
Abstract
Background:
High fertility rates and low infant mortality hurt maternal and child health and increase child dependency ratios, leading to poor economic development, low standards of living and low educational attainment. Despite efforts over the years, Ghana’s fertility rates have declined at a rate lower than the global average. Using the multi-indicator cluster survey (MICS) data, we analysed the factors associated with three fertility dimensions: parity, high fertility and the desire for more children in Ghana.
Objective:
The study aimed to investigate the factors associated with parity, high fertility and the desire for another child in Ghana.
Design:
The MICS are cross-sectional, nationally representative surveys that employ a multi-stage, stratified cluster sampling approach to select sample units.
Methods:
The data for this study were obtained from the 2017 to 2018 Multiple Indicator Cluster Survey (MICS) conducted in Ghana. Three outcome variables – parity, high fertility and the desire for another child – were defined. The explanatory variables consisted of respondents’ sociodemographic and economic variables. The sample consisted of 11,228 women. We employed descriptive statistics, logistic regression and the generalised Poisson regression for the data analysis.
Results:
Factors that are negatively associated with parity and high fertility include higher educational level, frequency of watching television, being insured and computer use. Residing in an urban location, being older, being in a higher wealth quintile (compared to the poorest) and the frequency of listening to the radio are all positively related to parity and being in a high-fertility zone. Women who have attained a higher level than middle/JHS, the older ones and those who are insured tend to desire another child.
Conclusion:
The study found that educational level, media (television) exposure, insurance uptake and computer use are associated with a lower likelihood of having fewer children, while being in a union, residing in an urban location, being older, having higher wealth and exposure to radio are associated with parity and being in a high-fertility zone. Our study contributes to a deeper understanding of the drivers of fertility and the desire for more children in the context of low- and middle-income countries.
Introduction
As of 2020, the fertility rate in sub-Saharan Africa (SSA) was 4.5, accounting for 50% of the global fertility. 1 Historically, developed and developing nations have exhibited a noticeable difference in fertility rates, with developing nations experiencing considerably higher rates, averaging 5.42 births per woman, compared to an average of 2.15 births per woman in developed countries. Recently, fertility decline has been noticed in SSA, albeit at a slow pace and shaped by traditional and contemporary factors. 2 It is argued that the slow fertility transition in SSA, including Ghana, is attributed to a lack of demand among Africans to limit family size due to distinct family structures and economic conditions. In addition, religious attitudes towards fertility play a crucial role in influencing both family economics and the acceptability of various forms of fertility control. 3 Although studies exist in SSA, there is still no consensus on the effect of these traditional and contemporary factors.1,2,4,5 They are dynamic, and their influence on fertility changes over time.
In a multi-country study of 32 countries in SSA, the desire for children was found to be low among women aged 45–49, those with higher education and those whose partners had higher education, compared to women aged 15–19, those with no formal education and those whose partners had no formal education, respectively. Findings from a scoping review of 258 studies in SSA from 1990 to 2021, which included men and/or women aged 15–49 years, grouped the determinants of the desire for more children into economic value and costs of children, marriage, mortality and health, education and status, and demographic predictors. Recent evidence in Ethiopia suggests that the desire for a (another) child is lower for women aged 15–24 and 25–34 compared to women in the 35–49 age group, and that the desire for more children is higher for women without formal education or primary education compared to those who attain higher levels of education. 5
The 2022 Ghana Demographic and Health Survey (GDHS) reports an average fertility rate for women aged 15–49 years of 3.9 (4.8 for rural areas and 3.2 for urban centres). 6 Many factors continue to influence fertility in Ghana. A recent piece of qualitative evidence in Ghana has identified the rising cost of children, the need to ensure comfortable lives for children, women’s participation in the labour market and access to modern contraceptives as factors leading to the desire for fewer children. 7 Although women’s education is associated with reduced fertility rates and delayed marriage in Ghana, the effect varies depending on the economic status of the household and whether the neighbourhood is urban or rural. 8 In Ghana, females who married at a young age experienced reduced educational achievement, greater adherence to patriarchal gender norms and decreased autonomy within their households. 8
In a panel study using three waves (2003, 2008 and 2014) of the GDHS, which restricted the sample to women currently married or living in a union and aged 45–49, the evidence shows that underachieved fertility increased from 25.1% in 2003 to 35.8% in 2014, supporting the idea that fertility rates have reduced in SSA. 9 Nevertheless, in the same study, it was observed that achieved fertility increased from 23.8% in 2003 to 26.0% in 2014, while overachieved fertility decreased from 51.1% in 2003 to 38.2% in 2014, highlighting the fact that overachieved fertility (or high fertility) remains a significant problem in Ghana. In a pooled sample (1993–2014) of the GDHS analysis to determine the predictors of overachieved and underachieved fertility, it came to light that 44% of women had overachieved (had high fertility) with significant predictors such as a partner wanting more children, experiencing child loss and being married more than once. 10 On the other hand, 36% had underachieved fertility with factors such as having a partner with fewer fertility preferences, being of the Islamic faith and women who had ever used modern contraceptives.
