
Abstract
Background:
Pre-eclampsia is a hypertensive disorder of pregnancy and a major cause of maternal and neonatal mortality worldwide, with a disproportionately high burden in sub-Saharan Africa.
Objective:
This review synthesised evidence on how men engage with pre-eclampsia in the region.
Design:
This systematic review included qualitative designs and cross-sectional studies.
Data sources and methods:
Search was done across five primary databases (PubMed, Scopus, Embase, CINAHL and Web of Science). Additional searches were carried out in online sources like institutional repositories, HINARI, Dimensions AI and Google Scholar for studies published between 2000 and 2025. This review followed PRISMA guidelines and the Joanna Briggs Institute (JBI) framework. Data were appraised using JBI tools and synthesised thematically.
Results:
Twelve studies from Tanzania, Uganda, Ghana, Nigeria and Mozambique were included. Knowledge of pre-eclampsia varied widely; that is, only 24.8% of men demonstrated high awareness, while misconceptions, such as attributing the condition to stress, cold or supernatural forces, were common. Men’s roles spanned financial provision, decision-making, emotional and household support and information sharing, but overall involvement was moderate. Perceptions were shaped by cultural, social and spiritual narratives, while health system barriers such as unclear roles and exclusionary practices reduced engagement.
Conclusion:
Male partners’ knowledge, perceptions and roles significantly affect maternal outcomes in sub-Saharan Africa. Findings show the need for targeted education, culturally sensitive interventions and health system reforms that encourage male participation. Strengthening men’s engagement could reduce delays in care-seeking, improve antenatal care utilisation and contribute to lowering maternal and neonatal mortality.
Trial registration:
Open Science Framework with the DOI: https://doi.org/10.17605/OSF.IO/WHB93.
Plain language summary
This review looked at how men in sub-Saharan Africa understand and support women with pre-eclampsia, a dangerous pregnancy condition that can lead to death if not treated. Based on studies from five countries, many men had limited or incorrect knowledge about the condition, often linking it to stress or supernatural causes. While men did provide support like money, help at home, or making health decisions, their involvement was often unclear or limited due to cultural beliefs and health systems that left them out. Educating men and including them more in pregnancy care could help save the lives of mothers and babies.
Introduction
Pregnancy is often celebrated as a period of anticipation and hope, yet for millions of women worldwide, it can be overshadowed by the silent threat of pre-eclampsia (PE). This is a hypertensive disorder of pregnancy and a leading contributor to maternal and perinatal morbidity and mortality worldwide, affecting approximately 2%–8% of pregnancies globally.1,2 It is associated with severe complications, including preterm birth, foetal growth restriction, placental abruption and maternal organ dysfunction, and accounts for an estimated 76,000 maternal and 500,000 foetal or neonatal deaths annually. 3 The issue is particularly acute in sub-Saharan Africa, where maternal mortality due to pre-eclampsia is disproportionately high. Estimates indicate that hypertensive disorders contribute to nearly 10%–15% of maternal deaths in the region, compared to 2%–5% in high-income countries.4,5
In high-income countries, progress in screening, antenatal care (ANC) and emergency obstetric interventions has significantly reduced the toll of pre-eclampsia. Guidelines advocate for early detection through regular blood pressure and proteinuria monitoring, as well as risk-based preventive measures such as low-dose aspirin and calcium supplementation. 6 Planned early delivery, especially in cases of severe or late preterm pre-eclampsia, has been shown to improve maternal outcomes while balancing neonatal risks. 5 Moreover, advances in simulation-based medical education and emergency response protocols have improved the management of acute complications like eclampsia and Hemolysis, elevated liver enzymes, low platelet count (HELLP) syndrome. 7 However, even in these well-resourced settings, pre-eclampsia remains a significant contributor to maternal deaths and is associated with lifelong cardiovascular complications for both mothers and their offspring. 8 The challenge, however, becomes exponentially more pressing when the lens is shifted to low- and middle-income countries (LMICs), particularly those in sub-Saharan Africa. Multiple systemic barriers explain this burden, that is, limited access to ANC, late recognition of symptoms, delays in referral, shortages of essential drugs such as magnesium sulfate and inadequate health infrastructure for emergency obstetric care.4,9 Even when women recognise symptoms such as headaches, visual disturbances, or swelling, sociocultural beliefs, gender dynamics and health system inefficiencies frequently delay timely care-seeking. 10 For many families, health-seeking decisions are further shaped by cultural narratives and pluralistic health practices, where biomedical care intersects with prayer, traditional remedies and community perceptions of illness. 9
While the scientific and clinical dimensions of pre-eclampsia are well documented, the social and relational contexts surrounding the condition are equally critical to maternal outcomes. In many parts of sub-Saharan Africa, men, particularly husbands or partners, play a decisive role in health-seeking behaviour, access to resources and the utilisation of healthcare services during pregnancy. Yet, their knowledge of pre-eclampsia, perceptions of its risks and practical role in supporting affected women remain poorly understood and inconsistently addressed within maternal health programs. Evidence shows that women’s ability to seek care promptly is often mediated by their partner’s recognition of warning signs, willingness to prioritise medical attention over cultural remedies and financial capacity to support facility-based care.9,10 Moreover, the paternal contribution to pre-eclampsia is not only social but also biological. Research indicates that paternal genes and immunological interactions between father and mother may influence the risk of pre-eclampsia, suggesting that men’s involvement in reproductive health should be framed beyond cultural or supportive roles to include biomedical relevance. 11
Despite this, the literature on pre-eclampsia in sub-Saharan Africa has historically centred on biomedical interventions, maternal knowledge and health system barriers, often sidelining men’s perspectives. Few studies have systematically synthesised how male partners understand pre-eclampsia, how they engage in decision-making and how their attitudes may facilitate or obstruct timely care. Yet, as global health increasingly acknowledges the importance of male involvement in maternal and child health, this gap becomes particularly striking. This systematic review therefore seeks to synthesise existing qualitative and quantitative evidence on the knowledge, role and perceptions of male partners regarding pre-eclampsia in sub-Saharan Africa.
