
Abstract
Background:
Knowledge about prevalent and deadly combinations of multimorbidity is needed.
Objective:
To determine the nationwide prevalence of multimorbidity and estimate mortality for the most prevalent combinations of one to five diagnosis groups. Furthermore, to assess the excess mortality of the combination of two groups compared to the product of mortality associated with the single groups.
Design:
A prospective cohort study using Danish registries and including 3.986.209 people aged ≥18 years on 1 January, 2000. Multimorbidity was defined as having diagnoses from at least 2 of 10 diagnosis groups: lung, musculoskeletal, endocrine, mental, cancer, neurological, gastrointestinal, cardiovascular, kidney, and sensory organs. Logistic regression (odds ratios, ORs) and ratio of ORs (ROR) were used to study mortality and excess mortality.
Results:
Prevalence of multimorbidity was 7.1% in the Danish population. The most prevalent combination was the musculoskeletal–cardiovascular (0.4%), which had double the mortality (OR, 2.03) compared to persons not belonging to any of the diagnosis groups but showed no excess mortality (ROR, 0.97). The neurological–cancer combination had the highest mortality (OR, 6.35), was less prevalent (0.07%), and had no excess mortality (ROR, 0.94). Cardiovascular–lung was moderately prevalent (0.2%), had high mortality (OR, 5.75), and had excess mortality (ROR, 1.18). Endocrine–kidney had high excess mortality (ROR, 1.81) and cancer–mental had low excess mortality (ROR, 0.66). Mortality increased with the number of groups.
Conclusions:
All combinations had increased mortality risk with some of them having up to a six-fold increased risk. Mortality increased with the number of diagnosis groups. Most combinations did not increase mortality above that expected, that is, were additive rather than synergistic.
Introduction
The number of people living with multimorbidity is high, 1 and the prevalence has risen considerably in high-income countries during the last decades. 2 Multimorbidity is most often defined as the co-occurrence of two or more chronic conditions in a person. 3 However, there is no consensus about the definition 4,5 that explains most of the observed differences in prevalence estimates. 6,7 Multimorbidity is associated with increased health-care use with higher costs as a consequence. 8 Patients with multimorbidity report lower quality of life, 9,10 more mental symptoms, 7 and experience more fragmented care. 11 Mortality increases with both number and certain combinations of diseases. 12–14 Despite ongoing research on patterns of multimorbidity, 15,16 health-care systems are still better prepared for handling single diseases than their combinations because of their focus on specialism rather than generalism. 17
Patients with multimorbidity require a comprehensive care approach, and treatments may depend on the specific combinations of diseases. 18 Therefore, in the present study, multimorbidity was defined by combinations of diagnoses from at least 2 of 10 groups of diagnoses. Knowledge about relevant combinations, that is, the most prevalent and their related mortality, may guide us regarding how to intervene. The association between multimorbidity and mortality is known. 14 There exist some longitudinal studies exploring mortality in relation to multimorbidity with long, that is, 10 years or longer 12,19,20 and shorter, 13,21,22 follow-up times. One of the studies explored the most prevalent and the most lethal combinations of two to five diseases, respectively, 19 and one explored specific lethal combinations of two and three conditions. 13 However, all these studies included persons aged >65 years with the last study only including a limited number of persons aged 85 years or older. 13 Multimorbidity is not just an issue for older people 7 and to be able to intervene efficiently a focus on the general population is necessary. This study investigates relevant combinations of multimorbidity, that is, prevalent combinations associated with high mortality. The mortality in relation to the most prevalent specific combinations of one to five organizationally and manageably similar groups of diagnoses, in an entire adult population, will be identified.
Objectives
This study has four aims: (1) to identify the most prevalent combinations (of one to five diagnosis groups) of multimorbidity; (2) to find among all combinations of two diagnosis groups the combinations with highest mortality; (3) to assess the excess mortality from having a combination of two diagnosis groups, compared to the product of the mortality when the same diagnosis groups appear individually; and (4) to estimate the mortality associated with the most prevalent combinations of three, four, and five diagnosis groups.
Material and methods
Study design and population
This study is a historical prospective cohort study in Denmark including 3.986.209 people aged ≥18 years and alive at baseline on 1 January, 2000 (Figure 1). The cohort was created based on information from the Danish Civil Registration System (CRS) 23 and followed for 15 years until 31 December, 2014. Background characteristics of the cohort were identified at baseline: age, sex, socioeconomic status (family income, highest completed education, work status, and assets), degree of urbanization, and cohabitation status. The level of multimorbidity was estimated at baseline by collecting information from the national health registries on all diagnoses related to hospital admissions or hospital outpatient clinic contacts 10 years before baseline (1 January, 1990, until 31 December, 1999). Our outcome was 15-year all-cause mortality. Patients who migrated or disappeared during the 10 years before baseline were excluded (Figure 1).

