
Abstract
Background:
Adverse birth outcomes associated with grand multiparity are more ambiguous than those linked to multiparity. The primary literature on this issue reveals inconsistent findings across various studies. A paucity of data is evident in systematic reviews and meta-analyses that assess adverse birth outcomes specifically for African grand multiparas.
Objectives:
To address the pooled adverse birth outcomes and their associated factors among African grand multiparas.
Design:
Systematic review and meta-analysis.
Data sources and methods:
Studies were systematically searched from April 20, 2024, to June 15, 2024, using Scopus, Web of Science, PubMed, Science Direct, African Journal Online, and the Wiley Online Library. The Joanna Briggs Institute tool was used for a quality assessment of each primary study. Data were extracted using Excel and analyzed with Stata 11 software. A random-effects model was employed to calculate the pooled estimates. The paper employs appropriate statistical techniques to assess publication bias and heterogeneity, such as the symmetry of the funnel plot, Egger’s test, and Cochran’s Q test. The study addresses a critical public health issue in Africa, contributing valuable data that could inform policy and healthcare practices aimed at reducing adverse birth outcomes among grand multiparas. A subgroup analysis was performed based on the publication years.
Results:
The pooled prevalence of adverse birth outcomes among African grand multiparas was 24.97%; 95% CI: 19.97–31.99. Pregnancy-related complications (AOR: 3.17; 95% CI: 2.35–4.28), a history of home births (AOR: 3.30; 95% CI: 1.70–6.40), and rural residence (AOR: 4.12; 95% CI: 3.12–5.44) were significantly associated with adverse birth outcomes among African grand multiparas.
Conclusion:
Overall, the pooled prevalence of adverse birth outcomes among grand multiparas was comparably high. Variables such as rural residence, previous pregnancy-related complications, and a history of home births were significantly associated with adverse birth outcomes. Strengthening institutional births, providing high-quality prenatal care, and early pregnancy follow-ups are recommended to reduce adverse birth outcomes in grand multiparous women. In addition, improving the availability of comprehensive contraceptive options for rural-residing African grand multiparous women is essential.
PROSPERO registration:
CRD42024569768.
Introduction
Grand multiparas, defined as women who have had five or more previous deliveries after a gestational age of 28 weeks or having a fetal weight of at least 1000 g in a developing setting.1,2 Over the years, various definitions of grand multiparity have emerged in the literature, with the number of previous childbirths ranging from 4 to 8. 3 However, in 1993, the International Federation of Obstetrics and Gynecology standardized the definition, describing grand multiparas as those who have had five to nine prior term deliveries. This definition was confirmed in a recent study, 4 which noted that 3%–4% of pregnant individuals are grand multiparas. 1 By contrast, the prevalence is significantly higher in developing countries, particularly in African nations, where the rate of multiparity ranges from 17% to 33%. 5 In sub-Saharan Africa (SSA), the rates of multiparity range from 18% to 28% in certain countries. 6 A study in 10 SSA countries found that less than 40% of grand multiparas in these high-fertility nations intended to use modern contraceptives, with country variations ranging from as low as 32.8% in Angola to as high as 71.2% in the Republic of the Congo. 6 According to the 2019 Ethiopian Mini Demographic Health Survey, the prevalence of grand multiparity was 26%. 7 Factors associated with the high rate of grand multiparity include limited access to healthcare, early marriages, the death of another child, low educational status, and reduced access to and intention to use contraception.8,9 Studies indicate that the prevalence of unmet needs for family planning was nearly 20% in Tanzania 5 and 22% in Ethiopia. 7 This paper contributes to the field by attempting to consolidate inconsistent findings and provide pooled prevalence estimates and associated risk factors for adverse birth outcomes among grand multiparas in Africa.