Methods
This review was conducted in line with the systematic review reporting framework outlined by Aromataris and Pearson 12 and endorsed by the Joanna Briggs Institute (JBI). The framework emphasises the following steps: (1) formulating a precise objective and research question, (2) establishing explicit inclusion and exclusion criteria, (3) employing a comprehensive search strategy, (4) critically appraising the quality of eligible studies, (5) extracting and analysing relevant data, (6) synthesising and presenting the findings and (7) ensuring transparency in the reporting process. In addition, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 13 guidelines were applied to document and present the search outcomes (Supplemental File). The protocol for this meta-ethnographic synthesis was registered with OSF (Open Science Framework) with the DOI: https://doi.org/10.17605/OSF.IO/WHB93 to avoid duplication and establish methodological accountability.
Research question
What is the knowledge and role of male partners on pre-eclampsia?
What is the perception of male partners on pre-eclampsia?
This research question was defined using the Population, phenomenon of interest and context framework (PICo). Population: male partners; Phenomenon of interest: knowledge, role and perception of male partners on pre-eclampsia; Context: sub-Saharan Africa.
Inclusion and exclusion criteria
The inclusion and exclusion criteria were established to ensure the selection of studies relevant to the review question. These criteria were guided by the Population, Concept and Context (PCC) framework outlined by Aromataris and Pearson. 12 A summary of the specific inclusion and exclusion parameters is provided in Table 1.
Inclusion and exclusion criteria.

Search strategy
Relevant studies were retrieved from five primary databases: Scopus, PubMed, Embase, CINAHL (Cumulative Index to Nursing and Allied Health Literature) and Web of Science. In collaboration with a chartered librarian, a comprehensive search strategy was designed using controlled vocabulary such as Medical Subject Headings (MeSH), along with keywords identified through an initial scoping search. The detailed, complete search process in all five databases is presented in Table 2. To supplement this, additional searches were carried out in online sources such as institutional repositories, Health InterNetwork Access to Research Initiative (HINARI), Dimensions AI and Google Scholar. Furthermore, reference lists of included studies were manually screened to identify additional relevant literature. The search was limited to studies published online from the year 2000 onwards. The last search was conducted on September 8, 2025.
Search strategy for selected databases.

CINAHL, Cumulative Index to Nursing and Allied Health Literature.
Study selection
All retrieved studies were imported into Mendeley Reference Manager version 1.19.8 for duplicate removal (https://static.mendeley.com/md-stitch/releases/live/20210125_v1_19_8.4e71755a.html). Subsequently, titles and abstracts of the remaining records were screened for potential eligibility by five trained graduate students, under supervision, using the predefined inclusion and exclusion criteria outlined in Table 1. Reference lists of eligible full-text studies were also reviewed to identify additional relevant records. For abstracts without accessible full texts, corresponding authors were contacted to obtain copies. Full-text screening of eligible studies was then conducted independently by two researchers, with any disagreements resolved through consultation with a third reviewer.
Data extraction
Data were extracted from the included studies using a pre-designed extraction form developed in Microsoft Word. To ensure reliability, the form was piloted with five randomly selected articles before full data extraction commenced. The authors were divided into two groups, with each group independently conducting the extraction process. Information retrieved included the author, year of publication, study location, design, sample size, as well as male partners’ knowledge, roles and perceptions regarding pre-eclampsia. The extracted data were cross-checked by E.J. and S.E.B., and any discrepancies were resolved through discussion with C.A. See Supplemental file for details of the extracted data.
Critical quality assessment
Quality appraisal of the included studies was carried out after data extraction using the standardised tools developed by the JBI. The purpose of this process was to evaluate and report the methodological quality of the studies rather than to exclude any of them. The JBI tools provide checklists tailored to different study designs, including cross-sectional, cohort, quasi-experimental, case-control and case-series studies. For cross-sectional studies, scores of 1–4 indicated high risk, 5–6 moderate risk and 7–8 low risk. Qualitative studies were rated as high risk (1–5), moderate risk (6–7) and low risk (8–10). The appraisals were independently conducted by E.J. and S.E.B., and it was supervised by C.A. See Supplemental Appendix for quality appraisal scores for the included studies.
Data analysis and synthesis
A thematic analysis was undertaken to explore and interpret patterns within the extracted data. This process involved systematic coding and categorisation to identify recurring themes related to male partners’ knowledge, roles and perceptions of pre-eclampsia. The analysis began with familiarisation through repeated reading of the extracted data to ensure a comprehensive understanding. Initial codes were then developed to label meaningful segments linked to the key concepts, which were subsequently grouped into potential themes. These themes were refined through iterative review and discussion among the research team to ensure accuracy and consistency of interpretation. A thematic framework was created to visually represent the relationships between the identified themes.
For data synthesis, a convergent qualitative approach was employed to integrate and interpret findings across the included studies. This involved systematically comparing and contrasting thematic results to highlight both commonalities and differences across varying study designs and contexts. Through an iterative process of reflection and dialogue, the research team generated overarching themes and sub-themes that captured the depth and diversity of male partners’ perspectives on pre-eclampsia. Emphasis was placed on maintaining transparency and rigour while ensuring the synthesis addressed the review question. This integrated perspective provides evidence with practical and policy relevance for enhancing educational strategies and outcomes.