The population cohort through study.
Nationwide registries
In Denmark, all live born children and new residents get a unique personal identification number stored in CRS. CRS provides information on vital status, address, family connections, emigration, and so on. 23 The personal identification number can be used to link information from all Danish registries on an individual level. Since registration in CRS is required by Danish law and the register is used continuously for administrative purposes, is updated weekly, and errors are corrected continuously, the register is believed to contain accurate information of high quality. 23
Information about diagnoses were obtained from three registers: the Danish National Patient Register (NPR), 24 the Danish Cancer Registry (CR), 25 and the Danish Psychiatric Central Research Register (PCRR). 26 NPR is believed to be complete at least after year 2000 where the codes became the payment basis for hospitals. 24 However, outpatient care and emergency admissions were first included in 1995. In NPR, diagnostic information is registered as International Classification of Diseases, 10th edition (ICD-10) and the earlier version 8th edition (ICD-8). 27 The shift between versions happened in 1994. CR includes data on all incident cancers in Denmark since 1943, and CR has used ICD-10 codes since 1978. 25 In Denmark, patients with mental illnesses and in need of secondary care are treated at public hospitals and registered in PCRR with ICD codes as in NPR. 26 To collect information on socioeconomic status, Statistics Denmark’s registers on income, 28 education, 29 work status, 30 and assets 28 were used.
The study was based on anonymized administrative register data, which is why neither collection of informed consent from the involved persons nor approval from the Ethics Committee was needed. The study was approved by The Danish Data Protection Agency, The Danish Health Data Authority, and Statistics Denmark.
Definition of multimorbidity
The definition of multimorbidity was based on diagnoses organized in 10 groups where the groups to some extent share treatments, clinical picture, or organization of health care: lung, musculoskeletal, endocrine, mental, cancer, neurological, gastrointestinal, cardiovascular, genitourinary, and sensory organs, with each group containing several diagnoses (Online Supplemental Material 1). Multimorbidity was defined as having diagnoses from two or more different groups. The diagnoses included within the 10 groups were selected based on clinical relevance, definitions used in earlier work on multimorbidity, 7,31 and recommendations from systematic reviews. 4,6,32,33 Moreover, by grouping diagnoses instead of handling them as singles, complexity is better embraced, since it is organizationally and physiologically more complex if patients suffer from diagnoses with differences in treatments and organization of health care.
Statistical analyses
Prevalence of multimorbidity is presented as numbers and percentages of the whole population. The association between 15-year mortality and multimorbidity (combinations of one to five mutually exclusive diagnosis groups of these 10 groups), compared with those not belonging to any of the groups, is assessed by odds ratios (ORs) from multivariable logistic regression (with every combination giving an OR) adjusted for age, sex, socioeconomic status (income, highest completed education, work status, and assets), degree of urbanization, and cohabitation status (incorporated in the analyses in the categorizations shown in Table 1). The large cohort made us able to look at all possible combinations of two diagnosis groups (45 in total). However, the expected small numbers of patients in some groups made us solely looking at the five most prevalent combinations for three, four, and five diagnosis groups, respectively.
