
Abstract
Obesity is a global issue. Despite efforts to confront it, the worldwide incidence of obesity continues to escalate [1]. The WHO estimates that approximately one billion people throughout the world are overweight and that over 300 million of these are obese. If current trends continue, the number of overweight persons will increase to 1.5 billion by the year 2015. The number of obese adults in Australia is estimated to have risen from 2 million in 1992 to 3.1 million in 2005 [2]. What contributes to the problem of obesity mainly stems from the imbalance between reduced exercise, overindulgence in energy-dense dietary intake, changing lifestyle and dietary composition. It has been known that obesity is related to systemic diseases such as diabetes mellitus, cardiovascular diseases, hyperlipidemia, sleep apnea, cancers and osteoarthritis.
Female obesity has a great impact on reproductive function and the hormonal milieu. As far back as 1934, the association between obesity and infertility was recognized when Irving Stein and Micheal Leventhal described a triad consisting of obesity, hirsutism and infertility: the ‘Stein–Leventhal Syndrome’ [3]. Overweight and obese women have more problems of menstrual irregularities, chronic or intermittent anovulation, infertility, signs of androgen excess, increased risk of miscarriages and hormone-sensitive carcinomas [4–6]. In the Million Women Study, it was noted that increasing BMI was associated with an increased incidence of endometrial carcinoma (relative risk [RR] = 2.89; 95% CI: 2.62–3.18). Obesity also has important implications for the delivery of obstetric care. It is well recognized that maternal obesity is associated with an increased risk of maternal, peripartum and neonatal complications [7].
Defining obesity
Total body fat can be measured precisely using skin fold thickness, underwater weighing, dual energy x-ray absorptiometry (DEXA), MRI and infrared spectroscopy [8]; however, its usage is limited for research purposes. In daily clinical use, more simple measures are used to assess the degree of obesity including BMI (Table 1), waist circumference (WC) and waist–hip ratio (WHR). Central adiposity is particularly important in clinical sequelae associated with an increased BMI. In both male and female sexes, obesity, and in particular, the abdominal obesity phenotype, may impair fertility. Generally, a WHR of more than 0.9 for men and more than 0.8 for women defines an increased risk of cardiovascular disease. Also, in women with a WHR of more than 0.8, it was noted that the RRS of irregular menstruation and oligomenorrhea were 1.56 and 2.29, respectively [10]. In a prospective cohort study on women attending infertility clinics and requiring donor insemination, a high WHR was associated with a markedly lower conception rate [11]. A unit increase of 0.1 in WHR led to a 30% decrease in probability of conception per cycle (hazard ratio: 0.76; 95% CI: 0.562–0.887) after adjustment for age, size, reasons for artificial insemination, cycle length and regularity, smoking and parity. Emerging scientific interest has increased our understanding of the main metabolic and hormonal factors involved in the pathophysiology of different obesity phenotypes. Although for a long time it was suggested that these alterations were secondary to obesity, it has recently become evident that they conversely play a role in the development of different obesity phenotypes and associated metabolic abnormalities [12].
Classification of overweight in adults according to BMI.

Adapted from [9].
Obesity & polycystic ovarian syndrome
Most obese women with infertility and signs or symptoms associated with androgen excess are affected by polycystic ovarian syndrome (PCOS), whose prevalence rates are suggested to be approximately 5–7% in western countries [13]. Prevalence of PCOS varies worldwide and this is mainly because different criteria are used for the diagnosis and there is also substantial heterogeneity of symptoms and signs among women with PCOS. Following a consensus held in Rotterdam, The Netherlands in 2003, an internationally accepted definition has been adopted by the European Society for Human Reproduction and Embryology and the American Society for Reproductive Medicine, known as the ESHRE/ASRM Rotterdam consensus [14]. Diagnosis of PCOS requires the presence of two of the following three diagnostic criteria:
Oligo- and/or an-ovulation
Clinical and/or biochemical evidence of hyperandrogenism
The presence of polycystic ovarian morphology on ultrasound
While the pathogenesis leading to the development of PCOS is not completely understood, it is increasingly recognized that in the majority of women with PCOS, insulin resistance and compensatory hyperinsulinemia plays an important role. Essentially, insulin resistance has a complex genetic and environment etiology. Insulin resistance appears to be selective with impaired glucose uptake, whilst other intracellular actions of insulin are preserved. At the ovarian level, by acting primarily through its own receptor and the IGF-1 receptor, insulin synergizes luteinizing hormone action and stimulates ovarian steroidogenesis both in thecal and granulosa cells [15]. Over a third to half of PCOS subjects are overweight or obese [16]. In PCOS women of Caucasian origin, it is noted that the severity of both metabolic and clinical symptoms is positively correlated with the BMI [16]. There is also evidence showing that even normal-weight PCOS women present with the abdominal phenotype of fat distribution [17]. Obesity acts as an amplifier of insulin resistance and hyperinsulinemia. The abdominal phenotype further worsens this. Obesity is therefore suggested as playing a specific pathophysiological role in the development of PCOS [18].