Results
Search results
The initial search yielded 1132 records, of which 1082 were retrieved from electronic databases (PubMed, Web of Science, Scopus, CINAHL and Embase) and 50 from other sources. After removing 1048 duplicates, 94 records were retained for screening. Screening of titles and abstracts led to the exclusion of 65 records that did not meet the inclusion criteria, leaving 29 records for full-text review. Reference list checks of eligible studies identified four additional records, bringing the total number of full-text articles assessed to 23. Of these, 11 were excluded: 5 for targeting an ineligible population, 4 because full texts could not be accessed and 2 for being published in languages other than English. Finally, 12 studies met all inclusion criteria and were incorporated into the qualitative synthesis. See Figure 1 for the search result and the screening process.

PRISMA flow diagram of records and screening process.
Characteristics of the included studies
A total of 12 studies published between 2013 and 2025 were included (Figure 3), representing research from five sub-Saharan African countries. Tanzania contributed the largest share (5; 41.7%), followed by Uganda (2; 16.7%), Ghana (2; 16.7%), Nigeria (2; 16.7%) and Mozambique (1; 8.3%; Figure 2). The evidence base was evenly split between qualitative designs (6; 50.0%) and cross-sectional studies (6; 50.0%; Figure 4). Qualitative studies explored perceptions, experiences and contextual factors,14–19 while cross-sectional designs examined associations and descriptive outcomes.20–25

Global distribution of the included studies.

Year of publication of the included studies.
Study designs employed by included studies.
Quality appraisal results of included studies
Of the 12 included studies, 6 (50.0%) were assessed as low risk of bias, while the remaining 6 (50.0%) were rated as moderate risk, based on the JBI appraisal tools applied to each design. The low-risk studies comprised all 6/6 qualitative designs (100%).14–19 The moderate-risk group consisted of all 6/6 cross-sectional studies (100%).20–25
Across the cross-sectional studies, methodological quality was consistently rated as moderate risk (100%). While most studies clearly outlined their inclusion criteria, applied appropriate sampling methods and measured exposures with reasonable accuracy, none adequately identified or adjusted for confounding factors. Strategies such as regression adjustment, stratification or sensitivity analyses were absent across all six studies, thereby weakening causal inferences and introducing uncertainty in interpreting associations. Additionally, limited detail was provided regarding the validity and reliability of measurement instruments, further contributing to their moderate-risk designation.
By contrast, all six qualitative studies were rated as low risk of bias (100%), consistently scoring 8/10 on the JBI checklist. Strengths included strong alignment between research questions, study designs and data collection methods. Most demonstrated rich contextual descriptions, clear thematic analysis and findings supported with direct participant quotations, enhancing credibility and transferability. However, a shared limitation was the limited consideration of reflexivity, with few studies critically examining the role of researcher influence or power dynamics in shaping the data. Despite this, their overall methodological coherence and transparency positioned them as robust contributions to the evidence base.
Review findings
Knowledge of male partners about pre-eclampsia
The reviewed studies reveal wide variability in male partners’ knowledge of pre-eclampsia and related maternal health conditions, with implications for their involvement in antenatal and postnatal care (PNC). Evidence suggests that in some contexts, men demonstrate relatively high awareness. Doe 20 reported that 63% of men had good knowledge of pregnancy care, which significantly influenced their participation in ANC, PNC and newborn care. Similarly, Quarcoo and Tarkang 21 found that although only 24.8% of male partners possessed high knowledge of maternal health issues, this subgroup was four times more likely to be involved in maternal health compared to those with lower knowledge (Adjusted Odds Ratio (AOR) = 4.14, p = 0.002). Yussuf et al. 19 demonstrated that 43.5% of male partners and 44.5% of pregnant women had adequate knowledge of pre-eclampsia/eclampsia (PE/E). This level of awareness was positively associated with ANC utilisation, with adequate knowledge more than doubling the likelihood of attendance (AOR = 2.827, 95% CI: 1.719–4.651, p < 0.001).
In contrast, other studies highlight persistent gaps and misconceptions. The majority of men had limited knowledge of maternal health, 21 while nearly half of male partners held strong myths about PE/E, which significantly reduced ANC attendance. 24 Misinterpretations of the condition were also common, as Falade-Fatila and Adebayo 23 reported that men perceived pre-eclampsia as stress-induced and eclampsia as a result of cold exposure. Likewise, Boene et al. 17 found that the terms pre-eclampsia and eclampsia were largely unknown, and symptoms were instead explained through local cultural beliefs (Table 3).
Knowledge of male partners about pre-eclampsia.