The Maternal Mortality Estimation Interagency Group reported an estimated 295,000 maternal deaths worldwide, with 196,000 (66%) occurring in SSA. 10 The maternal mortality ratio (MMR) in SSA was 542 deaths per 100,000 live births, significantly higher than the global average of 216 deaths per 100,000 live births. 11 Ninety-eight percent of these deaths occur in low- and middle-income countries (LMICs), with 75% occurring in SSA and Southern Asia. 12 Sustainable Development Goal 3 (SDG3) states that by 2030, all countries aim to reduce the infant mortality rate (IMR) to at least 12 per 1000 live births and maternal mortality (MMR) to at least 70 per 100,000 live births.13,14
Despite efforts to reduce IMRs and maternal mortality ratios (MMRs) in African countries, both rates remain high. 9 Adverse birth outcomes include maternal and fetal complications such as antepartum and postpartum hemorrhage (PPH), stillbirths, hypertension, anemia, preterm birth, congenital malformations, and perinatal mortality.15,16 A secondary study in the Nigerian Demographic and Health Survey found a higher prevalence of stillbirths (38.9%), low APGAR scores (51.9%), and low birth weights (40.7%) among grand multiparas. 17 In addition, risks of meconium aspiration (9.8%), the need for resuscitation (14.7%), and macrosomia aspiration (57.4%) have been reported among low multiparas. 18 More than 40% of stillbirths can be prevented by providing high-quality antepartum, intrapartum, and postpartum care, along with timely access to emergency obstetric care. 19
The association between grand multiparity and adverse birth outcomes has been a topic of much debate, with conflicting conclusions drawn from various studies. 5 Some studies have established that grand multiparas are at an increased risk for adverse maternal health outcomes,20,21 emphasizing the importance of contraceptive use to avert these outcomes. For instance, research indicates a higher incidence of obstetric complications among grand multiparas. 22 Other studies in Saudi Arabia and Uganda have shown comparable maternal and neonatal complications between grand multiparas and multiparas.23,24 To classify grand multiparas as a high-risk group, more evidence is needed. However, the prevalence of adverse outcomes remains high in African countries. This systematic review and meta-analysis aims to fill the gap by determining the pooled adverse birth outcomes and their associated factors among African grand multiparas.
Data sources and methods
This systematic review and meta-analysis was conducted as per the Systematic Reviews and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 25 (PRISMA) checklist, 2020 guided this systematic review (Supplemental Material).
Search strategy and data sources
The systematic review and meta-analysis format, along with the use of multiple reputable databases (PubMed/Medline, Scopus, Web of Science, Science Direct, African Journal Online, and Wiley Online Library), enhances the comprehensiveness and credibility of the findings from April 20, 2024, to June 15, 2024. A confirmatory search was also performed on Google Scholar to ensure that no primary studies were missed. Any additional data from identified studies were cross-checked and matched with existing datasets. To identify gray literature, the digital collections of the Ethiopian University of Science and Technology were explored. The search strategies were outlined below. The following keywords had been utilized during the searching process: ((adverse birth outcomes) OR (child) OR children OR (mother) OR (women) AND (associated factors) OR (determinants) OR (predictors) AND (grand multiparas) AND (Africa)). The search was specifically targeted at studies that examined the adverse birth outcomes and associated factors among grand multiparas in African countries. Duplicate studies from each database were exported to Endnote X7 citation manager software (Thomson Reuters, New York, NY) and subsequently removed. Any disagreements were resolved through discussion and consensus based on established criteria, or by involving all investigators when a consensus could not be reached.
After removing duplicate articles, three authors screened the titles and abstracts of all the collected records. The reference lists of the retrieved articles were also reviewed to identify additional relevant studies. The search strategies were outlined below. The following keywords had been utilized during the searching process: ((adverse birth outcomes) OR (child) OR children OR (mother) OR (women) AND (associated factors) OR (determinants) OR (predictors) AND (grand multiparas) AND (Africa)). The search was specifically targeted at studies that examined the adverse birth outcomes and associated factors among grand multiparas in African countries. Any disagreements were resolved through discussion and consensus based on established criteria, or by involving all investigators when a consensus could not be reached.
Study inclusion and exclusion criteria
Three authors (AGM, YAF, and WCT) subsequently screened the full titles and abstracts based on the inclusion criteria. Original research studies that reported the adverse birth outcomes and associated factors among African grand multiparas were included in the review. Observational studies without restrictions on publication year were considered. However, the searched articles were found to have been published from 2008 to 2024. The review included both comparative cross-sectional and retrospective cohort studies conducted in African countries that reported adverse birth outcomes and associated factors. Both published and unpublished articles written only in the English language were considered for inclusion. However, studies that did not clearly report the prevalence of adverse birth outcomes and associated factors among healthcare providers in Ethiopia were excluded. Exclusions were also made for articles that lacked a clear research topic, full texts, abstracts, editorial reports, letters, reviews, or commentaries. The qualifying standards for these reviews were established using the modified Population-Intervention-Comparison-Outcome-Type (PICOT) of the study-context framework (see Table 1).
