
Abstract
Background
Multimorbidity is rising in low-and middle-income countries such as Nepal, yet the research has not gained pace in this field. We aimed to systematically review the existing multimorbidity literature in Nepal and estimate the prevalence and map its risk factors and consequences.
Methods
We reviewed data collated from PubMed, Embase and CINAHL by including original studies that reported prevalence of multimorbidity in Nepal. The quality of included studies was assessed using the Appraisal Tool for Cross-sectional Studies. The summary of the review is presented both qualitatively as well as through meta-analysis to give pooled prevalence. We prospectively registered in PROSPERO (CRD42024499598).
Results
We identified 423 studies out of which seven were included in this review. All studies were conducted in a community setting except one which was hospital based. The prevalence reported across various studies ranged from 13.96% to 70.1%. The pooled prevalence of multimorbidity was observed to be 25.05% (95% CI: 16.99 to 34.09). The number of conditions used to assess multimorbidity ranged from four to nine. The major risk factors identified were increasing age, urban residence, and lower literacy rates.
Conclusion
A wide variance in the prevalence of multimorbidity was observed. Moreover, multimorbidity assessment tool/conditions considered for assessing multimorbidity were heterogeneous.
Keywords
Introduction
Multimorbidity is defined as the simultaneous presence of two or more long-term conditions in an individual without considering any as an index disease. 1 These conditions may or may not be related to each other. There is a rise in the prevalence of multimorbidity among low-and middle-income countries (LMICs) that can largely be attributed to urbanization, shift in dietary habits such as eating more processed food, sedentary lifestyle along with longevity due to recent improvements in the healthcare facilities. 2 Furthermore, the co-occurrence of prevailing infectious diseases of longer duration such as tuberculosis vis-à-vis rising non-communicable diseases (NCDs) like hypertension also contribute to the upsurge in multimorbidity in LMICs such as Nepal. 2 Multimorbidity is associated with an upward trend in healthcare utilization, expenditure, and poor patient reported outcome measures such as health related quality of life (HRQoL).3-5
A recent study from LMICs suggests the pooled prevalence of non-communicable disease multmorbidity was around 36.4%. 6 However, it did not include any studies from Nepal. Another systematic review observed the prevalence of chronic communicable diseases and NCD multimorbidity to range from 13% to 87% in LMICs, but it too did not have data from Nepal. 7 Nonetheless, data from the region indicates that Nepal is no exception to the multimorbidity trend observed in other LMICs. 8 The high prevalence of multimorbidity indicates an additional burden on already swamped healthcare systems of Nepal. 9 This is further compounded in rural areas with predominant poverty, lower literacy rates, lack of healthcare staff and poor resources including medications. 10 Lack of healthcare staff and irregular healthcare supplies may also mean a compromise in the continuity of care for the multimorbid individuals along with an additional burden on tertiary care health facilities in urban areas. 10 Hence, there is an urgent need to estimate the pooled burden of multimorbidity in the country so that the needs of multimorbid individuals may be highlighted. Moreover, the existing healthcare programmes and guidelines focus on single disease over multiple long-term conditions which make the care-seeking pathways convoluted. 11 This is not only challenging for the patients who navigate between multiple facilities or clinicians but also for healthcare providers to set priorities.
Multimorbidity research has not gained pace in smaller countries such as Nepal, and the existing literature is scattered across studies that are either confined to a particular region or smaller population/sample. Hence, there is a paucity of national level evidence which is required to guide the policy and healthcare service delivery in the country. Moreover, this also highlights the importance of finding gaps in present research in order to provide direction for future investigations. Hence, we aimed to systematically review the literature to estimate the prevalence of multimorbidity and identify its risk factors, commonly occurring patterns, and consequences (such as healthcare utilization, expenditure, and HRQoL) of multimorbidity in Nepal.