Obesity, menstrual disorders & infertility
The association between obesity and menstrual irregularities has been recognized. Obesity was present at a fourfold higher rate in women with menstrual irregularities compared with normally menstruating females [19]. Historical data from 26,638 women, aged 20–40 years, were used to study the association between obesity and menstrual abnormalities, including evidence of infertility. It was found that women with evidence of anovulatory cycles, in other words, irregular cycles greater than 36 days and hirsutism, were more than 30 lb (13.6 kg) heavier than women with no menstrual abnormalities after adjusting for height and age [19]. In adolescents and young women, the age of onset of obesity and that of menstrual irregularities are significantly correlated. In the 1958 British birth cohort, Lake
The link between obesity and infertility is complex. The available knowledge supports the concept that androgen alterations and their balance with estrogen represent the most important mechanism responsible for the development of subfertility or infertility in obese women. Sex hormone binding globulin (SHBG) is a protein carrier that binds testosterone and dihydrotestosterone with high affinity and estrogens with a lower affinity. The degree of obesity is inversely related to SHBG levels. In addition, body fat distribution further influences SHBG concentrations. Females with central adiposity have lower SHBG concentrations in comparison with peripheral obesity [22], therefore the percentage of free testosterone fraction tends to be higher in women with central obesity. In addition, the adipose tissue is a site of active androgen production, converting androgens into estrogens, and of androgen and estrogen inter-conversion, which largely depends on the amount of fat [22]. Increased androgen production and reduced binding of androgens to SHBG contribute to hyperandrogenism, resulting in anovulation through inhibition of follicular maturation.
Hormones regulating energy metabolism have been shown to exert different effects on several reproductive events. The roles of insulin and insulin-like growth factors have been studied extensively and are well known for their effects on reproductive events, such as ovarian steroidogenesis, folliculogenesis and ovulation physiology. Insulin resistance plays a key pathogenic role in PCOS, and insulin-sensitizing drugs are now widely used to induce ovulation and improve fertility in these women [23].
In addition to insulin, novel hormones, such as leptin, ghrelin, adiponectin, resistin and peptide YY3–36 have been discovered as important regulators of appetite and energy homeostasis [24,25]. The close relationship between energy metabolism, nutritional state and reproductive physiology suggests that disorders or alterations in nutritional state (obesity, malnutrition, anorexia nervosa and so on) and metabolic disturbances can disrupt the complex interplay of gonadotropins and gonadal hormones, which are essential for fertility. Recent research has demonstrated that leptin plays an integral role in the normal physiology of the reproductive system with complex interactions at all levels of the hypothalamic–pituitary–gonadal axis. Observational studies have demonstrated that levels of leptin excess, deficiency or resistance can be associated with abnormal reproductive function [26]. Increased body weight and fat tissue substantially disrupt menstrual pattern and fertility potential. In obese women, weight loss alone improves insulin resistance and promotes fertility.
In addition, expression of leptin, ghrelin and their receptors in various reproductive organs, such as the ovary, testis, endometrium, embryo and placenta, have been demonstrated to have important roles in different stages of embryo development and implantation [26,27].