Framework for determining the eligibility of studies (PICOT).

PICOT, Population-Intervention-Comparison-Outcome-Type.
Outcome of interest
In this review and analysis, studies focused on exploring adverse birth outcomes and related factors among grand multiparas in Africa. Specifically, studies examined the occurrence of adverse birth outcomes and identified associated factors in this population. This review included grand multiparas who experienced at least one adverse birth outcome as the primary focus of investigation.
Quality assessment
Eligible articles focusing on the adverse birth outcomes and associated factors among African grand multiparous women were included in this review. The quality of each article was assessed using the Joanna Briggs Institute tool. 26 Overall, the tool comprises nine items, with a maximum score of 9 and a minimum score of 0. Studies were categorized based on their quality score as either low (<7) or high (⩾7). The quality evaluation summary showed that more than three-fourths (n = 14, 77.8%) of the included studies were of high quality, while the remaining one-fifth (n = 4, 22.2%) of the studies were of medium quality. 6
Heterogeneity and publication bias
To assess the presence of heterogeneity among the studies included in our analysis, we utilized Cochran’s Q test and I 2 statistics. The interpretation of I-squared values followed established guidelines: 0%–25% indicates low heterogeneity, 25%–50% suggests moderate heterogeneity, 50%–75% indicates substantial heterogeneity, and 75%–100% suggests considerable heterogeneity. 27 To evaluate publication bias, employed subjective funnel plot observation and Egger’s test. Publication bias was considered significant at a p value less than 0.05. In addition, a sensitivity analysis using the leave-one-out method was conducted to evaluate the influence of individual studies on the overall pooled prevalence. 28 Subgroup analysis was performed based on publication year to explore potential variations across different time periods. Among the included studies, the subjectively observed was a symmetrical funnel plot.
Data processing and analysis
Three authors (AGM, YAF, and WCT) extracted standardized data using a Microsoft Excel format. Two authors (GAT and YAG) reviewed and verified the extracted data, with any discrepancies resolved through group discussions among the data extractors. The data were subsequently imported into Stata version 11 software (Stata Corp., LLC) for further analysis. The extracted data included the primary author’s name, publication year, geographical region of the study sample size, study population characteristics, study design, and prevalence. Data were analyzed using a random-effects model, specifically employing the Der Simonian–Laird method to combine outcome data. Results were reported as prevalence estimates of the outcome variables along with 95% confidence intervals (CIs). The Cochrane Q test and I 2 statistic were used to assess statistical heterogeneity.