The slow decline in fertility rates in SSA, including Ghana, compared to global rates, remains to be fully understood. Globally, there is a consensus that high fertility rates, in addition to reductions in infant mortality, will negatively impact maternal and child health and increase child dependency ratios, leading to poor economic development, low standards of living and low educational attainment. 11 Yet, a recent report by the United Nations Population Fund 12 highlights a growing concern that the fertility rates in many OECD countries are declining below sustainable levels and could lead to population collapse. Studying the drivers of fertility, in general, and, in particular, the desire for more children, is crucial for understanding population dynamics in this changing world. Such studies will also inform effective development policies that ensure an inclusive, prosperous and sustainable future without threatening the existence of humanity.13,14 Using nationally representative data (the multi-indicator cluster survey – MICS), we analyse the factors associated with parity, high fertility and the desire for more children in Ghana. Our study contributes to a further understanding of the drivers of fertility and the desire for more children in a low- and middle-income country context. This is crucial for policymakers in developing sustainable population policies.
Methodology
Data source and sampling technique
The data for this study were obtained from the 2017 to 2018 Multiple Indicator Cluster Survey (MICS) conducted in Ghana. The MICS are cross-sectional, nationally representative surveys that measure countries’ health indicators to inform policies, programmes and national development plans. A multi-stage, stratified cluster sampling approach was used to select the MICS sample units. Further details on the MICS sampling design and techniques can be obtained from https://mics.unicef.org/surveys. This study considered a sample of 11,228 women.
Outcome variables
The study employed three outcome variables: parity (measured as the number of children ever born), high fertility (if the number of children is above the average fertility rate of approximately 4 in Ghana) and the desire for another child, with a binary response of ‘yes’ or ‘no’. Examining the factors related to parity (general fertility rate) is crucial in understanding how women make fertility decisions. However, for policy purposes, we dichotomised the number of children born based on the national average fertility rate to understand the factors associated with giving birth to more than this national average. Such an analysis will inform policymakers in targeting desirable population growth rates for sustainable development. The third variable sought to understand the factors related to the desire for more children. Such an understanding is crucial in developing policies that support women’s access to fertility services.
Explanatory variables
The explanatory variables and their levels of measurement used for both models are as follows: educational level (none, primary, middle/junior secondary school, secondary, higher), currently married/living with a man (yes, no), place of residence (urban, rural), age (in years), wealth quintile (poorest, second, middle, fourth, richest), frequency of listening to the radio (not at all, less than once a week, at least once a week, almost every day), frequency of watching TV (not at all, less than once a week, at least once a week, almost every day), covered by health insurance (yes, no) and ever used a computer/tablet (yes, no).
Data analyses
The data were analysed using descriptive statistics, logistic regression and the generalised Poisson regression. Frequencies and percentages of all the socio-economic and demographic characteristics (excluding age), desire for more children and whether a woman exceeds the national fertility rate of 4 were computed, whilst the average (mean), minimum and maximum were obtained for age and number of children ever born.
Logistic regression (see equation (1)) was used to analyse factors related to the desire for one more child and high fertility (whether a woman exceeds the national fertility rate of 4). This stems from the fact that both variables are dichotomous, hence, taking the value 1 with a probability of success ϑ, or the value 0 with the probability of failure

where α = the constant of the equation and β = the coefficient of the predictor variables. An alternative form of the logistic regression equation is:
Coefficients for the model are tested for significance using the Wald test, the likelihood ratio test (16).