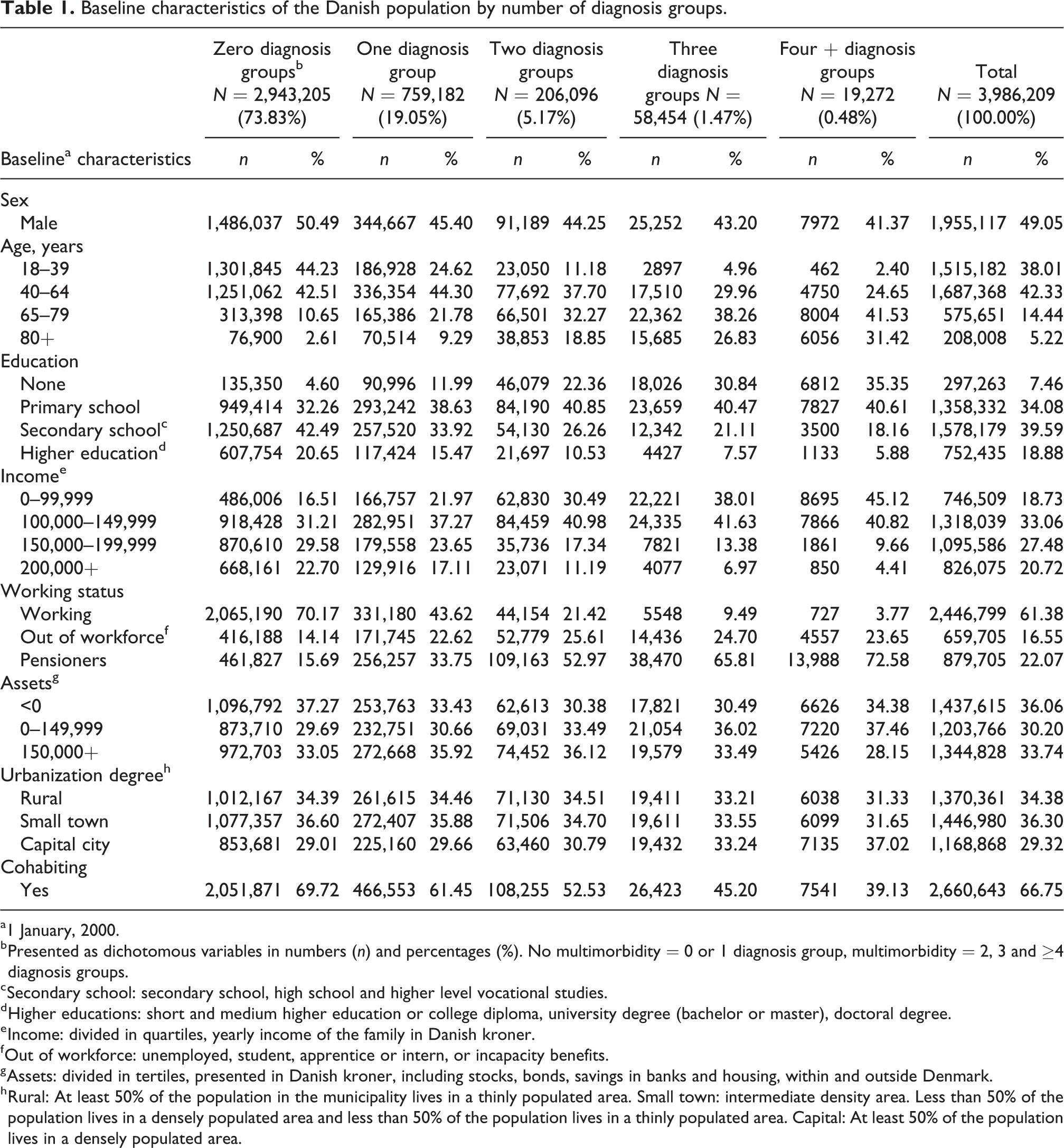
Baseline characteristics of the Danish population by number of diagnosis groups.
a1 January, 2000.
b Presented as dichotomous variables in numbers (n) and percentages (%). No multimorbidity = 0 or 1 diagnosis group, multimorbidity = 2, 3 and ≥4 diagnosis groups.
c Secondary school: secondary school, high school and higher level vocational studies.
d Higher educations: short and medium higher education or college diploma, university degree (bachelor or master), doctoral degree.
e Income: divided in quartiles, yearly income of the family in Danish kroner.
f Out of workforce: unemployed, student, apprentice or intern, or incapacity benefits.
g Assets: divided in tertiles, presented in Danish kroner, including stocks, bonds, savings in banks and housing, within and outside Denmark.
h Rural: At least 50% of the population in the municipality lives in a thinly populated area. Small town: intermediate density area. Less than 50% of the population lives in a densely populated area and less than 50% of the population lives in a thinly populated area. Capital: At least 50% of the population lives in a densely populated area.
A relative excess mortality for a combination of diagnoses from diagnosis groups A and B was calculated as a ratio of ORs (ROR) = ORA+B/(ORA×ORB), that is, the mortality increases associated with having diagnoses from both diagnosis groups A and B (a potential interaction) relative to the product of the mortality increases associated with having a diagnose from group A but not from group B, or vice versa. p-Values were calculated for all interactions. At the end of the follow–up, the group that emigrated or disappeared was considered to be alive at a 15-year follow-up. In sensitivity analyses, this group was considered dead at a 15-year follow-up. Analyses were performed using SAS, version 94 (SAS Institute Inc., Cary, North Carolina, USA).