Methods
Protocol and standards
We prospectively registered this systematic review with the International Prospective Register of Systematic Reviews (ID: CRD42024499598). 12 This review was conducted and reported following the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines (Supplemental Table S1). 13
Eligibility criteria
We included original observational studies that documented the prevalence, risk factors and consequences of multimorbidity in Nepal. Studies that included individuals aged 18 years and above, were done either in community-based settings or hospitals were considered in this review. We excluded studies that did not explicitly mention multimorbidity; or considered comorbidities with an index disease. Furthermore, we also excluded any type of reviews, qualitative studies, editorials, and commentaries.
Information sources and search strategy
To make our search exhaustive, we included both medical literature databases as well as grey literature. We comprehensively searched three electronic databases i.e. Medline through PubMed, Embase, and CINAHL. Additionally, the reference lists of included studies were hand searched for any other relevant articles. We also used the website of “International Research Community on Multimorbidity” (Link: (https://www.gla.ac.uk/schools/healthwellbeing/research/generalpractice/internationalmultimorbidity/publications/) to locate relevant publications.
PubMed was used to build the basic search syntax which comprised of two major concepts: multimorbidity and Nepal. We used medical subject headings (MeSH) terms along with various other associated key words for ‘multimorbidity’ and ‘Nepal’ that made our search strategy comprehensive. Further, Boolean operator ‘AND’ was used to join the two major concepts. The detailed search strategy for each of the database was developed separately and has been provided in Supplemental Table S2. We also used database specific terms such as Emtree terms for Embase. Articles published up to 4th July 2023 (in each of the database) were included in this review.
Study selection and data extraction
We retrieved articles from all databases and sieved them for duplicates using Endnote software followed by which the remaining articles were uploaded in Rayyan software for primary screening. In the first round of screening, two authors (AS, SSS) independently reviewed the included studies by reading their titles and abstracts. At this stage, articles were marked as relevant, irrelevant or unsure. The articles deemed as irrelevant by both the authors were excluded. Next, we read full-texts of all studies that were included after primary screening. Here, two reviewers (AS, SSS) independently assessed these articles by strictly adhering to the inclusion and exclusion criteria of this systematic review. Any differences between the two reviewers were resolved with the help of a third reviewer (SP) from the team.
We extracted data from the relevant studies by using a preformed data extraction sheet especially designed for this study. This data sheet was first piloted to check for disparities of any. Two reviewers (AS, SSS) extracted and entered the data. The data extracted were verified by a third reviewer (KCS) and any dissent was resolved by entire team in consensus. If the data were unclear or required further clarifications, we contacted the corresponding authors of the relevant study through email. We collated data on the following parameters: author, year of publication, study design and setting, age of the participants included, proportion of sex, total sample size, prevalence of multimorbidity; and patterns, risk factors and consequences (if reported).
Risk of bias in individual studies
Two reviewers (AS, SSS) independently appraised the included studies for the risk of bias using Appraisal Tool for Cross-sectional Studies (AXIS). 14 Dissent between the reviewers was resolved by a third reviewer (NS). AXIS is a widely used tool to assess the quality of cross-sectional studies based on twenty questions that cover introduction, methods, results, discussion and others. This tool majorly assesses the methods section with questions based on study design, sample size, and sampling method. We marked ‘Yes=1’ or ‘No/Don’t Know=0’ for each of the twenty questions. Finally, any study scoring 0-50% was marked as having ‘high risk of bias,’ 51-80% score as ‘medium risk of bias,’ and 81-100% score as ‘low risk of bias.’
Summary measures
We presented the findings using both qualitative synthesis (by narrating the characteristics of study) and quantitative synthesis (meta-analysis through pooled prevalence). For meta-analysis, STATA version 17.0 (Stata Corp., Texas) software was used. ‘metan’ command based on random-effects models. We also calculated I2 statistic to assess the heterogeneity between different studies included in the review. In this review, we anticipate a high heterogeneity as the data collected considered variability in inclusion criteria of age groups such as ≥18 years or ≥60 years. Hence, we planned sub-group analysis based on age i.e. separate pooled prevalence for ≥60 year age group.