The number of children ever born to a woman is a count variable. The idea is to identify the socio-economic and demographic factors that may influence one’s level of parity using the number of children ever born. Hence, the number of children ever born is estimated using the Poisson model, which is derived based on the standard Poisson distribution. 16
Let

Logarithmic transformation linearises the distribution, implying that it has a logarithm as its link function. The logarithm of the outcome variable is thus a linear function of the predictors, which consist of the socio-economic and demographic factors, among others, as shown in equation (4).

where
The basic count regression model is the Poisson regression, which assumes that the mean and variance of the outcome are equal. Our data, however, exhibited underdispersion (mean = 2.805, standard deviation = 2.436) for the outcome. This violates the assumption of equal dispersion for the simple Poisson model. As a result, we employed the generalised Poisson regression, 17 which is correct for the underdispersion. We calculated the incidence risk ratios (IRR) and the 95% confidence intervals (95% CI). All analyses were performed using STATA version 15. 18
Results
Figure 1 presents the distribution of the outcome variables. The graphs show that the number of children ever born follows the Poisson distribution, whilst the graphs for the desire for another child and high fertility follow the binary logistic distribution.
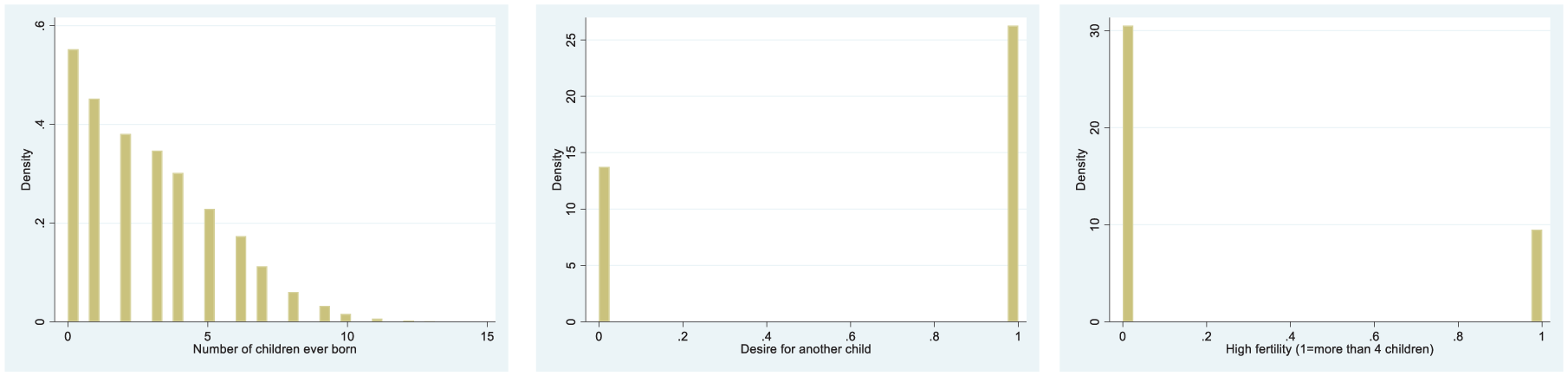
Distribution graphs of outcome variables.
Table 1 presents the results on the socio-economic and demographic characteristics of the respondents, categorised by the outcome variables.
Socio-economic and demographic characteristics of respondents by outcome variables.

The background characteristics of respondents are presented in the Supplemental File. The results in Table 1 show that, on average, women with no formal education had approximately five children, those who attained primary education had about three, and those who attained middle school education had about two. Those who attained secondary education or higher had about one child. When considering parity across wealth quintiles, we noticed that, on average, the poorest had more children (4) compared to the richest (2). In terms of marital status, individuals who are married or in a union have more children (approximately 4) compared to those who are not married or in a union (1). Again, those located in rural areas had more children (3) than those in urban areas. Regarding media exposure, women without exposure had more children than those who did. For example, women who did not listen to the radio at all and those who tuned in at least once a week had approximately three children, compared to those who listened at least once a week or almost every day. This observation is similar when considering the frequency of watching television. On average, there seems to be no difference in childbearing between the insured and uninsured. However, women who had never used a computer or a tablet had more children (3) compared to those who had ever used one (1).