Results
At baseline, the population consisted of 4.172.941 individuals (49.1% men and 50.9% women) and during follow-up 802.189 died (Figure 1).
The prevalence of multimorbidity in the Danish population was 7.1% at baseline (year 2000), increasing from 1.7% in those aged 18–39 years to 29.1% among those aged 80+ (Table 1). Multimorbidity was relatively more prevalent in females, those living alone, and those with low socioeconomic status.
Overall, musculoskeletal and cardiovascular diagnosis groups were the most frequent individual groups with a prevalence of 7.4% and 5.5%, respectively (Online Supplemental Material 2). The musculoskeletal–cardiovascular combination was the most prevalent pair of diagnosis groups, occurring in 16.001 people (0.4%) (Table 2, Figure 2, and Online Supplemental Material 3). The number of patients dropped rapidly by increasing the number of diagnosis groups. Of notice, the musculoskeletal and the cardiovascular diagnosis groups were included in almost all the five most common combinations of three, four, and five diagnosis groups (Table 2).
The five most prevalent combinations of one, two, three, four, and five diagnosis groups, respectively.a
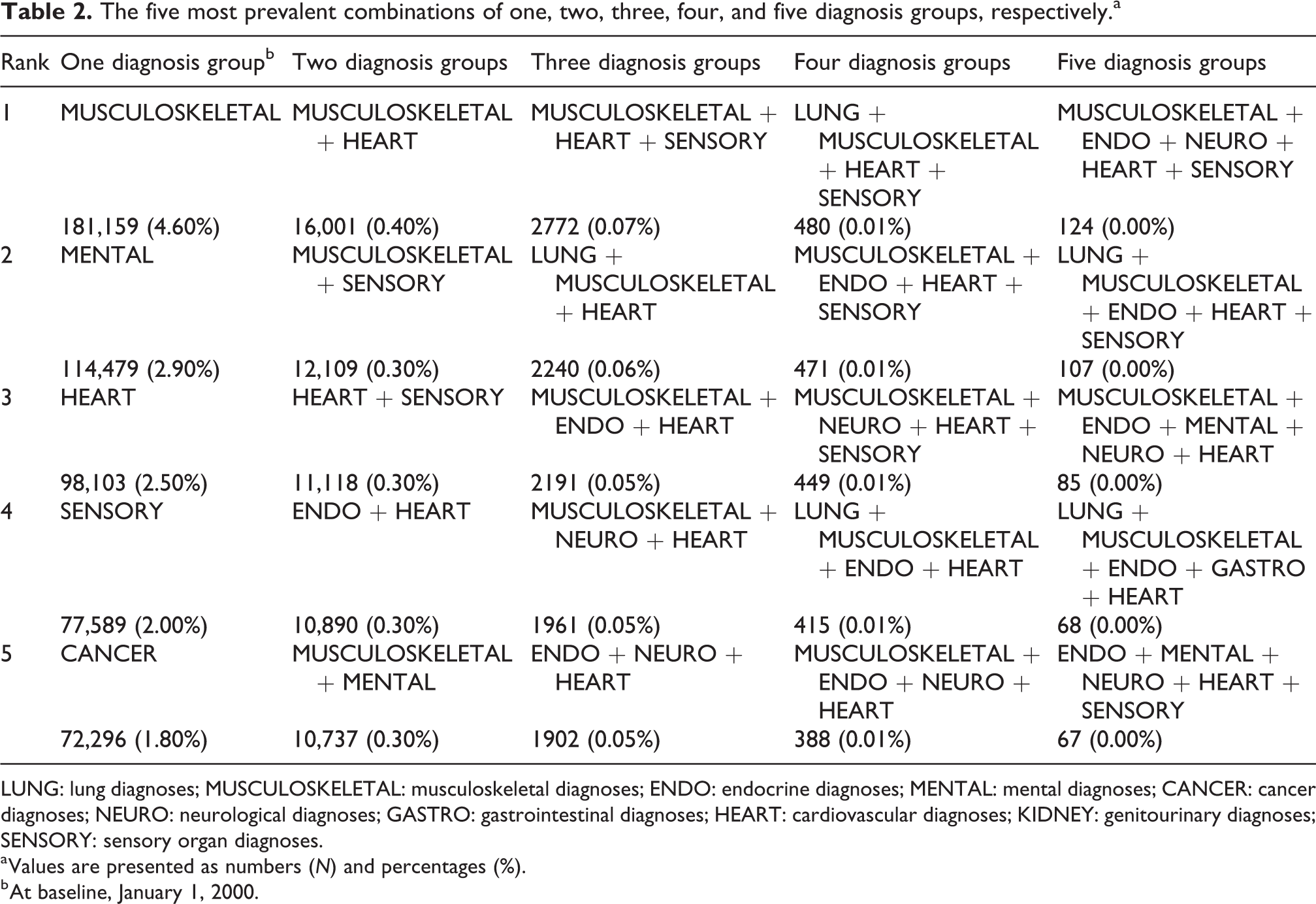
LUNG: lung diagnoses; MUSCULOSKELETAL: musculoskeletal diagnoses; ENDO: endocrine diagnoses; MENTAL: mental diagnoses; CANCER: cancer diagnoses; NEURO: neurological diagnoses; GASTRO: gastrointestinal diagnoses; HEART: cardiovascular diagnoses; KIDNEY: genitourinary diagnoses; SENSORY: sensory organ diagnoses.