Ethical considerations
This review is based on the published literature, hence has no ethical concerns. We have not used individual patient data thus, eliminating privacy concerns.
Results
We obtained a total of 423 articles from three databases out of which 150 were discarded due to being duplicates. After screening the full-texts of ten studies, a total of seven articles met the inclusion criteria (Figure 1). PRISMA flow diagram representing selection of studies included in systematic review.
General characteristics of selected studies
Characteristics of the included studies.

*NCD: Non-communicable diseases.
Assessment of risk of bias
The risk of bias was assessed for all seven studies that qualified to be included in the review. We observed that all studies15-17, 19-21 had low risk of bias except Khadka T et al., 2023 18 that had medium risk of bias (Supplemental Table S4).
Prevalence
The prevalence reported across various studies ranged from 13.96% to 70.1% (Table 1). We included five studies for meta-analysis which yielded a pooled prevalence of 25.05% (95% CI: 16.99 to 34.09); I2=97.95%, p=0.00 (Figure 2a).15,16,18-20 We excluded two studies from meta-analysis as they were based on the same dataset as of the other included studies.17,21 Considering the age group of ≥60 years, the pooled prevalence of multimorbidity was 33.83% (95% CI: 22.48 to 46.21); I2=98.3%, p=0.00 (Figure 2b). The overall pooled prevalence of community-based studies after excluding a hospital based study by Khadka T et., 2023
18
was 16.92% (13.11 to 21.11); I2=93.13%, p=0.00, while that for population aged 60 years and above it was 20.46% (95% CI: 14.51 to 27.15); I2=95.9%, p=0.00 (Supplemental Figure 1a and 1b). Overall pooled prevalence of multimorbidity; *ES: Effect size, CI: Confidence Interval. 
Pattern
Only one study reported the commonly occurring patterns of multimorbidity in Nepal 16 . The major dyads reported were hypertension + diabetes mellitus (5.7%), hypertension + chronic obstructive pulmonary disease (4.7%), and hypertension + chronic kidney disease (4%). 16 The identified triad was that of hypertension + diabetes mellitus + chronic kidney disease (1.4%). 16
Risk factors
Risk factors of multimorbidity as reported in the included studies.