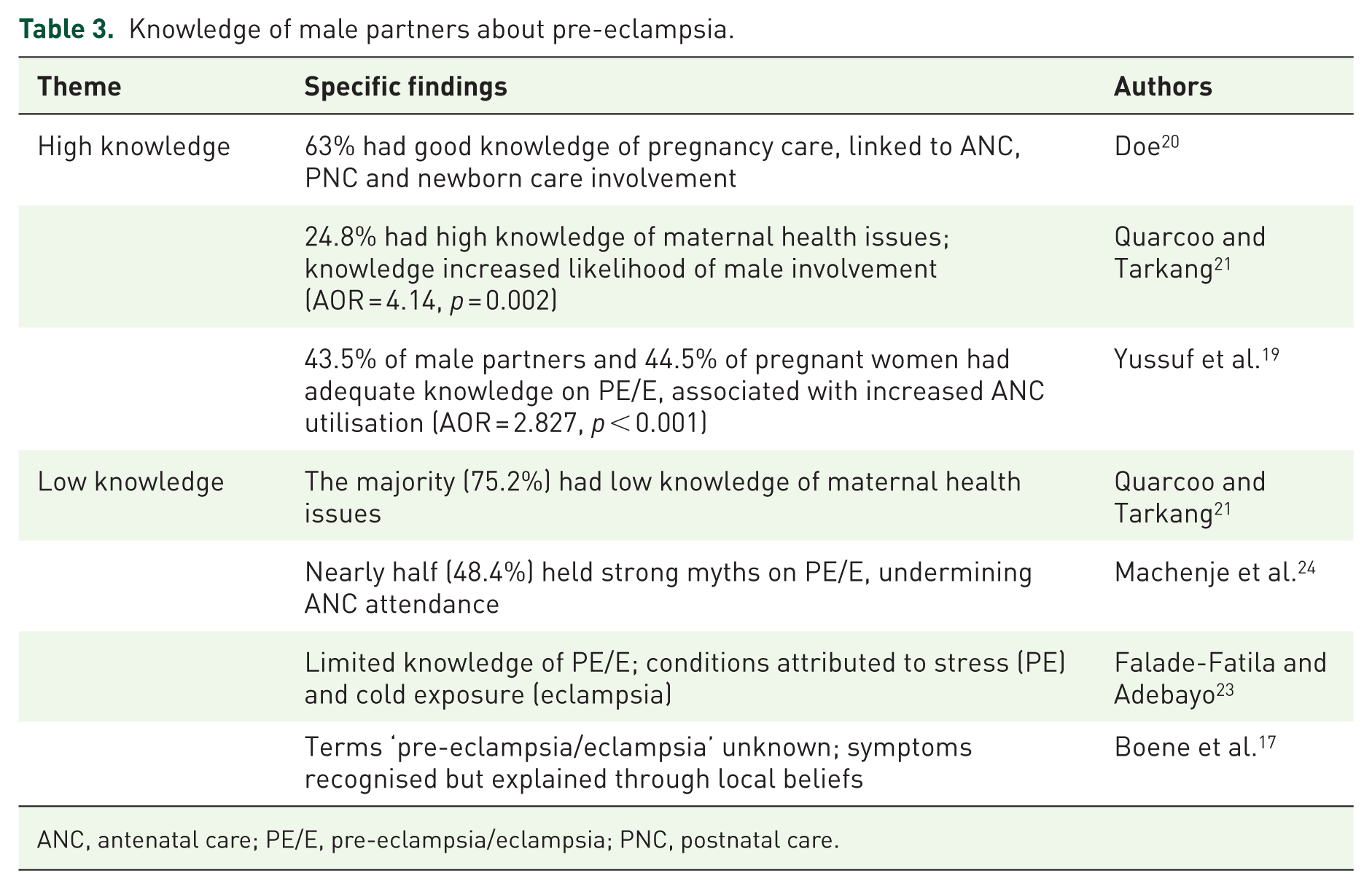
ANC, antenatal care; PE/E, pre-eclampsia/eclampsia; PNC, postnatal care.
Role of male partners in pre-eclampsia
The studies consistently demonstrate that male partners play diverse and complementary roles in supporting women at risk of pre-eclampsia. Across financial, decision-making, emotional, household and informational domains, their involvement significantly influences maternal care engagement and outcomes. Financially, male partners frequently facilitate access to antenatal, delivery and postnatal services by providing essential funds and covering costs associated with emergencies or complications.22,23 Such support reduces delays in care-seeking, showing the importance of economic involvement in maternal health. Decision-making roles were similarly prominent. Partners often determine the place of delivery, select healthcare providers and make critical choices during pregnancy-related complications, reflecting both practical and authoritative influence within households. 22 Their engagement in these decisions is closely linked to timely care utilisation and preparedness for obstetric emergencies.
Beyond finances and decisions, emotional and social support emerged as a key facilitator of maternal well-being. Presence during labour, reassurance and ongoing encouragement were associated with reduced anxiety and improved maternal confidence, highlighting the psychosocial dimension of male involvement.23,25 Complementing this, household support, such as assisting with domestic tasks, enabled women to conserve energy and prioritise health appointments. Importantly, informational roles shaped the quality of engagement. Male partners who were aware of maternal responsibilities and health risks guided participation in ANC and PNC, facilitated effective spousal communication and helped navigate health-related information.20,21 Knowledgeable partners were therefore better positioned to contribute meaningfully across all domains (Table 4).
Role of male partners in pre-eclampsia.