a Values are presented as numbers (N) and percentages (%).
b At baseline, January 1, 2000.

Prevalence (size of the circles), mortality (grey scale), and interaction or relative excess mortality or the ROR (border color of the circles) for all possible pairs of multimorbidity (adjusted for age, sex, socioeconomic status, cohabitation status, and degree of urbanization). ROR: ratio of odds ratio.
Figure 2 illustrates prevalence, mortality (OR), and relative excess mortality (ROR) for all possible combinations of two diagnosis groups (pairs). All combinations had increased mortality compared with individuals without diagnoses from any of the 10 diagnosis groups. Pairs containing a musculoskeletal diagnosis were generally associated with the lowest mortality with none of the combinations having an OR exceeding three. Combinations including lung diagnoses, on the other hand, had a three-fold increased mortality for all combinations with the exception of those including musculoskeletal diagnoses (Figure 2).
Furthermore, pairs including diagnoses from neurological, cancer, lung, cardiovascular, and mental diagnosis groups had the highest mortality, with the neurological–cancer combination having the highest OR (6.35; 95% confidence interval (CI): 5.71–7.06) followed by neurological–endocrine (5.94; 95% CI: 5.42–6.50) and cardiovascularlung (5.75; 95% CI: 5.42–6.10) (Online Supplemental Material 3). Men having diagnoses from either the endo or the cancer diagnosis groups had a doubled mortality risk compared to women. For the oldest age group, a high mortality risk was associated with having a diagnosis from the mental diagnosis group (Online Supplemental Material 4).
Relative excess mortality was highest for the combination of kidney–endocrine with 81% increased mortality. The mental–cancer combination, on the other hand, had a 34% reduced mortality compared with the product of the risks when these diagnosis groups appeared singly in two individuals (Figure 2 and Online Supplemental Material 5).
Mortality increased rapidly with the number of diagnosis groups, also after adjustment. The combination of five groups including musculoskeletal, endocrine, mental, neurological, and cardiovascular had by far the highest mortality (Table 3). The sensitivity analyses did not change the main results (Online Supplemental Material 6).
Prevalence and OR of mortality for the five most prevalent combinations of three, four, and five diagnosis groups.