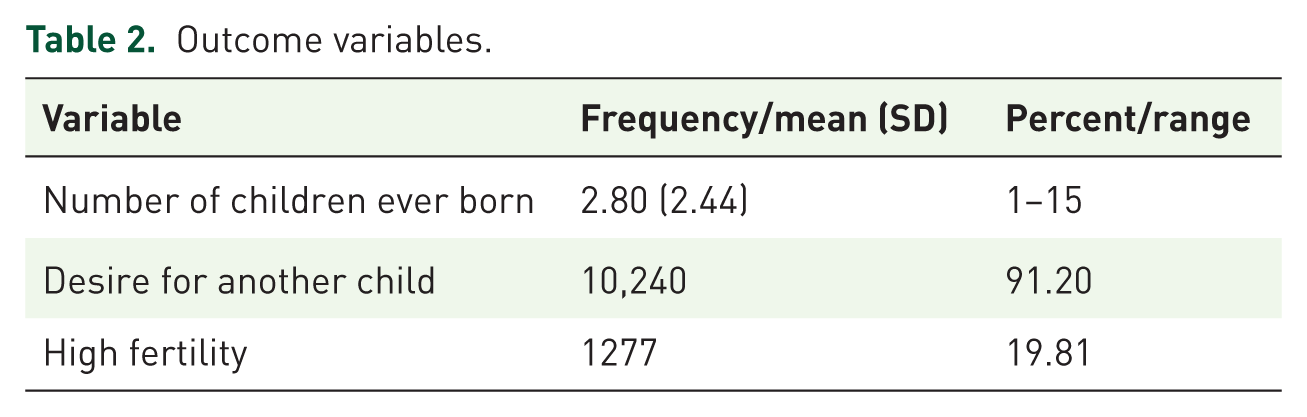
The results also reveal that women without formal education and those from low-income backgrounds are in the high-fertility zone specifically (Table 2).
Outcome variables.
Factors associated with fertility and desire for more children
The results on the factors related to parity, high fertility and the desire for another child are presented in Table 3. From the results, factors related to parity include educational level, location, age, wealth, frequency of listening to the radio and television, as well as computer use. We found that women who have attained formal education tend to give birth to fewer children compared to those with no formal education. For example, the chance of giving birth to more children significantly reduces for those who attained primary level education (IRR = 0.81; 95% CI = 0.77–0.84), middle/JSS (IRR = 0.64; 95 CI = 0.61–0.66) and secondary or higher (IRR = 0.38; 95% CI = 0.37–0.41), compared to women without formal education. Similarly, compared to women who do not watch television at all, those who watch at least once a week (IRR = 0.88; 95% CI = 0.84–0.92) and almost every day (IRR = 0.86; 95% CI = 0.83–0.90) are less likely to have more children. The situation is the same for women covered by health insurance (IRR = 0.94; 95% CI = 0.91–0.97) and those who have ever used a computer (IRR = 0.66; 95% CI = 0.62–0.70). However, women in unions (IR = 2.16; 95% CI = 2.10–2.25), those located in urban areas (IRR = 1.04; 95% CI = 0.99–1.07) and older women (IRR = 1.05; 95% CI = 1.04–1.05) are more likely to bear more children. Similarly, compared to those in the poorest wealth quintile, those in the second (IRR = 1.107; 95% CI = 1.06–1.16), middle (IRR = 1.07; 95% CI = 1.02–1.13) and the richest (IRR = 1.08; 95% CI = 1.01–1.14) quintiles are more likely to give birth to more children. In like manner, compared to women who do not listen to the radio at all, those who listen less than once a week (IRR = 1.04; 95% CI = 1.06–1.16), at least once a week (IRR = 1.05; 95% CI = 1.01–1.09) and almost every day (IRR = 1.12; 95% CI = 1.08–1.16) are more likely to bear more children.
Socio-economic and demographic factors associated with parity, excess fertility and desire for another child.

***denotes significance at the 1% level; ** denotes significance at the 5% level; and * denotes significance at the 10% level.
IRR, incidence risk ratios.