Results
Selection of studies
A total of 3953 records were identified using electronic search PubMed (1331), Scopus (121), African Journal Online (390), Wiley Online Library (903), Science Direct (642), Web of Science (480), and National Library (86). After assessing screening and eligibility criteria, we included 18 articles for the final analysis (Figure 1).
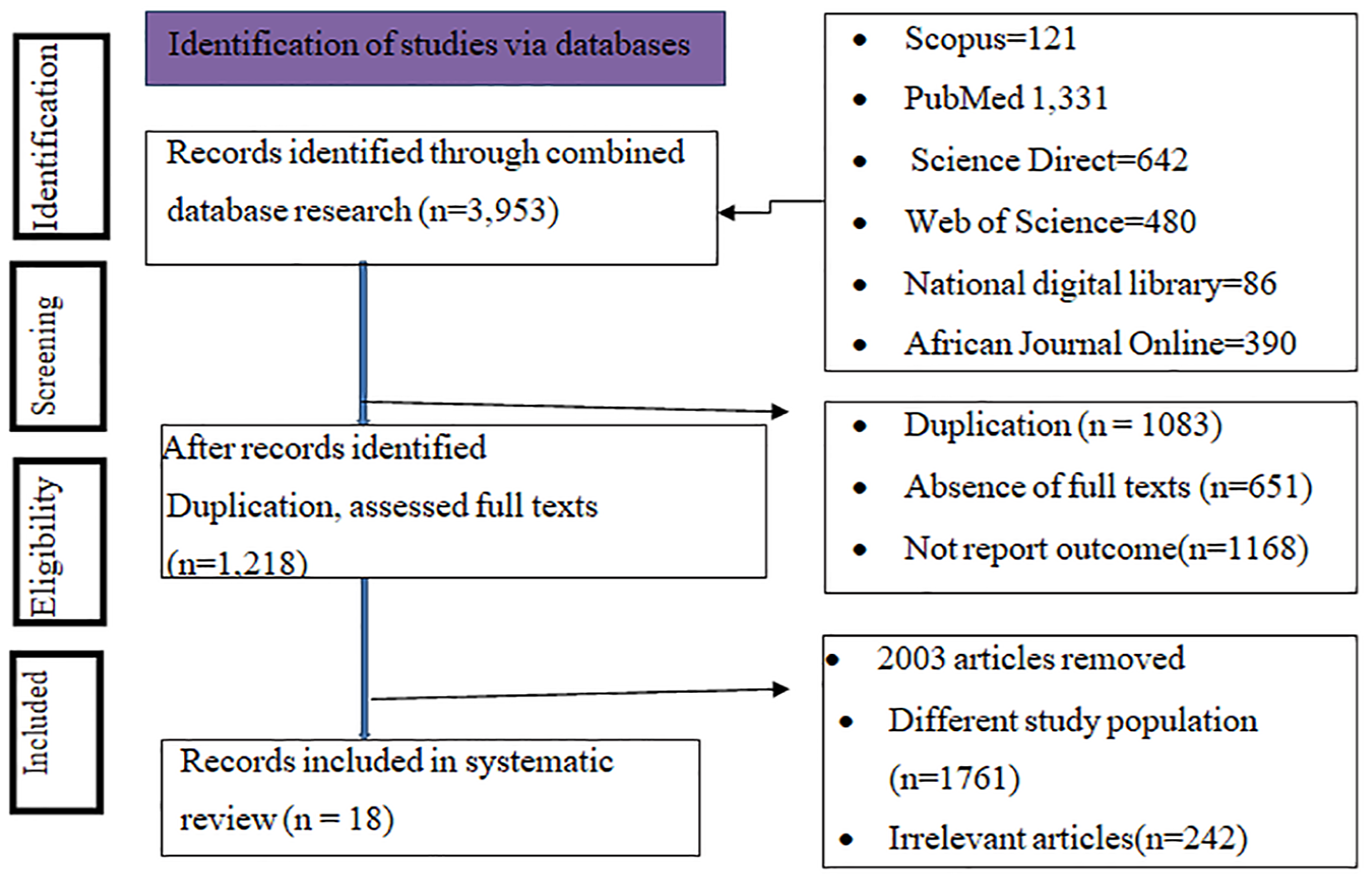
PRISMA flow chart for the systematic review and meta-analysis.
Description of the included studies
Among 18 eligible studies, 5 were retrospective controls, and 6 were comparative studies that specifically compared outcomes between grand multiparas and multiparas individuals. The sample sizes ranged from 150 in Sudan 29 to 5610 in Uganda. 24 The geographical distribution of the studies included Ethiopia (n = 6), Nigeria (n = 3), Sudan (n = 2), Tanzania (n = 2), South Africa (n = 1), and Uganda (n = 1; Table 2). All these studies assessed adverse birth outcomes and associated factors among African grand multiparous women. Among these adverse birth outcomes, PPH, premature membrane rupture, dystocia, second-to-fourth degree perineal tear, stillbirth/intrauterine fetal death, and low APGAR scores frequently occur in grand multiparas.
Characteristics of the included studies to estimate the pooled effect of adverse birth outcomes among African grand multiparas, 2024.

Meta-analysis
It seems like you were discussing findings from a research study on adverse birth outcomes among African grand multiparas. From a total of 27,122 study participants, the pooled prevalence of adverse outcomes was 7090 (13.90%), 95% CI: 12.81–14.99, with significant heterogeneity among the studies (I² = 97.2%; Figure 2).

Pooled estimates of adverse birth outcomes among African grand multiparous women.
Examination of the heterogeneity across the included studies
To reduce heterogeneity random-effect model analysis was used, yielding a significantly higher prevalence of 24.97%, 95% CI: 19.97–31.99. Subgroup analysis focusing on studies conducted before 2021 showed a similar prevalence of 25.25%, 95% CI: 14.20–36.31, I 2 = 98.1, p < 0.0001, and at 2021 or after 2021, which is 24.64%, 95% CI: 16.76–32.61 (Figure 3). Furthermore, the pooled prevalence of adverse outcomes was higher 28.16%, 95% CI: 16.54–39.77, I² = 96.9, p < 0.0001 among studies with a sample size of less than 548 compared to those with a sample size ⩾548 (22.45%), 95% CI: 13.54–31.36, I² = 97.2, p < 0.0001 (Figure 4). Significant heterogeneity was noted in the subgroup analyses.