The Nurses' Health Study in 1994 compared 2527 married nulliparous nurses unable to become pregnant for at least 1 year owing to ovulatory disorder with controls comprising of 46,718 married parous nurses with no history of infertility [28]. The risk of ovulatory infertility for women at different BMI levels at age 18 years was compared with that for women at 18 years whose BMI was 20–21.9 (median for the cohort). Logistic regression was used to adjust for other confounding variables. Multivariate relative risks for infertility were: 1.2 (BMI: <16), 1.1 (BMI: 16–17.9), 1.0 (BMI: 18–19.9), 1.0 (BMI: 20–21.9), 1.1 (BMI: 22–23.9), 1.3 (BMI: 24–25.9), 1.7 (BMI: 26–27.9), 2.4 (BMI: 28–29.9), 2.7 (BMI: 30–31.9) and 2.7 (BMI: >32). These findings suggested that an elevated BMI at age 18 years, even at levels lower than those considered to be obese, is a risk factor for subsequent ovulatory infertility. More recent data from this group show that ovulatory infertility can be largely attributed to overweight and sedentary lifestyle [29]. Recent data by Gesink Law
Obesity & infertility treatment
Most studies demonstrate conclusive evidence that increasing BMI is associated with an increased requirement of drugs to induce ovulation. Large doses of clomiphene of up to 200 mg per day were required to ensure ovulation in the heaviest women [31]. Similar trends were also observed in doses of gonadotrophins required to induce ovulation [32,33]. In a study of 335 women with WHO group ll anovulatory infertility [34], it was noted that with increasing BMI, a higher threshold dose of gonadotrophins was required (odds for needing a higher dose more than 75 IU was 1.47 [95% CI: 0.84–2.55] and 2.15 [95% CI: 1.17–3.94] for overweight and obese women, respectively) and there were more days of stimulation (OR: 1.8; 95% CI: 0.32–3.27 and OR: 2.91; 95% CI: 1.21–4.6) for overweight and obese women, respectively. In another study by Fedorcsak
The value of obesity as a predictor of infertility treatment outcome is controversial. While some studies reported a decrease in pregnancy and implantation rates in obese women [35–37], others reported no effects of extreme body weights [33,38]. Conflicting results may be related to the type of treatment, inconsistent definitions of obesity and smaller size of cohorts observed. In a study by Wang
There is evidence for an increased risk of miscarriage in obese women. Lashen
The poor reproductive performance in obese women, both in natural and assisted conception cycles, may be a result of a combination of lower implantation and pregnancy rates, higher preclinical and clinical miscarriage rates, and increased complications in pregnancy for both mother and fetus. These have been related to various endocrine and metabolic disturbances, such as effects on steroid metabolism and alterations in the secretion and action of insulin and other hormones, such as leptin, resistin, ghrelin and adiponectin [24], which may affect follicle growth, corpus luteum function, early embryo development, trophoblast function and endometrial receptivity.
The question remains as to the mechanism by which obesity may affect fecundity in women. Is it exclusively an ovarian effect, endometrial effect or a combined effect? The oocyte donation model is unique. By restricting study to oocytes donated by normal-weight women, the effect of obesity on oocyte development was eliminated, thus permitting an assessment of the extraovarian effect of excess bodyweight on successful pregnancy outcomes. However, data regarding the effects of BMI on the oocyte donation model are conflicting. While two authors observed no association between BMI, pregnancy rate and loss rate in oocyte donation cycles [42,43], others noted obesity to be an independent risk factor for miscarriage in women receiving donated oocytes [44,45]. Bellver
The ovary is not the only factor responsible for the poor reproductive outcome in obese patients: the endometrium or its environment also contributes to this discouraging prognosis, but in a more subtle manner. Thus, on the basis of many complications in pregnancies with obesity, it is justifiable to advise weight reduction in women contemplating pregnancy whether it is a cycle with their own oocyte or donated oocyte. The impact of obesity on reproduction is summarized in Table 2.
Impact of obesity on reproduction.