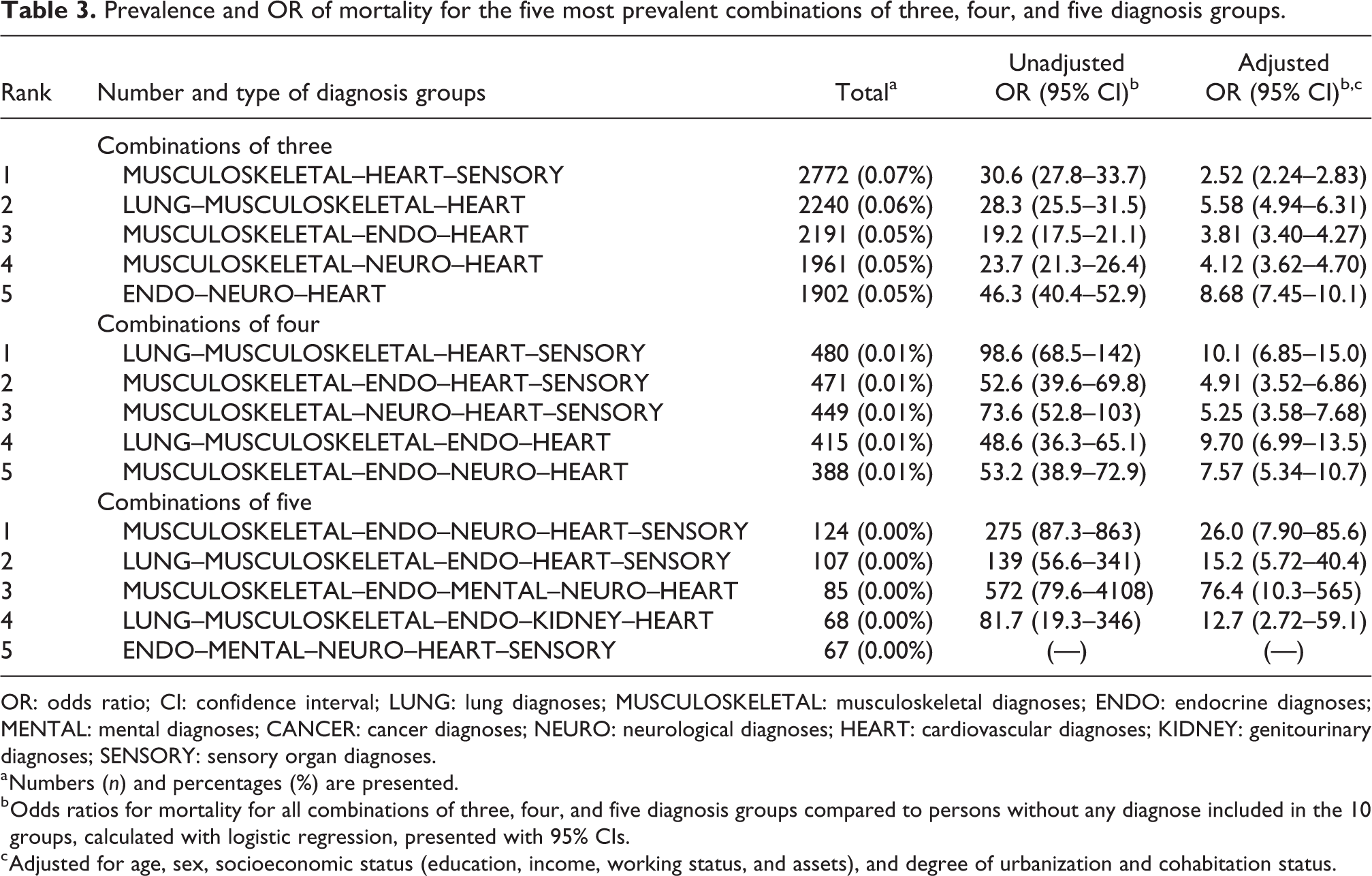
OR: odds ratio; CI: confidence interval; LUNG: lung diagnoses; MUSCULOSKELETAL: musculoskeletal diagnoses; ENDO: endocrine diagnoses; MENTAL: mental diagnoses; CANCER: cancer diagnoses; NEURO: neurological diagnoses; HEART: cardiovascular diagnoses; KIDNEY: genitourinary diagnoses; SENSORY: sensory organ diagnoses.
a Numbers (n) and percentages (%) are presented.
b Odds ratios for mortality for all combinations of three, four, and five diagnosis groups compared to persons without any diagnose included in the 10 groups, calculated with logistic regression, presented with 95% CIs.
c Adjusted for age, sex, socioeconomic status (education, income, working status, and assets), and degree of urbanization and cohabitation status.
Discussion
We examined the prevalence of different multimorbidity combinations and the associated mortality in a nationwide Danish population sample. The musculoskeletal–cardiovascular combination was the most prevalent, cancer–neurological had the highest mortality, and the lung–cardiovascular combination was both prevalent and lethal. Pairs including musculoskeletal diagnoses had a relatively low mortality. Some pairs interacted and had different mortalities when in combination, compared to the product of the individual mortalities. Prevalence dropped rapidly and mortality increased steeply with the number of diagnosis groups.