Regarding factors related to high fertility, women who attained primary (AOR = 0.80, 95% CI = 0.68–0.94)), middle/JSS (AOR = 0.54; 95% CI = 0.47–0.63) and secondary or higher (AOR = 0.31; 95% CI = 0.0.23–0.41) levels are less likely to have more than four children compared to those without any formal education. Similarly, women in urban locations (AOR = 0.70; 95% CI = 0.61–0.82), covered by health insurance (AOR = 0.85; 95% CI = 0.76–0.96) and those who ever used a computer (0.59; 95% CI = 0.39–0.89), are less likely to give birth to more than the national average of four children. In like manner, compared to those in the poorest wealth quintile, those in the middle (AOR = 0.61; 95% CI = 0.49 − 0.75), fourth (AOR = 0.36; 95% CI = 0.28–0.47) and richest (AOR = 0.19; 95% CI = 0.15–0.25) quintiles are less likely to give birth more than four children. In terms of the effect of listening to the radio, compared to those who do not listen at all, those who listen at least once a week (AOR = 0.82; 95% CI = 0.69–0.98) and those who listen almost every day (AOR = 0.76; 95% CI = 0.65–0.88) are less likely to give birth to more than four children. However, older women (AOR = 1.22; 95% CI = 1.21–1.23) and women who are in a union or cohabiting with a male partner are more likely to have more than four children (IRR = 2.91; 95% CI = 2.46–3.42), compared to women who are not in a union. The frequency of watching television does not affect the likelihood of having more than four children.
When turning attention to the desire for another child, the results show that, compared to women who do not have any formal education, those who attained secondary level education or higher (AOR = 1.31; 95% CI = 1.08–1.59) and those in a union (AOR = 1.22; 95% CI = 1.09–1.36) are more likely to desire another child. Additionally, women who listen to the radio almost every day (AOR = 1.15; 95% CI = 1.02–1.31), compared to those who do not listen at all, and women covered by health insurance (AOR = 1.12; 95% CI = 1.02–1.24) have a higher likelihood of desiring another child. On the other hand, older women (AOR = 0.862; 95% CI = 0.86–0.87) and those in the second poorest wealth quintile (AOR = 0.82; 95% CI = 0.70–0.96) have a lower likelihood.
Discussion
Our study contributes to the discourse on population dynamics in a changing world, re-examining the effects of socio-demographic factors on fertility and the desire for another child, specifically in the context of low- and middle-income countries. We found that education, exposure to television, being located in an urban area, having health insurance, and computer use reduced the likelihood of having more children and being in a high-fertility zone. However, education and insurance increased the possibility of desiring another. Being in a union increased the chance of having more children, being in a high-fertility zone and desiring another child. While wealth increases the likelihood of having more children, it reduces the probability of being in a high-fertility zone, but does not affect the desire for another child.
These findings reveal several insights. First, while attaining higher education reduces the likelihood of having more children, as has been established in previous studies, the desire for another child increases with education.19,20 This observation of negative education effect on parity may be because women with advanced education typically possess enhanced access to family planning knowledge, prioritise professional advancement and financial security, and enter marriage at a later age. These factors facilitate educated reproductive choices, resulting in postponed childbirth and lower fertility rates. However, having attained higher education and increased their economic and social value, such women are probably finding it easier to care for another child. In a cross-sectional study in Iran, the authors found that subjective norms, perceived social support and marital satisfaction influenced childbearing intentions. 21 More so, education is found to be an important source of subjective norms (social status) globally, with differences being larger between educational groups. 22 Such a perceived increase in social status occasioned by educational attainment tends to encourage women to desire to have another child. In addition, education increases the social net worth and earnings of individuals, making it easier to care for another child. Our findings, which show that those on a higher wealth index tend to have more children, further validate this point. Our findings align with those of Guzzo and Hayford, 23 who found that among young adults in the United States, those with higher education levels exhibit a somewhat greater propensity to desire and plan for children, as well as a somewhat bigger anticipated family size. Yet, our findings contradict those of Muluneh and Moyehodie, 5 who conclude that the desire for more children is higher among women without formal education than among those who attain higher levels of education. Gyan and Kpoor 7 have identified the rising cost of children and the need to ensure comfortable lives for children as disincentives for the desire for fewer children. With more education, these constraints may no longer exist, hence increasing the desire for another child.
Being in a union with a male partner has a significant influence on reproductive outcomes and the desire to have another child. Yeboah et al. 10 confirm that fertility increased from 23.8% in 2003 to 26.0% in 2014 among women currently married or living in a union, as some partners desire more children, experience child loss, and are married more than once. In many societies in SSA, one common purpose of being in a union (married or cohabiting) is to procreate, to the extent that when a woman is unable to give birth, even for justifiable reasons, such women are stigmatised.24,25 It was therefore expected that, compared to women who are not in a union, women in a union would have more children and/or desire to have another child.