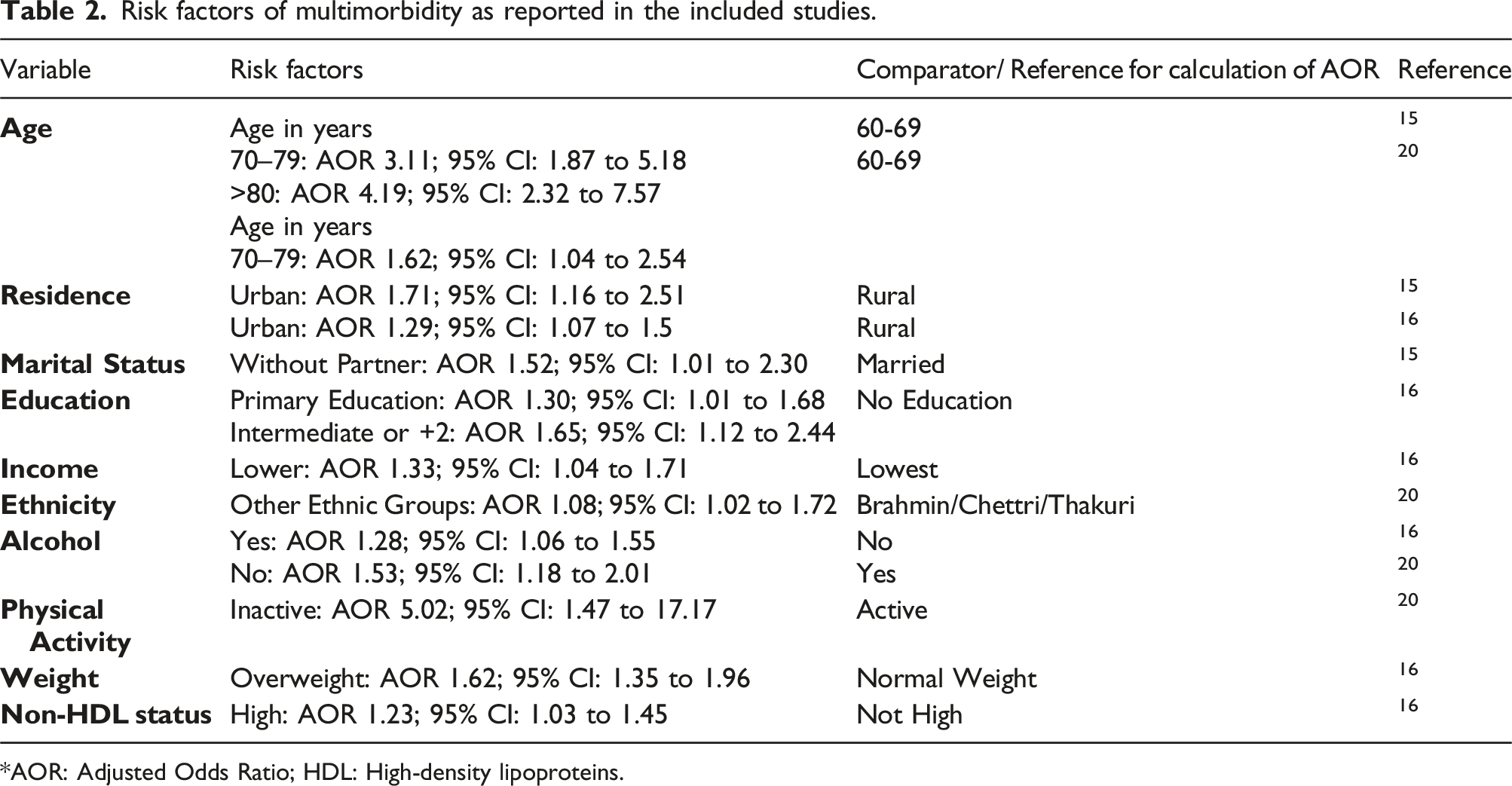
*AOR: Adjusted Odds Ratio; HDL: High-density lipoproteins.
Outcome/consequences
The outcomes/consequences were reported by only one study which highlighted that the multimorbid individuals had a higher risk of utilizing health services [AOR: 6.16 (95% CI: 3.31 to 11.46)] as compared to those who did not have any morbidity. 19
Discussion
Summary of evidence
In this systematic review of multimorbidity in Nepal, the prevalence of multimorbidity ranged from 13.96% to 70.1% with a pooled prevalence of 25%. The most commonly occurring dyad of chronic conditions was hypertension + diabetes mellitus. The major correlates of increasing levels of multimorbidity identified were increasing age, and urban residence. Additionally, fewer years of education, lower income levels, lack of physical activity, and overweight were also identified as risk factors of multimorbidity. Multimorbidity was associated with a higher risk of utilizing health services. There were no standard tools to assess multimorbidity with substantial heterogeneity in the included number of conditions to estimate multimorbidity.
Comparison with existing literature
The pooled prevalence of multimorbidity was observed to be around 25% which is comparable with the pooled prevalence reported [29.7% (95% CI: 26.4 to 33.0)] in a systematic review of multimorbidity among community dwelling adults of LMICs 22 (which did not include any studies from Nepal). Moreover, a systematic review conducted to estimate the burden of multimorbidity in South Asia reported its prevalence to range from 4.5% to 83% which is similar (13.96% to 70.1%) to the findings of the present review. 23 A recent meta-analysis reported the pooled prevalence of multimorbidty to be around 20% (95% CI: 19% to 20%) in India which is lower than the prevalence observed in Nepal. 24 A study conducted among adults aged >20 years in urban India and Pakistan reported the prevalence of multimorbidity to be around 9.4% 25 while another study among Bangladeshi adults aged >35 years reported the burden of multiple long term conditions to be 8.4%. 26 Hence, our findings indicate that the burden of multimorbidity in Nepal is comparable with other LMICs.