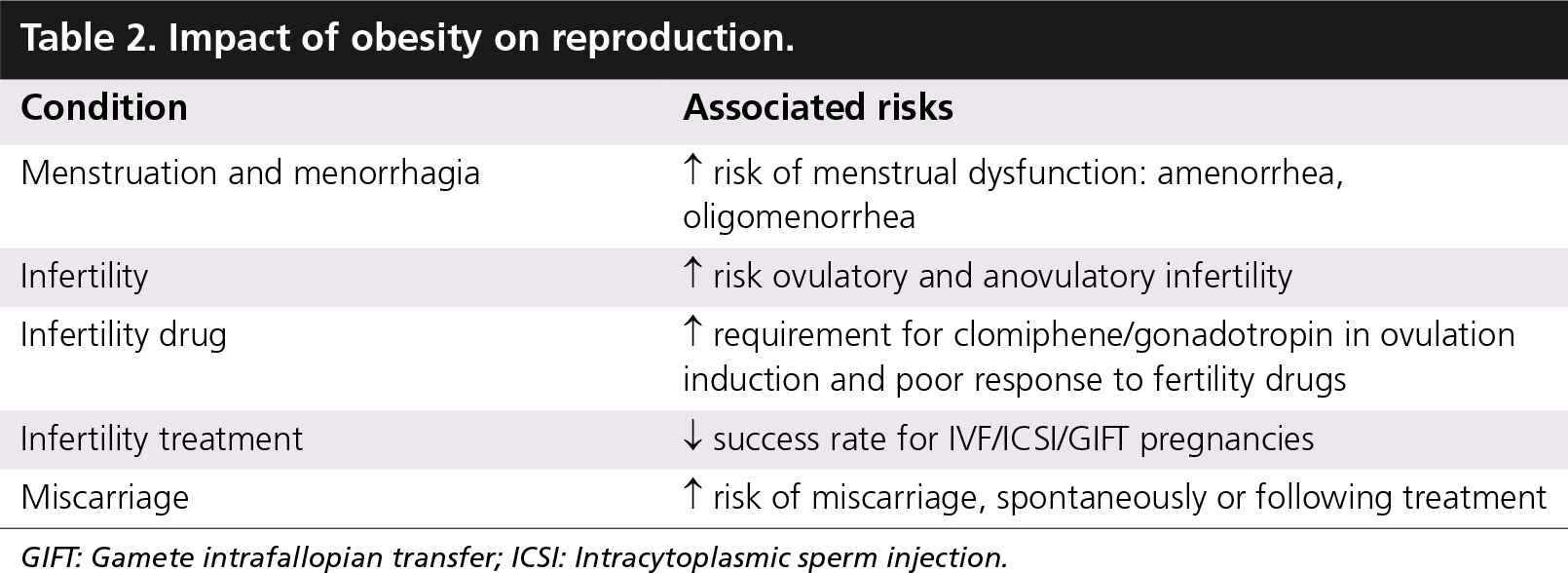
GIFT: Gamete intrafallopian transfer; ICSI: Intracytoplasmic sperm injection.
Obesity & prioritizing fertility treatment
In many countries, IVF is still considered very costly and unaffordable to many patients. In New Zealand, balancing the cost and outcomes together, the New Zealand Ministry of Health restricted access to publicly funded IVF and ICSI using the clinical priority access criteria (CPAC) approach. Seven separate criteria were developed to select the couples with the worst prognosis for spontaneous conception for treatment priority [46]. The introduction of the CPAC model has allowed greater and fairer access to ARTs in New Zealand. Since obesity was considered to reduce a women's chance of successful ART, the CPAC could only be applied to women who were inside the BMI 18–32 kg/m2 range. Women outside this range were only accepted on the basis that they had undergone weight improvement to within the agreed range. After 5 years of implementation, data from 1280 referred cases were analysed. A total of 38% of women with a BMI more than 32 kg/m2 had a birth following a treatment-related pregnancy or spontaneous pregnancy, compared with 52% of women with a BMI less than 32 kg/m2 [47]. The recent guidelines by UK NHS and British Fertility Society limiting ART services to those women with BMI less than 36 kg/m2 is another example of the influence of obesity on decisions regarding ART provision [101].
Obesity & obstetric problems
An overweight maternal condition exists in more than 20% of all pregnancies and represents a major public health issue because of the numerous known pregnancy risks and complications [48]. A study that was conducted on 25,601 Finnish women with singleton pregnancies noted that pregnancy outcomes were impaired in overweight and obese patients with respective ORs as follows: low Apgar score at 5 min (OR: 1.54 [95% CI: 1.20–1.98] and OR: 1.64 [95% CI: 1.22–2.28], respectively), newborn admission to intentive care unit (OR: 1.20 [95% CI: 1.06–1.37] and OR: 1.38 [95% CI: 1.17–1.61], respectively), cesarean delivery (OR: 1.22 [95% CI: 1.10–1.35] and OR: 1.68 [95% CI: 1.48–1.91], respectively), perinatal death (OR: 1.54 [95% CI: 0.98–2.42] and OR: 2.19 [95% CI: 1.33–3.62], respectively). It is noted clearly in this large retrospective study that transition from overweight to obesity worsens pregnancy outcome in a BMI-dependant manner. Transition from overweight to obese condition also doubles the risk of perinatal death [48].