Pooled estimates of adverse birth outcomes and subgroup analysis (by publication year) among African grand multiparous women.

Pooled prevalence of adverse birth outcomes by sample size subgroup analysis among African grand multiparas.
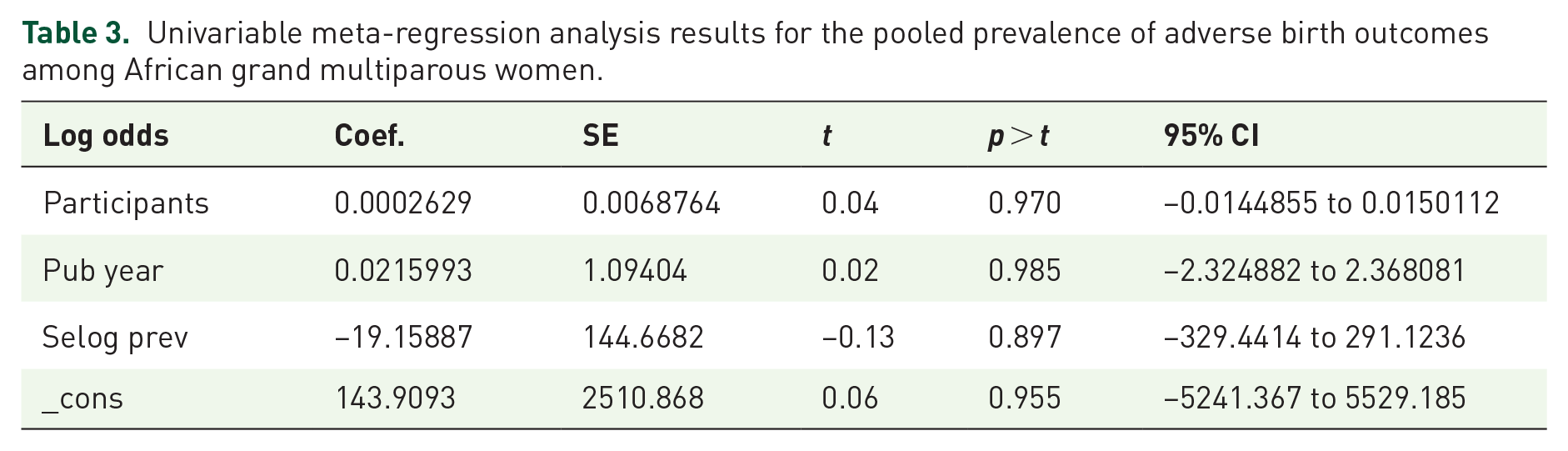
They assessed the effects of study participants, sample size, and year of study on heterogeneity among the studies using a meta-regression analysis. However, there was no significant prediction of heterogeneity based on the assessed variables (sample sizes, study participants, and year of study; Table 3). In the adjusted model, neither the sample size, the study participants, nor the year of the study indicated that heterogeneity in the effect size was consistent with the pooled prevalence.
Univariable meta-regression analysis results for the pooled prevalence of adverse birth outcomes among African grand multiparous women.
Publication bias
According to the symmetrical observation of the funnel plot, no publication bias was evident among the included studies (Figure 5). Similarly, the results of Egger’s test (p = 0.794) indicated a statistically nonsignificant difference, which was the absence of publication bias, as shown in Table 4.

Graphical representation of the absence of publication bias using funnel plots of all included studies.
The absence of publication bias.

Sensitivity analysis
The authors conducted a sensitivity analysis to identify the potential source of heterogeneity. Based on the results of a random-effects model, no single study affected the overall pooled prevalence of adverse birth outcomes among African grand multiparas (Figure 6).