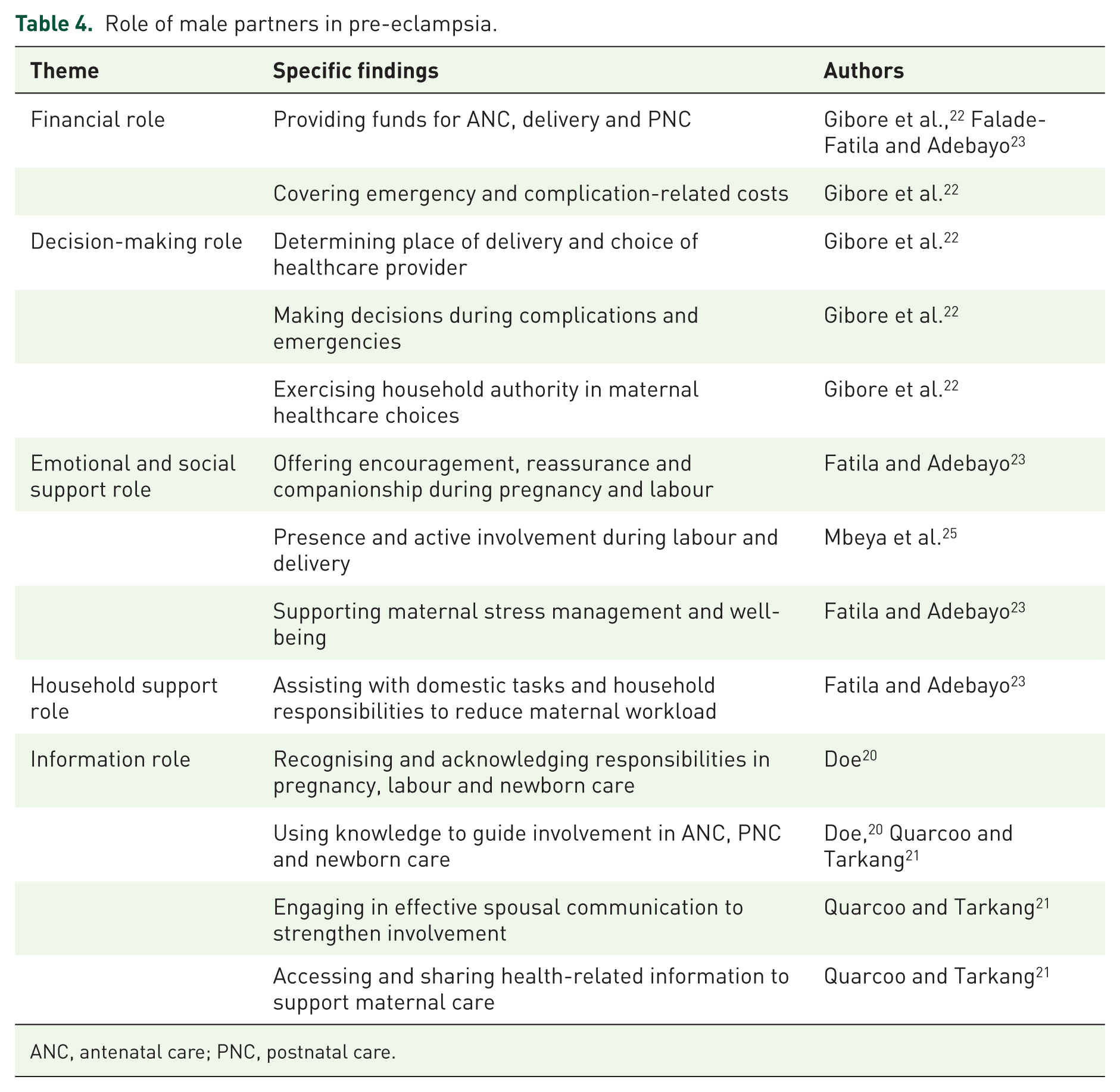
ANC, antenatal care; PNC, postnatal care.
Perceptions of male partners on pre-eclampsia
Male partners’ perceptions of pre-eclampsia (PE/E) were shaped by a combination of medical knowledge, cultural beliefs, social roles and spiritual interpretations. Across the studies, limited biomedical understanding emerged as a significant barrier to effective involvement. Men often demonstrated minimal awareness of PE/E and frequently attributed its occurrence to stress, environmental factors or other non-medical causes.15,16 The linkage between biomedical causes and clinical manifestations of PE/E was weakly understood, compounded by poor access to healthcare services and structural barriers within the health system. Men reported feeling alienated in hospital settings, and their roles in maternal care were often unclear, resulting in minimal participation during pregnancy and childbirth.14,18
Cultural explanations also strongly influenced male perceptions. Some men associated PE/E with marital discord or mistreatment, reflecting a broader social interpretation of illness that prioritises relational and environmental stressors over medical causation.16,17 Cultural beliefs further reinforced these non-biomedical interpretations, shaping how men engaged, or did not engage, with formal healthcare services. 18 Social norms additionally framed men’s understanding and involvement. Male partners frequently perceived their responsibility as a formal obligation rather than an active partnership in maternal health, suggesting that societal expectations of gendered roles limited both emotional and practical engagement. 14
Finally, spiritual and traditional beliefs are prominent in shaping perceptions. In several contexts, PE/E was viewed as a consequence of supernatural forces, such as snake illness or disturbances linked to the moon, highlighting the persistence of mystical explanations alongside biomedical interpretations (Table 5).15,17
Perceptions of male partners on pre-eclampsia.

PE/E, pre-eclampsia/eclampsia.
Discussion
Summary of findings
The synthesis of evidence shows that male partners’ knowledge, perceptions and roles in maternal health are highly variable, often influenced by cultural norms, healthcare system barriers and access to information. Knowledge among men was generally low to moderate. Only 24.8% of men demonstrated high knowledge of maternal health issues, although a majority (83.9%) recognised that male involvement is important. Awareness of pre-eclampsia and eclampsia was limited, with 43.5% of men and 44.5% of women having adequate knowledge. Misconceptions were common: 51.6% of participants held weak myths, while 48.4% held strong myths about these conditions. Importantly, men with higher knowledge were four times more likely to be actively involved in maternal health (AOR = 4.14, p = 0.002), and adequate knowledge of pre-eclampsia and eclampsia almost tripled the likelihood of attending ANC (AOR = 2.827, 95% CI: 1.719–4.651, p < 0.001). Conversely, participants with weak myths were significantly less likely to attend ANC (AOR = 0.370, 95% CI: 0.229, p < 0.001).