In another large review, involving 18,401 women who were booked for antenatal care in Queensland, Australia [49], it was noted that as BMI increases, cesarean section rates, maternal morbidity, neonatal morbidity, neonatal intensive care utilization and length of hospital stay all increase. There was also a doubling of birth defects from 1.9% in women with a BMI of 30–40kg/m2 to 4% in women with a BMI above 40kg/m2 (Table 3). Data from the Atlanta Birth Defects Risk Factor Surveillance Study from January 1993 until August 1997, noted that obese women were more likely than average-weight women to have an infant with spina bifida (unadjusted OR: 3.5; 95% CI: 1.2–10.3), omphalocele (OR: 3.3; 95% CI: 1.0–10.3), heart defects (OR: 2.0; 95% CI: 1.2–3.4), and multiple anomalies (OR: 2.0; 95% CI: 1.0–3.8) [50]. Overweight women were more likely than average-weight women to have infants with heart defects (OR: 2.0; 95% CI: 1.2–3.1) and multiple anomalies (OR: 1.9; 95% CI: 1.1–3.4). Several epidemiologic studies have suggested that being overweight before pregnancy is a risk factor for neural tube defects (NTDs) [51,52]. BMI of more than 29kg/m2 doubles the risk of NTDs (OR 1.9; 95% CI: 1.1–3.4) [52]. Werler
Adjusted odds ratio for maternal, peripartum and neonatal outcomes, according to BMI.

Adapted from [50].
The supposed mechanisms that increase the congenital anomaly rates include insulin resistance and its consequence, incipient hyperglycemia. In addition, the increased risk of congenital malformations, in particular NTDs, in children of obese women can be explained by difficulties in visualization when making the ultrasound scan and missing adjustment for weight when measuring biochemical markers [54].
Thus, preventive measures should be taken with overweight teenagers before their first pregnancy, and delivery wards should have an essential role in identifying women at high risk in their next pregnancy as a result of obesity. Modest weight loss would bring substantial advantages to the obstetric outcomes of these women.
Managing obesity
Treatment of obesity itself should be the initial aim in obese infertile women before embarking on ovulation-induction drugs or ART. Reduction of fat and abdominal fat should result in improved menstrual function and fertility and a reduction of metabolic risks. A reduction of 2–5% in body weight was associated with restoration of ovulation, an 11% reduction in abdominal fat, a 4 cm reduction in WC and a 71% increase in insulin sensitivity [55]. Weight loss results in an increase in SHBG, reduction in testosterone, improved menstrual function, improvement in conception rate and reduction in miscarriage rate. As central adiposity is associated with menstrual disorders and infertility, abdominal fat loss is critical in restoring ovulation.
Various strategies have been suggested to overcome the problem of obesity. Amongst these are dietary management, physical activity, behaviour modification, pharmacologic treatment and surgery. The issues are the long-term compliance to these strategies and maintaining the weight loss. The NIH recommends a multifaceted approach to treating obesity [56]. It emphasizes the importance of achievable and sustainable goals, notably a combination of diet, physical activity and behavior therapy (Box 1).
Dietary treatment
Bates and Whitworth were the first to show a reduction in plasma androgens with dieting, and associated return of menstrual cycle [57]. Subsequently other studies investigating dietary manipulation in subjects with obesity and PCOS [57], demonstrated that strict calorie restriction with 5% or greater weight loss led to changes in insulin, insulin-like growth factor, SHBG and menstruation.
NIH clinical guidelines for long-term treatment of overweight and obesity.
Sensible diet and changed eating habits for the long term
Effective physical activity programme sustainable long term
Behaviour modification, reduction of stress, well being
Social support by physician, family, spouse and peers
Smoking cessation and reduction in alcohol consumption
Avoidance of ‘crash diets’ and short-term weight loss
Minor roles for drugs involved in weight loss
Avoidance of aggressive surgical approaches for majority
Adaptation of weight loss programme to meet individual needs
Long-term observation, monitoring and encouragment of patients who have successfully lost weight
Adapted from [57].