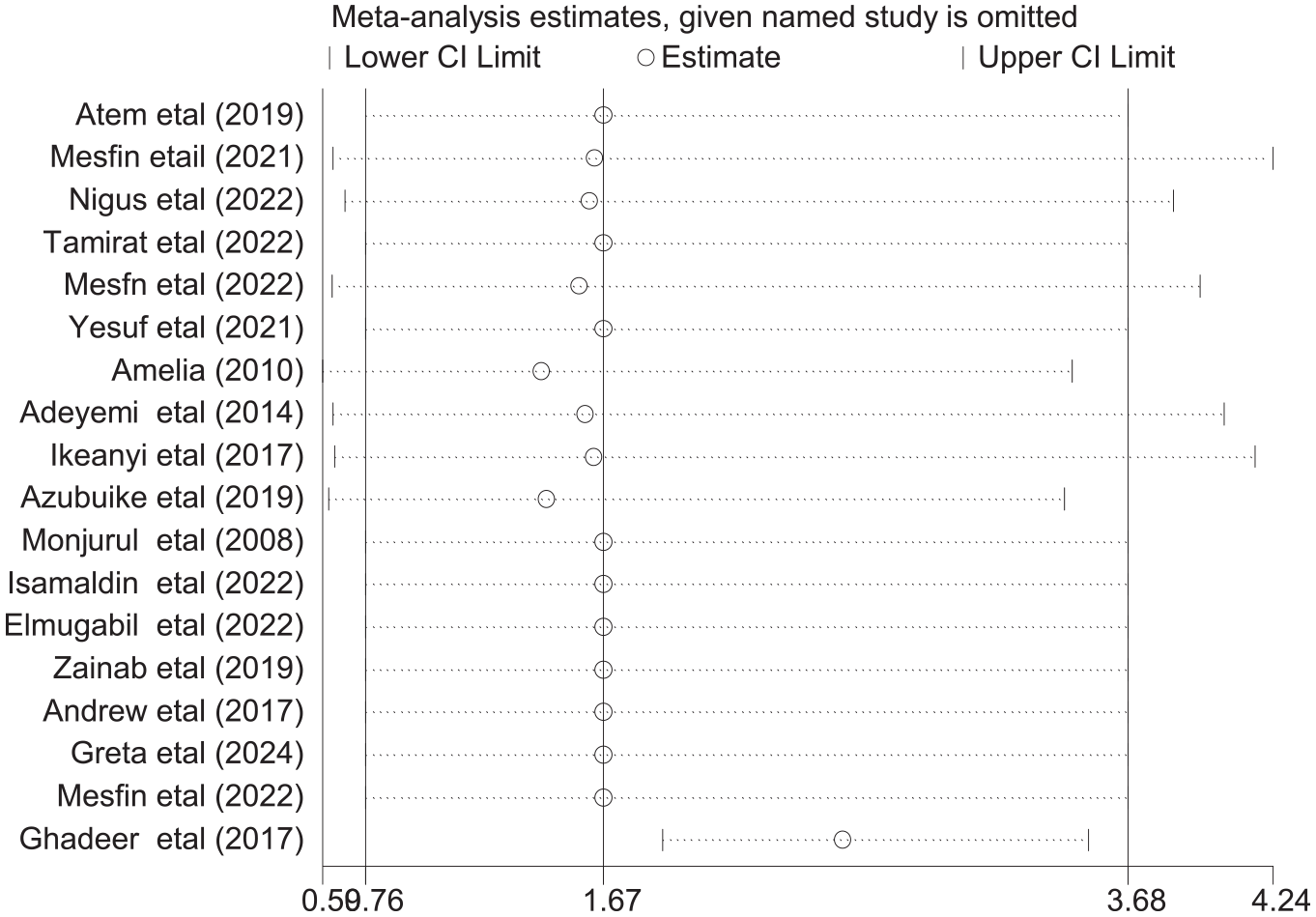
Results of the sensitivity analysis of 18 studies.
Factors associated with adverse birth outcomes
Figure 7 shows that the factors linked to adverse birth outcomes among African grand multiparous women were living in rural areas (AOR: 4.12, 95% CI: 3.12–5.44), having previous pregnancy-related complications (AOR: 3.17, 95% CI: 2.35–4.28), and having history of home birth (AOR: 3.30, 95% CI: 1.70–6.40), which were significantly associated with adverse birth outcomes among African grand multiparous women.

Factors associated with adverse birth outcomes, living in rural areas, having a history of birth complications, and home birth.