Prevalence of multimorbidity
By using a new definition, the prevalence of multimorbidity in the Danish population was 7.1%. In earlier studies, the prevalence of multimorbidity has been found to vary from 3.5% to 98.5% depending on age group and setting. 6,16 A Danish study using register data, but defining multimorbidity by counting diagnoses from a list of 39 conditions, estimated the prevalence to be 20% for people having two or three diagnoses and 9% for those having four or more. 34 In line with our results, several studies have found increasing prevalence with age 6,7,16,35 and higher rates in women. 16,36 The relatively low prevalence in the present study is mainly explained by (1) our definition of multimorbidity with the use of diagnosis groups, instead of single diagnoses; (2) our use of register data from secondary care, instead of data from primary care; and (3) our population, including adults aged ≥18 years and not only older people. 4–6
Our finding of musculoskeletal and cardiovascular as the most prevalent diagnosis groups, both as singles and in combination, is in line with earlier research, where cardiovascular, metabolic, and musculoskeletal clusters are found to be the most prevalent single clusters in all age groups. 37 Additionally, hypertension and osteoarthritis has been found to be the most frequent combination, 16 and also the combination of metabolic (including cardiovascular) and musculoskeletal conditions is common, where lower back pain is the condition most likely to occur with other conditions. 38 A systematic review found depression most likely to co-occur with other conditions and found the combinations of depression and arthritis and depression and diabetes to be the second and the third most common diagnosis pairs, respectively. 39 We did not find the mental–musculoskeletal and mental–endocrine combinations in the top three, maybe because we used secondary care diagnoses without information about less serious mental illnesses treated solely in primary care.
Mortality and relative excess mortality
We found the cancer–neurological combination to be the most hazardous, followed by neurological–endocrine and cardiovascular–lung. Moreover, we found mental diagnoses to be generally associated with higher mortality. Cardiovascular diseases in combination with either diabetes or mental problems have been shown to be both frequent and highly mortal. 19 Perhaps, neurological and cognitive functions are required to understand and cope with symptoms as well as health advices. Furthermore, neurological diagnoses like Parkinson’s disease and cerebrovascular diseases are strongly related to frailty indicators, for example, geriatric syndromes. 40 The cardiovascular–lung group may contain individuals who share lifestyle risk factors for developing chronic conditions like, for example, smoking. In this study, pairs including musculoskeletal diagnoses had the lowest mortality, which is in line with earlier work where arthritis was associated with lower risk of death. 19
The kidney–endocrine combination, followed by gastrointestinal–mental, had the highest relative excess mortality, higher mortality in combination than the product of the mortality associated with the individual diagnosis groups. On the contrary, cancer–mental, followed by gastro–cardiovascular, had lower mortality in combination compared to the product of the single diagnoses. To the best of our knowledge, only one study has explored the interaction effect of pairs of diagnoses included in multimorbidity on mortality, finding excess mortality for combinations including cancer, 13 which is in contrast to our findings. Although somewhat speculative, the high mortality connected with the kidney–endocrine combination could be an accumulation of diabetes patients who are worse off in this combination compared to those in other combinations. The lower excess mortality for the cancer–mental combination could be a result of better management of the mentally ill patients in general when they are diagnosed with a somatic disease. It could also be explained by patients in this group having cancers of lower stage.
In this study, mortality increased with the number of diagnosis groups which is in line with other studies. 12,18 The combination of musculoskeletal, endocrine, mental, neurological, and cardiovascular had a 70 times increased mortality, compared with people not belonging to any of the diagnosis groups, even after adjustment. The influence of age and socioeconomic status on multimorbidity is well-known. 7,41 One study found increased mortality of 25% when having three conditions, rising to 80% when having five or more. 19 Yet another study found a steep decline in survival rates when having three conditions or more and found people with zero, one, or two conditions having largely equal remaining life expectancy. 42 Other factors, besides number and type of conditions, 13 are shown to be important for mortality, for example, perceived stress. 34 Furthermore, socioeconomic status 41 and disability 22 have been identified as important intermediate factors for mortality.
Strengths and limitations
When defining multimorbidity, many studies use simple counts of diseases. 4,5 In the present study, multimorbidity is defined by counting groups of diagnoses with similarities in treatments and management in both primary and secondary health care. Therefore, when having multimorbidity according to this definition, diagnoses representing different parts of the health-care system are included, allowing for an extra organizational aspect to be considered. We believe this way of defining multimorbidity can better grasp the complexity and burden of multimorbidity than definitions resting on simple diagnosis counts. 43 A major strength of this study is the large nationwide cohort including the whole adult Danish population. The size makes it possible to explore not only combinations of two diagnosis groups but also combinations of more groups. However, even if the risk of selection bias and sampling error is low, interpretation has to be cautious since we can expect highly significant p-values for clinically less important associations. 44 Despite the high validity of CRS, 23 a total of 15,543 (0.4%) persons disappeared from the cohort without further information. However, sensitivity analyses including these individuals did not change the conclusions. The information on multimorbidity was based on registry data from 10 years before baseline to collect information on both prevalent and incident diagnoses. 44 Incident diagnoses could potentially have another disease trajectory, with higher mortality initially and prevalent diagnoses could be at risk of being caught later in the disease course. The primary argument for use of logistic regression analyses to assess the associations between multimorbidity and mortality is the independence between the prevalence of the outcome and the OR. This makes ORs directly comparable across the different diagnosis groups and furthermore enables us to construct measures combining several ORs such as the ROR.