Perceptions of maternal health were shaped by cultural beliefs and systemic challenges. Many men viewed involvement as an obligation rather than a choice, yet unclear roles, alienation in healthcare settings and limited access to biomedical information constrained engagement. Traditional and spiritual explanations for conditions such as eclampsia persisted, leading some men to rely on non-biomedical remedies and potentially delay timely care. Male partners played diverse roles, including financial support, decision-making, management of obstetric complications, birth preparedness and household assistance. Engagement varied across the continuum of care: 26.4% of men had high involvement, 55.2% moderate and 18.4% low, with the highest participation observed during labour and delivery. Studies consistently showed that men with better knowledge participated more in antenatal visits, birth preparedness and newborn care.
Knowledge of male partners about pre-eclampsia
Male partners’ knowledge of pre-eclampsia and related maternal health conditions is important in shaping their involvement in pregnancy care and the utilisation of antenatal and postnatal services. Across the reviewed studies, knowledge levels varied widely, reflecting differences in access to health information, exposure to formal health education, and prevailing social and cultural belief systems. Evidence from several studies indicates that higher levels of knowledge among male partners are associated with more positive maternal health behaviours. Doe 20 reported that 63% of male partners had good knowledge of pregnancy care, which was significantly linked to their involvement in ANC, PNC and newborn care. This suggests that informed male partners are more likely to provide practical and emotional support throughout the continuum of care. Similarly, Quarcoo and Tarkang 21 found that although only 24.8% of men demonstrated high knowledge of maternal health, this group was substantially more engaged in maternal health decision-making, being four times more likely to participate compared with men who had lower knowledge levels (AOR = 4.14, p = 0.002). In another study, Yussuf et al. 19 showed that 43.5% of male partners had adequate knowledge of PE/E, and this level of awareness was strongly associated with increased ANC utilisation (AOR = 2.827, 95% CI: 1.719–4.651, p < 0.001). Collectively, these findings indicate that knowledge enhances men’s capacity to recognise the seriousness of PE, support timely care-seeking and encourage adherence to clinical recommendations.10,11
Despite these positive patterns, the review also highlights substantial and persistent knowledge gaps. In some studies, the majority of male partners had a limited understanding of maternal health issues. Quarcoo and Tarkang 21 reported that 75.2% of men had low knowledge of maternal health, while Machenje et al. 24 found that nearly half of male partners held strong myths about PE/E, which significantly reduced ANC attendance. Such misconceptions may lead men to underestimate the severity of symptoms or discourage engagement with formal healthcare services, thereby increasing the risk of delayed diagnosis and management. Misinterpretations of PE/E were particularly evident in studies describing traditional and spiritual explanations for pregnancy complications. Falade-Fatila and Adebayo 23 reported that pre-eclampsia was often attributed to stress, while eclampsia was believed to result from exposure to cold. Similarly, Boene et al. 17 observed that the biomedical terms ‘pre-eclampsia’ and ‘eclampsia’ were largely unfamiliar, with symptoms explained through local belief systems. In such contexts, complications may be interpreted as spiritual afflictions or social problems, leading families to prioritise prayer, traditional remedies or community advice before seeking biomedical care. This reliance on non-medical explanations can delay presentation at health facilities, particularly when early warning signs are not recognised as indicators of a life-threatening condition.9,10
The contrast between high and low knowledge highlights the dual role of male partners’ awareness in maternal healthcare. Adequate knowledge acts as a facilitator, enabling men to support informed decision-making, encourage service utilisation and respond appropriately to obstetric emergencies. In contrast, low knowledge and entrenched misconceptions function as barriers, limiting male involvement and contributing to delays in care-seeking. These findings point to the need for targeted educational interventions that explicitly include male partners, address common myths and integrate culturally sensitive explanations of PE/E and its warning signs.1,9
Role of male partners in pre-eclampsia
The involvement of male partners in maternal health, particularly in the prevention and management of pre-eclampsia, is increasingly recognised as a determinant of maternal and neonatal outcomes. Findings from the reviewed studies indicate that men contribute to maternal care across multiple and interrelated domains, including financial provision, decision-making, emotional and social support, household assistance and information sharing. Financial support consistently emerged as a central and foundational role of male partners. Across several studies, men were reported to provide funds for ANC, delivery and PNC, as well as covering costs associated with emergencies and pregnancy-related complications.22,23 In many low- and middle-income settings, out-of-pocket payments remain a major barrier to accessing skilled maternal healthcare. When male partners are financially prepared and willing to support care-seeking, delays in diagnosis and treatment of pre-eclampsia can be reduced. This is particularly important given that early identification and timely management are central to preventing severe maternal and neonatal complications.1,2 Decision-making represents another prominent domain of male involvement. The findings indicate that male partners often determine the place of delivery, select healthcare providers and make urgent decisions during pregnancy-related complications. 22 In many settings, men hold significant authority within households, and their approval can strongly influence whether and when women seek care. Active participation in decision-making can therefore support timely referral, adherence to clinical advice and preparedness for obstetric emergencies. This is particularly relevant for pre-eclampsia, where rapid progression and unpredictable onset require prompt and informed responses. 11 Evidence also suggests that shared decision-making between partners strengthens trust in healthcare providers and promotes consistent engagement with recommended care pathways. 10
Beyond financial and decision-making roles, emotional and social support emerged as a vital component of male partner involvement. Reassurance, encouragement and companionship during pregnancy and labour were associated with reduced maternal anxiety and improved confidence, particularly among women experiencing high-risk pregnancies.23,25 Emotional support is especially important in the context of pre-eclampsia, which is often accompanied by fear, uncertainty and prolonged monitoring or hospitalisation. Chronic stress and anxiety have been linked to poorer maternal health outcomes and may exacerbate hypertensive disorders during pregnancy. 9 Household support further complements these roles by addressing the physical demands placed on pregnant women. Assisting with domestic tasks and household responsibilities reduces maternal workload and allows women to rest, attend health appointments and follow treatment plans more effectively. 23 This form of support reflects a shift away from traditional gender norms that limit male involvement to financial provision alone. In the context of pre-eclampsia, reduced physical strain may be particularly beneficial, as rest and regular monitoring are often advised as part of clinical management.