Discussion
The World Health Organization’s SDG3 states that by 2030, all countries will aim to reduce IMR to at least 12 per 1000 live births and MMR to at least 70 per 100,000 live births.13,14 The implementation of quality health care is recognized internationally as a critical aspect of the maternal and newborn health agenda. 14 Reproductive health services, such as comprehensive family planning services and preconception care in the clinic, are comprehensive for achieving this global agenda and quality health care among African grand multiparas. 42 Therefore, ensuring the reduction of adverse birth outcomes in grand multiparas is a key strategy for achieving this global agenda and quality of care. 43 The objective of this review was to determine the pooled prevalence of adverse birth outcomes and their associated factors among African grand multiparas.
The pooled prevalence of adverse birth outcomes among African countries’ grand multiparas was 24.97%, 95% CI: 19.97–31.99. This prevalence was comparable to findings from other developing regions in Bangladesh (25%), 44 and in SSA (27.8%) 45 among multiparas but higher than in Pakistan (13.83%) 46 and in India (8.7%). 47
The similarities in prevalence rates of certain health conditions among multiparas in different regions, such as Bangladesh, SSA, Pakistan, and India, can be attributed to several possible causes like similar challenges in healthcare systems, such as inadequate maternal health services, lack of access to antenatal care, and insufficient health education, can lead to comparable prevalence rates. Understanding these factors can help in developing targeted interventions and policies to address health disparities in these regions.
This review included studies in developing countries’ health services for African grand multiparas, which vary between 17% and 33% compared with developed countries. 42 However, the prevalence of grand multiparity in developed countries was low (3%–4%). 48 In Africa, grand multiparity was associated with factors such as poverty, lack of healthcare resources, poor antenatal care, illiteracy, and limited, modern contraceptive options were low. 42 By contrast, developed countries typically report lower rates of multiparity due to better healthcare infrastructure and higher contraceptive use. 9 Improving access to reproductive health services for African grand multiparas is crucial not only for reducing adverse birth outcomes but also for enhancing their overall quality of life and contributing to the achievement of global health goals. These results contribute to the understanding of maternal health challenges and policy development, directly linking to the achievement of SDG3, which focuses on maternal and neonatal health outcomes in Africa.
Among grand multiparas living in rural areas, those living in rural areas were more likely to have adverse birth outcomes. Possible explanations are socioeconomic status differences, such as better education and income, and access to healthcare facilities than rural mothers. In addition, rural mothers practice less health-seeking behaviors, face more transportation challenges when accessing healthcare facilities than urban mothers, which can result in delays in accessing healthcare. This association is supported by similar observations in Canada. 49 Understanding these dynamics is crucial for developing targeted maternal care strategies that address the specific needs of rural populations. Efforts to improve maternal health outcomes in rural areas should focus on enhancing access to healthcare services, promoting health education, raising awareness, and addressing barriers related to transportation and healthcare infrastructure. The insights gained from this review provide valuable information to guide the development of effective maternal care strategies, particularly in rural areas.
Grand multiparas who had previously experienced pregnancy-related complications were 3.17 times more likely to have adverse birth outcomes than participants who had not previously experienced pregnancy-related complications. This finding was supported by a study in Saudi Arabia, which grand multiparity was associated with pregnancy-related complications who grand multiparas faced greater risks of stillbirth, macrosomia, and preterm birth than multiparas. 50 To mitigate these risks, it is very important to implement comprehensive strategies at both the community and health facility levels. In addition, enhancing prenatal care services to monitor high-risk pregnancies more closely can aid in early detection and management of complications, potentially improving birth outcomes. To reduce adverse birth outcomes, address these factors by providing education and targeted interventions for grand multiparas.
This review revealed that the risk of adverse birth outcomes was 3.30 times greater for those with home birth than for those with a history of childbirth at health facilities. This study was in line with systematic reviews of low-income countries, 16 and in Kenya. 51 The benefits of institutional delivery include access to clean and safe delivery environments, skilled medical care, and timely interventions in cases of complications. These factors collectively contribute to reducing maternal and neonatal morbidity by preventing infections, trauma, and other adverse outcomes associated with home births. To promote safer childbirth practices and improve outcomes for grand multiparas in Africa and other countries (LMICs), it is crucial to advocate for and ensure access to institutional delivery services. 52 This could be because clean and safe delivery services provided at health facilities help reduce neonatal complications, which, in turn, prevent trauma, infection, and maternal and neonatal morbidity and mortality. In addition, this finding emphasizes the need to utilize institutional delivery services. Therefore, to improve maternal and child health outcomes, all healthcare providers should closely monitor institutional deliveries among high-parity women in maternal health services. Community mobilization, collaboration with traditional birth attendants, and addressing socio-cultural factors that affect the use of health facilities are vital for increasing the utilization of institutional delivery services for African grand multiparas.
