is stored in CRS. 18 The identification number makes it possible to link personal information from all Danish registries. The administrative purposes of CRS ground weekly updates and continuous corrections of errors. Because Danish law requires registration in CRS, the information is assumed to be of high quality. Information on vital status, emigration, family connections is provided by CRS. 18 The NPR, 19 the Danish Cancer Registry (CR), 20 and the Danish Psychiatric Central Research Register (PCRR) 21 provided the study with information about diagnoses. Outpatient care and emergency admissions, however, were first included in 1995. In NPR, the diagnostic information is coded as International Classification of Diseases, 10th edition (ICD-10), and until 1994, the earlier version 8th edition (ICD-8). 22 All incident cancers in Denmark, since 1943, are included in CR, and since 1978, they are coded as ICD-10 codes. 20 In PCRR, all patients having mental health diseases and in need of secondary health care at public hospitals are registered with ICD codes. 21 To be included with diagnoses from CR and PCRR, only information on whether a patient appears in the register, in the ten-year period before baseline, was required. Information on socioeconomic status, that is, income, 23 education, 24 work status, 25 and assets, 23 was retrieved from Statistics Denmark’s registers. Since the study used anonymized administrative register data, neither approval from the Ethics Committee nor informed consent from the study participants was required. The Danish Data Protection Agency, The Danish Health Data Authority, and Statistics Denmark approved the study.
Definition of multimorbidity
Multimorbidity in this study is based on ten groups of diagnoses: lung, musculoskeletal, endocrine, mental health, cancer, neurological, gastrointestinal, cardiovascular, genitourinary, and sensory organs. Each group contains several diagnoses that to some level share treatments, clinical picture, or organization of health care (Supplementary File 1), for example, the lung diagnosis group contains chronic obstructive pulmonary disease (COPD) (found in the Danish national health registers as ICD-10 code J44 or ICD-8 code 490), chronic bronchitis (J41-42; 491), emphysema (J43; 492), and asthma (J45-46; 493). Lung diagnoses were seen among 2.5% of the population (Supplementary File 2). Persons were defined as having multimorbidity, if diagnoses from at least two different groups, out of the ten, were present. Diagnoses included in the ten groups covered frequent conditions in the population and were selected based on clinical relevance, earlier definitions of multimorbidity9,26 and systematic reviews.22,27–30 We assumed that a combination of conditions that differ in how they are treated and managed in the health care system may be organizationally and physiologically more complicated. Therefore, we consider that groups of diagnoses, instead of individual diagnoses, better reflect the complexity related to multimorbidity. Prevalence of the included diagnoses in this study is listed in Supplementary File 2.
Statistical analyses
For combinations of two diagnosis groups, there are three possible chronologies: one can appear before the other or vice versa, or they can appear simultaneously. With ten diagnosis groups, this gives 45 × 3 = 135 chronologized combinations. The association between 15-year mortality and chronology of multimorbidity was calculated by comparing the risks (all 135 combinations), compared to persons not in any of the ten diagnosis groups with odds ratios (ORs) from multivariable logistic regression. Adjustments were made for age, sex, socioeconomic status, degree of urbanization, and cohabitation status. To assess excess mortality, we calculated a synergy or susceptibility factor. 31 This factor is calculated as a ratio of ORs (ROR) = ORA+B/(ORA × ORB). This means that if, for example, ROR > 1, there is higher mortality when two diagnosis groups appear in one person, compared to when the two diagnosis groups appear separately in two persons. 31 As for a given combination of diagnosis groups, a separate ORA+B is obtained for each of the three chronologies; excess mortality is also assessed by separate ROR for each chronology. We will focus our result section mainly on combinations with ROR > 1, but in some cases, combinations with ROR < 1 will be touched upon. SAS, version 9.4 (SAS Institute Inc., Cary, NC, USA) was used for statistical analyses.
Results
Baseline characteristics of the Danish population by number of diagnosis groups.

a1 January, 2000.
bPresented as dichotomous variables in numbers (N) and percentages (%). No multimorbidity = 0 or 1 diagnosis group, multimorbidity = 2 or ≥3 diagnosis groups.
cSecondary school: secondary school, high school, and higher-level vocational studies.
dHigher educations: short and medium higher education or college diploma, university degree (bachelor or master), doctoral degree.
eIncome: divided into quartiles, yearly income in Danish kroner.
fOut of workforce: unemployed, student, apprentice or intern, or incapacity benefits.
gAssets: divided in tertiles, presented in Danish kroner, including stocks, bonds, savings in banks and housing, within and outside Denmark.
hRural: at least 50% of the population in the municipality lives in a thinly populated area. Small town: Intermediate density area. Less than 50% of the population lives in a densely populated area and less than 50% of the population lives in a thinly populated area. Capital: At least 50% of the population lives in a densely populated area.