The key component of diet should be calorie restriction rather than the composition of the diet itself. Dietary intervention in managing obesity should aim for gradual weight loss via reduced calorie consumption and increased physical activity, with the overall aim of energy expenditure exceeding energy intake. Sensible eating plans, tailoring to individual weight and current dietary and exercise pattern, increase the chance of sustained weight loss. Diets based on healthy eating principles have a better long-term outcome, which is important because weight-loss maintenance requires that changes in eating habits be sustained for life (Box 2) [59].
Lifestyle modification
Lifestyle modification is of paramount importance in achieving and maintaining weight loss. Dietary management with lifestyle modification as an objective should be adopted initially, with pharmacological and other surgical/medical interventions reserved for use when weight loss regimes have proved unsuccessful. Exercise should be an integral component in any weight-loss programme. Exercise increases insulin sensitivity both by acting directly on muscle metabolism [60] and indirectly by assisting in weight management [61].
Other lifestyle issues that need to be addressed are smoking, alcohol consumption and stress-related environment. Smoking is a major risk factor for reduced fertility in women, with consequences including extended time to pregnancy, preterm birth and low birth weight [62]. High levels of alcohol intake have been associated with reduced fertility and increased risk of spontaneous abortion [63]. Therefore, cessation of smoking, cessation or reduction of alcohol and reduction of psychosocial stressors are important issue that need to be addressed.
An analysis of the Nurses' Health Study, which began in 1976 and enrolled 121,700 female nurses who were followed by questionnaire biannually, clearly demonstrated the role of diet and lifestyle in the risk of development of Type 2 diabetes. Women were free of cardiovascular disease, diabetes and cancer at baseline and were followed up over 16 years. Overweight and obesity was the single most important predictor of development of diabetes. However, lack of exercise, a poor diet and smoking were all associated with a significantly increased risk of diabetes even after adjusting for BMI [64].
Dietary management for weight loss.
Energy deficit of 500–600 kcal/day
Low fat (30% of energy), moderate protein (15%) and high carbohydrate (55%)
Increased nonrefined carbohydrate, such as wholegrain bread and cereals
Increased fruits and vegetables
Low-glycemic index food may aid weight loss through increased satiation
No evidence for the strategy of increasing dietary protein to replace carbohydrate
Clark
Overall, the weight of evidence supports the role of lifestyle modification in weight reduction with a corresponding improvement in reproductive function. A group environment provides support and could make it easier for patients to implement these lifestyle changes [59].
Pharmacological treatment
Pharmacotherapy for the management of obesity is primarily aimed at weight loss, weight-loss maintenance and risk reduction, and has included thyroid hormone, phenylpropanolamine, mazindol, fenfluramines and, more recently, sibutramine and orlistat. These agents decrease appetite, reduce absorption of fat or increase energy expenditure. However, studies evaluating the long-term efficacy of anti-obesity agents are limited. Longer and more methodologically rigorous studies of anti-obesity drugs that are powered to examine the long-term effect and end points such as cardiovascular morbidities are awaited [68]. Despite rapid strides toward an ideal anti-obesity agent, the role of diet, exercise and behavior modification must be considered the cornerstone for any potential future pharmacotherapy.