Our findings on the effect of location on fertility, albeit contradictory, are supported by the literature. The results show that women residing in urban locations were more likely to have more children but less likely to fall within the high-fertility zone, which means that these women did not have more than the national average of four children. Fertility heterogeneity across locations has been examined in many developed countries and in SSA.26–30 Our finding that those located in urban areas are more likely to have more children can be explained by findings in previous studies that the urban poor are more likely to experience fertility far above replacement levels.31,32 Similarly, our finding that those located in urban areas are less likely to have more than four children is supported by Yi and Shangguan, 33 who argue that Urban migrants typically embrace more conservative reproductive choices, such as reducing the probability of childbirth, postponing the age of first birth and extending intervals between births. 33
The age of a woman has a positive effect on fertility. This aligns even more with historical findings that younger persons demonstrate a heightened aspiration for parenthood and perceive it as possessing greater personal significance compared to older adults. 34 As women age, their reproductive ability diminishes. Fertility markedly diminishes with age, potentially diminishing the inclination or practicality of having more children. Moreover, advanced maternal age is frequently linked to increased health risks during pregnancy and labour for both the mother and the infant. This insight may dissuade women from desiring additional children as they age.
We found that frequently listening to the radio was associated with an increase in the number of children ever born. On the other hand, those who watch television more frequently are less likely to have more children. In the literature, media exposure is found to have a mixed effect on fertility. In one breath, media exposure, such as radio broadcasts, can markedly affect reproductive behaviour by increasing understanding and acceptability of contraceptive technologies, thereby reducing the number of children ever born.35,36 On the other hand, exposure to media that show maternal figures and depictions of beauty ideals has augmented the desired number of offspring throughout time. 37
Even though evidence from previous studies has shown that enhanced access to public health insurance substantially impacted the incidence of high-parity newborns, we found that health insurance uptake reduces the probability of having more children. 38 This seemingly unexpected relationship is confirmed by an earlier study, which examined the impact of social insurance on household fertility decisions. 39 In that study, it was found that the introduction of social health insurance in Ghana had a temporary pro-cyclical effect on fertility at the individual level. Still, no effect was observed in the more recent data. While insurance uptake can improve access to reproductive care and contraceptive use, thereby reducing fertility, it can also reduce the cost associated with seeking care during pregnancy and childbirth, thereby increasing fertility.
Conclusion and recommendations
The study highlights the relationship between socio-economic and demographic factors and three fertility parameters: the number of children ever born (parity), high fertility (defined as having more than four children) and the desire for another child among currently pregnant women. We employed generalised Poisson regression to analyse the factors related to the number of children ever born (parity) and logistic regression to analyse the factors associated with high fertility and a desire for another child. We found that education, exposure to television, being located in an urban area, having health insurance, and computer use reduced the likelihood of having more children and being in a high-fertility zone. However, education and insurance increased the possibility of desiring another. Being in a union increased the chance of having more children, being in a high-fertility zone and desiring another child. While wealth increases the likelihood of having more children, it reduces the probability of being in a high-fertility zone; however, it does not affect the desire for another child. By examining the drivers of fertility, our study contributes to the understanding of population dynamics in this changing world. It could also serve as a basis for future research on the emerging debate regarding sustainable or replacement-level fertility. Our findings that education, media (television) exposure, insurance uptake and computer use are related to the likelihood of having fewer children will inform effective development policies that ensure an inclusive, prosperous and sustainable future without threatening humanity’s existence. Given the slow decline in fertility in SSA amidst global fertility decline, our study contributes to a deeper understanding of the drivers of fertility and the desire for more children in a low- and middle-income country context. This is crucial for policymakers in developing sustainable population policies.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251372324 – Supplemental material for What factors influence fertility and the desire for more children in Ghana? Evidence from the multi-indicator cluster survey
Supplemental material, sj-docx-1-reh-10.1177_26334941251372324 for What factors influence fertility and the desire for more children in Ghana? Evidence from the multi-indicator cluster survey by Naasegnibe Kuunibe, Anthony Mwinilanaa Tampah-Naah and Lea Anzagra in Therapeutic Advances in Reproductive Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.