Our study has further limitations. Our use of secondary care data underestimates the true prevalence of multimorbidity as it is seen in primary care. However, in Denmark, nationwide primary care register data are not available. Moreover, the employed registries are relatively valid, 24,25 and by using this data source, we only include diagnoses with a certain gravity since the underlying condition lead to a referral to secondary care. Even though we adjusted our analyses for several important aspects of demography and socioeconomy, residual confounding cannot be ruled out since we were not able to get information on important lifestyle factors. Finally, we have no information on severity of the included diagnoses.
Implications
To the best of our knowledge, this is the first time mortality related to prevalent multimorbidity has been studied in an entire adult population over such a long time period. Consequently, this study adds clinically relevant patterns of multimorbidity valuable to consider when organizing health care and creating care plans to meet the demands of patients with multimorbidity. Combined specialist clinic visits for persons having, for example, musculoskeletal–cardiovascular and cardiovascular–lung combinations could be included in such coordinated care plans. Some diagnosis groups should create extra awareness, for example, neurological and lung, because of the high mortality for many of their combinations, and endocrine and cardiovascular because of the excess mortality when in different combinations compared to as singles.
Conclusions
The combination of cardiovascular and lung diagnoses was both prevalent and conferred high mortality. Some pairs of diagnosis groups had a higher mortality in combination than the combined mortality of the individual diagnoses, for example, kidney–endocrine, but generally combinations did not increase mortality above that expected, that is, were additive rather than synergistic. Mortality increased with the number of included diagnoses.
Supplemental Material
Supplementary_material_1_JoC - Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study
Supplementary_material_1_JoC for Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study by TG Willadsen, V Siersma, DR Nicolaisdóttir, R Køster-Rasmussen, DE Jarbøl, S Reventlow, SW Mercer, and N de Fine Olivarius in Journal of Comorbidity
Supplemental Material
Supplementary_material_2 - Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study
Supplementary_material_2 for Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study by TG Willadsen, V Siersma, DR Nicolaisdóttir, R Køster-Rasmussen, DE Jarbøl, S Reventlow, SW Mercer, and N de Fine Olivarius in Journal of Comorbidity
Supplemental Material
Supplementary_material_3 - Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study
Supplementary_material_3 for Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study by TG Willadsen, V Siersma, DR Nicolaisdóttir, R Køster-Rasmussen, DE Jarbøl, S Reventlow, SW Mercer, and N de Fine Olivarius in Journal of Comorbidity
Supplemental Material
Supplementary_material_4_JoC - Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study
Supplementary_material_4_JoC for Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study by TG Willadsen, V Siersma, DR Nicolaisdóttir, R Køster-Rasmussen, DE Jarbøl, S Reventlow, SW Mercer, and N de Fine Olivarius in Journal of Comorbidity
Supplemental Material
Supplementary_material_5_JoC - Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study
Supplementary_material_5_JoC for Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study by TG Willadsen, V Siersma, DR Nicolaisdóttir, R Køster-Rasmussen, DE Jarbøl, S Reventlow, SW Mercer, and N de Fine Olivarius in Journal of Comorbidity
Supplemental Material
Supplementary_material_6_JoC - Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study
Supplementary_material_6_JoC for Multimorbidity and mortality: A 15-year longitudinal registry-based nationwide Danish population study by TG Willadsen, V Siersma, DR Nicolaisdóttir, R Køster-Rasmussen, DE Jarbøl, S Reventlow, SW Mercer, and N de Fine Olivarius in Journal of Comorbidity
Footnotes
Authors’ note
The funding sources had no role in the study design, data collection, analysis and interpretation of data, in writing, or in the decision of journal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Danish Research Foundation for General Practice, The Health Foundation, The Research Council for Primary Care in the Capital Region of Denmark, Scholarship from University of Copenhagen, and Region Zealand’s Research Fund.
Supplementary Materials
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.