Given the importance of hyperinsulinemia in the development of hyperandrogenism and disrupted folliculogenesis in obesity and PCOS, the use of insulin-sensitizing drugs seems reasonable in order to facilitate spontaneous ovulation and restore fertility. The most extensively studied insulin-lowering agent in the treatment of PCOS is metformin. Metformin is a biguanide oral antihyperglycemic agent that has been extensively used in the treatment of Type 2 diabetes mellitus. It lowers blood glucose mainly by inhibiting hepatic glucose production and increase in the peripheral glucose uptake. Several other actions may contribute to this effect, such as increased intestinal use of glucose and decreased fatty acid oxidation. Therefore, metformin can reduce peripheral insulin concentrations and improve glucose tolerance and metabolism. There are also preliminary
A meta-analysis of 13 randomized trials [70] comparing metformin with placebo or metformin plus clomiphene with clomiphene alone in women with PCOS concluded that metformin increased the ovulation rate by a factor of approximately four. It was discovered that pregnancy rate did not differ significantly between metformin and placebo, but pregnancy rates for metformin plus clomiphene were significantly higher than for clomiphene alone. However, in a multicenter, randomized trial involving 20 Dutch hospital and 228 patients, Moll concluded that metformin is not an effective addition to clomiphene citrate as the primary method of inducing ovulation in women with PCOS [71]. The ovulation rate in the metformin/clomiphene group was 64% compared with 72% in the clomiphene/placebo group, a nonsignificant difference. In a larger study, which involved 626 infertile women with PCOS assigned to either clomiphene, metformin or combination therapy, Legro
Surgical treatment
In women with morbid obesity failing other interventions, weight loss may be induced with surgical intervention. Bariatric surgery today is the only effective therapy for morbid obesity. Bariatric operations are either restrictive, limiting the amount of food ingested; malabsorptive, limiting the amount of nutrient absorbed; or a combination of both [73]. Bariatric surgery dates back to the 1950s when jejunoileal bypass was introduced. Since then, numerous improvements have been made in procedures and techniques. Currently, the two most common bariatric procedures performed are laparoscopic adjustable gastric banding and laparoscopic Roux-en-Y gastric bypass. Both of these operations provide excellent results [74,75], with the majority of patients losing more than 50% of their excess weight and with most obesity-related comorbidities, such as diabetes and hypertension, reversed or prevented [76]. Morbidly obese patients considering such operations have to meet a strict criteria and must be evaluated by a multidisciplinary team. However, they would still need to commit to long-term dietary changes, behavioral modifications and medical supervision.
Eid
Executive summary
Obesity is related to many systemic diseases and abnormalities in hormonal and reproductive function.
Obesity can be measured clinically by body mass index (BMI), waist circumference and waist–hip ratio. Waist–hip ratio greater than 0.8 defines an increased risk of cardiovascular disease and reduce cumulative pregnancy rate.
30–50% of PCOS women are overweight or obese. Obesity, particularly abdominal obesity amplifies hyperinsulinemia.
Obesity is related to menstrual abnormalities; amenorrhea, oligomenorrhea and menorrhagia are fourfold higher in obese women.
Obesity also contributes to anovulatory and ovulatory infertility via altered imbalance between estrogen, androgen and SHBG.
Hyperandrogenism and hyperleptinemia are also related to anovulatory and ovulatory infertility in obese women.
Obesity is associated with a lower chance of live birth after IVF/intracytoplasmic sperm injection and with an impaired response to ovarian stimulation.
Obesity reduces the likelihood that a woman will be accepted for assisted reproductive techniques (ART) treatment, particularly in a nationally funded situation.
Overweight and obesity increases obstetric risks in a BMI-dependent manner. The risk of perinatal death and congenital abnormalities double in the obese mother.
Weight loss improves menstrual regularity, ovulation and fertility, and should be promoted as an initial treatment option for obese women with infertility. Only 3–5% weight loss is required.
Lifestyle modifications are the best way to achieve and sustain weight loss. These include sensible dieting, regular exercise, cognitive behavior therapy and a supportive group environment.
Pharmacologic intervention with metformin is not superior to clomiphene to induce ovulation and pregnancy/live birth rate in obese PCOS women.
Surgical intervention should be reserved if other measures of weight reduction fail. Although effective, it must be used together with dietary modifications and behavioral changes.
Future perspective
With an escalating figure of obesity worldwide, research in this area will definitely continue. While evidence from experimental, clinical and genetic research supporting the hypothesis for the fetal origins of PCOS has been documented, little is known about the possible contribution of ‘fetal programming’ to obesity. More research is needed at the molecular level to understand hormonal and biochemical associations with different obesity phenotypes. As obesity is not just an adult disease, with more children suffering from the problem lately, interventions in early life may have a great impact on adult health. Long-term follow up of childhood obesity and the impact of early interventions for weight reduction on the adult manifestation of reproductive disease is awaited. While it is acknowledged that obesity has a clear association with ART outcome, more research is needed to elucidate the mechanism underlying it, particularly to differentiate between endometrial or ovarian effect. Finally, there is no doubt that search for the ‘magic bullet’ to treat obesity will continue, but the importance of diet, exercise and lifestyle modification must continue to be the cornerstone of obesity management.
Footnotes