We observed that the studies included did not use standard tools to assess multimorbidity. Moreover, the number of conditions used to assess multimorbidity varied with studies considering as low as only four conditions to a maximum of nine conditions which is less than the findings of a recent systematic review based on 566 multimorbidity studies that observed the median number of conditions included to be 17 (IQR: 11-23). 27 Although there is no consensus on the minimum number of conditions being considered to assess multimorbidity, lesser number of conditions may clearly undermine the true prevalence. 28 A systematic review reported that the prevalence was severely underestimated if studies used a list of fewer than 12 chronic conditions, while less variation existed in studies using more than 12 conditions. 29 Here, it is worth noting that the pooled prevalence estimated in our meta-analysis could also be undermined due to inclusion of only four to nine conditions in the assessment of multimorbidity. Nonetheless, future studies should endeavor to use standard multimorbidity assessment tools that may help in estimating the real burden of disease and also make the findings comparable with other countries.
We identified hypertension + diabetes to the most commonly occurring dyad which is similar to the findings of a systematic review that reported the most frequently observed dyad comprised of the combination of a cardiovascular and metabolic diseases. 30 This further strengthens our opinion that the epidemiological and demographic shift in a small low-income country like Nepal is comparable to that of other LMICs and high-income countries. This cannot be overlooked; rather this evidence should be used to inform future policy decisions to form guideline for prevention and management of multimorbidty in Nepal.
We observed that the risk of multimorbidity increased with a rise in age, which is consistent with previous studies. 31 Chronic conditions commonly manifest in midlife (earlier in LMICs) and accumulate with advancing age. 32 It is likely that multimorbidity could be delayed or prevented by adopting lifestyle changes earlier in the life-course. 33 Additionally, this review also identified factors such as lack of physical activity and overweight to be associated with multimorbidity which is also similar to the findings of a systematic review that observed low levels of physical activity to be associated with a higher risk of having multmorbidity. 34 Another systematic review of longitudinal studies observed that the risk of multimorbidity increased [RR: 1.26; 95% CI: 1.12-1.40] amongst the overweight which also supports the findings of the present review. 35 Therefore, lifestyle changes such as undertaking physical activity, less salt and refined sugar in diet, abstinence from tobacco and alcohol, and avoiding unhealthy diet may be helpful in preventing multimorbidity. Moreover, in countries like Nepal joint-families (extended families with more than two generations living in a household) are common and hence family-centred interventions may be better placed to mitigate multimorbidity. 36
We observed urban residents had a higher chance of having multimorbidity than their rural counterparts. A probable reason for this could be difference in the availability and accessibility of healthcare resources, along with change in dietary habits (more processed food), and lack of physical activity among urban residents.10,37 In rural areas, these services are either not available or far off due to hilly terrains which may lead to delay in diagnosis and hence reporting of multimorbidity. 10 However, in urban areas, health facilities are better equipped with availability of clinicians and nurses that majorly lack in rural areas of Nepal 10 . Thus, there is an urgent need to strengthen primary care in rural areas of Nepal which is the key to achieve universal health coverage through equitable and affordable health services for all. Furthermore, this review also observed healthcare utilization to be associated with multimorbidity which is consistent with the reports of a systematic review of studies from 16 European countries that reported increased healthcare utilization in terms of doctor visits and hospitalizations. 38
We observed lesser years of education as a risk factor of multimorbidity which is consistent with the findings of a systematic review of studies from Southeast Asia that reported low education attainment to be associated with multimorbidity. 39 Health literacy and behavior change communication should focus on this population as it will help in making them aware to prevent the risk factors. Additionally, our systematic review also observed lower income levels as a correlate of multimorbidity which is also similar to the findings of another systematic review that observed increasing deprivation to be consistently associated with a rise in multimorbidity. 40 These individuals should be the special focus for government programmes as the social security net (provision of free and equitable healthcare services) will enable them to get timely diagnosis and treatment. Moreover, health assurance plans should target these individuals in order to prevent them from impoverishment due to bearing higher healthcare costs. Moreover, this will also help them in seeking continuity of care as it is critical for multimorbidity management.