The 10 diagnosis group combinations with highest mortality and excess mortality, respectively.

Diagnosed in the presented chronology.

Mortality risk associated with disease onset chronology in multimorbidity.
Multimorbidity including heart diagnoses was prevalent (1.8%) and associated with considerably increased mortality, especially if the heart diagnosis occurred as the second diagnosis (Figure 2(a) and (c)) (Supplementary Files 3 and 5). If diagnosed concurrently, mortality was generally higher than if diseases were diagnosed over time (Figure 2 (a)–(c)), especially in combination with lung diseases (OR 3.48 [95% CI 3.39–3.57] and ROR 1.54 [95% CI 1.41–1.70]) or kidney diseases (OR 3.45 [95% CI 3.05–3.85] and ROR 3.58 [95% CI 2.39–5.36]) (Figure 2(b)) (Supplementary Files 4 and 7).
Multimorbidity including sensory diagnoses was relatively common (1.1%) and was associated with high mortality, especially if it developed as the second disease. If diagnosed simultaneously with other diseases, lower excess mortality was observed for almost all combinations (Figure 2(b)) (Supplementary Files 4 and 7).
For multimorbidity including mental health diagnoses (0.6%), mortality was highest if the mental health diagnosis appeared as the first, for example, in combination with sensory (OR 4.10 [95% CI 3.90–4.29] and ROR 1.35 [95% CI 1.11–1.64]) diagnoses (Figure 2(a) and (c)) (Supplementary Files 3 and 5). Furthermore, when diagnosed concurrently, excess mortality increased for three (only two were significant) out of ten combinations, where, for example, the combination mental health and neurological diseases had lower excess mortality (OR 2.65 [95% CI 2.51–2.79] and ROR 0.59 [95% CI 0.51–0.68]) (Figure 2(b)) (Supplementary Files 4 and 7).
Multimorbidity including gastroenterological and kidney diagnoses (0.7% and 0.3%, respectively) did not confer a higher risk of death when diagnosed at different points in time. However, if diagnosed concurrently, mortality and excess mortality increased for almost all combinations. Overall, diagnoses that were made simultaneously, rather than consecutively, had higher excess mortality for the vast majority of combinations (Figure 2(b)) (Supplementary Files 4 and 7).
Discussion
This study investigated, in the full Danish adult population, how the association between multimorbidity and mortality is affected by the order in which the diseases in different multimorbidity combinations are diagnosed. Overall, chronology has a small effect on the association between multimorbidity and mortality, except for heart, sensory, and mental health diagnoses, where mortality is higher if a mental health diagnosis comes first or if a heart or a sensory comes second. Multimorbidity including heart diagnoses is particularly harmful when it concurs with either the lung or kidney. In general, excess mortality is higher if diagnosing coincides compared to if diagnosing spreads over time, especially for gastroenterological and kidney diagnoses. However, sensory diagnoses are seldom diagnosed concurrently with other diagnoses, and if so, both mortality and excess mortality is comparably low (Figure 2(b)).
Comparison with existing literature
Trajectories of multimorbidity have received increasing interest,16,32–34 as have multimorbidity clusters 35 and their relation to mortality.7,34,36,37 However, this is the first study to explore how chronology affects the association between multimorbidity and mortality. The main findings of our study are twofold: overall, chronology does not have a consistent effect on the association between multimorbidity and mortality (with few exceptions) and excess mortality is higher for the majority of multimorbidity combinations when diagnoses are made at the same time.