Strengths and limitations
This meta-analysis and systematic review was based on a thorough search that was independently screened, which reduced the possibility of publication bias. All sections of the manuscript were written based on the PRISMA 2020 guidelines, and the quality of each study was assessed using the Joanna Briggs Institute quality assessment tool. Although many studies assessed adverse birth outcomes and their determinants, some determinants were not assessed due to different category variables.
Implications for public health and policy
The high pooled prevalence of adverse birth outcomes among grand multiparas in Africa has several important implications for public health and policy:
Public health initiatives should prioritize the needs of grand multiparas, providing tailored antenatal care and education to address the specific risks associated with multiple pregnancies.
Improving access to quality healthcare services, including prenatal and postnatal care, is crucial. This includes ensuring that grand multiparas can access skilled birth attendants and emergency obstetric care when needed.
Raising awareness about the risks associated with grand multiparity is essential. Educational campaigns can inform women about the potential complications and encourage them to seek timely medical care.
Policymakers should consider developing guidelines that specifically address the health needs of grand multiparas, including recommendations for family planning, spacing of pregnancies, and monitoring of high-risk pregnancies.
There is a need for more research to understand the underlying causes of adverse birth outcomes in grand multiparas. Collecting and analyzing data can help identify trends and inform evidence-based interventions.
Integrating maternal health services with other health programs, such as nutrition and family planning, can provide comprehensive care that addresses the multifaceted needs of grand multiparas.
Engaging with community leaders, NGOs, and international organizations can enhance the effectiveness of public health strategies aimed at reducing adverse birth outcomes among grand multiparas.
Conclusion
Overall, the pooled prevalence of adverse birth outcomes among grand multiparas was comparably high. Variables such as rural residence, previous pregnancy-related complications, and a history of home births were significantly associated with adverse birth outcomes. Strengthening institutional births, providing high-quality prenatal care, and early pregnancy follow-ups are recommended to reduce adverse birth outcomes in grand multiparous women. In addition, improving the availability of comprehensive contraceptive options for rural-residing African grand multiparous women is essential.
Supplemental Material
sj-docx-1-reh-10.1177_26334941251342121 – Supplemental material for Adverse birth outcomes and associated factors among Sub-Saharan African grand multiparas: a systematic review and meta-analysis
Supplemental material, sj-docx-1-reh-10.1177_26334941251342121 for Adverse birth outcomes and associated factors among Sub-Saharan African grand multiparas: a systematic review and meta-analysis by Agerie Mengistie Zeleke, Getnet Azanaw Takele, Yosef Aragaw Gonete, Yeshiwas Ayale Ferede and Worku Chekol Tassew in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-2-reh-10.1177_26334941251342121 – Supplemental material for Adverse birth outcomes and associated factors among Sub-Saharan African grand multiparas: a systematic review and meta-analysis
Supplemental material, sj-docx-2-reh-10.1177_26334941251342121 for Adverse birth outcomes and associated factors among Sub-Saharan African grand multiparas: a systematic review and meta-analysis by Agerie Mengistie Zeleke, Getnet Azanaw Takele, Yosef Aragaw Gonete, Yeshiwas Ayale Ferede and Worku Chekol Tassew in Therapeutic Advances in Reproductive Health
Supplemental Material
sj-docx-3-reh-10.1177_26334941251342121 – Supplemental material for Adverse birth outcomes and associated factors among Sub-Saharan African grand multiparas: a systematic review and meta-analysis
Supplemental material, sj-docx-3-reh-10.1177_26334941251342121 for Adverse birth outcomes and associated factors among Sub-Saharan African grand multiparas: a systematic review and meta-analysis by Agerie Mengistie Zeleke, Getnet Azanaw Takele, Yosef Aragaw Gonete, Yeshiwas Ayale Ferede and Worku Chekol Tassew in Therapeutic Advances in Reproductive Health
Footnotes
Acknowledgements
The authors would like to thank the authors of the included primary studies were used as sources of information to conduct this systematic review and meta-analysis.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.