Informational support constitutes another key domain of male involvement. Male partners who are knowledgeable about pregnancy risks, early warning signs of pre-eclampsia and appropriate health-seeking behaviours play an important role in facilitating engagement with ANC and PNC services.20,21 Effective spousal communication enhances shared understanding of symptoms such as severe headaches, visual disturbances or swelling, which are critical indicators of disease progression. Knowledgeable partners are also better positioned to recognise the urgency of these symptoms and support timely care-seeking. 1 However, the influence of spiritual and traditional beliefs can sometimes complicate care-seeking behaviours. In some contexts, symptoms of pre-eclampsia may be interpreted as spiritual afflictions or attributed to supernatural causes, leading families to prioritise prayer, traditional remedies or spiritual consultations before seeking biomedical care. 9 Male partners are often important in endorsing or challenging these beliefs. When men favour traditional or spiritual explanations, this may delay presentation at health facilities and increase the risk of severe complications. Conversely, informed male partners who understand the medical nature of pre-eclampsia can help counter these delays by supporting prompt referral and adherence to clinical advice.
Perceptions of male partners on pre-eclampsia
Understanding male partners’ perceptions of pre-eclampsia (PE/E) is central to improving maternal health outcomes, particularly in LMICs where men often play a decisive role in healthcare access and decision-making. Across the reviewed studies, men’s knowledge, beliefs and socially defined roles consistently shaped how they understood PE/E, how they responded to symptoms, and the extent to which they supported their partners during pregnancy.14–16,18 Most studies reported that many men had little awareness of the condition and struggled to recognise it as a serious medical complication of pregnancy. PE/E was frequently explained as a result of stress, environmental exposure or lifestyle factors rather than underlying physiological processes.15,16 This weak understanding of biomedical causation was often accompanied by limited recognition of warning signs, such as headaches, swelling or high blood pressure. As a result, symptoms were sometimes normalised or underestimated, increasing the risk of delayed care-seeking and reduced adherence to medical advice. Health system factors further constrained men’s involvement. Several studies reported that male partners felt uncertain about their roles within maternal healthcare and perceived antenatal and delivery services as spaces primarily designed for women.14,18 Feelings of alienation in hospital settings, combined with limited opportunities to participate in consultations or decision-making, reduced men’s engagement. Poor access to healthcare services, logistical barriers and inadequate communication from health professionals reinforced these challenges.
Cultural interpretations are also important in shaping perceptions of PE/E. In some contexts, men associated the condition with marital conflict, mistreatment or relational stress, reflecting a broader understanding of illness that prioritises social harmony and interpersonal relationships over biomedical explanations.16,17 Cultural norms often legitimised these interpretations, framing maternal complications as consequences of social or environmental imbalance. Such beliefs influenced how danger signs were interpreted and whether formal healthcare was sought, with some men favouring culturally familiar remedies or home-based responses rather than immediate hospital care. 18 Social norms around gender and responsibility further shaped male involvement. Responsibility for maternal health was frequently viewed as an obligation rather than a shared partnership. Men commonly defined their role in terms of financial provision or logistical support, while emotional engagement and shared decision-making were less emphasised. 14 This gendered framing limited open communication between partners about pregnancy risks and reduced men’s active participation in recognising symptoms or advocating for timely care.
Spiritual and traditional beliefs were also central to how PE/E was understood. In several studies, the condition was interpreted as a spiritual or supernatural problem, attributed to forces such as ‘snake illness’, witchcraft or lunar disturbances.15,17 These beliefs often shaped care-seeking behaviour by directing families towards traditional healers, prayer or ritual practices as initial responses. For example, symptoms of PE/E might be managed through spiritual consultations or herbal treatments before biomedical care is considered. This sequence of care can delay hospital presentation, particularly when symptoms are believed to require spiritual resolution rather than medical intervention.9,10
Implications for policy, practice and public health education
The synthesis of evidence shows that male partners’ limited knowledge, cultural perceptions and varying engagement in maternal health have profound implications for policy, clinical practice and public health education. The low levels of knowledge and pervasive myths surrounding pre-eclampsia and eclampsia highlight the urgent need for strategies that formally integrate men into maternal health programs. Policymakers should consider frameworks that not only encourage male participation but also explicitly define their roles across antenatal, labour and PNC. Clear policies could address systemic barriers, such as hospital environments that inadvertently alienate men, ensuring that healthcare facilities become inclusive spaces where men are welcomed and empowered to participate meaningfully. The findings also suggest that healthcare providers need to actively engage male partners through targeted counselling, education and joint consultations. Men who are well-informed about maternal health complications, such as pre-eclampsia and eclampsia, are significantly more likely to support timely healthcare-seeking and participate in critical maternal and newborn care activities. Therefore, integrating structured male-inclusive education sessions into routine antenatal and postnatal visits could enhance their understanding and confidence, promoting shared decision-making and stronger household support for maternal care.
Community outreach programs, media campaigns and peer-education initiatives can help address traditional beliefs and spiritual interpretations that may delay care. Emphasising the practical roles of men, including financial support, birth preparedness and emotional care, can reinforce positive engagement. Furthermore, improving spousal communication and encouraging joint participation in maternal health decisions can strengthen household-level health behaviours, ultimately contributing to better maternal and neonatal outcomes.