In relation to the first finding, musculoskeletal diagnoses are both frequent and do not confer a high mortality risk, especially when the musculoskeletal diagnosis comes first. Musculoskeletal diagnoses are very prevalent among patients with multimorbidity. 38 However, the development of a musculoskeletal disorder in the presence of preexisting chronic conditions may result from a reduced physical performance and serve as a pathway to mortality.39,40 Multimorbidity including heart diagnoses is both prevalent and has higher mortality, especially if the heart disease is diagnosed second. Cardiovascular diseases often develop later in life or later in the multimorbidity trajectory.33,41 In our study, the combination of heart and lung disorders was associated with higher mortality, which may be because of residual confounding, for example, shared lifestyle risk factors such as smoking, which we were not able to control for. Mental health diagnoses are most harmful when they appear as the first diagnosis. Mental health conditions tend to appear at some point in the multimorbidity trajectory, with increasing risk with the number of somatic conditions9,41; however, for some ethnic and younger age groups, depression is often the starting diagnosis. 33 Furthermore, there is a relation between mental health conditions and the development of later somatic conditions. 42 Most severe and persistent mental disorders have an age of onset in the 20s and 30s; these mental disorders are risk indicators for somatic morbidity. 43 Severe mental health disorders reduce life expectancy by almost two decades. 44 This could probably be ascribed to several factors such as metabolic side effects of psychotrop medication and unhealthy lifestyle, but also shared genetic factors for the mental health disorders and some somatic conditions. 45
The second finding, that there is excess mortality (ROR > 1) if diagnoses coincide and ROR < 1 when the onsets are separated in time, could have several explanations. If patients are diagnosed with one condition and receive medical attention for this condition, there is a higher chance that a second condition is found and often earlier in the course of the disease. The second disease is therefore often less severe than if it was found as the first. 46 Hence, for disease onsets separated in time, a ROR < 1 is expected. This means that detection bias to some extent is inherent to multimorbidity. Since many definitions of multimorbidity include risk factors, 31 that is, conditions associated with a probability of disease,47,48 some patients, depending on the definition used, will be found even earlier in the disease trajectory.
For patients with multimorbidity, symptoms are frequent and the number of symptoms increases with the number of diagnoses. 49 At a certain point in the multimorbidity trajectory, or a certain speed in disease development, people become aware of sensations 50 and symptoms, sometimes overwhelming them, 51 increasing the chance that a doctor contact is established. 52 The simultaneous appearance of two or more diagnosis groups may also be the observation of the onset of systemic disease, which tends to be more hazardous or have some underlying etiology or pathology53,54 explaining the coincidence. Another explanation is that for a second condition to be discovered simultaneously with a first condition—which would be the focus of the hospital contact—it has to present itself prominently. Hence, this second condition will often be more dangerous than if it was found by itself. Conversely, especially since we use secondary sector data, the doctor’s actions taken in relation to a symptom may increase the risk or chance that another diagnosis is detected, for example, a well-treated diabetes diagnosis with several years of duration may first be recorded in the secondary sector as an auxiliary diagnosis at the time for a hospital contact for another disease. An excess mortality may then appear when the diabetes is subsequently downplayed in light of the new condition.
Strengths and limitations
In this study, the use of a large nationwide cohort including the whole adult (≥18 years) Danish population is a strength and the sample size makes it possible to explore not only combinations of two diagnosis groups but also combinations of the two in a chronological perspective. It is well known that in the case of multimorbidity, mortality increases considerably with age,7,9 as well with the number of diagnoses,7,38 and especially from three or more diagnoses mortality increases steeply. 12 Therefore, if we had studied combinations of multimorbidity containing more than two diagnosis groups or had included another age group, we may have had other and stronger associations to mortality. Often, studies use a simple count of diseases when defining multimorbidity27,30,55; however, in the present study, multimorbidity is defined based on diagnosis groups sharing similarities in how they are managed and treated in the health care system. Hence, having multimorbidity according to this definition allows for an extra organizational aspect to be taken into account, why we believe complexity and burden of multimorbidity, but also the association to mortality is better grasped. The use of data from secondary care underestimates the prevalence of multimorbidity seen in general practice. On the other hand, we include diagnoses of a certain severity since a referral is required to get in contact with the secondary health system. Furthermore, the used registers are highly valid19,20 and no nationwide primary care register exists in Denmark. Using registers, we are not able to get information on important lifestyle factors, and even though we adjusted our results for important factors known to be a risk factor for developing and dying from multimorbidity,9,56 residual confounding can still be present. The risk of selection bias and sampling error is low. The large sample size allows for very precise estimation, with concomitantly low p-values, also for clinically less relevant associations; thus, interpretation has to be cautious. 57 It is a limitation that we did not consider the time passed between the first and the second diagnosis. However, when using diagnoses collected over a period of 10 years (prior to baseline), both incident and prevalent diagnoses are believed to be found, that is, with certain disease trajectories or be caught late in the course of the disease. 57 The independence between the prevalence of the outcome and OR is the primary reason for using logistic regression to assess the associations between chronology in multimorbidity and mortality. Furthermore, the ORs are directly comparable across the different multimorbidity combinations and across chronology, as well as they enable us to construct the RORs. In an earlier study, sensitivity analyses assuming all persons who were lost to follow-up were deceased did not change the conclusions. 7
Implications
This study adds knowledge on how multimorbidity develops from a time perspective and how chronology influences mortality. This can be valuable when organizing care for patients with multimorbidity, especially if they have indications for prevention. In this sense, it is also important to have gained an understanding that chronology is not a major driver of mortality. Multimorbidity combinations including mental health conditions as the first diagnosis need extra attention (e.g., when diagnosing new conditions, planning tertiary prevention and care) because of the associated elevated mortality. Especially to focus on heart risk factors among patients with mental health conditions could be meaningful, and to target mental health conditions in relation to multimorbidity seems to be one of few successes in multimorbidity interventions until now.58,59 Furthermore, combined specialist clinics, or increased cooperation between the responsible hospital departments, for patients having certain combinations of multimorbidity, for example, combinations including cardiovascular and lung diagnoses, could be valuable. Furthermore, this study stresses awareness of multimorbidity including diagnoses that are diagnosed at the same point in time because of the synergy in mortality risk they seem to contain. The large sample makes it possible to reveal valuable clinical implications, but this would require a focus on single conditions instead of groups of diagnoses. Therefore, some research implications of this study will be to look further into diagnoses in combinations that contain especially high excess mortality. Furthermore, we will explore what time (long vs short) between diagnoses means for mortality.