Implications for policy, practice, and research
We observed the studies were limited to a few regions of Nepal that necessitates future nation-wide studies to assess multimorbidity. Moreover, the existing studies used neither standard tools nor uniform number of conditions in the assessment of multimorbidity. Here, it is worth noting that tools such as Multimorbidity Assessment Questionnaire for Primary Care (MAQ-PC) developed and validated in India (a country similar to Nepal) that aim to assess multimorbidity may be used to undertake future studies. 41 The social determinants of multimorbidity that are common across LMICs must be carefully addressed.42,43 These include special care for ageing population, those residing in rural areas, and people with lesser education levels. Community based care models may be implemented for older adults so that they are not dependent on the care givers/ family members for receiving continuity of care. Healthcare facilities especially primary care should be strengthened in rural areas so that healthcare facilities are easily accessible for masses. Additionally, complementary systems of medicine may also be explored and further strengthened so that healthcare facilities penetrate to each strata of the society. 44 Behavioral change communication (BCC) may play a major role in understanding the risk factors of multimorbidity that include alcohol, lack of physical activity, overweight, and high HDL levels. Here, it is worth noting that BCC may also be useful for individuals who are less educated as they could be made aware about the importance of timely availing healthcare facilities. BCC activities must consider social and lingual context so that it penetrates among masses. Future studies may consider prioritizing vulnerable populations such as tribal, urban poor and other ethnic groups. 45
Strengths and limitations
This is the first review to provide comprehensive evidence on multimorbidity in Nepal. However, we summarized the studies specifically describing “multimorbidity”, and there may be other evidence on prevalence of multiple long term conditions in Nepal but not labeled as “multimorbidity” which has not been captured. Moreover, prospectively registered protocol, and screening and data extraction by two independent reviewers are additional strength of this review. We performed meta-analysis to synthesize the prevalence of multimorbidity, but repetition in data did not allow us to include all the available studies. Another drawback of the study is that it is restricted to Nepal only but, Nepal being a LMIC requires this evidence to guide policy decisions for future. Nonetheless, this review identifies a large gap in the multimorbidity research in Nepal with very few and sparse studies.
Conclusion
The prevalence of multimorbidity was observed to be comparable with other similar LMICs that cannot be overlooked. Moreover, there was a lack of uniform multimorbidity assessment tool/conditions considered for assessing multimorbidity were heterogeneous in nature that calls for using standard tools for assessing multimorbidity in future. Additionally, it is imperative to assess national-level estimates of multimorbidity along with intervention studies in future.
Supplemental Material
Supplemental Material - Epidemiology of multimorbidity in Nepal: A systematic review and meta-analysis
Supplemental Material for Epidemiology of multimorbidity in Nepal: A systematic review and meta-analysis by Abhinav Sinha, S. Shradha Suman, Narayan Subedi, Krushna Chandra Sahoo, Mukesh Poudel, Arohi Chauhan, Banamber Sahoo, Marjan van den Akker, David Weller, Stewart W Mercer, and Sanghamitra Pati in Journal of Multimorbidity and Comorbidity
Footnotes
Acknowledgements
We thank the authors of the included studies who were kind enough to answer all our queries (through email) that arose during data extraction process.
Author’s contributions
Concept and design: AS, NS and SP. Acquisition, analysis, or interpretation of data: AS, SSS, KCS, BS and NS. Drafting of the manuscript: AS, KCS, NS, and SP. Critical revision of the manuscript for important intellectual content: AC, MP, SWM, DW, and MvdA. Statistical analysis: AS, SSS and KCS. Administrative and technical support: BS. Supervision: SP and SWM. All authors have agreed on publishing the final version of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
All data underlying this research will be made available on reasonable request to the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.