Limitations in this review
This systematic review included twelve studies published between 2013 and 2025, offering a useful but geographically restricted evidence base on male involvement in maternal health. The studies were drawn from only five sub-Saharan African countries, with a clear concentration in a small number of settings. Tanzania accounted for the largest share of included studies, followed by Uganda, Ghana, Nigeria and Mozambique. This uneven geographic distribution limits the extent to which the findings can be generalised beyond these contexts. Male involvement in maternal health is strongly shaped by sociocultural norms, health system structures and policy environments, which vary widely across regions. Consequently, the predominance of evidence from a few countries may not fully reflect experiences in other parts of sub-Saharan Africa or in non-African settings. Language restrictions further constrain the breadth of the evidence. All included studies were published in English, which may have resulted in the exclusion of relevant research reported in local languages or non-English journals, particularly from francophone or lusophone African countries. This introduces a potential language bias and may contribute to the observed regional imbalance in the literature. Methodologically, the review included an equal number of cross-sectional and qualitative studies. Cross-sectional studies primarily quantified levels of knowledge, involvement and attitudes, but their design limits causal interpretation. While qualitative studies provided rich insights into perceptions, lived experiences and sociocultural influences on male engagement, several lacked explicit reflexivity regarding researcher positionality, which may influence interpretation. Although the mixed-methods approach allowed for triangulation, the dominance of descriptive designs restricts conclusions about effectiveness or long-term impact.
Recommendation for future studies
The growing body of research on male partners’ knowledge, roles and perceptions regarding pre-eclampsia in sub-Saharan Africa paints a compelling yet incomplete picture of male involvement in maternal health. While existing studies provide valuable insights into how men engage with pregnancy, childbirth and PNC, the evidence reveals significant gaps that future research must address to inform effective interventions. Most of the quantitative evidence comes from cross-sectional surveys, capturing knowledge levels and reported involvement at a single point in time. While informative, these snapshots cannot explain how male engagement evolves throughout pregnancy and beyond. Longitudinal research could follow men from early ANC through postnatal support, offering a dynamic view of participation and identifying the factors that sustain or hinder involvement. Intervention studies, meanwhile, could test programs designed to improve male knowledge of pre-eclampsia, address cultural barriers and strengthen practical support for maternal care. Measuring the impact of such interventions would provide actionable evidence for policymakers and health practitioners.
Additionally, future studies should prioritise robust measurement and rigorous reporting, including standardised tools for knowledge and involvement, careful control of confounding variables and reflexive discussion in qualitative work. Engaging men, women, healthcare providers and community leaders will ensure culturally sensitive, practical and sustainable strategies. Strengthening this evidence base will be key to promoting meaningful male participation, ultimately improving maternal and neonatal health outcomes across sub-Saharan Africa. Finally, current studies are heavily concentrated in Tanzania, Nigeria and Ghana, leaving many sub-Saharan contexts unexplored. Future research should aim for broader, multi-country studies, capturing diverse sociocultural and linguistic settings. This would ensure that findings are both relevant and transferable, avoiding overgeneralisation from a limited number of countries.
Conclusion
The findings from the included studies suggest that male partners’ knowledge, perceptions and engagement are central to maternal and neonatal health outcomes. Evidence indicates that knowledge levels are generally low, with only 24.8% of men demonstrating high awareness of maternal health issues and 43.5% having an adequate understanding of pre-eclampsia and eclampsia. Misconceptions and reliance on traditional or spiritual explanations are widespread, often delaying timely care and undermining antenatal and postnatal interventions. Men with higher knowledge were four times more likely to be actively involved in maternal health (AOR = 4.14, p = 0.002), and an adequate understanding of pre-eclampsia and eclampsia nearly tripled the likelihood of ANC attendance (AOR = 2.827, 95% CI: 1.719–4.651, p < 0.001). Barriers such as unclear roles, cultural beliefs, poor spousal communication and alienating healthcare environments further limit male participation. Conversely, access to accurate information, inclusive healthcare practices and culturally sensitive education facilitates active engagement, leading to improved maternal care-seeking, birth preparedness and newborn support. Male roles include decision-making, financial support, management of complications and household assistance, yet overall engagement remains moderate (26.4% high involvement, 55.2% moderate, 18.4% low).
These findings emphasise that male involvement is not peripheral but essential. Policymakers, healthcare providers and public health educators should focus on empowering men with knowledge, addressing misconceptions and creating supportive healthcare environments. Future research should investigate culturally tailored interventions, long-term outcomes of male engagement and strategies to enhance household-level support. Collectively, strengthening male participation has the potential to reduce maternal morbidity and mortality, foster shared responsibility and promote healthier families and communities.
Supplemental Material
sj-doc-1-reh-10.1177_26334941261432063 – Supplemental material for Knowledge, role and perceptions of male partners on pre-eclampsia in sub-Saharan Africa: a systematic review of evidence from qualitative and quantitative studies
Supplemental material, sj-doc-1-reh-10.1177_26334941261432063 for Knowledge, role and perceptions of male partners on pre-eclampsia in sub-Saharan Africa: a systematic review of evidence from qualitative and quantitative studies by Christiana Asiedu, Emmanuella Florence Odi Asiedu, Eunice Johnson and Sarah Esi Bilson in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941261432063 – Supplemental material for Knowledge, role and perceptions of male partners on pre-eclampsia in sub-Saharan Africa: a systematic review of evidence from qualitative and quantitative studies
Supplemental material, sj-docx-2-reh-10.1177_26334941261432063 for Knowledge, role and perceptions of male partners on pre-eclampsia in sub-Saharan Africa: a systematic review of evidence from qualitative and quantitative studies by Christiana Asiedu, Emmanuella Florence Odi Asiedu, Eunice Johnson and Sarah Esi Bilson in Therapeutic Advances in Reproductive Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.