Conclusions
In general, the chronology in which diseases develop in multimorbidity is not associated with mortality, with a few exceptions for combinations including heart, sensory, and mental health diagnoses. This opens up for focus on preventive actions in order to mitigate some of the consequences of multimorbidity. Multimorbidity definitions are wide and diverse, and even in secondary care, the prevalence may partly be explained by the exposure to health care contacts among these patients, where conditions are found earlier in the disease trajectory. Finally, awareness is needed for diagnoses found concurrently since they act synergistically in relation to mortality, compared to multimorbidity found over time.
Supplemental Material
Supplemental Material - The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study
Supplemental Material for The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study by Tora G Willadsen, Volkert Siersma, Dagny R Nicolaisdóttir, Rasmus Køster-Rasmussen, Susanne Reventlow and Maarten Rozing in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study
Supplemental Material for The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study by Tora G Willadsen, Volkert Siersma, Dagny R Nicolaisdóttir, Rasmus Køster-Rasmussen, Susanne Reventlow and Maarten Rozing in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study
Supplemental Material for The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study by Tora G Willadsen, Volkert Siersma, Dagny R Nicolaisdóttir, Rasmus Køster-Rasmussen, Susanne Reventlow and Maarten Rozing in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study
Supplemental Material for The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study by Tora G Willadsen, Volkert Siersma, Dagny R Nicolaisdóttir, Rasmus Køster-Rasmussen, Susanne Reventlow and Maarten Rozing in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study
Supplemental Material for The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study by Tora G Willadsen, Volkert Siersma, Dagny R Nicolaisdóttir, Rasmus Køster-Rasmussen, Susanne Reventlow and Maarten Rozing in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study
Supplemental Material for The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study by Tora G Willadsen, Volkert Siersma, Dagny R Nicolaisdóttir, Rasmus Køster-Rasmussen, Susanne Reventlow and Maarten Rozing in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study
Supplemental Material for The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study by Tora G Willadsen, Volkert Siersma, Dagny R Nicolaisdóttir, Rasmus Køster-Rasmussen, Susanne Reventlow and Maarten Rozing in Journal of Multimorbidity and Comorbidity
Supplemental Material
Supplemental Material - The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study
Supplemental Material for The effect of disease onset chronology on mortality among patients with multimorbidity: A Danish nationwide register study by Tora G Willadsen, Volkert Siersma, Dagny R Nicolaisdóttir, Rasmus Køster-Rasmussen, Susanne Reventlow and Maarten Rozing in Journal of Multimorbidity and Comorbidity
Footnotes
Author Contributions
T.G.W. designed, wrote, and edited the manuscript, researched the data, and contributed to the discussion. V.S. and D.R.N. performed the analyses, researched the data, contributed to the discussion, and reviewed/edited the manuscript. R.K.-R., S.R., and M.R. researched the data, made important contributions to the discussion and content, and reviewed/edited the manuscript. All authors approved the final version of the manuscript. T.G.W., V.S., and D.R.N. have full access to data and take full responsibility for the reliability and truthfulness of the data and the data analyses. T.G.W. is the guarantor of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Helsefonden, grant number 19-B-0173 and Fonden for Almen Praksis (A3515).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.